
Abstract
Purpose
Although individual studies have reported high prevalence of musculoskeletal symptoms (MSS) among construction workers, no systematic review has summarized their prevalence rates. Accordingly, this systematic review/meta-analysis aimed to synthesize MSS prevalence in different construction trades, gender and age groups, which may help develop specific ergonomic interventions.
Methods
Nine databases were searched for articles related to the research objective. Two reviewers independently screened citations, extracted information and conducted quality assessment of the included studies. Meta-analyses were conducted on clinical and statistical homogenous data.
Results
Thirty-five out of 1130 potential citations were included reporting diverse types of period prevalence and case definitions. Only the 1-year prevalence rates of MSS (defined as at least one episode of pain/MSS in the last year) at nine anatomical regions had sufficient homogeneous data for meta-analysis. Specifically, the 1-year prevalence of MSS was 51.1% for lower back, 37.2% for knee, 32.4% for shoulder, 30.4% for wrist, 24.4% for neck, 24.0% for ankle/foot, 20.3% for elbow, 19.8% for upper back, and 15.1% for hip/thigh. Female workers demonstrated a higher prevalence of MSS while there was insufficient information on the prevalence of trade-specific or age-related MSS. The quality assessments revealed that many included studies estimated prevalence solely based on self-reported data, and did not report non-respondents’ characteristics.
Conclusions
Lumbar, knee, shoulder, and wrist MSS are the most common symptoms among construction workers. Future studies should standardize the reporting of period prevalence of MSS in different construction trades to allow meta-analyses and to develop relevant MSS prevention program.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Musculoskeletal symptoms (MSS) are one of the most prevalent occupational health problems among construction workers (Inyang et al. 2012). Given the high physical work demand, prolonged awkward static/repetitive postures, whole-body vibration, long working hours, and unfavorable work environment (Buchholz et al. 1996; Forde and Buchholz 2004; Antwi-Afari et al. 2017; Umer et al. 2017a, b), construction workers are constantly exposed to multiple ergonomic risk factors. Consequently, work-related musculoskeletal symptoms are the main contributing factor to non-fatal injuries in the construction industry (Wang et al. 2015).
The high prevalence of work-related MSS not only causes work absenteeism, schedule delays and compensation claims but also heightens the recruitment/training costs of the construction industry (Inyang et al. 2012). Approximately 33.0% of the total absenteeism in the US construction industry in 2012 were attributed to MSS (BLS 2013). Similarly, The Alberta Construction Safety Association reported that 41.9% of all accepted lost time claims in 2008 were related to MSS (Inyang et al. 2012). In Germany, MSS is the major cause of occupational disabilities among construction workers (Arndt et al. 2005).
Although individual studies have reported prevalence rates of various MSS in numerous construction trades, no systematic review has summarized these findings. Without such information, it is difficult for relevant stakeholders (e.g. policymakers, project managers, and healthcare providers) to comprehend the scope of the problem and to allocate resources to develop/evaluate prevention or treatment strategies for musculoskeletal symptoms in various trades of the construction industry. Importantly, given the increased employments of females (Kinoshita and Guo 2015) and older workers (Samorodov 1999; Schwatka et al. 2012) in the construction industry, it is essential to critically appraise the evidence regarding the prevalence of MSS in construction workers of different genders or ages. This information can help develop specific management strategies (e.g. job modification) to reduce the risk of work-related MSS in vulnerable subgroups.
Given the above, the primary objective of this systematic review was to synthesize the prevalence of various MSS in the construction industry. The secondary objectives were to compare the prevalence of MSS: (1) among different construction trades (2) between male and female workers, and (3) among different age groups in the industry.
Methods
This systematic review protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO, Registration ID: CRD42016036051). The current review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines (Moher et al. 2009).
Literature search and study selection
Candidate publications were searched from nine databases from their inception to August 2016: Academic Premier (1990 +), CINAHL (1937 +), Health and Safety Science Abstract (1981 +), Medline (1965 +), PsycINFO (1806 +), Science Direct (1823 +), Scopus (1996 +), SportDiscus (1830 +) and Web of Science (1970 +). The search string included keywords, MeSH terms, and free-text words and consisted of three parts. The first part was related to prevalence or incidence. The second part encompassed the topic of MSS, while the third one covered construction trades. Since there were no universal list/definitions of the construction trades around the globe, the search string utilized both distinct trade names and general terms to amass all potential articles. Appendix A in Supplementary material illustrates the exact search strategy employed. Moreover, the corresponding authors of the included articles were contacted via email to identify additional articles.
Articles were included if they were primary studies published in peer-reviewed journals regarding the prevalence rates of MSS in one or more construction trades. There was no language restriction. Studies were excluded had they solely reported MSS related to infections, or accidents occurred at or outside worksites. Additionally, publications that did not directly or indirectly provide the prevalence rate of MSS (e.g. proportion of affected workers) were excluded. For multiple articles presenting the same data from a single cohort, only the one with the largest relevant data set was included.
Citations identified from the systematic searches were stored in EndNote X7 (Thomson Reuters, New York, USA) and duplicated citations were removed. Two reviewers (WU and MA) independently screened the titles and abstracts and selected the potential citations based on the selection criteria. Any disagreement was resolved by consensus. Those potential citations were then retrieved for full-text reading. The same screening procedures were adopted for full-text screening. Disagreements between the two reviewers were discussed to achieve consensus. Persistent disagreements were resolved by the third reviewer (AW). The reference lists of the included articles were searched for relevant citations. Forward citation tracking of the included articles was conducted using Scopus to identify relevant articles that were missed at the initial database searches.
