
Abstract
Purpose
Welding fume consists of metal fumes, e.g., manganese (Mn) and gases, e.g., ozone. Particles in the respirable dust (RD) size range dominate. Exposure to welding fume could cause short- and long-term respiratory effects. The prevalence of work-related symptoms among mild steel welders was studied, and the occupational exposure to welding fumes was quantified by repeated measurements of RD, respirable Mn, and ozone. Also the variance components were studied.
Method
A questionnaire concerning airway symptoms and occupational history was answered by 79 % of a cohort of 484 welders. A group of welders (N = 108) were selected and surveyed by personal exposure measurements of RD and ozone three times during 1 year.
Results
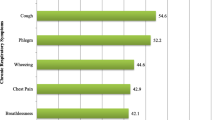
The welders had a high frequency of work-related symptoms, e.g., stuffy nose (33 %), ocular symptoms (28 %), and dry cough (24 %). The geometric mean exposure to RD and respirable Mn was 1.3 mg/m3 (min–max 0.1–38.3 mg/m3) and 0.08 mg/m3 (min–max <0.01–2.13 mg/m3), respectively. More than 50 % of the Mn concentrations exceeded the Swedish occupational exposure limit (OEL). Mainly, low concentrations of ozone were measured, but 2 % of the samples exceeded the OEL. Of the total variance for RD, 30 and 33 % can be attributed to within-worker variability and between-company variability, respectively.
Conclusions
Welders had a high prevalence of work-related symptom from the airways and eyes. The welders’ exposure to Mn was unacceptably high. To reduce the exposure further, control measures in the welding workshops are needed. Correct use of general mechanical ventilation and local exhaust ventilation can, for example, efficiently reduce the exposure.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Welding is a common occupation in Sweden. It has been reported that approximately 25,000 full-time welders are occupied in Sweden and further additionally 250,000 jobs related to welding (Taube 2013). Welding in mild steel accounts for the majority of all welding (Beckett 1996) and the most common method is gas metal arc welding (GMAW). GMAW includes predominant welding methods such as metal arc active gas (MAG) and metal arc inert gas (MIG).
The majority of the welding fumes generated during welding originate from the electrodes, which is mainly determined by the composition of the welded metal (Antonini 2003). The welding fume consists of a complex aerosol of mainly metal fumes and gases, which reacts with the air, and metal oxide particles are formed. The welding fume particles can consist of, e.g., iron (Fe), manganese (Mn), lead (Pb), copper (Cu), zinc (Zn), nickel (Ni), cobalt (Co), and hexavalent chromium (Cr(VI)) depending on the used materials. The emitted primary particles are in the nanosized range between 2 and 70 nm in particle diameter, and the primary particles will immediately aggregate and form larger aggregates (Zimmer and Biswas 2001; Isaxon et al. 2013). For GMAW, the median particle diameters were 149 and 160 nm, respectively (Zimmer and Biswas 2001; Isaxon et al. 2013). Antonini (2003) reported that the majority of the particles in the welding fume were typically 0.5 μm, and welding fume particles can therefore be considered to be in the respirable size range.
Welders are exposed to different types of metal particles which could cause adverse health effects. Welding fume has been classified as possibly carcinogenic to humans (Group 2B) by the International Agency for Research on Cancer since there is an increased risk for welders to develop lung cancer (IARC 1990). Welding fume exposure is potentially harmful to the airways and could cause both short-term and long-term respiratory effects such as chronic bronchitis, occupational asthma, and pneumoconiosis (Sferlazza and Beckett 1991; Antonini 2003; Jönsson et al. 2011; Zeidler-Erdely et al. 2012; Taube 2013).
Furthermore, metal fume fever can be elicited by Zn and Cu exposure (Nemery 1990). Mn in the welding fumes may cause neurotoxical effects in concentrations of <0.2 mg/m3 (Antonini et al. 2006; Bowler et al. 2007; Furbee 2011; Wastensson et al. 2012). The effects may be those of neurological and neurobehavioral deficits, e.g., changes in mood and short-term memory, altered reaction time, and reduced hand–eye coordination (Bowler et al. 2007). Chronic Mn exposures <0.5 mg/m3 may cause tremor, weakness, and impaired eye–hand coordination (Fitsanakis et al. 2006; Klos et al. 2006). A recent Swedish study of former welders with previous Mn exposure reported of poorer motor function in welders’ hands compared with the controls (Wastensson et al. 2012). Inhalation of Mn may also cause adverse health effects to the liver, kidney, and male infertility (Taube 2013).
Welders’ exposure during GMAW was recently quantified as respirable dust (RD) to a median concentration of 1.3 mg/m3 (Lehnert et al. 2012). Another study measured the welders’ exposure to total dust (TD) ranging from 2.9 to 4.4 mg/m3 (Boelter et al. 2009). Welding performed in small, enclosed areas can cause even higher exposures. A summary of the literature regarding Mn exposure to welders shows that the air concentrations were frequently at or higher than 0.2 mg/m3 (Flynn and Susi 2010).
