
Abstract
Purpose
Randomized controlled trials (RCTs) of interventions aimed at reducing work-related stress indicate that cognitive behavioural therapy (CBT) is more effective than other interventions. However, definitions of study populations are often unclear and there is a lack of interventions targeting both the individual and the workplace. The aim of this study was to determine whether a stress management intervention combining individual CBT and a workplace focus is superior to no treatment in the reduction of perceived stress and stress symptoms and time to lasting return to work (RTW) in a clinical sample.
Methods
Patients with work-related stress reactions or adjustment disorders were randomly assigned to an intervention group (n = 57, 84.2% female) or a control group (n = 80, 83.8% female). Subjects were followed via questionnaires and register data. The intervention contained individual CBT and the offer of a workplace meeting. We examined intervention effects by analysing group differences in score changes on the Perceived Stress Scale (PSS-10) and the General Health Questionnaire (GHQ-30). We also tested if intervention led to faster lasting RTW.
Results
Mean baseline values of PSS were 24.79 in the intervention group and 23.26 in the control group while the corresponding values for GHQ were 21.3 and 20.27, respectively. There was a significant effect of time. 10 months after baseline, both groups reported less perceived stress and improved mental health. 4 months after baseline, we found significant treatment effects for both perceived stress and mental health. The difference in mean change in PSS after 4 months was − 3.09 (− 5.47, − 0.72), while for GHQ it was − 3.91 (− 7.15, − 0.68). There were no group differences in RTW.
Conclusions
The intervention led to faster reductions in perceived stress and stress symptoms amongst patients with work-related stress reactions and adjustment disorders. 6 months after the intervention ended there were no longer differences between the groups.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Departments of occupational medicine in Denmark have seen a rise in referrals of patients with work-related stress and adjustment disorders (Rohde 2006). The number of cases of mental disorder reported to the National Board of Industrial Injuries in Denmark in 2011 was 38% higher than in 2005 and constitutes one of the largest diagnostic groups along with neck and shoulder complaints and skin diseases (National Board of Industrial Injuries in Denmark 2012). Work-related stress is also related to an increased risk of long term sick-leave (Lund et al. 2005). Adjustment disorders are amongst the most frequent causes of sick-leave due to mental health problems (Koopmans et al. 2011; Nielsen et al. 2010). In Denmark, 19% of a cohort on sick-leave due to stress and burnout had not returned to work within 40 weeks (Nielsen et al. 2011). There is not a sufficient basis for a reliable estimate of the extent of mental health problems in Denmark, but one assessment suggests that the yearly costs of mental health problems is around 7.5 billion Euros (Borg et al. 2010). This figure refers to the combined costs to society including indirect costs such as reduced productivity, sickness absence, disability pensions, as well as direct costs incurred by the health system, which the authors state make up 10% of the total. However, indirect costs related to presenteeism were not included. Presenteeism at work entails further substantial productivity loss costs (Vänni et al. 2017; Ströberg et al. 2017; Johns 2010). Both for the individual and from an economic perspective, there are many reasons for preventing and treating work-related stress conditions.
However, interventions with a well documented effect are rarely offered to these patients. At some departments of occupational medicine in Denmark psychological counselling is offered, while other clinics do not have this possibility. Only in recent years have randomized controlled trials of interventions aimed at work-related stress been carried out in Denmark (Willert et al. 2009, 2010, 2011; Netterstrøm et al. 2012).
The literature contains many empirical studies of stress intervention programs. Unfortunately the quality of these is far from consistent. Randomized controlled trials (RCT) are best able to answer the question of whether or not a given intervention has the desired effect. There are two quantitative meta-analyses that review RCT’s and other experimental designs (Van der Klink et al. 2001; Richardsen and Rothstein 2008). A general conclusion is that stress intervention programs are effective compared with no treatment, and that cognitive-behavioral treatments appear to be more effective than other treatments.
However, the existing literature is characterized by a number of methodological weaknesses. One of these concerns study samples. Given the number of RCT’s that have been conducted, the lack of studies using referred patients with a documented clinical need of treatment is surprising. Most studies are conducted with volunteers, typically selected from particular companies. It is often unclear if subjects under treatment actually experience stress and they are usually not on sick-leave. Only a few studies have selected subjects on the basis of high baseline stress levels. Most stress management interventions are secondary prevention programs that try to reduce stress symptoms before they lead to serious health problems (Richardsen and Rothstein 2008). Another weakness concerns type of intervention. Previous studies have tended to assess either interventions focusing on the individual or interventions focusing on the workplace, i.e. primary preventive programs, such as job redesign.
From a psychological perspective, stress is seen as a state arising from a transaction between the individual and the environment (Lazarus and Folkman 1984). As such, a focus on only the individual or the work environment, when intervening, can be expected to lead to sub-optimal results. The extent to which an individual will benefit from applying coping techniques newly acquired through CBT is likely to be conditional upon workplace factors, e.g. the amount of control the job allows. There is a need for “the development and controlled evaluation of interventions involving a combined individual and organizational focus” (Van der Klink et al. 2001, p 275). Munz et al. (2001) evaluated a stress intervention that combined individual and organizational elements, and report positive results. However, a RCT-design was not employed and volunteer subjects were used. Blonk et al. (2006) employed a RCT-design to examine a combined individual and workplace intervention amongst self-employed people rather than employees.