Data extraction
The two reviewers independently extracted relevant data from the included articles. The extracted data included year of the publication, duration and location(s) of data collection, study design, involved trade(s), sample size, response rate, age and gender of the participants, case definition, types of period prevalence (e.g. point or 1-week), and data pertaining to the prevalence or frequencies of different MSS in the sample. Consensus meetings were held to resolve any discrepancies arising from data extraction.
Quality assessment
Both reviewers independently evaluated the quality of each included study using a tool developed by Loney et al. (1998). The tool (Appendix B in Supplementary material) has been used in many systematic reviews to evaluate the quality of primary incidence/prevalence studies (Graham et al. 2003; Fejer et al. 2006; Peppas et al. 2008; King et al. 2011; Kok et al. 2015). The tool consists of eight questions in three domains. The first six questions appraised the study methodology (i.e. study design and method, sampling frame, adequacy of the sample size, validity of the measurement tools, potential biases of the outcome measurement, and response rate and descriptions of non-respondents). The last two questions evaluated domains related to the results reporting quality and sociodemographic description of participants. Six of the eight questions in the tool score either 0 or 1 point each, while another two questions comprise two sub-questions. Each sub-question may score a maximum of 0.5 points. Accordingly, each study might score between 0 and 8. Studies with scores ≤ 4 were labeled as low quality, whereas studies with scores > 4 were considered as high quality (Wong et al. 2013; Kok et al. 2015). Discrepancies between reviewers were resolved by discussion.
Data synthesis
The 95% confidence interval of the prevalence rate in a given included study was estimated using Wald’s formula had it not been reported (Agresti and Coull 1998). Meta-analysis was planned for each type of period prevalence rate of a given MSS if the studies had an identical case definition. I-squared (I2) statistic was used to quantify the extent of statistical heterogeneity among the prevalence estimates. A random-effect model was used to estimate the period prevalence. Outliers were subjectively identified through scatterplots and were discarded from meta-analysis if the study quality was low (Hoy et al. 2012). RevMan 5.3 (The Cochrane Collaboration, Oxford, UK) was used for the meta-analysis. To minimize publication bias, comprehensive literature searches were conducted to ensure that relevant studies were included (Hoy et al. 2012).
Results
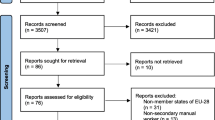
The searches identified 1130 citations (Fig. 1). Five hundred and twenty-eight citations were screened for titles and abstracts after duplicates’ removal. Among them, 484 were excluded as the titles and abstracts were unrelated to construction or MSS. Fifty-two articles were selected for full-text screening (including eight articles identified from forward citation tracking and reference lists of the included studies). Seventeen articles were excluded after reviewing the full text because they did not report prevalence data or had insufficient data for the prevalence estimation (e.g. injury/claim data without healthy workers’ statistics, or hospital reports). Therefore, 35 articles were included in this review (Table 1).

A flowchart depicting the systematic search
Study characteristics
Four types of study designs were observed in the included studies. Twenty-six studies were cross-sectional studies. One study was a repeated cross-sectional cohort study (Hoonakker and van Duivenbooden 2010). Four studies were case–control studies (Arndt et al. 1996; Rothenbacher et al. 1997; Ueno et al. 1999; Burström et al. 2013), and four were prospective cohort studies (Elders and Burdorf 2004; van der Molen et al. 2009; Boschman et al. 2012; Dong et al. 2012). The included studies comprised 303,384 construction workers in at least 19 different construction trades/specialties from 15 countries. Two cohorts were reported in four distinct included articles (Arndt et al. 1996; Rothenbacher et al. 1997; Molano et al. 2001; Elders and Burdorf 2004). Since none of them reported duplicate data from the same cohort, all four studies were included for review. Most of the included studies were conducted in the USA (n = 9) followed by the Netherlands (n = 7) and India (n = 3) (Table 1). Other data were collected from Denmark, Hungary, Iran, Japan, Malaysia, Nigeria, Saudi Arabia, Sweden, Taiwan, Thailand, and the UK (Table 1).
The included studies had variable sample sizes, data collection methods, and response rates. The sample size of the included studies ranged from 22 to 118,258 (Pandey et al. 2012; Burström et al. 2013). Of them, 23 (66%) had a sample size of more than 300 participants. Twenty-three included studies used self- or researcher-administered questionnaires to collect prevalence data (Table 1). Four studies used face-to-face interviews, three used phone interviews, two used postal questionnaires, and two adopted semi-structured questionnaires for data collection (Table 1). Further, one study estimated the prevalence of MSS solely based on physical examination findings (Arndt et al. 1996). Thirteen studies did not report the response rate (Table 1). Five studies had a response rate of less than 70%, while 17 studies reported response rates ranging from 70.2% (Kim et al. 2014) to 98% (Caban-Martinez et al. 2010).
The included studies reported divergent types of period prevalence for work-related MSS (Table 1). Seven studies exclusively reported point prevalence, two described 6-month, 18 reported 1-year, and one described 2-year prevalence. Two studies revealed prevalence over the entire working career. Only five studies reported two to three types of period prevalence. The case definitions employed by the included studies also varied markedly from subjective pain perception to symptoms that caused the sufferer to seek medical care (Table 1).
Study quality
The quality assessment scores varied from a minimum of two (Alghadir and Anwer 2015) to a maximum of eight (Lemasters et al. 1998) with a mean value of 4.9 (1.5) (Table 2). Eleven out of 35 included studies (31%) were rated as low quality (Table 2). Overall, the included studies scored well on items related to demographics and work setting description (86%), and the use of a validated questionnaire for data collection (77%). Only five included studies adopted physician examinations of sub-samples to validate the results of self-reported prevalence or used physical examinations as a primary tool for data collection (Arndt et al. 1996; Rothenbacher et al. 1997; Lemasters et al. 1998; Engholm and Holmström 2005; Meo et al. 2013). However, the included studies scored poorly on the description of non-respondents’ characteristics (refusers, n = 29) and on the confidence interval of prevalence rate (n = 22) (Table 2, Appendix B in Supplementary material).