The exposure to welding fumes is regulated by occupational exposure limits (OELs) set for exposure during a working day, normally 8 h (level limit values). The Swedish Work Environment Authority has set OELs for inorganic RD to 5 mg/m3, for Mn to 0.1 mg/m3 as RD, and for ozone to 0.2 mg/m3 (Swedish Work Environment Authority 2011).
There are several factors that determine the occupational exposure to welders, e.g., welding process, protective measures, workplace characteristics and practice, including number of welders, work speed, and technique, position during welding, and mechanical ventilation (Hobson et al. 2011). Modern welding workshops and plants often have general mechanical ventilation systems. Together with the use of control measures, e.g., local exhaust ventilation (LEV), welding gun with integrated exhaust ventilation, the occupational exposure to welding fumes can be reduced and controlled. Welders sometimes use personal protective equipment (PPE) such as powered air purifying respirators (PAPRs). However, irrespective of the use of control measures, welders are a frequent group of patients in our polyclinic due to symptoms from the airways.
The aim of this study was (1) to study the prevalence of symptoms from eyes and airways among welders, (2) to survey the occupational exposure to welding fumes in southern Sweden during MIG/MAG welding in mild steel by repeated personal measurements of RD and its metal content and ozone, and (3) to study how much of the variation in exposure of RD that was attributed to within and between individual and company factors.
Methods
Study population
The study consists of two parts. In the first part, medium-sized companies in southern Sweden with mild steel welding departments were recruited for participating in a cross-sectional study concerning welders’ occupational exposure to welding fumes and work-related symptoms. In total, 11 companies were included in the study and 484 workers were identified as regular welders by the managements and unions and included in the cohort (Jönsson et al. 2013). The welders answered a questionnaire concerning symptoms and occupational history (see below), and the response rate was 79 % (N = 382). The characteristics of the mild steel welders can be seen in Table 1. From workshops with more than eleven welders, all non-smoking subjects who had reported work-related symptoms from the upper and/or lower airways the last month in the screening questionnaire were invited to participate in the personal exposure measurements (PEMs). Thus, 76 workers with work-related symptoms were included in the study together with 32 welders without a history of work-related airway symptoms, who were matched to the symptomatic welders with regard to factory, age, and atopy by history. In total, 108 welders participated in this study, and for more information which welders that were included see Jönsson et al. (2013).
In the second part of the study, a panel of welders (N = 108) were selected for a more in-depth study regarding symptoms and exposure, collected with a diary for three two-week periods. The selected welders were non-smokers and were divided into three groups: welders with symptoms from the upper airways, welders with symptoms from the lower airways, and welders without symptoms. The result from the diary study will be published elsewhere (Jönsson et al. 2013). The selected welders were surveyed by PEMs of RD and ozone three times during 1 year. The study was approved by the Research Ethics Committee (LU 276-03) at Lund University (Lund, Sweden).
Questionnaire
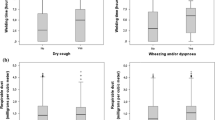
A slightly modified questionnaire developed by the European Study Group on Acid Anhydrides (ESGAA; Drexler et al. 1999) was used. It was asked about work tasks, atopy, smoking habits, and symptoms from eyes, upper and lower airways during the last month and their relation to work tasks. Atopy was defined as a history of hay fever, asthma, or atopic eczema during childhood or adolescence. Asthma-like symptoms included attacks of dyspnea and wheezing breath. Dry cough denoted attacks of cough without sputum. Ocular symptoms denoted foreign body sensation, scratching, burning, and/or itching. Work-related symptoms were defined as those symptoms directly associated with work and/or symptoms recovering during weekends and holidays (Ferris 1978).
Personal exposure measurement
During 1 year, PEMs were performed in the selected panel of welders working at 11 different companies. All companies were visited three times (winter, spring, summer after vacations) for the exposure measurements. In total, 108 welders participated in the PEMs. All welders participating in the study were equipped with two parallel sampling systems, one for RD and one for ozone. The samplers were placed in the workers breathing zone. For welders using PPE, sampling was performed outside the PPE.
Description of the companies
Eleven medium-sized companies participated in the study. Workplace characteristics of the companies based on questionnaire data regarding the presence of general mechanical ventilation, use of LEV, use of PAPR, and coexistence of grinding can be seen in Table 2. A description of each of the companies based on observations made by the occupational hygienists who performed the PEMs follows:
Company 1
Company 1 manufactured asphalt rollers. The production was mainly concentrated on three departments: component-, rolling mills-, and prototype workshops. In the first two departments, welding was extensive and took place inside/on the components or at welding benches. LEVs were quite common. In the prototype workshop, welding was sparser. The production was normal during all sampling periods.
