
Abstract
The maximal lactate steady state (MLSS) is the highest blood lactate concentration (BLC) that can be identified as maintaining a steady-state during a prolonged submaximal constant workload. Comparative interpretation of published data about MLSS is complicated by the fact that different methods of testing have been utilized. Thus, three methods, corresponding to the time course of changes in BLC incurred during either 30 min (MLSS I) or 20 min (MLSS II and III) of constant submaximal workload exercise, were compared in 26 male subjects [mean (SD) age 24.6 (5.6) years, height 181.6 (4.9) cm, body mass 74.4 (5.2) kg]. MLSS I [5.1 (1.3) mmol·l-1], II [4.9 (1.3) mmol·l-1], and III [4.3 (1.3) mmol·l-1] were different (P<0.01). The workload corresponding to MLSS III [244.8 (44.0) W] was lower (P<0.01) than that at MLSS I [254.0 (40.8) W] and II [251.9 (40.4) W]. No difference could be confirmed between the workloads established for MLSS I and MLSS II. The differences between MLSS I, MLSS II, and MLSS III and corresponding workloads reflect insufficient contribution to lactate kinetics by testing procedures that depend strongly upon the time course of changes in BLC during the initial 20–25 min of constant-workload exercise. Based on the present findings, constant-load tests lasting at least 30 min and a BLC increase of no more than 1.0 mmol·l-1 after the 10th testing minute appear to be the most reasonable with respect to valid testing results.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The maximal lactate steady state (MLSS) is the highest blood lactate concentration (BLC) that can be identified as maintaining a steady-state during prolonged submaximal constant workload. The workload corresponding to the MLSS (MLSS workload) presumably represents the highest submaximal exercise intensity (MLSS intensity) that can be performed without anaerobic energy metabolism (Beneke 1995; Heck 1990; Heck et al. 1985). Above MLSS intensity, the kinetics of the BLC show a clearly identifiable increase with time during constant-workload exercise (Beneke 1995; Heck 1990; Heck et al. 1985).
The physiological background of the MLSS is comparable with the theory of the anaerobic threshold. Determination of the anaerobic threshold requires an incremental load test that is a generally accepted and a more or less standardized basic procedure of exercise testing (Beneke 1995; Heck 1990; Mader and Heck 1986). Nevertheless, various concepts of the anaerobic threshold do not necessarily provide identical levels of lactate and/or workloads at MLSS and/or MLSS workload (Beneke 1995). Consequently, the determination of MLSS requires several subsequent constant submaximal load tests performed on separate days (Aunola and Rusko 1992; Beneke 1995; Beneke and von Duvillard 1996; Beneke et al. 1996; Haverty et al. 1988; Heck 1990; Mocellin et al. 1990; Urhausen et al. 1993).
The interpretation of selected findings regarding the MLSS is complicated by the fact that different test protocols and definitions of MLSS have been utilized in the past. In principle, all methods differed with respect to test duration, period of constant-load exercise observed for the interpretation of the BLC kinetics, and the maximally accepted increase in BLC (Table 1). However, thus far only three selected methods have been compared intraindividually (Beneke et al. 1996). The present study adds corresponding knowledge and may provide a general approach for the comparative interpretation of previous MLSS results.
Methods
Subjects
A total of 26 men [mean (SD) age 24.6 (5.6) years, height 181.6 (4.9) cm, body mass 74.4 (5.2) kg, oxygen uptake 4.5 (0.6) l·min−1] volunteered to participate in this study. Of these, 18 subjects were endurance athletes (triathlon, cycling, or rowing) with a weekly volume of training between 10 and 20 h. Eight subjects were recreational sportsmen and not specifically trained. All were healthy. Institutional ethical approval was received, and informed consent to participate was obtained from all subjects prior to all testing.
Procedure
All subjects performed one incremental maximal-load test and five to ten constant submaximal load tests on an electronically braked cycle ergometer (380, Fa. Elema Schönander, Siemens, Germany). The pedaling rate was set at 60 rev·min−1. Individual tests were conducted at the same time in the afternoon. Intervals between two tests lasted at least 48 h. All subjects were instructed not to engage in strenuous activity during the day before an exercise test.
Test protocols
The incremental progressive-load program started at 50 W and was increased by 50 W every 3 min until exhaustion. The number of stages completed at prescribed workloads was between five and eight and a half. The resulting test duration lasted 15–25.5 min. This test provided the peak workload measured at the termination of the test and the BLC power ratio for every stage of each workload. Based on the latter, the individual workloads corresponding to a BLC value of 3.0 mmol·l-1 were determined.