Different types of estimated period prevalence of MSS
The included studies reported diverse types of period prevalence and case definitions of MSS (Tables 2 and 3). Since, most studies reported 1-year prevalence using the case definition of having at least one episode of pain/MSS in the last 12 months, only 1-year prevalence of MSS at nine body regions (as described in the Nordic Musculoskeletal Questionnaire) were pooled to calculate the respective mean prevalence. The following section summarizes the most common MSS (two to three body regions) for each period prevalence. The detailed period prevalence rates of MSS in different body regions are presented in Table 3.
Seven studies reported point prevalence of MSS among construction workers (Tables 2 and 3) with lumbar, neck and lower limb MSS being the most common ones. In the USA, the point prevalence of lumbar pain/MSS ranged from 33 to 39%, while neck and knee MSS were also common with a prevalence rate of 22% each (Goldsheyder et al. 2002; Dong et al. 2012). In Saudi Arabia, the most common MSS were legs, lumbar and foot with the estimated point prevalence rates of 23.9, 16.5 and 13.4%, respectively (Meo et al. 2013). A Japanese study involving multiple construction trades reported that the point prevalence rates of lumbar and shoulder MSS were substantial with the respective estimated rates of 53.2 and 28.7% (Ueno et al. 1999). Likewise, the point prevalence of self-reported back pain ranged from 47.8 to 60.3% among German construction workers whereas another German study entailing physical examination/diagnosis revealed a slightly lower prevalence of back MSS (32.5%) (Arndt et al. 1996; Rothenbacher et al. 1997). Similarly, back MSS is the most noteworthy MSS among Dutch construction workers. The point prevalence rates of back MSS among young and older workers were 25.0 and 43.8%, respectively (de Zwart et al. 1999).
Two studies reported 1-week prevalence of MSS while one reported the 2-week prevalence (Table 3). Two most prevalent recurring MSS were found at lumbar and neck regions among Indian construction workers with estimated 1-week prevalence rates of 34 and 17%, respectively (Bodhare et al. 2011). Conversely, MSS in the knee region was the most common type among Danish floor layers and carpenters in the last 7 days, with prevalence rates of 39 and 27%, respectively (Jensen et al. 2000). Additionally, the 2-week prevalence of activity-limiting lumbar MSS was 14% among American carpenters (Gilkey et al. 2007).
Only one study reported the 1- and 3-month MSS prevalence while two reported 6-month MSS prevalence rates of different body regions (Table 3). Caban-Martinez et al. (2010) estimated the 1-month pain/MSS prevalence of knee (33.8%), shoulder (6.2–7.7%), and ankle (3.1–4.6%) among Hispanic-American construction workers. Additionally, their reported 3-month prevalence of all-day-lasting lumbar pain was 63%. The two most prominent regular/recurring MSS in sand–cement-bound and anhydrite-bound screed Dutch floor layers were lumbar and shoulder MSS with 6-month prevalence rates of 39 and 27%, and 26 and 13%, respectively (Visser et al. 2013). A prospective Dutch survey on bricklayers also revealed that the 6-month prevalence rates of recurring MSS were 42% for back and 27% for the knee at baseline, while the respective rates at 1-year follow-up were 53 and 56% (Boschman et al. 2012).
The pooled mean 1-year prevalence rates of MSS (defined as at least one episode of pain/MSS in the last 12 months) are shown in Fig. 2 and Appendix C. The estimated mean 1-year prevalence rates were 51.1% for the lumbar region [95% confidence interval (CI) 40.9–61.3%, from 19 estimates, Fig. 2], 37.2% for knee (95% CI 22.4–52.0%, from 13 estimates), 32.4% for shoulder (95% CI 17.2–47.7%, from 10 estimates), 30.4% for wrist (95% CI 19.1–41.7%, from 9 estimates), 24.4% for neck (95% CI 10.0–38.9%, from 12 estimates), 24.0% for ankle/foot (95% CI 15.2–32.8%, from 7 estimates), 20.3% for elbow (95% CI 7.7–32.9%, from 6 estimates), 19.8% for upper back MSS (95% CI 5.8–33.8%, from 6 estimates) and 15.1% for hip/thigh (95% CI 0.5–29.7%, from 5 estimates) (Table 3, Appendix C in Supplementary material).

The 1-year prevalence of lumbar MSS in different construction trades
Three studies reported 1-year prevalence rates of various chronic MSS (Tables 1 and 3). Notably, chronic elbow and wrist MSS (18.8%), and chronic shoulder MSS (18.4%) were commonly found among American carpenters (Lemasters et al. 1998). For Indian construction workers, 1-year prevalence rates of chronic lumbar, neck and knee MSS were substantial with estimated rates of 92.0, 48.0 and 47.0%, respectively (Bodhare et al. 2011). Additionally, 1-year prevalence rates of chronic knee MSS among Danish floor layers and carpenter were 56.4 and 68.0%, respectively (Jensen et al. 2000).