Company 2
Company 2 produced fork-lift trucks. The premises included two parallel halls where most of the work took place at welding benches on each side of a middle pathway. Adjustable LEVs were standard. Some automated robot welding occurred in the halls as well. Production was normal except for one sampling period (summer after vacations).
Company 3
Company 3 manufactured big dumper trucks. The production took place in large premises mainly served by mechanical ventilation of the displacement type. The production was normal during all three sampling periods.
Company 4
Company 4 produced hydraulic lifting tables on a rather small scale. The work was located in one large and one much smaller room with displacement type general ventilation. Welding took place on welding benches. The production was normal during all three sampling periods.
Company 5
Company 5 manufactured windmill towers in two huge halls. The premises were mainly ventilated by self-draft and by the frequent opening of large sliding doors (natural ventilation). Aero tempers in the ceiling helped to warm the internal air. The welders worked mainly in or on top of the big tower segments. Apart from the common welding methods like MIG or MAG, some semi-automatic submerged arc melt welding was used. The production was normal except after the summer vacations when it was around 50 % due to the lack of steel.
Company 6
Company 6 produced railway wagons in a workshop adjacent to company 5. The layout of the halls and ventilation was about the same. Welding took place mainly at welding benches but also directly to the details lying on the floor. Production was normal during all three sampling periods.
Company 7
Company 7 manufactured parts for fork-lift truck producers, like rams and cabins in three rooms at two different workshops. The premises were equipped with general ventilation and LEVs at the welding benches where most of the welding was done. The production was normal except for the spring measurements when production was about 70 %.
Company 8
Company 8 made fork-lift trucks in one big room supplied with general mechanic ventilation which was insufficient as smoke gathered in the ceiling at the end of the workday. The work of the welders was intermittent including intensive welding during 1–2 days followed by 0.5–1 day of grinding the objects. Integrated exhaust ventilation in the welding guns was common. Production was normal during all three sampling periods.
Company 9
Company 9 produced heating boilers and heat pumps in rather large halls. The welders were organized in work groups with job rotation that were responsible for a certain part of the production. The work took place at welding benches. The production was normal during all three sampling periods.
Company 10
Company 10 manufactured stoves of different kinds on rather cramped premises. The ceiling height was low. The welders worked at welding benches adjusted to the size of the objects. The benches had LEVs but they were often too far away from the welding point. Production was normal during all three sampling periods.
Company 11
Company 11 was a supplier of part for among other car producers and producers of oil coolers. The welding was performed in many small rooms mainly at welding benches. The general mechanical ventilation was reinforced in two rooms. Some welders used integrated exhaust ventilation in the welding guns. The production was normal except for the winter period when it reached about 60 %. The production in one small department with two workers was low also during the spring sampling period.
Air monitoring
The air samples were collected in the workers breathing zones and were in the most cases performed during full-shift work, in average 6.2 h (min–max 0.5–9.1 h).
Sampling of respirable dust
The exposure to respirable portions of welding fumes (RD) was measured by air sampling on preweighed mixed cellulose ester filters (0.8 μm pore size, 37 mm diameter) fitted in leak-free cassettes (SURE-SEAL) made of conductive polypropylene attached to RD cyclones made of nickel-plated aluminum (IL-4, BGI Inc., USA). Battery-powered sampling pumps (MSA Escort Elf®, SKC Aircheck™) were operated at a flow rate of 2.2 l/min. The airflow was continuously monitored by flow meters.
A setup consisting of two parallel sampling systems for RD was used for assessing the workplace protection factor (WPF) for PAPRs. One sampling system was used for sampling inside the PAPR and one sampling system was used for sampling outside the PAPR on the shoulder in the breathing zone. Parallel samplings with the setup were performed on one welder and with a “dummy” PAPR. The parallel sampling on the welder was performed during 170 min. The parallel sampling for the “dummy” PAPR was performed as close as possible to a welder. One sampler was placed inside the PAPR and the outside sampler was placed on the welders shoulder in the breathing zone. The sampling period was 415 min.
Sampling of ozone
Ozone was sampled on double nitrite-impregnated glass fiber filters fitted in 37-mm polypropylene cassettes. Battery-powered sampling pumps (SKC Airlite™, SKC 222) were operated at a flow rate of 0.2 l/min. Pumps were calibrated following standard procedures, and the flow rate was continuously monitored by the use of flow meters.
Size-selective sampling
Welding fume and grinding dust in the breathing zone was independently sampled on 25- and 37-mm PTFE (Teflon) filters by means of a personal cascade impactor (5-stage Sioutas Personal Cascade Impactor, SKC Inc., USA). Flow rate was 9 l/min by the use of a battery-powered pump (Leland Legacy, SKC Inc., USA). The filters were weighed before and after sampling. A total of four welding samples and one grinding sample were collected.
Analysis
Respirable dust sample
The filter samples were analyzed gravimetrically for RD according to a certified method. The LOD was set to 0.05 mg/sample.