The present study involves a tertiary intervention containing both individual and organizational elements within the framework of a randomized controlled trial. Furthermore, subjects are patients routinely referred to the Department of Occupational Medicine in Herning who undergo a thorough clinical assessment prior to inclusion. Patients are on sick-leave at baseline due to work-related stress reactions and adjustment disorders.
The objective is to evaluate the effect of this intervention. We hypothesized that the intervention group would experience faster recovery (reduced self-perceived stress and a greater reduction in symptoms of poor mental health) compared with a control group. We also expected faster recovery in the intervention group to be linked to faster RTW.
Method and design
The study was designed as a prospective randomized controlled trial with a treatment group and a control group (trial number: ISRCTN11561502). Effect evaluation was undertaken on the basis of questionnaire data collected at baseline, after 4 months (end of treatment period) and 10 months after baseline. RTW was also assessed using national register data.
Recruitment of study sample
Patients were referred by their general practitioners when it was suspected that symptoms were related to work stress. Subjects were prospectively recruited amongst these routinely referred patients, thereby reducing problems associated with self-selection. A sample size of 120 (60 per group) was required to detect a group difference of ½ SD equal to 3 points on one of the outcome measures, the Perceived Stress Scale (see below). The calculation was based on the following: significance level = 95%, power = 80% and correlation coefficient between baseline and follow-up = 0.15. Recruitment occurred between September 2008 and January 2011. The recruitment period was longer than anticipated, due to more patients being excluded than expected.
Inclusion criteria for the trial were (1) a diagnosis of adjustment disorder or reaction to stress (ICD-10 code: F43.2–F43.9, but not post traumatic stress disorder) or mild depression (F32.0); (2) clinical assessment concluded that working conditions played a major role in symptom development; (3) currently employed at the workplace where stressful working conditions had occurred; (4) on sick-leave due to stress at time of recruitment.
Exclusion criteria were (1) resigned/fired from workplace prior to baseline or no intention to return; (2) continuous pre-baseline sick-leave > 4 months; (3) comorbidity of another psychiatric illness (e.g. moderate to severe depression); (4) substance abuse; (5) comorbidity of recently diagnosed chronic somatic disease; (6) pregnancy; (7) any form of disability pension.
Inclusion was not dependent upon employment sector or type of work-related stressors. Subjects were referred to the department because of stressful conditions that are typical for patients who are normally referred, e.g. interpersonal conflicts, bullying, high job demands and role ambiguity. Often there was a combination of such factors.
When it was apparent from written referrals that exclusion criteria were present the patient was excluded before clinical assessment. All patients selected for assessment were sent a baseline questionnaire to be filled in the week before clinical interview and informed consent was obtained. The clinical interview was conducted by a psychologist according to protocol.
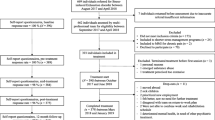
Subjects were randomly assigned to either the treatment or control group. The control group was hereafter only followed via questionnaires. The randomization procedure was carried out by a project secretary. Each subject was assigned the next 4-digit number on a list of true random numbers. If the sum of these digits was even, she entered the treatment group. If it was odd, she entered the control group. The secretary knew only that the patient was a study participant. The psychologist who conducted the clinical interview and assessed eligibility of participation was not able to influence the randomization procedure. Subjects in the treatment group received a letter with a date and time for their next appointment, the first of six treatment sessions, which was no later than 2 weeks after assessment. These individual sessions were conducted by the same psychologist who initially interviewed the patient. The selection process and information on dropout and exclusion is shown in Fig. 1.

Flowchart of patient recruitment
Intervention
The intervention, which is described in a manual (in Danish), contains two elements (1) 6 one hour sessions of individual CBT lasting a maximum of 4 months; (2) the offer of participation by the psychologist in a meeting between the patient and the employer aimed at discussing how the workplace could aid RTW and reduce stress levels.
Individual sessions focussed on how the patient interpreted and coped with stressful situations. Homework assignments were given between sessions. The program was developed specifically for use with patients with stress reactions and adjustment disorders in cooperation with experts in cognitive therapy. Several psychologists functioned as therapists. To ensure conformity to the manual they underwent a short training program and received external supervision. The program is standardised in that the manual specifies which CBT techniques may be used. Since symptoms, type of stressors and factors such as the extent of maladjusted cognition could vary greatly between patients, it was important that the therapist was able to fine-tune the program to the needs of the patient. The content of the sessions was, therefore, not identical for every patient. In each case the therapist could choose which techniques from the manual were relevant. In this way, treatment could take into account the particular context of the individual patient while remaining within the framework of the manual. To ensure adherence to the manual, the actual content of every treatment session was documented by indicating on a check list which techniques had been employed. The results of this process evaluation (not shown) revealed which CBT-techniques were most commonly used. Typically, early sessions involved psycho-education concerning the nature of stress and patients were introduced to a stress model, which forms the theoretical basis of the intervention. Constructing lists of problems and aims was also used early on to synchronize the expectations of the therapist and patient. Homework between early sessions usually entailed registering the occurrence of symptoms or problems. Intermediary sessions often included the analysis and restructuring of inappropriate thoughts and interpretations and working with the patient’s underlying assumptions. Later sessions included a focus on what the patient could do, once treatment was over, to prevent relapse.
