
Abstract
The aim of this study was to investigate whether post-exercise vitamin C supplementation influences recovery from an unaccustomed bout of exercise. Sixteen male subjects were allocated to either a placebo (P; n=8) or vitamin C (VC) group (n=8). Subjects performed a prolonged (90-min) intermittent shuttle-running test, and supplementation began after the cessation of exercise. Immediately after exercise the VC group consumed 200 mg of VC dissolved in a 500 ml drink, whereas the subjects in the P group consumed the drink alone. Later on the same day and then in the morning and evening of the following 2 days, subjects consumed additional identical drinks. Plasma VC concentrations in the VC group increased above those in the P group 1 h after exercise and remained above P values for the 3 days after exercise. Nevertheless, post-exercise VC supplementation was not associated with improved recovery. Post-exercise serum creatine kinase activities and myoglobin concentrations were unaffected by supplementation. Muscle soreness and the recovery of muscle function in the leg flexors and extensors were not different in VC and P groups. Furthermore, although plasma concentrations of interleukin-6 and malondialdehyde increased following exercise, there was no difference between VC and P groups. These results suggest that either free radicals are not involved in delaying the recovery process following a bout of unaccustomed exercise, or that the consumption of VC wholly after exercise is unable to deliver this antioxidant to the appropriate sites with sufficient expediency to improve recovery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Unaccustomed exercise elicits muscle damage and a reduction in the ability to generate force, with such effects usually attributed to mechanical damage generated during the exercise itself (Armstrong et al. 1991; Clarkson and Sayers 1999). However, there have been a number of reports that the extent of muscle damage increases in the post-exercise period, which is clearly unrelated to continued mechanical stress (Kuipers et al. 1983; Newham et al. 1983; MacIntyre et al. 1996). It has been suggested that such secondary damage is related to inflammation in response to the initial muscle damage (MacIntyre et al. 1996), and that such a response is also the primary cause of delayed-onset muscle soreness (Smith 1991). A number of authors have proposed that destructive phagocytes may be responsible for secondary injury, since they are unable to distinguish healthy tissue from injured tissue (Weiss 1989; MacIntyre et al. 1996). Activated neutrophils and macrophages release a number of destructive agents into the extracellular medium, including the superoxide radical (Weiss 1989), and as a result there is the potential for significant oxidative stress in the post-exercise period. Furthermore, the results of animal studies have suggested that xanthine oxidase might also contribute to post-exercise oxidative stress (Duarte et al. 1993; Radak et al. 1995). Recent evidence directly supports these possibilities, as damaged rabbit muscle is exposed to increased concentrations of free radicals up to 24 h after injury (Best et al. 1999). Consequently, although muscle damage may begin during exercise, oxidative stress following exercise may be responsible for substantial amplification of initial muscle damage and therefore play a role in delaying recovery.
The involvement of oxidative stress in the amplification of initial muscle damage might suggest that the requirement for antioxidants is increased in the post-exercise period. Furthermore, the apparent role of vitamin C (VC) in the neutralisation of phagocyte-derived oxidants may mean that this antioxidant is of particular importance (Anderson and Lukey 1987). As a corollary, there appears to be a reduction in plasma concentrations of VC the day after exercise (Gleeson et al. 1987). Furthermore, investigations that have continued to supplement with VC after exercise have shown evidence of improved recovery (Kaminski and Boal 1992; Jakeman and Maxwell 1993). In contrast, acute supplementation 2 h prior to exercise had no effect on various measures of recovery, despite achieving some of the highest plasma concentrations of VC that have been reported in the literature (Thompson et al. 2001a). It is possible that the transient increase in VC elicited by this approach did not provide VC at the time when it was most needed (i.e. post-exercise), because plasma concentrations of VC rapidly returned to baseline following exercise (Thompson et al. 2001a). With this latter point in mind, and because plasma concentrations of VC are quickly increased following the consumption of this antioxidant (Thompson et al. 2001a), it may be possible to improve recovery through the administration of VC solely after exercise. Certainly this approach would offer a great deal of convenience, as supplementation may be simply undertaken after a demanding bout of exercise in anticipation of an increased antioxidant requirement. However, there is no evidence to directly support this strategy, and therefore the aim of the present study was to investigate whether post-exercise VC supplementation would influence recovery from an unaccustomed bout of exercise.