Metal composition analysis
The metal composition of the RD samples was quantified. The filter samples were worked up by digestion with nitric acid. Analysis was performed by inductively coupled plasma-mass spectrometry (ICP-MS; Thermo X7, Thermo Elemental, Winsford, UK), and elements such as Fe, Mn, Pb, Zn, Cu, Cd, Cr, and Ni were detected. The LOD for each element was calculated as three times the standard deviation of blank filters. The LOD was typically <0.33 μg Fe/sample, <0.002 μg Cd/sample, <0.01 μg/sample for Mn, Zn, Cu, Ni, and Cr, <0.08 μg/sample for Pb.
Ozone analysis
Ozone was determined by ion chromatography (OSHA ID-214, OSHA 2008). The limit for detection (LOD) for ozone was 0.75 μg/sample.
Statistics
The exposure is presented as both arithmetic mean (AM) and geometric mean (GM) with geometric standard deviation (GSD) due to lognormally distributed data. Values below the LOD were given the value half the LOD. To test association between symptoms and atopics, smoking habits or years welding Fisher’s exact test were used. The median numbers of years occupied with welding were chosen as cutoff for welding years. The within-individual (σ²Within i), between-individuals (σ²Between i), within-company (σ²Within c), and between-companies (σ²between c) components of variance were estimated by the Nested procedure of SAS (balanced data) of log-transformed personal exposure levels. The statistical tests were performed in SPSS 15.0 for Windows (SPSS Inc.) and SAS 9.2 for Windows (SAS Institute Inc.). We regarded p < 0.05 as statistically significant.
Results
Prevalence of symptoms
The median welding time was 15 years (min–max 1–45 years) for the cohort of welders which consisted of 379 males and 3 females. Other self-reported descriptive data such as atopy and smoking habits for the welders are described in Table 1. Of the welders, 79 % were non- and ex-smokers. The last month prevalence symptoms in general and work-related are shown in Table 3. Most frequent work-related symptoms were nasal (33 %) and ocular symptoms (28 %). Dry cough was reported by 24 % and work-related wheezing by 12 % of the welders. Atopic welders had statistically significant more work-related stuffy nose and attacks of shortness of breath than none atopic welders (Table 4). Subjects who had welded less than 15 years had significantly more nose bleeding related to work and more often chest tightness than those who had welded more than 15 years (Table 4).
Exposure measurements
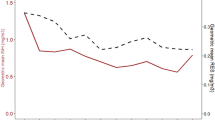
A total of 789 samples of RD, respirable Mn, and ozone were collected. The time-weighed averaged exposure of RD, Mn, and ozone for the welders at the eleven companies is summarized in Table 5a–c. The RD concentrations ranged from 0.1 to 38.3 mg/m3. The GM for RD in the 11 companies was 1.3 mg/m3. Less than 10 % of the RD concentrations exceeded the Swedish OEL, 5 mg/m3. The exposure level of respirable Mn was 0.08 mg/m3 (GM) with a range between <0.01–2.13 mg/m3. More than 50 % of the measured Mn values exceeded the OEL. The majority of the other measured respirable metal concentrations of Cd, Ni, Pb, Cu, Zn, and Ni had undetectable concentrations and were for this reason not reported. The correlation between RD and respirable Mn was strong (R 2 = 0.87) and can be seen in Fig. 1. Thus, it is clearly shown that GMAW in mild steel also causes exposure to Mn and that the sampled RD in average consisted of 7 % Mn. Fe was, of course, the predominant component (~90 % of the RD).

Correlations between respirable dust and respirable Mn in 262 full-shift air samples collected during GMAW (two outliers were excluded)
Parallel sampling inside and outside the PAPRs revealed a protection factor of 3 compared to the assigned protection factor of 50. The corresponding protection factor for the “dummy” PAPR was 20.
The GM for ozone was 0.03 mg/m3 (min–max <0.01–0.66 mg/m3). Six of the samples (2 %) exceeded the Swedish OEL of 0.2 mg/m3.
The results from the size-selective sampling of dust are presented in Table 6. The dominating particle fraction in the welding fume based on the mass had a particle size <0.25 μm (53 %). The dust generated by grinding was composed of particles with large diameter. In the emitted grinding dust, the dominated mass fraction (59 %) had a size between 2.5 and 10 μm in size.
Calculations of the within and between variance for RD revealed that the largest fractions of the total variance can be attributed to between-company factors (33 %) and to the within-worker variance or interday variability (30 %). The between-worker variability produced a 19 % variation and within-company factors can be attributed to 18 % of the total variance.
