
Abstract
Purpose
To reduce the socio-economic burden of persistent low back pain (LBP), factors influencing the progression of acute/subacute LBP to the persistent state must be identified at an early stage.
Methods
Prospective inception cohort study of patients attending a health practitioner for their first episode of acute/subacute or recurrent LBP. Patients were assessed at baseline addressing occupational, psychological, biomedical and demographic/lifestyle factors and followed up over 6 months. Multivariate logistic regression analysis was performed separately for the variables groups of the four different domains, controlling for age, gender and body mass index. The overall predictive value was calculated for the full regression models of the different domains. Finally, all significant variables from the different domains were combined into a final predictor model.
Results
The final four-predictor model predicted 51 % of variance of persistent LBP and included ‘resigned attitude towards the job’ (OR 1.73; 95 % CI 1.16–2.59), ‘social support at work’ (OR 0.54; 95 % CI 0.32–0.90), ‘functional limitation’ (OR 1.05; 95 % CI 1.01–1.10) and ‘duration of LBP’ (OR 1.04; 95 % CI 1.02–1.06). The accuracy of the model was 83 %, with 92 % of non-persistent and 67 % of persistent LBP patients correctly identified.
Conclusions
In this study of patients with acute/subacute LBP, ‘resigned attitude towards the job’ increased the likelihood of persistent LBP at 6 month. Addressing this factor with workplace interventions has the potential to modify the outcome. In patients experiencing ‘social support at work’, the development of persistent LBP was less likely and might therefore be considered as potential resource for prevention of persistent LBP.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Socio-economic costs of persistent low back pain (LBP) exceed the costs of acute and subacute LBP by far (Katz 2006). This makes the early identification of patients at risk of developing persistent LBP essential, especially in working populations (Hilfiker et al. 2007). According to the bio-psycho-social model, the differentiation into risk versus protective factors for the development of persistent LBP should be considered (Heneweer et al. 2007; Steenstra et al. 2005). Thereby, modifiable risk and protective factors could be addressed proactively to limit the associated socio-economic burden.
The Multinational Musculoskeletal Inception Cohort Study (MMICS) Statement recommends internationally accepted measures (Pincus et al. 2008). Among these measures, occupational factors have the highest reliability according to a recently published review on prognostic factors for persistent LBP (Melloh et al. 2009) and are important modifiable factors that can be addressed proactively. Consequently, this study focused on occupational factors and additionally other possible psychological, pain/functional limitation and health behaviour influences that have been found in multiple previous studies to be modifiable factors for the development of persistent LBP.
Following the MMICS recommendations that only those variables that scored highest in this consensus statement of experts in the field should be part of a minimum set of prognostic measures, we hypothesised that:
-
1.
Factors such as resigned attitude towards the job would be occupational risk factors (H1a), depression a psychological risk factor (H1b), with further risk factors for developing persistent LBP being functional limitation, higher age and high body mass index (H1c);
-
2.
Social support at work would be an occupational protective factor (H2a), with further protective factors for developing persistent LBP being good physical and mental health status, and being physically active (H2b).
The aim of this study was to identify those risk and protective factors that increase or decrease the likelihood of patients with an episode of acute LBP to progress to the persistent state.
Method
Our study has been approved by the local Lower South Regional Ethics Committee (LRS/08/03/008). All participants gave their informed consent prior to their inclusion in the study. The protocol for our study has been published previously (Melloh et al. 2008).
An inception cohort of 315 patients in primary care settings was recruited consecutively from 14 health practitioners across New Zealand. Participants were asked to take part in the study when attending a health practitioner for their first episode of acute/subacute LBP or for recurrent LBP. The latter was defined according to Stanton et al. (2011) as LBP with a least 30 LBP-free days between two episodes and exceeding 20 out of 100 points on the Visual Analogue Scale (VAS).