Methods
Subjects
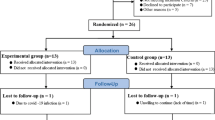
Sixteen male students volunteered to take part in this study, which had approval from Loughborough University Ethical Advisory Committee. All subjects were informed verbally and in writing about the nature and demands of the study, and subsequently completed a health history questionnaire and gave their written informed consent. Subjects who smoked or took vitamin supplements were excluded from the investigation. All participants were habitually active in a variety of sports, although none were familiar with the exercise protocol used in the present study. Subjects were allocated to either a VC or a placebo (P) group in a double-blind design (Table 1). Physical characteristics, self-reported levels of habitual activity, and skinfold measurements taken from four sites (biceps, triceps, subscapular and suprailiac) were similar between the two groups (Table 1). Furthermore, normal dietary intake of VC was assessed over a 5-day period prior to other testing and was similar between groups (Table 1).
Experimental design and procedures
Subjects performed the Loughborough Intermittent Shuttle Test (LIST) as described previously (Thompson et al. 1999). Briefly, the LIST consisted of 90 min of variable intensity shuttle-running over a 20 m distance, including walking, jogging and sprinting. Subjects were instructed to abstain from strenuous exercise for 2 days prior to exercise, and not to resume exercising until the conclusion of testing. On the day of the test subjects arrived at the laboratory after an overnight fast of between 10 h and 12 h. An indwelling cannula (18G, Venflon BOC Ohmeda AB, Sweden) was inserted into a forearm vein under local anaesthetic (1% lignocaine, Antigen Pharmaceuticals, Ireland) and kept patent with sterile saline solution (0.9% sodium chloride, Steripak, UK). A resting blood sample was then taken after subjects had been standing for at least 15 min, after which subjects consumed a light standardised meal and drink and rested for 2 h. The meal consisted of 1.7 g white bread and 0.3 g of low-fat spread, both values are per kilogram body mass (Sainsbury's, UK).
Pre-exercise muscle function and soreness were assessed during the 2 h period between the consumption of the pre-exercise meal and the start of the LIST. Muscle function was assessed in the flexors and extensors of both legs on an isokinetic dynamometer (CYBEX model 770, LUMEX, USA). Subjects were familiarised with the muscle function test on at least two occasions during preliminary visits to the laboratory. Prior to all muscle function measurements, subjects were taken through a standardised warm-up consisting of 5 min of gentle running and stretching. There were five stages to the muscle function test: (1) ten sub-maximal contractions at 1.05 rad s−1, (2) three maximal contractions at 1.05 rad s−1, (3) two warm-up movements at a faster speed of 3.14 rad s−1, immediately followed by three maximal contractions at this speed, (4) one 5-s isometric extension at an angle of 1.13 rad flexion, and finally, (5) one 5-s isometric flexion at an angle of 0.35 rad flexion. There was a 25-s rest period between each of these stages. The intensity of pre-exercise soreness was rated on a ten-point scale ranging from 1 (not sore), to 10 (very very sore). Soreness was assessed whilst the subjects actively contracted specific muscles as described previously (Thompson et al. 1999). Briefly, this involved the performance of a variety of fixed-weight exercises at 75% of each individual's one-repetition maximum. Soreness was assessed in this manner during a hamstring curl, quadriceps extension, lateral pull, biceps curl and triceps extension (CYBEX models 4113, 4108, 5315 and 4005, LUMEX, USA).
Subjective ratings of perceived exertion were recorded every 15 min during the LIST (Borg 1973), and heart rate was monitored every 15 s by short-range telemetry (Sports Tester, Polar Electro, Finland). Subjects were allowed to consume water ad libitum throughout exercise, although the volume was monitored and used in the subsequent calculation of sweat loss. Nude body mass was determined immediately before and after exercise. A venous blood sample was taken immediately post-exercise and additional samples were taken 1 and 2 h after exercise.