Each constant-load test session consisted of a warm-up period of 3 min at 50 W and a 30-min constant-workload exercise bout. In the first constant-load test, the workload was identical to that determined previously at the BLC value of 3.0 mmol·l-1 in the incremental load test. In general, in a prolonged constant-load test this workload intensity gives a BLC steady state that is slightly higher than 3.0 mmol·l-1. If during the first constant-load test a steady state or a decrease in lactate was observed, further subsequent 30-min constant-load tests with 3–10% higher workload intensities were performed on separate days until no BLC steady state could be maintained. If the first constant-load test resulted in a clearly identifiable increase of the BLC and/or could not be completed due to exhaustion, further constant workloads were conducted with subsequently reduced workload intensities.
Lactate
Capillary blood samples (20 µl) were taken from the hyperemic ear lobe (Finalgon, Thomae, Biberach, Germany) at the beginning of the test and at the end of each stage. At the constant workloads, lactate levels were measured at the beginning and at the end of the warming-up period, and at the end of every 5th min. Lactate was analyzed by the enzymatic photometric method (Boehringer, Mannheim, Germany). At BLC levels in the range 0.6–11.7 mmol·l-1, the coefficient of variation for repetitive analysis of the identical sample was 4.8 (4.2)% (Beneke et al. 1994).
Maximal lactate steady state
Each constant-workload test was analyzed according to three different methods of defining MLSS (MLSS I, II, and III): MLSS I was determined by analyzing the BLC between the 10th and the 30th min of constant workload exercise. During this period the increase of BLC was limited to no more than 1.0 mmol·l-1 (e.g., 0.05 mmol·l-1·min-1; see also method nos. 3, 4, 8, 9, and 12 in Table 1). MLSS II was based on the time course of changes in BLC between the 10th and the 20th min. During this period of constant-workload exercise, the maximal increase of BLC was limited to no more than 0.5 mmol·l-1, which was similar to the increase per unit time as defined for MLSS I (0.05 mmol·l-1·min-1), but reduced the test duration by 33% (see also method no. 2 in Table 1). For MLSS III, the time course of changes in BLC between the 10th and the 20th min were also considered. Here, MLSS was defined as an increase in BLC of no more than 0.2 mmol·l-1 (e.g., 0.02 mmol·l-1·min-1; see also method no. 7 in Table 1).
MLSS I was calculated as the average BLC measured at the 15th, 20th, 25th, and 30th min; MLSS II and III were the average of BLC values measured at the 15th and 20th min of the corresponding constant-load tests.
Statistics
Data are reported as the mean (SD). Wilcoxon and Friedmann tests were used to determine intraindividual mean differences. Differences between methods were further analyzed by orthogonal regression, and the relationship between variables was tested by linear and by non-linear regression procedures. If a steady-state BLC was assumed, the time course of BLC was described utilizing the following mono-exponential term (Dost 1968): BLC(t) = BLCSS − (BLCSS − BLC0) e (-t/τ), where BLC(t) = BLC as function of test duration (mmol·l-1), BLCSS = steady-state BLC (mmol·l-1), BLC0 = BLC at the beginning of constant-workload exercise (mmol·l-1), t = duration of constant-workload exercise (min), τ = time constant of the BLC response (min). For all statistical analyses, the level of significance was set at P≤0.05.
Results
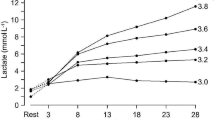
MLSS I, MLSS II, and MLSS III were significantly different (P≤0.01; Table 2). The time courses of the BLC values resulting in MLSS I and MLSS II exhibited an increase (P≤0.05) until the 25th and 20th min, respectively. The corresponding values of τ were 4.76 (0.21) min and 4.27 (0.23) min. For MLSS III there was no increase of BLC after the 10th min, resulting in a τ value of 2.56 (0.19) min (Fig. 1).

Time course of changes in blood lactate concentration (BLC), as assessed by three different methods of determining the maximum lactate steady state (MLSS): MLSS I, II, and III. For a detailed account of these methods, please refer to Methods. The non-linear increase in BLC observed during the initial phase of the constant-workload test can be described by τ values of 4.76 (0.21) min for MLSS I (r = 0.97, n = 182, P≤0.001), 4.26 (0.26) min for MLSS II (r = 0.96, n = 130, P≤0.001), and 2.56 (0.19) min for MLSS III (r = 0.98, n = 130, P≤0.001)
The workloads at MLSS I and MLSS II were higher (P≤0.01) than that at MLSS III (Table 2). High correlations were found between the peak workload [356.2 (48.9) W] and the workloads at MLSS I, II, and III, respectively (Fig. 2).