To be eligible, patients had to be between 18 and 65 years of age, be able to read and write in English, and provide written consent. Patients were excluded if they had chronic LBP (defined as LBP continuing for more than 12 weeks at the time of the first visit to a health practitioner) (Airaksinen et al. 2006; Balague et al. 2007), specific LBP (infection, tumour, osteoporosis, ankylosing spondylitis, fracture, deformity, inflammatory process, cauda equina syndrome) (van Tulder et al. 2006), a severe comorbidity determining overall well-being (e.g. painful disabling arthritic hip joints) and were pregnant or unwilling to complete questionnaires.
Potential participants were screened by a research nurse employing a standardised structured telephone interview. If eligible, patients were sent a baseline questionnaire by mail and asked to return it within 1 week. Possible prognostic factors for persistent LBP were measured by these patient-reported outcome questionnaires. Follow-up questionnaires were sent out after 3, 6, 12 weeks and 6 months. If not returned, a reminder was sent out after 1 and 2 weeks. As compensation for their time, participants received $NZ10 vouchers for each returned questionnaire. Baseline and follow-up questionnaires were based on the recommendations of the MMICS Statement (Pincus et al. 2008) addressing occupational (work dissatisfaction, a resigned attitude towards the job, job insecurity, concentration requirements, work organisational problems and interruptions, time pressure, emotion suppression, social support at work, job control, physically demanding occupation, educational status), psychological (depression, somatisation, fear avoidance, catastrophising) and additional (pain and duration of LBP, radiating pain below the knee, functional limitation, physical and mental health status, age, body mass index, smoking, and physically active) risk factors for the development of persistent LBP and resources preventing persistent LBP. Occupations were dichotomised into physically demanding and non-demanding. We coded agricultural or fishery worker, craft or trades worker, plant/machine operator or assembler, elementary worker and armed forces as physically demanding. Legislator/senior official/manager, professional, technician, clerk and service/sales persons were coded as non-demanding occupations.
Statistical analysis
Patients with persistent LBP at 6-month follow-up were compared to patients with non-persistent LBP. Persistent LBP was defined by an Oswestry Disability Index (ODI) score at baseline and 6 month >10 points (Ostelo et al. 2008) and an ODI change score ≤10 points between baseline and 6-month follow-up. Ten points are considered to be the minimal clinically important difference (MCID) of the ODI (Ostelo et al. 2008). The normal value for the ODI in a general population is ten points (Fairbank and Pynsent 2000). Therefore, patients with an ODI score ≤10 points at 6-month follow-up were considered to be non-persistent.
After initial screening of potential predictor variables following the literature, first, univariate logistic regression analyses and then multivariate logistic regression analyses were performed separately for the variables groups of four different domains occupational, psychological, pain/functional limitation and demographic/health behaviour, controlling for age, gender and body mass index. The overall predictive value was calculated for the full regression models of the different domains. Finally, all significant variables from the different domains were combined into a final predictor model. Data were analysed using IBM SPSS Statistics 19 (IBM Corp., Armonk, NY, USA). Statistical significance was set at the p < 0.05 level, two-tailed.
Results
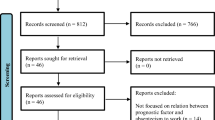
In total, 562 patients suffering from acute or subacute LBP were screened consecutively from April 2008 until October 2010. One hundred and twenty-four patients were found ineligible because they were either LBP-free at the time of the screening interview (ten), had chronic LBP for more than 12 weeks (93) or specific LBP (eight), had osteoarthritis of the hip or knee joint (two), were pregnant (three), were not available for follow-ups (two) or were above 65 years of age (six). Twenty-six patients decided not to participate, and 97 did not return the baseline questionnaire in spite of two reminders. Three hundred and fifteen patients were enrolled: 146 patients were lost to follow up and 169 patients participated over the 6-month period. Baseline characteristics of the participants and the individuals lost to follow up are shown in Table 1. Those individuals lost to follow up showed a significantly lower mental health measured by the SF-12 Mental Component Scale, a higher depression score on the Zung self-rating depression scale and a higher affective pain score measured by the McGill Pain Questionnaire. All other baseline characteristics did not demonstrate any significant difference.