For 3 days after the LIST, subjects returned to the laboratory after an overnight fast and at approximately the same time of the morning (within 1 h). A blood sample was taken by venepuncture from a forearm vein after the subject had been standing for at least 15 min. Subsequently, subjects rated the intensity of soreness and performed the muscle function test outlined above.
For the 2 days prior to the main trial and 3 days afterwards subjects weighed and recorded a prescribed diet that was designed by a dietician to be similar to their own. This prescribed diet was based on the 5-day weighed food and fluid intake records that were determined before any other testing had taken place. However, the amount of dietary VC was controlled in order to provide 100 mg day−1. In addition to the 100 mg of VC that all subjects received in their diets, subjects in the VC group consumed 200 mg of VC, twice a day, for the 3 days after exercise. This dosage is associated with complete bioavailability (Levine et al. 1996), and prolonged intake at this level has had beneficial outcomes in the past (Jakeman and Maxwell 1993). VC (ascorbic acid) was administered dissolved in 500 ml of an energy-free version of a commercially available drink (Lucozade-Sport, SmithKline Beecham, UK), with the same drink without VC being given to subjects in the P group. An investigator added VC to the drinks immediately prior to consumption, and the subjects consumed all drinks in the laboratory. The first drink was given immediately after completion of the LIST, and the second drink in the evening of the same day. For the following 2 days subjects consumed further drinks in the morning and evening of each day. Weighed food records were analysed by a registered dietician using the software COMP-EAT 4.0 (Nutrition Systems, UK).
Blood sampling and analysis
Approximately 11 ml of whole-blood was withdrawn at each time point, and 7 ml of whole-blood was added to tubes containing ethylenediaminetetra-acetic acid (EDTA) as an anticoagulant. Several small aliquots of EDTA-treated blood (20 μl) were removed for the determination of lactate, glucose and changes in plasma volume as described previously (Thompson et al. 1999). An aliquot of EDTA-treated blood (~4 ml) was subsequently centrifuged at 3,000 g for 15 min (4°C) to obtain plasma, most of which was dispensed and immediately frozen in liquid nitrogen. An aliquot of plasma (0.6 ml) was added to 0.6 ml of 10% metaphosphoric acid (Sigma, UK), mixed, and immediately frozen in liquid nitrogen and stored at −70°C until the supernatant was analysed for VC as described previously (Thompson et al. 2001a). The remaining EDTA-treated whole blood (~3 ml) was transferred to tubes containing separation medium, and lymphocytes were collected and analysed for VC as described previously (Thompson et al. 2001a). Serum was obtained by allowing whole blood (~4 ml) to clot for 20 min, followed by chilled centrifugation (4°C) at 3,000 g (Koolspin, Burkard Scientific, UK).
Serum creatine kinase (CK), myoglobin and uric acid were determined at 37°C using commercially available methods (Roche Products, UK), and an automated system (COBAS Mira Plus, Roche Diagnostic Systems, Switzerland). Serum cortisol concentrations were determined using a commercially available radioimmunoassay (Coat-A-Count, Diagnostica Products, USA). Radioactivity was measured using an automated gamma counter (Cobra II, Packard Instrument Co., USA). Plasma was analysed for interleukin-6 (IL-6) using a commercially available solid-phase high-sensitivity ELISA (Quantikine, R and D Systems, UK), and plasma malondialdehyde (MDA) analysis was based on the method described by Fukunaga et al. (1993).
Statistical analysis
An independent two-way analysis of variance with repeated measures was used to compare results between treatments and over time. Where significant F ratios were found, a Tukey Honest Significant Difference test was used to determine the location of the variance. When there were only single comparisons, a Student's t-test for correlated data was used to determine whether any differences between treatments existed. Certain results were not normally distributed (CK and myoglobin), and therefore these values were log transformed prior to ANOVA. Log transformation always resulted in a normal distribution, and therefore these ANOVA results are reported. Significance was accepted at the 5% level, and values are presented as means (SEM). Effect size (ES) is also presented as suggested by Thomas et al. (1991) and was calculated at the time point after supplementation that was associated with the maximum difference between supplemented and P groups (treatment − control). These results were treated according to convention where 0.2 represents a small effect, 0.5 a moderate effect and 0.8 a large effect.