Five studies reported the 1-year prevalence of activity-limiting MSS but the prevalence rates varied among populations (Tables 1 and 3). The estimated 1-year prevalence rate of activity-limiting lumbar MSS was 38.0% among American carpenters (Gilkey et al. 2007), while those of lumbar and neck MSS in Swedish construction workers were 24.3 and 8.6%, respectively (Burström et al. 2013). Among Indian construction workers, 1-year prevalence rates of activity-limiting MSS in lumbar (42.0%) and neck (21.0%) regions were most notable (Bodhare et al. 2011). Similarly, the 1-year prevalence of activity-limiting MSS among Nigerian construction workers were 48.2, 26.5 and 25.3% for neck and upper limb, lower limb, and trunk and waist, respectively (Ekpenyong and Inyang 2014). Further, the two most common MSS that limited activity of Dutch scaffolders for several hours over the last 12 months were back (60.0%) and knee (37.0%) (Molano et al. 2001).
One study investigated 2-year prevalence rates of MSS that required medical assistance in US roofers (Welch et al. 2008). It showed that lumbar (28.7%) and knee (15.0%) were most affected (Table 3). Two studies investigated the prevalence of chronic MSS over the entire career of construction workers. Specifically, chronic lumbar (56.0%), wrist/hand/finger (40.4%), and knee (39.4%) MSS were most prevalent among US iron-workers (Forde et al. 2005). Similarly, prevalence rates of chronic back (50.5%) and shoulder MSS (40.7%) were eminent in American construction apprentices throughout their entire career (Kim et al. 2014). Additionally, Gilkey et al. (2007) found that the lifetime prevalence of activity-limiting lumbar MSS in US carpenters was 54.0%.
Trade-specific analysis
Many included studies did not provide stratified prevalence data that hampered comparison among various trades. Only 16 studies reported trade-specific MSS prevalence (Arndt et al. 1996; Rothenbacher et al. 1997; Lemasters et al. 1998; Ueno et al. 1999; Jensen et al. 2000; Molano et al. 2001; Elders and Burdorf 2004; Forde et al. 2005; Gilkey et al. 2007; Welch et al. 2008; van der Molen et al. 2009; Boschman et al. 2012; Visser et al. 2013; Ekpenyong and Inyang 2014; Hanklang et al. 2014; Eaves et al. 2016). Unfortunately, given the divergent reports of period prevalence and inconsistent definitions of body parts and cases, no meta-analysis was conducted for each trade. Two studies found that lumbar pain was the most prevalent MSS among bricklayers (Rothenbacher et al. 1997; Boschman et al. 2012), although others reported that neck, upper limb, and legs MSS were predominant in bricklayers (Arndt et al. 1996; Ekpenyong and Inyang 2014). Similarly, lumbar MSS were the most ubiquitous in carpenters (Arndt et al. 1996; Ueno et al. 1999; Gilkey et al. 2007; van der Molen et al. 2009; Eaves et al. 2016), while MSS of knee (Rothenbacher et al. 1997) and upper extremity (e.g. wrist and elbow) (Lemasters et al. 1998; Ekpenyong and Inyang 2014) were also common. For electricians, MSS of lumbar (Ueno et al. 1999; Burström et al. 2013) and upper extremity (Ekpenyong and Inyang 2014) were most common. Similarly, MSS of lumbar (Visser et al. 2013) and knees (Jensen et al. 2000) were most prevalent among floor layers. For iron-workers, lumbar (Ueno et al. 1999; Forde et al. 2005), wrist and shoulder (Ekpenyong and Inyang 2014; Hanklang et al. 2014) MSS were mostly reported. Likewise, plumbers mostly suffered from back (Arndt et al. 1996; Rothenbacher et al. 1997; Ueno et al. 1999), wrist and knees (Eaves et al. 2016) MSS. Additionally, lumbar pain (Arndt et al. 1996; Rothenbacher et al. 1997; Ueno et al. 1999) was prominent in laborers, painters, plasterers, pavers (van der Molen et al. 2009), roofers (Welch et al. 2008) and scaffolders (Elders and Burdorf 2004).
Gender analysis
There is a paucity of studies that reported gender-specific MSS prevalence. Thirteen out of the 35 included studies did not report the gender composition within the sample population (Table 1). Eight included studies recruited more than 85% of male participants. Two solely enrolled women construction workers (Telaprolu et al. 2013; Hanklang et al. 2014). Only two studies provided gender-segregated MSS prevalence data (Merlino et al. 2003; Guo et al. 2004). Both found that females had significantly higher 1-year prevalence of MSS (difference ranging from 0.9% in wrist to 30.1% in shoulder) as compared to their male counterparts.
Age-stratified analysis
Since the included studies used variable age group stratification methods, study designs and statistical analyses, no meta-analysis was conducted. The age range of construction workers in the included was large, ranging from a mean age of 17 (Rosecrance et al. 2001) to 71 years (Dong et al. 2012). Most studies reported both mean and standard deviation of participants’ age, while only a few reported age ranges (Table 1).
Nine of the included studies provided age-stratified analysis on prevalence data of MSS in construction workers (Alghadir and Anwer 2015; Bodhare et al. 2011; Eaves et al. 2016; Hoonakker and van Duivenbooden 2010; Jensen et al. 2000; Telaprolu et al. 2013; Ueno et al. 1999; Welch et al. 2008; de Zwart et al. 1999). Five of them found no significant association between stratified age groups and MSS prevalence (Jensen et al. 2000; Welch et al. 2008; Telaprolu et al. 2013; Alghadir and Anwer 2015; Eaves et al. 2016). Conversely, one study proclaimed a trend of increasing MSS prevalence with age although no detailed statistical result was reported (Hoonakker and van Duivenbooden 2010). The remaining three studies found significant positive associations between age and point (Ueno et al. 1999; de Zwart et al. 1999) or 1-year (Bodhare et al. 2011) MSS prevalence.