Correlation between peak workload and MLSS I workload (r = 0.84, n = 26, P≤0.001, y = 0.7x + 3.55), MLSS II workload (r = 0.85, n = 26, P≤0.001, y = 0.7x + 1.51), and MLSS III workload (r = 0.89, n = 26, P≤0.001, y = 0.81x + 42.1), respectively
Only 19 of the 26 subjects were able to sustain a 30-min constant workload of 273.7 (36.9) W, which was 6.1 (3.3)% higher (P≤0.001) than the MLSS I workload. After 30 min, the BLC was 8.2 (2.4) mmol·l-1. The clearly identifiable increases in BLC between the 10th, 20th, and 30th min were 1.1 (0.7) and. 2.4 (1.0) mmol·l-1, respectively (Fig. 3).

BLC during a 30-min constant-workload test at MLSS I workload and at 106% of MLSS I workload. Only 19 of the 26 subjects were able to sustain 30 min of constant-workload exercise with a more or less linear increase in BLC after the 10th testing minute
Discussion
Published methods of MLSS determination are different in principle with respect to test duration and the period of constant workload selected for the interpretation of the BLC response and the maximally accepted increase of BLC (Table 1). All investigators except those of method no. 6 (Table 1), which cannot be evaluated with the present study, restricted the maximal increase of BLC per unit time to a range between 0.02 and 0.05 mmol·l-1·min-1. Method no.13 (Table 1) is the only procedure involving a constant workload lasting longer than 30 min. Method nos.10 and 14 (Table 1) required less than 20 min. Methods nos. 2, 10, and 14 (Table 1) had been developed especially for children. They were based on the assumption that shorter durations of testing may be favorable for the compliance of children, and have been compared previously (Beneke et al. 1996). The present study emphasizes and extends the latter findings that distinct methods of MLSS determination result in different values for the MLSS and MLSS workloads. The procedures of the present study cover the relevant range of BLC increases and also test durations except method no. 13 (Table 11). Thus, the present combination of methods and results enable a general interpretation of currently relevant procedures for measurement of MLSS.
The observed differences between MLSS I, II, and III can be explained by the typical time course of the changes in BLC during constant-load tests, which result from the dynamic equilibrium between lactate appearance in and disappearance from the blood compartment. The time course is determined by BLC0, BLCSS and τ (Beneke et al. 1996; Dost 1968; Heck 1990; Heck et al. 1994). τ specifies the velocity of the adaptation to the resulting BLCSS. After a period of 4τ, 99% of the final BLCSS is reached. Previous investigations have demonstrated, that τ is related to the level of the BLCSS (τ = a × BLCSS + b); a and b were found to be 0.4318 min·mmol·l-1 and 1.264 min (Heck 1990), and 0.39 min·mmol·l-1 and 0.98 min (Heck et al. 1994), respectively. The latter results are in line with the value of τ determined for MLSS III (Fig. 1). The τ values for MLSS I and II were higher than expected. These differences appear to be a consequence of the BLCSS definitions used. Previously, the kinetics of BLCSS were analyzed by restricting the change of BLC during the 10th and 30th min of constant-workload exercise to maximal increases and decreases of 0.1 mmol·l-1, respectively. This is less than the maximal increase of the BLC defined as a MLSS condition by the same research group (Heck 1990; Heck et al. 1985). At levels of BLCSS between 4.0 and 5.0 mmol·l-1 a change of 0.1 mmol·l-1 corresponds to a magnitude of 2.0–2.5% of BLCSS. Thus, in the previous studies on BLC kinetics, it was reported that at least 97% of the final BLCSS was attained after 10 min. The chosen pharmacokinetic model calculates that 95% of the BLCSS was reached after a period of 3τ. Consequently, based on the selected tests in those previous studies (Heck 1990; Heck et al. 1994), values of τ that were higher than approximately 3.3 min could not be detected.
At MLSS I, the increases in BLC between the 10th and 30th min of the constant-load test were 0.4 (0.5) mmol·l-1. The BLC did not change during the final 5 min of the MLSS I workload, proving a BLCSS. Approximately 92% of the final BLCSS was, or can be assumed to be reached after the initial 10 min (Fig. 1). The τ value corresponding to MLSS I led to a BLCSS after 17–20 min with an increase of BLC of approximately 0.2 mmol·l-1 and, therefore, if a testing protocol of 20 min of constant-workload exercise had been used, the BLC would have increased more or less until termination of the test. Consequently, the slight difference in the level of MLSS I and MLSS II appearing at nearly the same workload may be explained by the fact that MLSS I was calculated by averaging the BLC values measured at the 15th, 20th, 25th, and 30th min, whereas MLSS II was an average of the values of the 15th and 20th min. Both methods, MLSS I and MLSS II, and therefore procedure nos. 2–5, 8, 9, 12, and 13 (Table 1) appear to provide reasonable results of MLSS workload. The definition of a maximal increase of the BLC after the 10th min of constant-workload exercise of no more than 1.0 mmol·l-1 based on constant workloads lasting 30 min and possibly longer, seem to provide the best test results of MLSS and MLSS workload. Consequently, MLSS III and procedure nos. 1, 7, 10, and 14 (Table 1) obviously do not consider the time course of changes in BLC sufficiently and they are not suitable for detecting the MLSS.