Results
The physiological responses to exercise were similar between groups. Heart rate throughout exercise was 169 (3) beats min−1 in the VC group and 172 (3) beats min−1 in the P group. Mean rating of perceived exertion during the LIST was the same, being 15 (1) in both groups. Blood glucose concentrations at the end of exercise were 4.1 (0.3) mmol l−1 in the VC group, and were not different to the 4.2 (0.2) mmol l−1 observed in the P group. Blood lactate concentrations at the end of exercise were also comparable in both groups [5.0 (0.6) vs 4.4 (0.7) mmol l−1 for VC and P groups]. Mean ambient temperature was similar in VC and P groups [18.3 (0.5) vs 18.6 (0.6)°C], as was relative humidity [64 (4) vs 64 (5)%]. Subjects in the VC group consumed 1.5 (0.2) l of water during exercise and lost 2.0 (0.1) kg in body mass (after correction for fluid intake), which was not different to the P group, who consumed 1.8 (0.2) l of water and lost 2.2 (0.2) kg in body mass. Mean sprint time over the course of the LIST was 2.54 (0.07) s in the VC group, which was not different to the mean time of 2.52 (0.03) s in the P group. Plasma volume changes were not different between VC and P groups at any point over the period of testing (data not shown).
There were no differences between groups in terms of dietary composition over the 5-day period of the test (Table 2). Furthermore, subjects in both groups successfully adhered to the prescribed diet, and daily VC intake was close to the target of 100 mg.
Plasma and lymphocyte VC
Plasma VC concentrations increased similarly over the course of exercise in VC and P groups (Fig. 1) (P<0.01). This was to be expected, as VC was not given to the supplemented group until after exercise. Values remained significantly elevated in the P group for a further hour after the completion of exercise (P<0.01). Plasma concentrations of VC increased above those seen in the P group 1 h after consuming VC (Fig. 1), and remained significantly above P values for the following 72 h (P<0.01). The highest observed mean plasma VC concentration in the supplemented group was 92.2 (7.0) μmol l−1, which was 1 h after exercise (ES = 1.60).

Plasma (A) and lymphocyte (B) vitamin C (VC) concentrations. Values represent means (SEM) (n=8). *Placebo (P) and VC groups above baseline values (P<0.01), †VC group above P group values and baseline values (P<0.01), #P group above baseline values (P<0.01). −2 Baseline, Pre pre-exercise, PE post-exercise
Lymphocyte VC concentrations increased after exercise in both groups (Fig. 1), and remained significantly above baseline levels until 24 h after exercise (P<0.01). Although there was a tendency for lymphocyte concentrations to be higher in the VC group after taking the supplement, values were not significantly different at any time (ES = 0.51).
Markers of muscle damage
Serum activities of CK were elevated above baseline levels immediately after exercise in both groups (P<0.01), although peak activity was not seen until 24 h after exercise (Fig. 2). CK activities remained significantly above pre-exercise values until 72 h post-exercise, and were not different between groups at any point (ES = −0.26). Serum myoglobin concentrations also increased above pre-exercise values immediately after exercise (P<0.01), and appeared to peak 1 h post-exercise (Fig. 2; ES = −0.12). Myoglobin concentrations in both groups remained above baseline values 24 h after exercise (P<0.01), and every subject had elevated serum myoglobin concentrations at this point.

Serum creatine kinase activities (A) and myoglobin concentrations (B). Values represent means (SEM) (n=8). *P and VC groups above baseline values (P<0.01)
Plasma MDA and IL-6
Plasma MDA concentrations were above baseline values in both groups at the end of exercise (Fig. 3), and remained above baseline values until 24 h after exercise (P<0.05). There were no differences for MDA between VC and P groups at any time throughout the study (ES = −0.65). Plasma levels of IL-6 increased in both groups over the course of exercise (P<0.01), but there were no differences between groups at any time point (Fig. 4; ES = 0.26).