The stress model on which the intervention is based is from Nielsen et al. (2008) (Fig. 2). It attempts to integrate a CBT approach to stress that focuses on the individual (right side of Fig. 2) with an organisational approach, which focusses on the psychosocial work environment (left side of Fig. 2). The model is process oriented. On the one hand there are psychological processes through which the person appraises and interprets events and situations at the workplace. If these appraisals are negative, e.g. involve threats of harm or loss, resulting physical discomfort and negative emotions will motivate actions, i.e. coping, attempts at reasserting a feeling of control or, if this fails, avoidance, that aim at reducing this discomfort. On the other hand, these psychological processes do not occur in a vacuum. They unfold within an organisational context, which means that others (managers, colleagues) can influence the same situations. Thus, the individual is a part of social and organisational processes that she only has limited control over. The extent to which the individual employee and other members of a work team or department have similar or divergent views concerning situations that the employee experiences as stressful is central to the intervention strategy. During the individual sessions time is also spent focusing on the dialogue between employee and workplace, on potential communication problems, and on ways of promoting a shared understanding of how stress arises and can be dealt with. The second part of the intervention has a more direct focus on this aspect.

Cognitive-organisational model of stress
Patients were told that the psychologist could take part in a meeting between the patient and employer. Such meetings were held with 25% of the patients in the intervention group. In the remaining cases, patients were advised on issues to discuss with their immediate supervisor. In these cases the psychologist aimed at influencing the workplace indirectly via the patient, who was encouraged to discuss specific problems, identified during initial clinical assessment and subsequent sessions, with her leader. When the psychologist did not participate in these meetings, it was usually because the patient preferred to take the meeting alone. The intervention program allowed for an extra session with the patient to prepare for the workplace meeting.
The meeting focussed on how stressful working conditions could be changed, either temporarily or permanently. Temporary changes were often agreed upon in connection with a period of part-time sick-leave, where work was gradually resumed over a couple of months with work hours and task complexity increasing week for week until sick-leave termination. The meeting aimed at initiating a process through which stressors were reduced; role ambiguity was clarified, poor working relationships were improved, or the patient’s influence over work tasks increased, dependent on the particular problems faced by the patient. The psychologist acted as mediator, attempting to improve mutual understanding between the two parties. The psychologist advised the workplace regarding what it could do to aid RTW. Discussions could concern the patient being transferred to a different work team, if other solutions to interpersonal conflicts could not be found, or which tasks could be given to colleagues in cases of work overload. In most cases of graded RTW a written plan of action was agreed upon.
Outcome measures
Stress level was measured with Cohen’s Perceived Stress Scale (PSS-10) (Cohen et al. 1983; Cohen and Williamsen 1988), while mental health was measured with the General Health Questionnaire (GHQ-30) (Goldberg and Williams 1988).
PSS-10 measures the extent to which a person feels life is stressful, unpredictable and uncontrollable. The 10 items have 5 response categories from 0 to 4. Item responses are summed giving a total score ranging from 0 to 40. Higher scores indicate higher levels of perceived stress. Cronbach’s alpha in the present study was 0.83.
GHQ-30 has often been used in epidemiological research and intervention studies. The 30 items have 4 response categories that are subsequently dichotomized, giving a total score from 0 to 30. Higher scores indicate poorer mental well-being. Cronbach’s alpha was 0.90.
RTW was based on data from the Danish Register for Evaluation of Marginalisation (DREAM). DREAM contains information on all public transfer payments administered by Danish ministries and municipalities for all citizens since 1991 on a weekly basis, including sick-leave. Lasting RTW was defined as full-time resumption of work (or equivalent) for 4 consecutive weeks.
Other measures
Age and gender were derived from civil registration numbers linked to DREAM, where data on number of weeks of sick leave the previous year prior to baseline was also obtained. Participants indicated in the baseline questionnaire if they were on full or part time sick leave as well as their level of education, medication and occupation. Occupation was divided into two groups in the adjusted analyses of RTW; health, social services and childcare in one group, all others in the other group. Diagnoses were obtained from initial clinical assessment.
Analysis strategy
Baseline characteristics in the two groups were compared with chi-squared test of comparable distributions, Student’s t test and the Mann–Whitney U test. Analyses of intervention effects (PSS-10 and GHQ-30) were performed by multivariate repeated measurements analysis. Because of some missing values, especially at 4 and 10 months follow-up, a mixed model was used, which allow all data to be included. When individual items in a scale were missing, single mean imputation was used. The imputed value was calculated on the basis of the mean of the other items in the scale for the individual subject. Single imputation was only used if at least half the scale items had been answered. Model validation was conducted using QQ-plots by group of residuals versus predicted values and residual probability plots.
To compare changes over time for the two self-reported outcomes, effect size was estimated using Cohen’s d (Cohen 1988). We have presented Cohen’s d as negative numbers, which reflects a reduction in perceived stress or GHQ-symptoms.