One hundred and five patients at 6-month follow-up were classified as non-persistent, 64 (38 %) as persistent. ODI scores in the non-persistent LBP group decreased over time, whereas scores in the persistent LBP group remained at the same level (Fig. 1). ODI baseline scores in the non-persistent group ranged between 0 and 62 points (mean = 16.9 points), scores in the persistent group between 12 and 60 points (mean = 27.1 points), revealing a higher functional limitation at baseline for the persistent LBP group based on differences in means (p < 0.001).

ODI score change in persistent and non-persistent LBP group
Taking into account all five measurement points between baseline and 6-month follow-up, the trend analysis confirmed a decline of the ODI over time for the non-persistent group. This was a first-order trend with a linear decrease over all five time points. In the persistent group, no first-order trend for the ODI over time could be demonstrated (Fig. 1).
In the univariate logistic regression analyses, the odds of having persistent LBP at 6-month follow-up were 1.60 for a resigned attitude towards the job at baseline (95 % CI 1.24–2.08), 0.54 for social support at work (95 % CI 0.37–0.80) and 0.74 for job satisfaction (95 % CI 0.57–0.96) (Table 2). In the multivariate analyses, the odds were 1.83 for a resigned attitude towards the job (95 % CI 1.23–2.72) and 0.44 for social support at work (95 % CI 0.26–0.75) but were not significant for job satisfaction (Table 3). There was no correlation between persistent LBP and a physically demanding occupation or the educational status. A chi-squared test of the full occupational predictor model was significant (χ2 = 36.3, df = 16, p < 0.01; Table 3). Occupational factors and control variables predicted 33 % variance in persistent LBP. The lack of significance of the chi-squared Hosmer–Lemeshow test indicated that the occupational predictor model has a good fit for the data. The accuracy of the model was 71 % with 83 % of non-persistent and 51 % of persistent LBP patients correctly identified.
The odds of having persistent LBP in the univariate analyses at 6-month follow-up were 1.08 for depression at baseline (95 % CI 1.04–1.12), 1.11 for somatisation (95 % CI 1.04–1.12) and 1.05 for catastrophising (95 % CI 1.01–1.08) (Table 2). The odds of having persistent LBP in the multivariate analyses were 1.06 for depression (95 % CI 1.02–1.11) but were not significant for somatisation and catastrophising. A chi-squared test of the full psychological predictor model was significant (χ2 = 30.7, df = 8, p < 0.01; Table 3). Psychological factors and control variables predicted 24 % variance in persistent LBP. The lack of significance of the chi-squared Hosmer–Lemeshow test indicated that the psychological predictor model has a good fit for the data. The accuracy of the model was 71 with 85 % of non-persistent and 48 % of persistent LBP patients correctly identified.
In the univariate logistic regression analyses, the odds of having persistent LBP at 6-month follow-up were 1.07 for functional limitation at baseline (95 % CI 1.03–1.10), 1.03 for duration of LBP (95 % CI 1.01–1.04), 1.03 for sensory pain (95 % CI 1.01–1.05), 1.07 for affective pain (95 % CI 1.02–1.12), 1.02 for pain intensity (95 % CI 1.00–1.03) and 0.94 for mental health (95 % CI 0.91–0.98) (Table 2). In the multivariate analyses, the odds were 1.09 for functional limitation (95 % CI 1.03–1.15) and 1.03 for duration of LBP (95 % CI 1.02–1.05) but not significant for all other variables. A chi-squared test of the full pain/functional limitation predictor model was significant (χ2 = 48.7, df = 12, p < 0.001; Table 3). Pain/functional limitation factors and control variables predicted 37 % variance in persistent LBP. The lack of significance of the chi-squared Hosmer–Lemeshow test indicated that the pain/functional limitation predictor model has a good fit for the data. The accuracy of the model was 78 % with 90 % of non-persistent and 58 % of persistent LBP patients correctly identified.
The odds of having persistent LBP in the univariate analysis at 6-month follow-up were 1.08 for a high body mass index at baseline (95 % CI 1.02–1.14; Table 2) but not significant in the multivariate analysis.