Plasma malondialdehyde concentrations. Values are means (SEM) (n=8). *P and VC groups above baseline values (P<0.05)

Plasma interleukin-6 concentrations. Values are means (SEM) (n=8). *P and VC groups above pre-exercise values (P<0.01)
Muscle function
Muscle function was impaired in the leg flexors in both VC and P groups (Table 3). Muscle function was also impaired in the leg extensors in both groups, although the decline was less pronounced than in the leg flexors (data not shown). Maximal isometric force was below baseline levels in both leg flexors for 72 h after exercise (P<0.01), but was not different between groups. Similarly, maximal isokinetic torque at 1.05 rad s−1 was not different between groups but was below baseline for 48 h after exercise (P<0.01). At the faster speed of 3.14 rad s−1, muscle function was only significantly below baseline levels immediately after exercise (P<0.05). The ES values for muscle function are presented in Table 3 (range, −0.29 to 1.14).
Soreness
Muscle soreness increased in both VC and P groups 24–72 h after exercise (Table 4). The hamstrings and quadriceps were both greatly affected, and hamstring soreness persisted until 72 h after exercise. Soreness did not significantly increase above pre-exercise levels in the biceps or triceps of either group. There appeared to be a tendency for soreness to be higher in the VC group, although values were only significantly different 24 h after exercise in the leg extensors (P<0.05). The ES values for muscle soreness are presented in Table 4 (range 0.46–1.14).
Cortisol and uric acid
Serum levels of cortisol were not different between VC and P groups at any point (Table 5). Cortisol concentrations increased at the end of exercise in both groups, and remained above pre-exercise levels 1 h after exercise (P<0.01; ES = −0.48). There were no differences in serum concentrations of uric acid between groups at any point over the testing period (Table 5). Uric acid concentrations increased above pre-exercise levels and remained elevated until 24 h after exercise (P<0.05; ES = −0.80).
Discussion
The aim of the present study was to investigate whether post-exercise VC supplementation influences recovery from an unaccustomed bout of exercise. VC supplementation successfully increased plasma VC concentrations above those in the P group 1 h after exercise, and plasma VC concentrations remained above P values for the 3 days after exercise. Nevertheless, post-exercise VC supplementation was not associated with improved recovery following exercise. The level of circulating muscle proteins, the sensation of muscle soreness, plasma markers of lipid peroxidation and inflammation, and the loss of muscle force were similar in VC and P groups.
Plasma concentrations of VC increased at the end of exercise in the present investigation, which is in agreement with a number of previous studies (Gleeson et al. 1987; Rokitski et al. 1994; Thompson et al. 2001a, b). Post-exercise VC supplementation increased plasma concentrations of VC after this point, and therefore successfully increased the availability of this antioxidant within 1 h of exercise. Plasma concentrations of VC have been reported to fall in the days following physical stress (Shukla 1969; Gleeson et al. 1987), although they did not change in the P group in the present study. It is likely that the provision of 100 mg of VC in the normal diet of the P group was sufficient to prevent any such decline from occurring. Nevertheless, plasma VC concentrations in the supplemented group remained above the P group for the 3 days of supplementation after exercise.
VC was also determined in lymphocytes, which, along with other leukocytes, are believed to reflect tissue concentrations of VC (Levine et al. 1996). Although there was a tendency for lymphocyte VC concentrations to be greater following supplementation, this difference was not statistically significant. This finding may be related to the relatively high VC intake of our subjects as, on average, they consumed 138 mg of VC a day in their normal diet prior to supplementation. It has been suggested that all types of leukocyte, including lymphocytes, become saturated at VC intakes of 100–200 mg per day (Levine et al. 1996). Therefore, it is likely that lymphocytes were already saturated prior to supplementation in the present study, and that increasing the availability of VC led to no further uptake by these cells. However, compartments such as the plasma do not become saturated until consumption is considerably greater than that observed in the normal diet of the subjects in the present study (Levine et al. 1996; Benzie and Strain 1997). This is an important factor, since the rationale for supplementing with VC after exercise in the current investigation was that extracellular oxidative stress might be responsible for the amplification of muscle damage in the post-exercise period.