To test the robustness of the results with regard to psychological outcomes considering loss to follow-up, we conducted a number of sensitivity analyses with imputation of missing data on the perceived stress scale according to the last score carried forward at 4 and 10 months follow-up, realistic improvements over time and realistic worsening over time.
RTW was analysed with cox regression. Time to RTW was defined as the period from the clinical interview to the first week of four in a row with no transfer income (or equivalent, i.e. education). RTW was visualised by a Kaplan-Meyer Plot using the cumulative number of weeks of sick-leave in the 44 weeks from inclusion. Group differences were analysed with Cox regression. We adjusted for gender, age, part time/full time sick leave, occupation, number of weeks on sick leave the previous year before inclusion and diagnosis at baseline. Model validation of the proportional hazards assumption was conducted by performing a log–log plot of the survival curves as well as the proportional hazards test.
It can be seen in Table 1 that a single subject was not on sick-leave at baseline. It was discovered during data analysis that this person had been on sick-leave but had just resumed work when entering the study. The person was comparable to other participants with regards to baseline scores on outcome measures and satisfied all other inclusion criteria. This subject completed the intervention and all questionnaires and was included in the analyses, except from the analysis of RTW where this patient and two others were excluded, as they did not have a registration of sick leave in the DREAM register, probably because their employer had not claimed compensation.
Statistical analyses were performed using STATA (STATA Corp. Lp, College station, TX) software package 11.2 and 13.1.
Results
Table 1 shows demographic characteristics of the two groups at baseline. There are relatively many female employees from the public sector (nurses, nursing assistants, teachers), which reflects the usual trend in referrals to the department. There were no significant differences in demographics between the groups.
Changes in PSS and GHQ scores over time are shown in Figs. 3 and 4, respectively. In each case, subjects in both groups improved during 10 months of follow-up. Reductions in symptoms and perceived stress occurred faster during the first 4 months.

Changes in perceived stress from baseline to 4 and 10 months follow-up

Changes in mental health from baseline to 4 and 10 months follow-up
Table 2 shows the crude analyses of changes in PSS and GHQ from baseline to 4 months follow-up in both groups. Tables 3 and 4 depict the corresponding analyses of changes from 4 to 10 months and from baseline to 10 months, respectively.
At 10 months follow-up both groups experience fewer symptoms and less perceived stress compared to baseline. In both groups there is a large and significant effect of time (Table 4).
In the crude analyses, a moderate intervention effect was found in the period from baseline to 4 months follow-up for both PSS and GHQ (Table 2). A significantly greater improvement in perceived stress and mental health was seen in the intervention group than in the control group. In both cases Cohen’s d indicated a moderate treatment effect.
From 4 to 10 months after baseline (Table 3) there is a stronger effect of time in the control group compared with the intervention group, perhaps because there now is less room for further improvement in the intervention group. In the intervention group, there is no effect of time from 4 to 10 months on PSS while there is for the control group. GHQ scores continue to improve in both groups between 4 and 10 months after baseline, but the improvement in this period is more marked for the control group.
A number of sensitivity analyses were conducted to test the robustness of the results. Imputation of values that were missing according to different scenarios of last score carried forward, worsening or improving, respectively, did not change the results.
When adjusting for the baseline value of the outcome, the treatment effects at 4 months follow-up were reduced to small effect sizes. For PSS10 the difference in mean change = − 2.18, 95% CI − 4.34 to − 0.03, P = 0.047 and Cohen’s d = − 0.36, 95% CI − 0.71 to − 0.004. For GHQ30 the difference in mean change = − 2.97, 95% CI − 5.69 to − 0.24, P = 0.033 and Cohen’s d = − 0.37, 95% CI − 0.78 to − 0.03. The overall results at 10 months follow-up were not changed by adjusting for baseline levels of outcome measures.
There were no between group differences in sick-leave duration (se Fig. 5). At 44 weeks after baseline the HR for lasting RTW for the intervention group was 0.84 (P = 0.372, 95% CI 0.56–1.24). Adjustment for potential confounders did not change the estimates (HR = 0.81, P = 0.285, 95% CI 0.54–1.20).

Sick-leave termination
Discussion
Our results indicate that patients with work-related stress reactions and adjustment disorders generally experience improvements during sick-leave. The time effect is not surprising since most adjustment disorders are expected to last under 6 months according to ICD-10 diagnostic criteria (ICD-10 Classification of Mental and Behavioural Disorders 1992). Indeed, this substantial natural recovery has been named as a factor that may hinder the detection of treatment effects (De Vente et al. 2008). Nevertheless, our results also show that participants in the intervention group recovered significantly faster. After a 4 month treatment period, the intervention group reported fewer symptoms of poor mental health and lower levels of perceived stress.