When combining all significant variables from the different domains into one model, a final four-predictor model was found significant comprising resigned attitude towards the job, social support at work, functional limitation and duration of LBP ((χ2 = 64.1, df = 8, p < 0.001; Table 4). All factors and control variables predicted 51 % variance in persistent LBP. The lack of significance of the chi-squared Hosmer–Lemeshow test indicated that this final predictor model has a good fit for the data. The accuracy of the model was 83 % with 92 % of non-persistent and 67 % of persistent LBP patients correctly identified (Table 4).
Discussion
This study focused on occupational, psychological, pain/functional limitation and demographic/health behaviour risk factors for the development of persistent LBP and resources preventing persistent LBP 6 months after an acute/subacute episode of LBP in a primary care setting. It is centred on widely used validated assessment instruments suggested by the MMICS Statement.
Resigned attitude towards the job was found to be an occupational risk factor for the development of persistent LBP at 6-month follow-up. Social support at work demonstrated to be a protective factor, meaning that development of persistent LBP was less likely.
Resigned attitude towards the job is understood as a defensive, resentful adaptation to working conditions that are not optimal (Kälin et al. 2000; Semmer 2003). Mannion and Elfering could show in their systematic review (Mannion and Elfering 2006) that a resigned attitude towards the job comprises job continuation in spite of dissatisfaction; the belief that the present situation should be accepted as potential other jobs could be worse; and that there are limited expectations for an employee. Job-related resignation could be shown to correlate with functional limitation according to a study by (Schade et al. 1999). In this study, job-related resignation explained 12 % of variance of functional limitation in activities of daily living. These findings concur with our results, showing that a resigned attitude towards the job is a strong occupational risk factor that should be taken into consideration in workplace interventions for individuals suffering from an episode of acute or subacute LBP. In a study on employees of a municipal office undergoing technological change, Elfering et al. (2010) demonstrated that employees with possibilities of a higher participation during this change suffered less frequently from episodes of LBP. Therefore, primary and secondary prevention of occupational LBP should adhere to the principle of participation in job design.
Social support at work comprises emotional support and assistance by both colleagues and supervisors (Semmer and Udris 2007). This study does not distinguish between different types of social support at work, that is, between the social support at work provided by colleagues or supervisors. A future study should differentiate between support providers as findings by (Elfering et al. 2002) suggest that provider-specific constellations of social support at work may have either a positive or a negative influence on the development of LBP. In addition to a direct protective effect on the development of persistent LBP indicated by the present study, social support at work may also have a moderating effect, with its absence leading to a stronger correlation between risk factors and the development of persistent LBP (Semmer and Udris 2007).
In the present study, occupational risk and protective factors from hypotheses 1a and 2a could be confirmed which is consistent with results from (Elfering 2006), (Elfering and Mannion 2008) and (Linton 2001). However, findings from this study need to be considered in the context of its sample size. Although they should not be underestimated, stressor effects in the workplace are often moderate (Semmer and Udris 2007). Large workplace stressor effects would have been required in order to be observed in a study of this sample size.
Our results indicate a higher functional limitation and a longer duration of LBP at baseline to be risk factors for the development of persistent LBP (H1c). These factors show that current state of functional limitation and pain history are predictive for general practitioners.
The presented final four-predictor model comprising resigned attitude towards the job, functional limitation and duration of LBP as predictors for the development of persistent LBP and social support at work as predictive resource preventing the development of persistent LBP should be interpreted cautiously. This predictor model explained 51 % of variance of the development of persistent LBP, suggesting that there may be other predictive factors not identified in this study. The model has a good applicability to rule out patients with a low risk of developing persistent LBP (specificity 0.92) but is less appropriate to rule in patients with a high risk of developing persistent LBP (sensitivity 0.67) (Bossuyt et al. 2004).