Additionally, four studies investigated the relation between age and prevalence of MSS without using stratified age data. Three studies reported positive associations between age and MSS prevalence. Specifically, a longitudinal study reported a significant increase in the prevalence of low back pain over a 15-year period although the results were confounded by workers’ job history and job exposures (Dong et al. 2012). Another study found that older Nigerian workers doubled the odds of suffering from work-related MSS than their younger counterparts (Ekpenyong and Inyang 2014). An Iranian study also found significant positive association between workers’ age and MSS prevalence (Gheibi et al. 2009). However, a study on US ironworkers found that older age was significantly associated with a lower risk of lumbar MSS after adjusting for prior injuries and work duration (odds ratio: 0.97) (Forde et al. 2005).
Discussion
This is the first systematic review to synthesize the prevalence of MSS in the construction industry. Although 35 articles were included, their heterogenous period prevalence rates and case definitions prevented the meta-analysis of each period prevalence except for 1-year prevalence (defined as at least one episode of pain/MSS in the last year). Nevertheless, our meta-analysis showed that lower back had the highest mean 1-year prevalence of MSS (51.1%) among construction workers while hip/thigh had the lowest one (15.1%). Collectively, findings from different types of period prevalence consistently suggested that construction workers most commonly suffer from lumbar, knee, shoulder and wrist MSS.
While subgroup analyses were planned for MSS prevalence of all available construction trades, the lack of relevant information prevented these analyses. Intuitively, the prevalence of MSS is related to work conditions, work-related risk factors, cultures, and personal characteristics. For example, Asian construction workers prefer to squat during work as compared to those in western countries (Chung et al. 2003; Jung and Jung 2008), which may affect their body biomechanics (Umer et al. 2017b) and predispose them to task-specific MSS. Since certain work-related tasks (e.g. frequent bending and twisting, whole-body vibration and carrying load) may increase the risk of lumbar MSS, proper ergonomic interventions should be implemented to reduce the occurrence of lumbar MSS (Burdorf and Sorock 2016). Imperatively, the current review only identified a few studies reporting MSS prevalence in individual construction trades. Therefore, there is an urgent need to investigate MSS prevalence in different trades so that trade-specific prevention/treatment strategies can be developed and implemented.
While only two studies reported MSS prevalence of both genders in the construction industry (Merlino et al. 2003; Guo et al. 2004), both indicate that female workers are more susceptible to MSS. Although speculative, this phenomenon may be attributed to differences in between-gender physique (e.g. lower muscle strength in females) (Miller et al. 1993), genetic pain coping (Bartley and Fillingim 2013), or the higher reliance on male anthropometric data for designing workspace/tools (Pheasant 1996). Importantly, with the increasing global trend of female participation in the labor force (Kinoshita and Guo 2015), it is crucial for stakeholders to investigate causes underlying differential MSS prevalence, and adopt preventive measures to minimize the risk of work-related MSS in both genders.
The current review highlights an age-related MSS trend that deserves further investigation. Thirteen included studies examined the relation between ages of construction workers and MSS prevalence with or without providing age-stratified prevalence data. Six of them concluded a non-significant association between the two variables (Jensen et al. 2000; Forde et al. 2005; Welch et al. 2008; Telaprolu et al. 2013; Alghadir and Anwer 2015; Eaves et al. 2016), while seven found a significant association between them (Bodhare et al. 2011; Dong et al. 2012; Ekpenyong and Inyang 2014; Gheibi et al. 2009; Hoonakker and van Duivenbooden 2010; Ueno et al. 1999; de Zwart et al. 1999). Despite the inconsistent findings, it cannot downplay the importance of clarifying the association between age and work-related MSS in construction workers. It is known that the proportion of older workforce is increasing in many industrialized countries (Samorodov 1999). Older workers commonly experience decline in physical work capacity (Kenny et al. 2008), cardiac output (Fitzgerald et al. 1985), muscle strength and mass (Thomas 2010). Physical decline alongside the presence of MSS will increase the risk of work injury in older workers who usually have higher rehabilitation demands (Schwatka et al. 2012). Importantly, literature suggests that previous occupational biomechanical exposures (e.g. twisting and bending) can increase the risk of future episodes of low back pain in older/retired workers (Plouvier et al. 2015). Accordingly, future studies should clarify the relation between age and work-related MSS, and develop strategies to minimize the propensity of MSS in older workers.
Limitations
Like other reviews, our study has several limitations. First, given the heterogeneous populations, case definitions, work tasks and study designs of the included studies, our estimated 1-year prevalence should be interpreted with caution. Specifically, the current meta-analysis defined pain cases as having at least one episode of pain/MSS in the last year. The use of such a lenient case definition for meta-analysis without considering other factors (e.g., pain intensity, frequency, duration, work-related disability, or work absence) might have limited the generalizability of the meta-analysis results (Bedouch et al. 2012). Previous epidemiological research has shown that using different case definitions (e.g. based on pain intensity or frequency) to evaluate the MSS prevalence of a given population would lead to different conclusions (Beaton et al. 2000; Village 2000; Hegmann et al. 2014). Although using a more specific case definition (Table 1) in the current meta-analysis could have improved the generalizability and homogeneity of findings specific to the case definition, such approach would have also excluded many primary studies from the meta-analysis. To improve future meta-analyses, future epidemiological studies should use standardized case definitions to evaluate the prevalence of MSS in the construction industry. Second, since many included studies adopted self-reported prevalence without validated medical examinations, their reported prevalence might have been underestimated/overestimated. Third, 29 out of the 35 included studies did not report non-respondents’ characteristics, which might represent a group with distinct MSS prevalence. Fourth, since included studies used inconsistent study protocols and period prevalence, future studies should adopt standardized measurement tools and study protocols to enable between-study comparisons.