Despite this faster recovery in the intervention group, there was no group difference in terms of RTW. Research on interventions aimed at facilitating RTW in adults with adjustment disorders has generally not been successful at demonstrating positive effects (Arends et al. 2012). A couple of exceptions exist. In a RCT study by Blonk et al (2006), subjects who received a combination of individual CBT and a workplace intervention attained full work resumption faster than a control group, despite the absence of treatment effects on measures of psychological complaints. This result may reflect that all participants were self-employed, since company owners are likely to have more influence over working conditions and the structuring of graded RTW than employees. Using a cluster randomized controlled design, Van der Klink et al. (2003) report faster RTW for sick-listed employees from a Dutch company following intervention based on CBT and contact to the workplace compared to care as usual. Again this was despite a lack of a treatment effect in terms of psychological well-being. It is unclear if adjustment disorders in this study were work-related. Two reviews of intervention studies that aim at reducing symptoms and facilitating RTW in patients with burnout have recently been conducted. Ahola et al. (2017) included 14 studies reporting the effects of 18 interventions and find mixed results. Burnout symptoms were not systematically alleviated by individually-focussed interventions, while studies evaluating the effect of combined interventions and the effects of interventions on RTW were too few in number to draw conclusions. They also conclude that burnout is not a stable condition, but diminishes in time in most cases. Perski et al. (2017) performed meta-analyses when reviewing 8 tertiary interventions in clinical burnout and report a significant effect in comparison with control conditions regarding days until RTW. They suggest, however, that interpretation should be cautious because of significant heterogeneity. No intervention effects were found regarding full RTW. Intervention effects concerning symptoms were not found. They find some support for suggesting that combined interventions that enable a workplace dialogue with employers are more successful in facilitating RTW. This is in line with research on interventions with employees on sick-leave with back pain, where it has been found that workplace involvement improves RTW rates (Carroll et al. 2010). Research on burnout interventions would benefit from consensus on the definition and assessment of burnout (Ahola et al. 2017). Indeed, the question of whether or not burnout is a distinct phenomenon or a form of depression is controversial and empirical evidence for the distinctiveness of burnout is inconsistent (Bianchi et al. 2015). In the present study, patients diagnosed with moderate to severe depression during clinical assessment were excluded, as were more chronic cases of stress (sickleave > 4 months). Many but not all of the studies reviewed by Perski et al. (2017) appear to have similarly excluded depressive patients and are, therefore, comparable to our study.
When faster improvements in mental health do not translate into faster RTW, it is probably because RTW is a more complex phenomenon than previously assumed. RTW is likely to reflect the combined influences of many factors and not just improved mental state. For example, a prospective study in Sweden has found that both organisational and individual factors influence RTW and that gender differences exist (Holmgren et al. 2013). These authors found that a combination of a good organizational climate and higher individual levels of work commitment predicts faster RTW, but only for women. Participants in this Swedish cohort were on sick-leave for different reasons, both physical and psychological, but the authors point out that organizational climate and work commitment are affected by stressful working conditions. It appears likely that organizational climate and work commitment will play an even bigger role for persons on sick-leave because of work related stress. Even after clear improvements in stress symptoms have occurred, the individual may be reticent about returning to work if, for example, there is a poor social climate or conflicts in the workplace, which may trigger worries about relapse in the event of returning too soon. A Dutch study has also demonstrated that complaint reduction in connection with recovery from work related stress and RTW are two relatively independent processes (De Vente et al. 2015).
Our results are somewhat in line with previous Danish studies (Willert et al. 2009, 2010, 2011; Netterstrøm et al. 2012) and reviews of the international literature (Van der Klink et al. 2001; Richardsen and Rothstein 2008). As noted earlier though, many of the previous RCT’s have evaluated secondary interventions. Results concerning tertiary interventions have been more mixed (Arends et al. 2012; Ahola et al. 2017; Perski et al. 2017). Some demonstrate treatment effects on psychological outcomes (Willert et al. 2009; Netterstrøm et al. 2012), while others do not (De Vente et al. 2008; Blonk et al. 2006; Van der Klink et al. 2003; Huibers et al. 2004). It appears that treatment effects with regard to psychological well-being have been more forthcoming when wait-list control groups have been used; while negative results have been found in studies using no-treatment or care as usual control groups. A meta-analysis of 49 RCT’s evaluating psychotherapy has found that the effect size estimates for CBT were substantially different depending on the control condition (Furukaxa et al. 2014). These authors suggest that waiting list control groups may act as a ‘nocebo’ condition that perhaps delays recovery by creating expectations of later improvements once the waited for intervention takes place. It should be noted that a wait-list control group was not used in the present study.
Another possible reason for mixed results could be between study differences in how samples are defined and selected. Stress patients can differ widely both in terms of symptoms and type of stressors, e.g. work overload or bullying. A recent study identified several predictors of faster recovery from work-related stress (De Vente et al. 2015), e.g. male gender, less working hours, more co-worker support. We have tested the current intervention in a separate RCT design using the same inclusion and exclusion criteria (Dalgaard et al. 2017). In this case, however, the intervention group returned to work 4 weeks faster than the control group, while no significant intervention effect was found for PSS or GHQ. While we do not have a clear answer as to why results are different, a likely possibility is differences in participant selection. Participants in the present study were referred by general practitioners. Dalgaard et al. (2017) selected participants from the sickness benefit departments of local municipalities, which in practice meant they had been on sick leave longer than participants in the present study, giving them a longer period of recovery prior to entry into the study. It is possible that the timing of intervention is important, i.e. that early intervention can facilitate symptom reduction, but more time is needed before patients can benefit from help concerning graded RTW (e.g. sufficient reductions in exhaustion or improvements in cognitive capacity are needed). This creates a challenge for researchers since it is often not possible to identify the precise onset of a stress condition and people vary in terms of how long they wait before choosing sick leave. More research is needed to identify predictors of the recovery process and possible moderators of treatment effects.