The increase in circulating muscle proteins (CK and myoglobin) observed following the intermittent exercise protocol used in the present study is consistent with findings reported in earlier studies (Thompson et al. 1999, 2001a, b). CK activity peaked the day after exercise, whereas myoglobin concentrations peaked 1 h after exercise. The temporal discrepancy between these two markers of muscle damage has been reported following several forms of exercise (Sorichter et al. 1997; Koller et al. 1998), and may be related to different rates of release or clearance of these proteins. The results of the present study suggest that myoglobin is released more rapidly than CK, which may be due to the considerable size difference between these molecules. Furthermore, myoglobin is cleared within a few minutes from the circulation (Klocke et al. 1982), whereas the half-life for CK is approximately 15 h (Neumeier et al. 1981). Consequently, it is unlikely that post-exercise VC supplementation would have had any effect on serum myoglobin concentrations within 1 h of exercise, or serum CK activity on the day of exercise. Nevertheless, since myoglobin concentrations remained elevated until 24 h post-exercise, and CK until 72 h post-exercise, there was probably sufficient time for these processes to be influenced by supplementation. However, the similar level of blood-borne muscle proteins in P and supplemented groups indicates that the administration of VC after the cessation of exercise was unable to affect membrane permeability and the release of muscle proteins into the circulation.
In the present study, plasma MDA was elevated for 24 h after exercise in both P and VC groups. This indicates that lipid peroxidation continued until this time, as MDA is normally cleared from the circulation within several hours (Jenkins et al. 1993). Theoretically, the loss of sarcolemmal integrity may be due to extensive lipid peroxidation of membrane unsaturated fatty acids (Demopoulos 1973). Lipid peroxidation may also decrease membrane fluidity, and therefore alter membrane structure and function without the loss of membrane integrity (Demopoulos 1973). The lack of any difference between VC and P groups suggests that supplementation had no effect on post-exercise lipid peroxidation.
It has been suggested that the best measure of muscle damage is not a biochemical marker such as CK, but the functional assessment of maximal voluntary force (Warren et al. 1999). Contractile dysfunction may highlight damage inside cells that is not reflected by the extent of lipid peroxidation or the efflux of muscle proteins (Kong et al. 1994; Van Der Meulen et al. 1997). In the present study, both VC and P groups exhibited poorer muscle function for up to 72 h after exercise, and the decline was most prominent in the leg flexors. This is in agreement with our earlier observation that this muscle group is the most affected after this type of exercise (Thompson et al. 1999, 2001b). A decline in the ability to generate force may be largely the result of damage produced by severe mechanical stress (Armstrong et al. 1991). Alternatively, impaired muscle function may occur partly as a consequence of free-radical reactions (Zerba et al. 1990). The results of the present investigation suggest that if the disturbance to muscle function reported in the present investigation was mediated by radicals generated in the post-exercise period, supplementation with VC appeared to be unable to alter the extent of this decline.
Secondary damage may be the result of the non-specific actions of phagocytes during an inflammatory response (Weiss 1989; MacIntyre et al. 1996). The prolonged efflux of muscle proteins in the present study may indicate that the damage process continued in the post-exercise period. Furthermore, circulating levels of cytokines increase during inflammation, including after damaging exercise (Pedersen et al. 1998). As reported previously (Thompson et al. 2001b), there was an increase in plasma IL-6 after the intermittent exercise protocol used in the present investigation. However, whereas prolonged VC supplementation had a pronounced effect on plasma IL-6 2 h after exercise (Thompson et al. 2001b), VC supplementation after exercise in the present study did not have any effect on post-exercise plasma IL-6 concentrations. As a corollary, since it has been proposed that muscle soreness is directly related to the inflammatory response (Smith 1991), the similar soreness sensation in VC and P groups may be further evidence that post-exercise supplementation had no effect on the normal inflammatory response to intense exercise. Indeed, it is interesting to note that there was actually a tendency for soreness to be higher in the VC group.