Implications
Despite the limitations, our review has strong implications for construction managers, ergonomists, policy makers and researchers. The results signify that more than half of the construction workforce face lumbar MSS, nearly one-third of them face knee, shoulder and wrist MSS annually. These figures underscore the necessity of deriving relevant policies and developing/implementing effective prevention strategies to attenuate the prevalence of work-related MSS in the construction industry.
Conclusions
This is the first systematic review to synthesize the prevalence of various MSS in the construction industry. Lumbar, knee, shoulder and wrist MSS are consistently found to be the most prevalent among construction workers. Existing evidence suggests that female construction workers may be more vulnerable to work-related MSS although the relation between age and MSS prevalence among construction workers remains unclear. Collectively, further prevalence and mechanistic studies are warranted to identify the prevalence and underlying causes of different work-related MSS in various construction trades so that effective prevention and treatment strategies for these MSS can be developed/implemented.
References
Agresti A, Coull BA (1998) Approximate is better than “exact” for interval estimation of binomial proportions. Am Stat 52:119–126. doi:10.1080/00031305.1998.10480550
Alghadir A, Anwer S (2015) Prevalence of musculoskeletal pain in construction workers in Saudi Arabia. Sci World J. doi:10.5958/0976-5506.2015.00013.3
Antwi-Afari MF, Li H, Edwards DJ et al (2017) Effects of different weights and lifting postures on balance control following repetitive lifting tasks in construction workers. Autom Constr 83:41–47. doi:10.1016/j.autcon.2017.07.007
Arndt V, Rothenbacher D, Brenner H et al (1996) Older workers in the construction industry: results of a routine health examination and a five year follow up. Occup Environ Med 53:686–691. doi:10.1136/oem.53.10.686
Arndt V, Rothenbacher D, Daniel U et al (2005) Construction work and risk of occupational disability: a ten year follow up of 14474 male workers. Occup Environ Med 62:559–567. doi:10.1136/oem.2004.018135
Bartley EJ, Fillingim RB (2013) Sex differences in pain: a brief review of clinical and experimental findings. Br J Anaesth 111:52–58. doi:10.1093/bja/aet127
Beaton DE, Cole DC, Manno M et al (2000) Describing the burden of upper-extremity musculoskeletal disorders in newspaper workers: what difference do case definitions make? J Occup Rehabil 10:39–53. doi:10.1023/A:1009489712094
Bedouch P, Marra CA, FitzGerald JM et al (2012) Trends in asthma-related direct medical costs from 2002 to 2007 in British Columbia, Canada: a population based-cohort study. PLoS One 7:1–8. doi:10.1371/journal.pone.0050949
Bodhare T, Valsangkar S, Bele S (2011) An epidemiological study of work-related musculoskeletal disorders among construction workers in Karimnagar, Andhra Pradesh. Indian J Community Med 36:304–307. doi:10.4103/0970-0218.91420
Boschman JS, van der Molen HF, Sluiter JK, Frings-Dresen MHW (2012) Musculoskeletal disorders among construction workers: a one-year follow-up study. BMC Musculoskelet Disord. doi:10.1186/1471-2474-13-196
Buchholz B, Paquet V, Punnet L et al (1996) PATH: a work sampling-based approach to ergonomic job analysis for construction work path: a work sampling-based approach to ergonomic job analysis for construction and other non-repetitive work. Appl Ergon 27:177–187. doi:10.1016/0003-6870(95)00078-X
Burdorf A, Sorock G (2016) Positive and negative evidence of risk factors for back disorders. Scand J Work Env Heal 23:243–256. doi:10.5271/sjweh.217
Bureau of Labor Statistics (BLS) (2013) Nonfatal occupational injuries and illnesses requiring days away from work, 2012. https://www.bls.gov/news.release/archives/osh2_11262013.pdf. Accessed 9 Oct 2017
Burström L, Järvholm B, Nilsson T, Wahlström J (2013) Back and neck pain due to working in a cold environment: a cross-sectional study of male construction workers. Int Arch Occup Environ Health 86:809–813. doi:10.1007/s00420-012-0818-9
Caban-Martinez AJ, Lee DJ, Clarke TC et al (2010) Self-reported joint and back pain among Hispanic construction workers: a pilot workplace musculoskeletal assessment. J Musculoskelet Res 13:49–55. doi:10.1142/S0218957710002508
Chung MK, Lee I, Kee D (2003) Effect of stool height and holding time on postural load of squatting postures. Int J Ind Ergon 32:309–317. doi:10.1016/S0169-8141(03)00050-7
Deros BM, Daruis DD, Khamis NK et al (2014) Prevalence of work related musculoskeletal disorders symptoms among construction workers: a case study in Malaysia. Iran J Public Health 43:53–57
Dong XS, Wang X, Fujimoto A, Dobbin R (2012) Chronic back pain among older construction workers in the United States: a longitudinal study. Int J Occup Environ Health 18:99–109. doi:10.1179/1077352512Z.0000000004
Eaves S, Gyi DE, Gibb AGF (2016) Building healthy construction workers: their views on health, wellbeing and better workplace design. Appl Ergon 54:10–18. doi:10.1016/j.apergo.2015.11.004