In a previous article (Dalgaard et al. 2014), we presented results from our study where quality of sleep and cognitive deficits were employed as outcomes. While there was a tendency towards improved quality of sleep and less distraction in the intervention group, differences between groups at 4 and 10 months did not reach statistical significance. Measures of general mental health and perceived stress are probably more likely to capture treatment effects given that specific symptoms vary greatly among patients with adjustment disorders, and selection into the study was not based on particular symptoms. In addition, our intervention did not focus explicitly on sleeping difficulties or cognitive deficits.
Our intervention combined individual and organisational elements. When treating work-related stress reactions, it makes sense, both clinically and theoretically, to target both sides of the person–environment interaction that has presumably contributed to symptom development. Individuals vary greatly with regard to what they find stressful, and organisations vary greatly with regard to what types of stressors they contain. The intervention under study here built upon a thorough assessment of each patient that provided information concerning how both person-related and work environment factors combined over time to create situations that were particularly stressful for the individual concerned. This information led to hypotheses that could be worked with during the therapeutic sessions and the workplace meetings. We also believe that involving the workplace, when possible, is desirable for ethical reasons. Relapse is presumably more likely if patients return to unchanged working conditions. Involving the workplace may also increase management awareness of stressors, and thus benefit co-workers.
On the other hand, involving the workplace presents many challenges. Physicians and psychologists from hospital departments of occupational medicine in Denmark have no powers to enforce recommendations upon a workplace. Thus, persuading employers to accept advice requires diplomatic skills and good arguments. While we have no data on the matter, it was our experience that the relationship between employee and immediate supervisor plays an important role. It is likely that we were more easily able to gain access to a workplace when the patient had a positive and trusting relationship with management. It was nevertheless also our experience that our focus on the workplace furthered an improved dialogue between employee and employer and a shared understanding of stressful working conditions.
The present study has both strengths and weaknesses. Its main strength is the RCT-design, which greatly increases confidence in the conclusion that it is the intervention alone that explains post intervention between group differences. As far as we are aware it is the first RCT of a tertiary cognitive-behavioural program in combination with a focus on changing stressful work conditions amongst employees with work-related adjustment disorders. Furthermore, a diagnostically well defined study population was used with a clear clinical need of intervention—patients on sick-leave with work-related stress reactions and adjustment disorders routinely referred to a department of occupational medicine. This reduces the risk of selection bias. Another strength is the use of register data in the analyses of RTW, since reporting bias is not present and loss to follow-up was minimal.
Some limitations also need to be mentioned. We aimed at using a true no-treatment control group. This may be seen as a strength in comparison with a waiting-list control group, as mentioned above. However, patients in our control group were free to seek treatment elsewhere, which many did. In the control group 41% received some help outside of the study from psychologists. This may have impacted on the study’s ability to uncover a treatment effect. If this was the case, it is more likely that our results underestimate rather than overestimate any intervention effects. On the other hand, patients’ opportunity to seek treatment elsewhere reflects the daily clinical reality, so our control group might better be viewed as a ‘care as usual’ group. This strengthens the study’s external validity. At 4 months there were no between group differences regarding medication.
Another limitation is the greater drop-out rate observed in the control group. This probably reflects a reduced motivation to continue participation amongst some of those selected into the control group. No differences were found between dropouts and non-dropouts at 4 months follow-up on either demographic variables or baseline values of outcome measures. However, at 10 months follow-up non-responders were younger; less educated and contained more men compared to responders. Nonetheless, sensitivity analyses accounting for different scenarios of symptom development among non-responders did not alter the results. It is, therefore, unlikely that the difference in drop-out has introduced systematic bias. The fact that more patients were allocated to the control group meant that the two groups were almost equal in size at the end of the study. It was coincidental that more patients entered the control group. At the start of the project a list of true random numbers was generated, which was used in the randomisation procedure. However, the length of this list was not limited beforehand, which allowed one group to grow faster than the other. It was necessary to stop further intake before the groups had acquired equal size, because the inclusion period had already been prolonged. The stop date was chosen according to the expected point at which both groups would contain at least 60 participants.
The follow-up time of 6 months post intervention means that we are not able to assess if any intervention effects might appear later, e.g. subsequent differences in sickness absence. It is also possible that undetected treatment effects exist in sub-groups. Our sample is quite heterogeneous in terms of sex, age, type of work, types of stressors, part- or fulltime sick leave at baseline. Unfortunately, sub-groups are too small to allow separate analyses.
Since participants could not be blinded as to experimental condition, information bias due to desirable responding on self-report measures can not be completely ruled out.
Only sick leave spells of 3 weeks or more are included in DREAM, thus providing less sensitive measures of short-term absences. This is, however, not a problem in the present study since our participants were absent from work for considerably longer periods. It should also be noted that DREAM does not distinguish between part and full time sick leave, so we were unable to examine eventual group differences in returning to work on reduced hours.