A limitation of this study is that about one-third of patients developing persistent LBP were not correctly identified in the final four-predictor model. Also, that we did control for age, gender and body mass index but not for smoking in order not to lose too many cases due to the many missings for the variable smoking. Furthermore, the predominant use of patient-reported outcome measures for generating information is subjective by nature. Finally, attrition bias can be seen as a threat to the representativeness of the study sample. However, a recent study found that attrition has only marginal influence on the point estimates of LBP-related outcomes (Schmidt et al. 2011). In the present study, the loss-to-follow-up was consistently about 15 % at each follow-up time point. This means that this loss was a systematic one and not due to any specific event. The total loss-to-follow-up was 46 % over the whole study period. This apparently high rate should be considered in the context of a postal survey, where direct contact with the participants was limited to the initial screening interview. A recent study on 342 LBP patients presenting in primary care was followed up six times over a 6-month period and showed a comparable loss-to-follow-up of 45 % (Dunn et al. 2006).
A strength of the present study is that only validated and common instruments were used. Consistent use of outcome measures recommended by the MMCIS Statement will facilitate comparison of results with other studies. A further strength is that baseline characteristics of participants and individuals lost to follow up did not show significant differences, except for a lower mental health, and higher depression and affective pain scores for those individuals lost to follow up. This is typical for study populations where the healthier individuals stay in the study. Without this bias, the predictive value of the psychological factors would have been even higher because of variance restriction in the criterion.
Implications for practice
Findings from this study confirm the requirement for measurement of occupational factors in screening tools for patients at risk of developing persistent LBP. Predictors easily identified with use of widely available screening tools will facilitate the provision of necessary treatment to reduce the societal and financial burden of persistent LBP and avoid major loss in enjoyment of life. The benefit of including modifiable risk factors such as a resigned attitude towards the job and modifiable protective factors such as social support at work in screening tools is that these factors can be addressed in primary and secondary prevention, for example, in workplace intervention.
Conclusions
In this study of patients with acute/subacute LBP from a primary care setting, resigned attitude towards the job increased the likelihood of persistent LBP at 6 month. Addressing this factor with workplace interventions has the potential to modify the outcome. In patients experiencing social support at work, the development of persistent LBP was less likely. Social support at work might therefore be considered as a potential resource for prevention of persistent LBP. Further research is required to investigate different types of social support at work regarding their prognostic influence on the development of persistent LBP.
References
Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, Mannion AF, Reis S, Staal JB, Ursin H, Zanoli G (2006) Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J 15 Suppl 2:S192–S300
Balague F, Mannion AF, Pellise F, Cedraschi C (2007) Clinical update: low back pain. Lancet 369(9563):726–728
Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwig LM, Lijmer JG, Moher D, Rennie D, de Vet HC (2004) Towards complete and accurate reporting of studies of diagnostic accuracy: the STARD initiative. Fam Pract 21(1):4–10
Dunn KM, Jordan K, Croft PR (2006) Characterizing the course of low back pain: a latent class analysis. Am J Epidemiol 163(8):754–761
Elfering A (2006) Work-related outcome assessment instruments. Eur Spine J 15(Suppl 1):S32–S43
Elfering A, Mannion AF (2008) Epidemiology and risk factors of spinal disorders. In: Boos N, Aebi M (eds) Spinal disorders—fundamentals of diagnosis and treatment. Springer, Berlin Heidelberg, New York, pp 153–173
Elfering A, Semmer NK, Schade V, Grund S, Boos N (2002) Supportive colleague, unsupportive supervisor: the role of provider-specific constellations of social support at work in the development of low back pain. J Occup Health Psychol 7(2):130–140