Ekpenyong CE, Inyang UC (2014) Associations between worker characteristics, workplace factors, and work-related musculoskeletal disorders: a cross-sectional study of male construction workers in Nigeria. Int J Occup Saf Ergon 20:447–462. doi:10.1080/10803548.2014.11077057
Elders LAM, Burdorf A (2004) Prevalence, incidence, and recurrence of low back pain in scaffolders during a 3-year follow-up study. Spine (Phila Pa 1976) 29:E101–E106. doi:10.1097/01.BRS.0000115125.60331.72
Engholm G, Holmström E (2005) Dose-response associations between musculoskeletal construction workers dose-response associations between musculoskeletal disorders and physical and psychosocial factors among construction workers. Scand J Work Env Heal 31:57–67
Fejer R, Kyvik KO, Hartvigsen J (2006) The prevalence of neck pain in the world population: a systematic critical review of the literature. Eur Spine J 15:834–848. doi:10.1007/s00586-004-0864-4
Fitzgerald MD, Tanaka H, Tran ZV et al (1985) Age-related declines in maximal aerobic capacity in regularly exercising vs. sedentary women: a meta-analysis. J Appl Physiol 83:160–165
Forde MS, Buchholz B (2004) Task content and physical ergonomic risk factors in construction ironwork. Int J Ind Ergon 34:319–333. doi:10.1016/j.ergon.2004.04.011
Forde MS, Punnett L, Wegman DH (2005) Prevalence of musculoskeletal disorders in union ironworkers. J Occup Environ Hyg 2:203–212. doi:10.1080/15459620590929635
Gheibi L, Nasl Saraji J, Zeraati H, Pouryaghub G (2009) Assessment of ergonomic situation of workers in a dam construction workshops using the NIOSH-CPWR Checklist. J Sch Public Heal Inst Public Heal Res 7:13–24
Gilkey DP, Keefe TJ, Bigelow PL et al (2007) Low back pain among residential carpenters: ergonomic evaluation using OWAS and 2D compression estimation. Int J Occup Saf Ergon 13:305–321. doi:10.1080/10803548.2007.11076731
Goldsheyder D, Nordin ÃM, Weiner SS, Hiebert R (2002) Musculoskeletal symptom survey among mason tenders. Am J Ind Med 42:384–396. doi:10.1002/ajim.10135
Graham ID, Harrison MB, Nelson EA et al (2003) Prevalence of lower-limb ulceration: a systematic review of prevalence studies. Adv Skin Wound Care 16:305–316. doi:10.1097/00129334-200311000-00013
Guo HR, Chang YC, Yeh WY et al (2004) Prevalence of musculoskeletal disorder among workers in Taiwan: a nationwide study. J Occup Health 46:26–36. doi:10.1539/joh.46.26
Hanklang S, Kaewboonchoo O, Silpasuwan P, Mungarndee SS (2014) Musculoskeletal disorders among Thai women in construction-related work. Asia-Pacific J Public Heal 26:196–202. doi:10.1177/1010539512466429
Hegmann KT, Thiese MS, Garg EMWA et al (2014) Impacts of differences in epidemiological case definitions on prevalence for upper-extremity musculoskeletal disorders. Hum Factors J Hum Factors Ergon Soc 56:191–202. doi:10.1177/0018720813487202
Hoonakker P, van Duivenbooden C (2010) Monitoring working conditions and health of older rorkers in Dutch construction industry. Am J Ind Med 53:641–653. doi:10.1002/ajim.20838
Hoy D, Bain C, Williams G et al (2012) A systematic review of the global prevalence of low back pain. Arthritis Rheum 64:2028–2037. doi:10.1002/art.34347
Inyang N, Al-hussein M, El-rich M, Al-jibouri S (2012) Ergonomic analysis and the need for its integration for planning and assessing construction tasks. J Constr Eng Manag 138:1370–1376. doi:10.1061/(ASCE)CO
Jensen LK, Mikkelsen S, Loft IP, Eenberg W (2000) Work-Related knee disorders in floor layers and carpenters. J Occup Environ Med 42:835–842
Jung HS, Jung H-S (2008) Evaluation of proper height for squatting stool. Ergonomics 51:671–690. doi:10.1080/00140130701744506
Kenny GP, Yardley JE, Martineau L, Jay O (2008) Physical work capacity in older adults: implications for the aging worker. Am J Ind Med 51:610–625. doi:10.1002/ajim.20600
Kim S, Dutra LM, Okechukwu CA (2014) Contractor-, steward-, and coworker-safety practice: associations with musculoskeletal pain and injury-related absence among construction apprentices. Int Arch Occup Env Heal 87:493–500. doi:10.1007/s00420-013-0889-2
King S, Chambers CT, Huguet A et al (2011) The epidemiology of chronic pain in children and adolescents revisited: a systematic review. Pain 152:2729–2738. doi:10.1016/j.pain.2011.07.016
Kinoshita Y, Guo F (2015) What can boost female labor force participation in Asia? International Monetary Fund https://www.imf.org/external/pubs/ft/wp/2015/wp1556.pdf Accessed 9 Oct 2017
Kok LM, Huisstede BMA, Voorn VMA et al (2015) The occurrence of musculoskeletal complaints among professional musicians: a systematic review. Int Arch Occup Environ Health. doi:10.1007/s00420-015-1090-6
Lee HY, Yeh WY, Chen CW, Wang JD (2005) Prevalence and psychosocial risk factors of upper extremity musculoskeletal pain in industries of Taiwan: a nationwide study. J Occup Health 47(4):311–318
Lemasters GK, Atterbury MR, Booth-Jones AD et al (1998) Prevalence of work related musculoskeletal disorders in active union carpenters. Occup Environ Med 55:421–427. doi:10.1136/oem.55.6.421
Loney PL, Chambers LW, Bennett KJ et al (1998) Critical appraisal of the health research literature: prevalence or incidence of a health problem. Chronic Dis Can 19:170–176
Meo SA, Alsaaran ZF, Alshehri MK et al (2013) Work-related musculoskeletal symptoms among building construction workers in Riyadh, Saudi Arabia. Pak J Med Sci 29:1394–1399