We planned a combined intervention aimed both at the individual and the workplace. Unfortunately we were unable to conduct a direct intervention at most workplaces. In 14 cases (25%) the psychologist participated in a meeting with the patient’s immediate supervisor. In the remaining cases the workplace intervention occurred indirectly. The patient was advised about concrete conditions at work that needed to be addressed, including recommendations about temporary or permanent changes, and then encouraged to discuss these matters with management. This may have weakened the intended workplace intervention. The 4 month follow-up questionnaire contained items about actual changes at the workplace. In the intervention group 67% agreed temporary changes in working conditions with employers compared to 53% in the control group. Figures for permanent changes were similar. The most common changes in the intervention group involved reductions in workload, changes in working hours, transfers to other departments or teams, clearer role definitions and altered task priorities.
It is also a limitation that we cannot determine to what extent the effective element of the intervention is the psychological counselling, the workplace intervention, or their combination.
Regarding generalizability, our sample is comparable to those employed in other Danish studies (Willert et al. 2009; Netterstrom et al. 2012) and reflects the fact that publicly employed women, for unknown reasons, are more likely to be referred to clinics of occupational medicine than other demographic groups. The extent to which our findings are applicable to men in the private sector is not clear. It is also unclear to what extent the Danish context, with its specific legislation on sick-leave and where everyone has free access via their general practitioner to departments of occupational medicine, has influenced our results.
Conclusion
The work focussed cognitive intervention evaluated here led to a faster reduction of symptoms (GHQ) and self perceived stress (PSS), compared to a control group, amongst patients with work-related stress reactions and adjustment disorders referred to a hospital department of occupational medicine. However, 10 months after baseline there were no longer differences in symptoms or self-perceived stress between the groups, indicating a good rate of natural recovery in these patients. The intervention did not lead to faster RTW.
References
Ahola K, Toppinen-Tanner S, Seppänen J (2017) Interventions to alleviate burnout symptoms and to support return to work among employees with burnout: Systematic review and meta-analysis. Burnout Res 1:1–11
Arends I, Bruinvels DJ, Rebergen DS, Nieuwenhuijsen K, Madan I, Neumeyer-Gromen A, Bültmann U, Verbeek JH (2012) Interventions to facilitate return to work in adults with adjustment disorders. Cochrane database of Systematic Reviews 2012, Issue 12. Art. No. CD006389. https://doi.org/10.1002/14651858.CD006389.pub2
Bianchi R, Schonfeld IS, Laurent E (2015) Burnout-depression overlap: a review. Clin Psychol Rev 36:28–41
Blonk RWB, Brenninkmeijer V, Lagerveld SE, Houtman ILD (2006) Return to work: a comparison of two cognitive behavioural interventions in cases of work related psychological complaints among the self-employed. Work Stress 20(2):129–144
Borg V, Andersen Nexø M, Kolte IV, Friis Andersen M (2010) Hvidbog om mentalt helbred, sygefravær og tilbagevenden til arbejde (White paper on mental health, sickness absence and return to work). Det Nationale Forskningscenter for Arbejdsmiljø (Danish National Research Centre for the Working Environment), Copenhagen
Carroll C, Rick J, Pilgrim H, Cameron J, Hillage J (2010) Workplace involvement improves return to work rates among employees with back pain on long-term sick leave: a systematic review of the effectiveness and cost-effectiveness of interventions. Disabil Rehabil 32(8):607–621
Cohen J (1988) Statistical power analysis for the behavioral sciences. Lawrence Earlbaum Associates, Hillsdale
Cohen S, Williamsen G (1988) Perceived stress in a probability sample of the United States. In: Spacapan S, Oskamp S (eds) The social psychology of health. Sage, Newbury Park
Cohen S, Kamarck T, Mermelstein RA (1983) A global measure of perceived stress. J Health Soc Behav, 24:385–396
Dalgaard L, Eskildsen A, Carstensen O, Willert MV, Andersen JH, Glasscock DJ (2014) Changes in self-reported sleep and cognitive failures: a randomized controlled trial of a stress management intervention. Scand J Work Environ Health 40(6):569–581
Dalgaard VL, Aschbacher K, Andersen JH, Glasscock DJ, Willert MV, Carstensen O, Biering K (2017) Return to work after work-related stress: a randomized controlled trial of a work-focussed cognitive behavioural intervention. Scand J Work Environ Health 43(5):436–446
De Vente W, Kamphuis JH, Emmelkamp PMG, Blonk RWB (2008) Individual and group cognitive behavioural treatment for work-related stress complaints and sickness absence: a randomized controlled trial. J Occup Health Psychol 13(3):214–231
De Vente W, Kamphuis JH, Blonk RWB, Emmelkamp PMG (2015) Recovery of work-related stress: complaint reduction and work-resumption are relatively independent processes. J Occup rehabil 25:658–668