In summary, the results of the present investigation demonstrate that there is no benefit from the administration of VC after a demanding bout of exercise. It is possible that inflammation is initiated in order to facilitate tissue healing (Tidball 1995), and plays no part in the secondary damage process. Similarly, xanthine oxidase-derived free radicals may not contribute to muscle damage and impair the recovery process. However, earlier studies have suggested that this is not the case, as anti-inflammatory agents (Hasson et al. 1993; Bushell et al. 1996), and inhibitors of xanthine oxidase (Duarte et al. 1993; Radak et al. 1995), appear to confer distinct benefits. A more probable explanation is that consumption of VC wholly after exercise is unable to deliver this antioxidant to the appropriate sites with sufficient expediency to improve recovery.
References
Anderson R, Lukey P (1987) A biological role for ascorbate in the selective neutralisation of extracellular phagocyte-derived oxidants. Ann N Y Acad Sci 498:229–247
Armstrong R, Warren G, Warren J (1991) Mechanisms of exercise-induced muscle fibre injury. Sports Med 12:184–207
Benzie I, Strain J (1997) Acute post-ingestion changes in plasma ascorbic acid concentration: Relationship to dose and existing body stores. Nutr Res 17:187–190
Best T, Fiebig R, Corr D, Brickson S, Ji L (1999) Free radical activity, antioxidant enzyme, and glutathione changes with muscle stretch injury in rabbits. J Appl Physiol 87:74–82
Borg G (1973) Perceived exertion: a note on ''history'' and methods. Med Sci Sports Exerc 5:90–93
Bushell A, Klenerman L, Davies H, Grierson I, Jackson M (1996) Ischaemia-reperfusion-induced muscle damage. Acta Orthop Scand 67:393–398
Clarkson P, Sayers S (1999) Etiology of exercise-induced muscle damage. Can J Appl Physiol 24:234–248
Demopoulos H (1973) Control of free radicals in biologic systems. Fed Proc 32:1903–1908
Duarte J, Appell H, Carvalho F, Bastos M, Soares, J (1993) Endothelium-derived oxidative stress may contribute to exercise-induced muscle damage. Int J Sports Med 14:440–443
Fukunaga K, Suzuki T, Takama K (1993) Highly sensitive high-performance liquid chromatography for the measurement of malondialdehyde in biological samples. J Chromatogr B Anal Technol Biomed Life Sci 621:77–81
Gleeson M, Robertson J, Maughan R (1987) Influence of exercise on ascorbic acid status in man. Clin Sci 73:501–505
Hasson S, Daniels J, Divine J, Niebuhr B, Richmond S, Stein P, Williams J (1993) Effect of ibuprofen use on muscle soreness, damage, and performance: a preliminary investigation. Med Sci Sports Exerc 25:9–17
Jakeman P, Maxwell S (1993) Effect of antioxidant vitamin supplementation on muscle function after eccentric exercise. Eur J Appl Physiol 67:426–430
Jenkins R, Krause K, Schofield L (1993) Influence of exercise on clearance of oxidant stress products and loosely bound iron. Med Sci Sports Exerc 25:213–217
Kaminski M, Boal R (1992) An effect of ascorbic acid on delayed-onset muscle soreness. Pain 50:317–321
Klocke F, Copley D, Krawczyk J, Reichlin M (1982) Rapid renal clearance of immunoreactive canine plasma myoglobin. Circulation 65:1522–1528
Koller A, Mair J, Schobersberger W, Wohlfarter T, Haid C, Mayr M, Villiger B, Frey W, Puschendorf B (1998) Effects of prolonged strenuous endurance exercise on plasma myosin heavy chain fragments and other muscular proteins. J Sports Med Phys Fitness 38:10–17
Kong Y, Lesnefsky E, Ye J, Horwitz L (1994) Prevention of lipid peroxidation does not prevent oxidant-induced myocardial contractile dysfunction. Am J Physiol 267:H2371–H2377