Merlino LA, Rosecrance JC, Anton DC, Cook TM (2003) Symptoms of musculoskeletal disorders among apprentice construction workers. Appl Occup Environ Hyg 18:57–64. doi:10.1080/10473220301391
Miller AEJ, Macdougall JD, Tarnopolsky MA, Sale DG (1993) Gender differences in strength and muscle fiber characteristics. Eur J Appl Physiol Occup Physiol 66:254–262
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Reprint–preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Phys Ther 89:873–880. doi:10.1136/bmj.b2535
Molano SM, Burdorf A, Elders LAM (2001) Factors associated with medical care-seeking due to low-back pain in scaffolders. Am J Ind Med 40:275–281. doi:10.1002/ajim.1099
Pandey V, Chakraborty T, Mukhopadhyay S (2012) Prevalence of musculoskeletal disorders, levels of physical activity and perceived quality of life amongst construction site managers in Mumbai: a case study. Work 43:447–451. doi:10.3233/WOR-2012-1461
Peppas G, Alexiou VG, Mourtzoukou E, Falagas ME (2008) Epidemiology of constipation in Europe and Oceania: a systematic review. BMC Gastroenterol 8:5. doi:10.1186/1471-230X-8-5
Pheasant S (1996) Bodyspace: anthropometry, ergonomics and the design of work, second. Taylor & Francis, London
Plouvier S, François J, Cyr D et al (2015) Occupational biomechanical exposure predicts low back pain in older age among men in the Gazel Cohort. Int Arch Occup Env Heal 88:501–510. doi:10.1007/s00420-014-0979-9
Rosecrance J, Pórszász J, Cook TM et al (2001) Musculoskeletal disorders among construction apprentices in Hungary. Cent Eur J Public Health 9:183–187
Rothenbacher D, Brenner H, Arndt V et al (1997) Disorders of the back and spine in construction workers. Spine (Phila Pa 1976) 22:1481–1486
Samorodov A (1999) Ageing and labour markets for older workers. Employment and Training Department, International Labour Office Geneva. http://www.ilo.int/wcmsp5/groups/public/@ed_emp/documents/publication/wcms_120333.pdf Accessed 9 Oct 2017
Schwatka NV, Butler LM, Rosecrance JR (2012) An aging workforce and injury in the construction industry. Epidemiol Rev 34:156–167. doi:10.1093/epirev/mxr020
Telaprolu N, Lal B, Chekuri S (2013) Work related musculoskeletal disorders among unskilled Indian women construction workers. Natl J Community Med 4:658–661
Thomas DR (2010) Sarcopenia. Clin Geriatr Med 26(2):331–346. doi:10.1016/j.cger.2010.02.012
Ueno S, Hisanaga N, Jonai H et al (1999) Association between musculoskeletal pain in Japanese construction workers and job, age, alcohol consumption and smoking. Ind Health 37:449–456
Umer W, Li H, Szeto GP, Wong AY (2017a) A low cost ergonomic intervention for mitigating physical and subjective discomfort during manual rebar tying. J Constr Eng Manag. doi:10.1061/(ASCE)CO.1943-7862.0001383
Umer W, Li H, Szeto GPY, Wong AYL (2017b) Identification of biomechanical risk factors for the development of lower-back disorders during manual rebar tying. J Constr Eng Manag. doi:10.1061/(ASCE)CO.1943-7862.0001208
van der Molen HF, Sluiter JK, Frings-Dresen MHW (2009) The use of ergonomic measures and musculoskeletal complaints among carpenters and pavers in a 4.5-year follow-up study. Ergonomics 52:954–963. doi:10.1080/00140130902763560
Village J (2000) A comparison of “case definitions” to estimate prevalence of work-related musculoskeletal disorders in hospital laundry workers and the influence of psychosocial variables. Proc Hum Factors Ergon Soc Annu Meet 44:577–580. doi:10.1177/154193120004403049
Visser S, van der Molen HF, Kuijer PPFM et al (2013) Evaluation of two working methods for screed floor layers on musculoskeletal complaints, work demands and workload. Ergonomics 56:69–78. doi:10.1080/00140139.2012.736541
Wang D, Dai F, Ning X (2015) Risk assessment of work-related musculoskeletal disorders in construction: state-of-the-art review. J Constr Eng Manag. doi:10.1061/(ASCE)CO.1943-7862.0000979
Welch LS, Haile E, Boden LI, Hunting KL (2008) Age, work limitations and physical functioning among construction roofers. Work 31:377–385
Wong AYL, Parent EC, Funabashi M et al (2013) Do various baseline characteristics of transversus abdominis and lumbar multifidus predict clinical outcomes in nonspecific low back pain? A systematic review. Pain 154:2589–2602. doi:10.1016/j.pain.2013.07.010
De Zwart BCH, Frings-Dresen MHW, van Duivenbooden JC (1999) Senior workers in the Dutch construction industry: a search for age-related work and health issues. Exp Aging Res 25:385–391. doi:10.1080/036107399243841
Acknowledgements
The authors would like to thank Dr. Liliana Lapierre for assisting the screening of a Spanish article, Mr. Peyman Azad for translating and extracting relevant information from a Persian article, and Dr. Martha Funabashi for screening a Portuguese article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Umer, W., Antwi-Afari, M.F., Li, H. et al. The prevalence of musculoskeletal symptoms in the construction industry: a systematic review and meta-analysis. Int Arch Occup Environ Health 91, 125–144 (2018). https://doi.org/10.1007/s00420-017-1273-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-017-1273-4