Furukaxa TA, Noma H, Caldwell DM, Honyashiki M, Shinohara K, Imai H, Chen P, Hunot V, Churchill R (2014) Waiting list may be a nocebo condition in psychotherapy trials: a contribution from network meta-analysis. Acta Psychiatr scand 130:181–192
Goldberg DP, Williams P (1988) A user’s guide to the general health questionnaire. NFER-Nelson, Windsor
Holmgren K, Ekbladh E, Hensing G, Dellve L (2013) The combination of work organizational climate and individual work commitment predicts return to work in women but not in men. J Occup Med 55(2):121–127
Huibers MJH, Beurskens AJHM., van Schayck CP, Bazelmans E, Metsemakers JFM, Knottnerus JA, Bleijenberg G (2004) Efficacy of cognitive-behavioural therapy by general practitioners for unexplained fatigue among employees. Br J Psychiatry 184:240–246
ICD-10 Classification of Mental and Behavioural Disorders. Clinical Descriptions and Diagnostic Guidelines (1992) Geneva: WHO
Johns G (2010) Presenteeism in the workplace: a review and research agenda. J Organ Behav 31(4):519–542
Koopmans PC, Bultmann U, Roelen CA, Hoedeman R, van der Klink JJ, Groothoff JW (2011) Recurrence of sickness absence due to common mental disorders. Int Arch Occup Environ Health 84(2):193–201
Lazarus RS, Folkman S (1984) Stress, appraisal and coping. Springer, New York
Lund T, Labriola M, Christensen KB, Bültmann U, Villadsen E, Burr H (2005) Psychosocial work environment exposures as risk factors for long-term sickness absence among Danish employees: results from DWECS/DREAM. J Occup Environ Med 47(11):1141–1147
Munz DC, Kohler JM, Greenberg CI (2001) Effectiveness of a comprehensive worksite stress management program: combining organizational and individual interventions. Int J Stress Manag 8(1):49–62
National Board of Industrial Injuries in Denmark (Arbejdsskadestyrelsen) (2012) Arbejdsskadestatistik 2011 (Industrial Injuries Statistics 2011) (www.ask.dk)
Netterstrøm B, Friebel L, Ladegaard Y (2012) The effects of a group based stress treatment program (the Kalmia concept) targeting stress reduction and return to work. A randomized, wait-list controlled trial. J Environ Occup Sci 1(1):111–120
Nielsen K, Rasmussen K, Carstensen O, Glasscock D (2008) Forandring som vilkår (Change as a permanent condition). Børsens Forlag, Copenhagen
Nielsen MB, Bultmann U, Amby M, Christensen U, Diderichsen F, Rugulies R (2010) Return to work among employees with common mental disorders: Study design and baseline findings from a mixed-method follow-up study. Scand J Public Health 38(8):864–872
Nielsen MB, Madsen IE, Bultmann U, Christensen U, Diderichsen F, Rugulies R (2011) Predictors of return to work in employees sick-listed with mental health problems: findings from a longitudinal study. Eur J Pub Health 21(6):806–811
Perski O, Grossi G, perski A, Niemi M (2017) A systematic review and meta-analysis of tertiary interventions in clinical burnout. Scand J Psychol 58:551–561
Richardsen KM, Rothstein HR (2008) Effects of occupational stress management intervention programs: a metaanalysis. J Occup Health Psychol 13:69–93
Rohde B (2006) Mange flere patienter har psykiske belastningsreaktioner (Many more patients with reactions to stress). Arbejdsmiljø 3-2006:9–10
Strömberg C, Aboagye E, Hagberg J, Bergström G, Lohela-Karlsson M (2017) Estimating the effect and economic impact of absenteeism, presenteeism, and work environment-related problems on reductions in productivity from a managerial perspective. Value Health 20:1058–1064
Van der Klink JL, Blonk RWB, Schene AH, van Dijk FJH (2001) The benefits of interventions for work-related stress. Am J Public Health 91(2):270–276
Van der Klink JJL, Blonk RWB, Schene AH, Van Dijk FJH (2003) Reducing long term sickness absence by an activating intervention in adjustment disorders: a cluster randomised controlled design. Occup Environ Med 60:429–437
Vänni K, Neupane S, Nygård CH (2017) An effort to assess the relation between productivity loss costs and presenteeism at work. Int J Occup Saf Ergon 23(1):33–43
Willert MV, Thulstrup AM, Hertz J, Bonde JP (2009) Changes in stress and coping from a randomized controlled trial of a three-month stress management intervention. Scand J Work Environ Health 35(2):145–152
Willert MV, Thulstrup AM, Hertz J, Bonde JP (2010) Sleep and cognitive failures improved by a three-month stress management intervention. Int J Stress Manag 17(3):193–213
Willert MV, Thulstrup AM, Bonde JP (2011) Effects of a stress management intervention on absenteeism and return to work—results from a randomized wait-list controlled trial. Scand J Work Environ Health 37(3):186–195
Acknowledgements
This research project was supported by a grant from the Danish Working Environment Research Fund (Grant No. 34-2007-03).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Glasscock, D.J., Carstensen, O. & Dalgaard, V.L. Recovery from work-related stress: a randomized controlled trial of a stress management intervention in a clinical sample. Int Arch Occup Environ Health 91, 675–687 (2018). https://doi.org/10.1007/s00420-018-1314-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-018-1314-7