Discussion
Prevalence of symptoms
This group of full-time welders working with GMAW in mild steel reported frequent work-related symptoms from eyes and airways although the exposure in general not exceeded the current Swedish exposure limits. The prevalence of symptoms was in the same range of magnitude as found in workers exposed to other potential harmful environments using the same questions such as exposure to potassium aluminum-tetrafluoride soldering flux (Larsson et al. 2007) and powder painting (Blomqvist et al. 2005). The present findings are in agreement with earlier studies also reported regarding respiratory symptoms in welders (Wolf et al. 1997; Sharifian et al. 2011; Temel et al. 2010). The risk for symptoms may in the present study be underestimated prevalence because of a healthy workers selection as indicated by the fact that welders with shorter time of welding reported more work-related nose bleeding and wheeze than welders with a longer time. The welders may be differently sensitive to welding fume as atopic welders have more nasal symptoms and dyspnea than none atopics. It is well known that atopics may be more sensitive to irritants and thus more frequent live the work place (Blomqvist et al. 2005).
In this study, the welders were exposed to low to moderate concentrations of RD while their exposures to irritating gases were low. However, the welders had nevertheless a high frequency of work-related symptoms. An epidemiologic study reported that exposure to Mn concentrations only 10–50 times higher than normal urban concentrations of Mn might cause adverse respiratory effects (Sarić and Piasek 2000). Two other studies found that Mn exposed workers had significantly higher prevalence of airways symptoms than the controls (Roels et al. 1987; Boojar and Goodarz 2002). Thus, it is the possibility that the Mn exposure that contributes and causes the work-related symptoms is reported by the welders in this study. Another possibility is that the actual particle concentrations themselves that cause irritations in the airways. However, this needs to be further investigated.
Welding fume
Although some of the welders’ exposure to RD was above the OEL, this study has shown that the main concern regarding exposure is to Mn. The fact that more than 50 % of the measured Mn concentrations exceeded the OEL for Mn is unacceptable. The majority of the welders worked without PAPRs (60 %). For the welders who used PAPRs (40 %), the PEMs were performed outside PAPR, and thus, their actual exposures to Mn and RD were of course lower than reported. The results are, however, not surprisingly high as earlier studies have measured Mn exposure during GMAW and AM/GM of Mn concentration between 0.07 and 0.5 mg/m3 (Smargiassi et al. 2000; Susi et al. 2000; Korczynski 2000; Wallace et al. 2001; Ellingsen et al. 2006). There are therefore concerns for adverse health effects caused by both Mn exposure, e.g., neurotoxical effects, and carcinogenic effect due to exposure to welding fumes.
The correlation between welding fume measured as RD and respirable Mn was very strong (Fig. 1). A similar correlation between the two has also recently been presented by Lehnert et al. (2012).
Mn is always used as an alloy in mild steel to improve the metallurgical properties, e.g., the strength of the steel, ductility (Taube 2013). The Mn content in mild steel is usually between 0.6 and 2.0 %, and GMAW in mild steel produces the oxides MnO(s), MnO2(s), and Mn2O4(s) (IVL 2006; Taube 2013). Mn has a lower boiling point compared with Fe and is therefore more concentrated in the welding fume, which means that the Mn concentration in the welding fume is higher than the concentration in the electrode (Ewing and Harris 2005). According to our results, the mass-based content of Mn in the welding fumes was in average 7 %. A similar mass-based Mn content in the welding fume (7 %) was also found by Schoonover et al. (2011).
The high correlation makes it possible to back calculate exposure levels between Mn and RD in these environments. For example, a welding fume exposure of RD at the same level as the Swedish OEL (5 mg/m3) will correspond to an air concentration of respirable Mn of approximately 0.4 mg/m3, which is a Mn exposure that strongly exceeds the Swedish OEL for Mn (0.1 mg/m3). To not exceed the OEL for Mn, the RD must be lower than 1.4 mg/m3. In the field of occupational hygiene, it is a general recommendation to have some margin to the OEL since the exposure varies between day-to-day. It is often assumed that exposures below one-third of the OEL mean that the used control measures are probably good enough (HSE 2006). In this case, it equals an Mn value of 0.03 mg/m3, and by utilizing the correlation between respirable Mn and RD, a corresponding RD concentration of 0.6 mg/m3 could be calculated (approximately equal to the 20th percentile of the RD data).
During the three sampling periods, four companies (no. 2, 5, 7, 11) each reported once the production level to be lower than normally during the measurement. Of course, the study aimed to sample during normal production conditions, but sometimes reduced production level could not be avoided. For three of the companies (no. 2, 5, 11), the production level was found to be reduced during the sampling period since the GM was lower (28–51 %) compared with the GMs from the other two sampling periods in the company. However, it was only in 9 % of the exposure measurements that were affected by reduced production level at the company. We assess the welding exposure in the total study to only be marginally affected by this production reduction.