Elfering A, Dubi M, Semmer NK (2010) Participation during major technological change and low back pain. Ind Health 48(3):370–375
Fairbank JC, Pynsent PB (2000) The oswestry disability index. Spine 25(22):2940–2952 (discussion 2952)
Heneweer H, Aufdemkampe G, van Tulder MW, Kiers H, Stappaerts KH, Vanhees L (2007) Psychosocial variables in patients with (sub)acute low back pain: an inception cohort in primary care physical therapy in The Netherlands. Spine 32(5):586–592
Hilfiker R, Bachmann LM, Heitz CAM, Lorenz T, Joronen H, Klipstein A (2007) Value of predictive instruments to determine persisting restriction of function in patients with subacute non-specific low back pain. Systematic review. Eur Spine J 16(11):1755–1775
Kälin W, Semmer N, Elfering A, Tschan F, Dauwalder J, Heunert S, Crettaz F (2000) Work characteristics and well-being of Swiss apprentices entering the labor market. Swiss J Psychol 59(4):272–290
Katz JN (2006) Lumbar disc disorders and low-back pain: socioeconomic factors and consequences. J Bone Jt Surg Am 88(Suppl 2):21–24
Linton SJ (2001) Occupational psychological factors increase the risk for back pain: a systematic review. J Occup Rehabil 11(1):53–66
Mannion AF, Elfering A (2006) Predictors of surgical outcome and their assessment. Eur Spine J 15(Suppl 1):S93–S108
Melloh M, Aebli N, Elfering A, Roder C, Zweig T, Barz T, Herbison P, Hendrick P, Bajracharya S, Stout K, Theis JC (2008) Development of a screening tool predicting the transition from acute to chronic low back pain for patients in a GP setting: protocol of a multinational prospective cohort study. BMC Musculoskelet Disord 9:167
Melloh M, Elfering A, Egli Presland C, Roeder C, Barz T, Rolli Salathe C, Tamcan O, Mueller U, Theis JC (2009) Identification of prognostic factors for chronicity in patients with low back pain: a review of screening instruments. Int Orthop 33(2):301–313
Ostelo RW, Deyo RA, Stratford P, Waddell G, Croft P, Von Korff M, Bouter LM, de Vet HC (2008) Interpreting change scores for pain and functional status in low back pain: towards international consensus regarding minimal important change. Spine 33(1):90–94
Pincus T, Santos R, Breen A, Burton AK, Underwood M (2008) A review and proposal for a core set of factors for prospective cohorts in low back pain: a consensus statement. Arthritis Rheum 59(1):14–24
Schade V, Semmer N, Main CJ, Hora J, Boos N (1999) The impact of clinical, morphological, psychosocial and work-related factors on the outcome of lumbar discectomy. Pain 80(1–2):239–249
Schmidt CO, Raspe H, Pfingsten M, Hasenbring M, Basler HD, Eich W, Kohlmann T (2011) Does attrition bias longitudinal population-based studies on back pain? Eur J Pain 15(1):84–91
Semmer N (2003) Individual differences, work stress, and health. In: Schabracq M, Winnubst J, Cooper C (eds) Handbook of work and health psychology, 2nd edn. Wiley, Chichester, pp 83–120
Semmer NK, Udris I (2007) Bedeutung und Wirkung von Arbeit. In: Schuler H (ed) Lehrbuch Organsationspsychologie, 4th edn. Huber, Bern, pp 157–195
Stanton TR, Latimer J, Maher CG, Hancock MJ (2011) A modified Delphi approach to standardize low back pain recurrence terminology. Eur Spine J 20(5):744–752
Steenstra IA, Verbeek JH, Heymans MW, Bongers PM (2005) Prognostic factors for duration of sick leave in patients sick listed with acute low back pain: a systematic review of the literature. Occup Environ Med 62(12):851–860
van Tulder M, Becker A, Bekkering T, Breen A, del Real MT, Hutchinson A, Koes B, Laerum E, Malmivaara A (2006) Chapter 3. European guidelines for the management of acute nonspecific low back pain in primary care. Eur Spine J 15 Suppl 2:S169–S191
Acknowledgments
This research was funded by the Wishbone Trust of New Zealand, Wellington; Lottery Health Research, Wellington; the Bruce McMillan Trust, Dunedin; the Dunedin School of Medicine; realHealth International; and the University of Berne. MM was funded by a scholarship awarded by the University of Otago. We gratefully acknowledge Kirsten Stout from the Centre for Musculoskeletal Outcomes Research (CMOR) at Dunedin School of Medicine, University of Otago, for developing and maintaining the documentation and data management system.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Melloh, M., Elfering, A., Chapple, C.M. et al. Prognostic occupational factors for persistent low back pain in primary care. Int Arch Occup Environ Health 86, 261–269 (2013). https://doi.org/10.1007/s00420-012-0761-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-012-0761-9