Kuipers H, Drukker J, Frederik PM, Geurten P, Kranenburg G (1983) Muscle degeneration after exercise in rats. Int J Sports Med 4:45–51
Levine M, Conry-Cantilena C, Wang Y, Welch R, Washko P, Dhariwal K, Park J, Lazarev A, Graumlich J, King J, et al (1996) Vitamin C pharmacokinetics in healthy volunteers: evidence for a recommended dietary allowance. Proc Natl Acad Sci U S A 93:3704–3709
MacIntyre D, Reid W, Lyster D, Szasz I, McKenzie D (1996). Presence of WBC, decreased strength, and delayed soreness in muscle after eccentric exercise. J Appl Physiol 80:1006–1013
Neumeier D, Prellwitz W, Knedel M (1981) Creatine kinase isoenzymes after myocardial infarction. In: Lang H (ed) Creatine kinase isoenzymes. Springer, Berlin Heidelberg New York, pp132–154
Newham D, McPhail G, Mills K, Edwards R (1983) Ultrastructural changes after concentric and eccentric contractions of human muscle. J Neurol Sci 61:109–122
Pedersen B, Ostrowski K, Rohde T, Bruunsgaard H (1998) The cytokine response to strenuous exercise. Can J Physiol Pharmacol 76:505–511
Radak Z, Asano K, Inoue M, Kizaki T, Oh-ishi S, Suzuki K, Taniguchi N, Ohno H (1995) Superoxide dismutase derivative reduces oxidative damage in skeletal muscle of rats during exhaustive exercise. J Appl Physiol 79:129–135
Rokitski L, Logemann E, Sagredos A, Murphy M, Wetzel-Roth W, Keul J (1994) Lipid peroxidation and antioxidant vitamins under extreme endurance stress. Acta Physiol Scand 151:149–158
Shukla S (1969) Plasma and urinary ascorbic acid levels in the post-operative period. Experientia 25:704
Smith L (1991) Acute inflammation: the underlying mechanism in delayed onset muscle soreness? Med Sci Sports Exerc 23:542–551
Sorichter S, Mair J, Koller A, Gebert W, Rama D, Calzolari C, Artner-Dworzak E, Puschendorf B (1997) Skeletal troponin I as a marker of exercise-induced muscle damage. J Appl Physiol 83:1076–1082
Thomas JR, Salazar W, Landers DM (1991) What is missing in p<0.05? Effect Size. Res Q Exerc Sport 62:344–348
Thompson D, Nicholas CW, Williams C (1999) Muscle soreness following prolonged intermittent high-intensity shuttle running. J Sports Sci 17:1-9
Thompson D, Williams C, Kingsley M, Nicholas CW, Lakomy HKA, McArdle F, Jackson MJ (2001a). Muscle soreness and damage parameters after prolonged intermittent shuttle-running following acute vitamin C supplementation. Int J Sports Med 22:68–75
Thompson D, Williams C, McGregor S, Nicholas CW, McArdle F, Jackson MJ, Powell J (2001b) Prolonged vitamin C supplementation and recovery from demanding exercise. Int J Sports Nutr Exerc Metab 11:468–484
Tidball J (1995) Inflammatory cell response to acute muscle injury. Med Sci Sports Exerc 27:1022–1032
Van Der Meulen J, McArdle A, Jackson M, Faulkner J (1997) Contraction-induced injury to the extensor digitorum longus muscles of rats: the role of vitamin E. J Appl Physiol 83:817–823
Warren G, Lowe D, Armstrong R (1999) Measurement tools used in the study of eccentric contraction-induced injury. Sports Med 27:43–59
Weiss S (1989) Tissue destruction by neutrophils. N Engl J Med 320:365–376
Zerba E, Komorowski T, Faulkner J (1990) Free radical injury to skeletal muscles of young, adult and old mice. Am J Physiol 258:C429–C435
Acknowledgements
The authors would like to acknowledge the financial support of SmithKline Beecham, UK. The work described in this paper complies with the current laws of the UK.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Thompson, D., Williams, C., Garcia-Roves, P. et al. Post-exercise vitamin C supplementation and recovery from demanding exercise. Eur J Appl Physiol 89, 393–400 (2003). https://doi.org/10.1007/s00421-003-0816-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-003-0816-4