Technically, the Mn exposure could be reduced and controlled by use of control measures, e.g., general mechanical ventilation and LEV. It was recently suggested that 40–50 % or more of the exposure was reduced with LEV compared with natural ventilation (Meeker et al. 2007; Flynn and Susi 2012; Lehnert et al. 2012). We observed that at least two companies (no. 4, 5) let their welders use PAPRs to reduce the occupational exposure to welding fumes instead of use of LEV (Table 2). However, PAPRs only reduce the air concentrations of welding fume in the breathing zone of the welders. Another common observed welding situation was incorrect use of the LEV by placing it in a position too far away from the welding point which resulted in that the welding fume comes into the welders breathing zone (IVL 2006). This was more common when manufacturing larger objects. In some of the studied companies (no. 5, 6, 8), the general ventilation systems were insufficient to ventilate out the emitted welding fumes. In practice, this means that many welders get exposed to unnecessary high concentrations of welding fumes. According to the traditional hierarchy of risk controls, PPE should be the last control measure to use. Control measures such as elimination and engineering controls are more effective and protective than PPE. Therefore, to reduce or control the exposure to welding fumes, the companies need both general mechanical ventilation and LEV. The welders also need to be trained to use the LEV correctly.
Approximately 40 % of the monitored welders used PPE. PAPRs supply filtrated clean air in the breathing zone of the welder and according to the suppliers of PAPRs the protection factor is 50, which in theory means a 50 times lower concentration in the air in the breathing zone compared with the surrounding workplace air. However, our study indicated that welding with PAPRs did not protect the welders to the extent of the assigned protection factor due to individual factors such as work practice. During the PEMs, we often observed that welders opened up the PAPRs directly after welding to be able to visually inspect the welding point. However, directly after welding, the concentration of welding fume is still high in the breathing zone. Thus, since the PAPRs were opened up quite frequently during welding, the welders were thereby exposed to welding fumes and do not get the high protection that correct use of PAPRs could offer. The correct way would have been to only open up the welding shields and keep the PAPRs on. Thus, in practice the WPF might be lower than the assigned one.
Since the PEMs were performed in the breathing zone, which in practice means air sampling at the welders shoulders, the exposure for those welders using PAPRs is overestimated. The correct way would have been to sample the air inside the PAPRs. However, when the PEMs were performed, no minimized filter cassettes were available, and the used 37-mm sampling cassettes were too big to be placed inside the PAPRs. Of practical reason, all air samples were collected in the breathing zones. However, since we did the parallel exposure measurements at one welder and one “dummy” PAPR, we could estimate the WPFs to be between 3 and 20. We believe that the parallel measurement performed at the welder more reflects the WPF for welders, and our estimation agrees with what other studies also reported. Han (2002) reported the WPF for filtering half-masks used by welders to be between 2 and 133 with a GM of 16. Measurements of Fe oxide fumes were 36–71 % lower inside the helmet compared with the outside (Goller and Paik 1985). Another study reported of WPF to range from 5 to 753 for, e.g., exposure to Fe (Janssen et al. 2007).
Air sampling of ozone was done parallel with the RD. The measured concentrations were low, and approximately 90 % of the samples had an ozone concentration below 10 % of the Swedish OEL. This is in coherence with earlier reported studies, i.e., Schoonover et al. (2011) showed that the ozone exposure was approximately 0.02 mg/m3 (GM) during GMAW. In 2 % of the samples, the OEL was exceeded. The ozone exposure might probably be short peak exposures during welding, and this type of intermittent exposure cannot be monitored with filter sampling methods, but instead direct-reading instruments are needed.
During some specific welding processes, NO2 can be emitted. At two of the companies, orientating measurements of NO2 were preformed, but only very low concentrations were measured.
Repeated PEMs of different occupational exposures have shown that the variability can be high in both within workers over time and between workers in the same occupation (Peretz et al. 1997; Rappaport et al. 1999; Wambach 2002). The manufacturing companies included in this study produced very different products and that is likely the explanation why the between-company variability was high. Also the within-worker variability was high and can be due to different types of work tasks during a day or on different days (Liu et al. 2011). In practice, it means that the welders had non-uniform exposures, and this is especially true for the welders working at companies producing larger products such as vehicles. Jobs with non-uniform exposures can be explained by individual variables such as work tasks, equipment, ventilation, location, and practices (Rappaport et al. 1999). The between-worker variability among the welders was lower (Table 7). Thus, it seems like many of the welders in the study had similar work tasks. According to Liu et al. (2011), between-worker variability is likely to result from personal environments, e.g., location, type of equipment and specialized work activities. Knowledge about how the occupational exposure to welding fume varies is important and can be especially essential for strategies of PEMs.
Conclusions
Welders in the Swedish manufacturing industry had a high prevalence of work-related symptom from the airways and eyes although the exposure levels generally did not exceed the current Swedish OEL except for Mn. Since the exposure to irritating gases was low and the exposure to RD was low to moderate in concentration, the work-related symptoms were probably related to the high exposure to Mn. The welders’ exposure to Mn was very high since more than 50 % of the measured Mn concentrations in air exceeded the OEL for Mn which is unacceptable. Based on the high frequency of work-related symptom, the OEL to Mn might need to be lowered. To reduce the exposure to welding fume, hierarchy of risk controls must be applied. Technical improvements in the welding workshops are needed. Control measures such as general mechanical ventilation and LEV must be used to be able to efficiently eliminate the welding fume and thereby control and reduce exposure.