A limitation of the present study is that it remains unknown whether MLSS I really determined the highest BLC above which a clearly identifiable increase of BLC can be observed during prolonged constant-workload exercise, because in the present study all tests were terminated after 30 min. However, further arguments seem to support the meaningfulness of MLSS I and comparable procedures. Only 73% of the subjects were able to sustain a complete 30-min constant-load test at a workload above MLSS I intensity. During these tests, the time course of changes in BLC did not indicate a steady state. After the initial 10 min, the BLC increased more or less linearly until test termination (Fig. 3).
In conclusion, the present study showed that numerous methods adopted for the determination of MLSS have not adequately considered the kinetics of the BLC during prolonged constant-workload testing. Due to insufficient test durations and negligence of the delayed adaptation of the BLC to a given constant workload, they detect levels of BLC significantly lower than that of the MLSS. Based on the present findings, constant-load tests lasting at least 30 min, and a BLC increase of no more than 1.0 mmol·l-1 after the 10th testing minute appear to be the most reasonable with respect to valid testing results.
References
Aunola S, Rusko H (1992) Does anaerobic threshold correlate with maximal lactate steady-state? J Sports Sci 10:309–323
Beneke R (1995) Anaerobic threshold, individual anaerobic threshold, and maximal lactate steady-state in rowing. Med Sci Sports Exerc 27:863–867
Beneke R, von Duvillard SP (1996) Determination of maximal lactate steady-state response in selected sports events. Med Sci Sports Exerc 28:241–246
Beneke R, Boldt F, Richter TH, Kress A, Leithäuser R, Behn C (1994) Laktatmessung in der Sportmedizin—drei Geräte im Vergleich. Dtsch Z Sportmed 45:60–69
Beneke R, Schwarz V, Leithäuser R, Hütler M, von Duvillard SP (1996) Maximal lactate steady-state in children. Ped Exerc Sci 8:328–336
Billat V, Dalmay F, Antonini MT, Chassain AP (1994) A method for determining the maximal steady state of blood lactate concentration from two levels of submaximal exercise. Eur J Appl Physiol 69:196–202
Dost FH (1968) Grundlagen der Pharmakokinetik. Georg Thieme Verlag, Stuttgart, pp 29–62
Haverty M, Kenney WL, Hodgson JL (1988) Lactate and gas exchange responses to incremental and steady state running. Br J Sports Med 22:51–54
Heck H (1990) Laktat in der Leistungsdiagnostik. Wissenschaftliche Schriftenreihe des deutschen Sportbundes. Verlag Karl Hofmann, Schorndorf
Heck H, Mader A, Hess G, Mücke S, Müller R, Hollmann W (1985) Justification of the 4-mmol/l lactate threshold. Int J Sports Med 6:117–130
Heck H, von Rosen I, Rosskopf P (1994) Dynamik des Blutlaktats bei konstanter Fahrrad- und Drehkurbelarbeit. In: Liesen H, Weiß M, Baum M (eds) Regulations- und Repairmechanismen. Dt Ärzte-Verlag, Köln, pp 187–190
Mader A, Heck H (1986) A theory of the metabolic origin of "anaerobic threshold". Int J Sports Med 7[Suppl 1]:45–65
Mocellin R, Heusgen M, Korsten-Reck U (1990) Maximal steady-state blood lactate levels in 11-year-old-boys. Eur J Pediatr 149:771–773
Stockhausen W, Huber G, Maier JB, Tinsel J, Keul J (1995) Ein einzeitiges Verfahren zur Bestimmung des maximalen Laktat-Steady-State auf dem Fahrradergometer. Dtsch Z Sportmed 46:291–302
Urhausen A, Coen B, Weiler B, Kindermann W (1993) Individual anaerobic threshold and maximum lactate steady-state. Int J Sports Med 14:134–139
Williams JR, Armstrong N (1991) Relationship of maximal lactate steady-state to performance at fixed blood lactate reference values in children. Ped Exerc Sci 3:333–341
Acknowledgements
The author gratefully extends his gratitude to Mrs. R. M. Leithäuser for her careful review of this manuscript and stimulating discussion. Thanks are also extended to all subjects who participated in this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Beneke, R. Methodological aspects of maximal lactate steady state—implications for performance testing. Eur J Appl Physiol 89, 95–99 (2003). https://doi.org/10.1007/s00421-002-0783-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-002-0783-1