References
Antonini JM (2003) Health effects of welding. Crit Rev Toxicol 33:61–103
Antonini JM, Santamaria AB, Jenkins NT, Albini E, Lucchini R (2006) Fate of manganese associated with the inhalation of welding fumes: potential neurological effects. Neurotoxicology 27:304–310
Beckett WS (1996) Industries associated with respiratory diseases. In: Harber P, Schenker MB, Balmes JR (eds) Welding: occupational and environmental respiratory diseases. Mosby, St. Louis, pp 704–717
Blomqvist A, Duzakin-Nystedt M, Ohlson CG, Andersson L, Jönsson B, Nielsen J, Welinder H (2005) Airways symptoms, immunological response and exposure in powder painting. Int Arch Occup Environ Health 78:123–131
Boelter FW, Simmons CE, Berman L, Scheff P (2009) Two-zone model application to breathing zone and area welding fume concentration data. J Occup Environ Hyg 6:298–306
Boojar MM, Goodarz F (2002) A longitudinal follow-up of pulmonary function and respiratory symptoms in workers exposed to manganese. J Occup Environ Med 44:282–290
Bowler RM, Roels HA, Nakagawa S, Drezgic M, Diamond E, Park R et al (2007) Dose-effect relationships between manganese exposure and neurological, neuropsychological and pulmonary function in confined space bridge welders. Occup Environ Med 64:167–177
Drexler H, Schaller KH, Nielsen J, Weber A, Weihrauch M, Welinder H, Skerfving S (1999) Efficacy of measures of hygiene in workers sensitised to acid anhydrides and the influence of selection bias on the results. Occup Environ Med 56:202–205
Ellingsen DG, Dubeikovskaya L, Dahl K, Chashchin M, Chashchin V, Zibarev E, Thomassen Y (2006) Air exposure assessment and biological monitoring of manganese and other major welding fume components in welders. J Environ Monit 8:1078–1086
Ewing W, Harris M (2005) Manganese and welding fume. The AIH Diplomate, issue 05–2
Ferris BG (1978) Epidemiology standardization project (American thoracic society). Am Rev Respir Dis 118:1–120
Fitsanakis VA, Au C, Erikson KM, Aschner M (2006) The effects of manganese on glutamate, dopamine and gamma-aminobutyric acid regulation. Neurochem Int 48:426–433
Flynn MR, Susi P (2010) Manganese, iron, and total particulate exposures to welders. J Occup Environ Hyg 7:115–126
Flynn MR, Susi P (2012) Local exhaust ventilation for the control of welding fumes in the construction industry—a literature review. Ann Occup Hyg 56:764–776
Furbee B (2011) Welding and parkinsonism. Neurol Clin 29:623–640
Goller JW, Paik NW (1985) A comparison of iron oxide fume inside and outside of welding helmets. Am Ind Hyg Assoc J 46:89–93
Han D-H (2002) Correlations between workplace protection factors and fit factors for filtering facepieces in the welding workplace. Ind Health 40:328–334
Hobson A, Seixas N, Sterling D, Racette BS (2011) Estimation of particulate mass and manganese exposure levels among welders. Ann Occup Hyg 55:113–125
HSE (2006) Exposure measurement: air sampling. COSHH essentials general guidance G409. Health and safety executive, London. Available as http://www.hse.gov.uk/pubns/guidance/g409.pdf. Accessed 27 Nov 2012
IARC (1990) Monographs on evaluation of carcinogenic risks to humans. Vol. 49: chromium, nickel and welding. IARC Press, Lyon, France
Isaxon C, Dierschke K, Pagels J, Löndahl J et al (2013) A novel system for source characterization and controlled human exposure to nanoparticle aggregates generated during gas–metal arc welding. Aerosol Sci Technol 47:52–59
IVL Svenska Miljöinstitutet AB (2006) Krom och mangan vid svetsning—exponering och behov av åtgärder. IVL Rapport B1675. [Swedish Environmental Research Institute (2006) Chromium and manganese during welding–exposure and need of measures]
Janssen LL, Nelson TJ, Cuta KT (2007) Workplace protection factors for an N95 filtering facepiece respirator. J Occup Environ Hyg 4:698–707
Jönsson LS, Nielsen J, Broberg K (2011) Gene expression analysis in induced sputum from welders with and without airway-related symptoms. Int Arch Occup Environ Health 84:105–113
Jönsson LS, Tinnerberg H, Jacobsson H, Andersson U, Axmon A, Nielsen J (2013) Exposure to particles and ocular symptoms in welders. A study of dose-response relationship. Int Arch Occup Environ Health (in preparation)
Klos KJ, Chandler M, Kumar N, Ahlskog JE, Josephs KA (2006) Neuropsychological profiles of manganese neurotoxicity. Eur J Neurol 13:1139–1141
Korczynski RE (2000) Occupational health concerns in the welding industry. Appl Occup Environ Hyg 15:936–945
Larsson B, Karlsson J-E, Nielsen J (2007) Respiratory and ocular symptoms in workers exposed to potassium aluminium-tetrafluoride soldering flux. Int Arch Occup Environ Health 80:627–633
Lehnert M, Pesch B, Lotz A et al (2012) Exposure to inhalable, respirable, and ultrafine particles in welding fume. Ann Occup Hyg 56:557–567
Liu SA, Hammond SK, Rappaport SM (2011) Statistical modeling to determine sources of variability in exposures to welding fumes. Ann Occup Hyg 55:305–318
Meeker JD, Susi P, Flynn MR (2007) Manganese and welding fume exposure and control in construction. J Occup Environ Hyg 4:943–951
Nemery B (1990) Metal toxicity and the respiratory tract. Eur Respir J 3:202–219
Peretz C, Goldberg P, Kahan E, Grady S, Goren A (1997) The variability of exposure over time: a prospective longitudinal study. Ann Occup Hyg 41:485–500
Rappaport SM, Weaver M, Taylor D et al (1999) Application of mixed models to assess exposures monitored by construction workers during hot processes. Ann Occup Hyg 43:457–469
Roels H, Lauwerys R, Buchet JP, Genet P, Sarhan MJ, Hanotiau I, de Fays M, Bernard A, Stanescu D (1987) Epidemiological survey among workers exposed to manganese: effects on lung, central nervous system, and some biological indices. Am J Ind Med 11:307–327
Sarić M, Piasek M (2000) Environmental exposure to manganese and combined exposure to gaseous upper respiratory irritants: mechanism of action and adverse health effects. Rev Environ Health 15:413–419
Schoonover T, Conroy L, Lacey S, Plavka J (2011) Personal exposure to metal fume, NO2, and O3 among production welders and non-welders. Ind Health 49:63–72
Sferlazza SJ, Beckett WS (1991) The respiratory health of welders. Am Rev Respir Dis 143:1134–1148
Sharifian SA, Loukzadeh Z, Shojaoddiny-Ardekani A, Aminian O (2011) Pulmonary adverse effects of welding fume in automobile assembly welders. Acta Med Iran 49:98–102
Smargiassi A, Baldwin M, Savard S, Kennedy G, Mergler D, Zayed J (2000) Assessment of exposure to manganese in welding operations during the assembly of heavy excavation machinery accessories. Appl Occup Environ Hyg 15:746–750
Susi P, Goldberg M, Barnes P et al (2000) The use of a task-based exposure assessment model (T-BEAM) for assessment of metal fume exposures during welding and thermal cutting. Appl Occup Environ Hyg 15:26–38
Swedish Work Environment Authority (2011) AFS 2011:18. Occupational exposure limits, Stockholm
Taube F (2013) Manganese in occupational arc welding fumes–aspects on physicochemical properties, with focus on solubility. Ann Occup Hyg 57:6–25
Temel O, Sakar Coşkun A, Yaman N, Sarioğlu N, Alkaç C, Konyar I, Ozgen Alpaydin A, Celik P, Cengiz Ozyurt B, Keskin E, Yorgancioğlu A (2010) Occupational asthma in welders and painters. Tuberk Toraks 58:64–70
Wallace M, Shulman S, Sheehy J (2001) Comparing exposure levels by type of welding operation and evaluating the effectiveness of fume extraction guns. Appl Occup Environ Hyg 16:771–779
Wambach PF (2002) Variation in exposure levels for high hazard frequently monitored agents. AIHA J 63:421–429
Wastensson G, Sällsten G, Bast-Pettersen R, Barregard L (2012) Neuromotor function in ship welders after cessation of manganese exposure. Int Arch Occup Environ Health 85:703–713
Wolf C, Pirich C, Valic E, Waldhoer T (1997) Pulmonary function and symptoms of welders. Int Arch Occup Environ Health 69:350–353
Zeidler-Erdely PC, Erdely A, Antonini JM (2012) Immunotoxicology of arc welding fume: worker and experimental animal studies. J Immunotoxicol 9:411–425
Zimmer AT, Biswas P (2001) Characterization of the aerosols resulting from arc welding processes. J Aerosol Sci 32:993–1008
Acknowledgments
We would like to thank Ulf Bergendorf, Occupational and Environmental Medicine, for help with the personal exposure measurements. The study was funded by the Swedish Council for Working Life and Social Research (FAS).
Conflict of interest
All authors state no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hedmer, M., Karlsson, JE., Andersson, U. et al. Exposure to respirable dust and manganese and prevalence of airways symptoms, among Swedish mild steel welders in the manufacturing industry. Int Arch Occup Environ Health 87, 623–634 (2014). https://doi.org/10.1007/s00420-013-0896-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-013-0896-3