
Abstract
Purpose
The study investigates the long-term effects of accumulated working conditions on depressive symptoms in junior doctors. Drawing on the Job Demand-Control-Support model, this study aims to identify personal and job-related determinants for self-reported depression in junior doctors—a professional group that is vulnerable to depression.
Methods
We conducted a prospective cohort study with measures of work characteristics and depressive symptoms over three time-points among hospital doctors during postgraduate specialty training in Germany. Participants were 415 junior doctors with full-time contract (47.5% women; mean age, 30.5 years). The outcome was depressive symptoms assessed with the Spielberger State-Depression Scale. Odds ratios (OR) were computed to analyse the cumulative effect of initial depressive symptoms scores, demographic variables, and working characteristics across T1 and T2 on subsequent depressive symptoms at T3.
Results
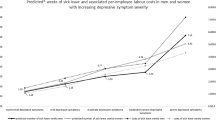
The percentage of junior doctors reporting depressive symptoms scores above a critical value varied between 12.0% at T1, 10.4% at T2, and 13.3% at T3; N = 34 doctors (8.19%) were classified as incident cases during the observation period. Elevated depressive symptoms at T3 were positively predicted by depressive symptoms scores across T1 and T2 (OR: 1.37; 95% confidence interval: 1.25–1.50) and negatively by professional tenure (0.54; 0.31–0.96), free weekends (0.52; 0.28–0.97), and job autonomy (0.35; 0.18–0.65).
Conclusions
After controlling for demographic and working time influences, findings suggest that junior doctors’ perceived job autonomy is negatively associated with future depressive symptoms. Enhancing job control emerges as a promising strategy to lower the risk of depression during first years of professional practice.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Depression is considerably more prevalent in young doctors than in the general population, especially during the first postgraduate years of training or residency in a hospital (West et al. 2006; Shanafelt et al. 2002; Tyssen and Vaglum 2002; Dyrbye et al. 2006). This partly explains the increased risk of suicide among medical doctors compared to other academic professionals (Frank et al. 2000; Schernhammer and Colditz 2004). Moreover, depressed doctors may be a hazard not only to themselves, but also to patient safety (Fahrenkopf et al. 2008; West et al. 2006). Less clear than its risks, however, are the job-related causes of depression in junior doctors.
The work–depression relationship in junior doctors
Recent meta-analyses in the general working population conclude that psychological work stressors, such as perceived high job strain (high demand, low control), effort–reward imbalance, and injustice, are all related to a moderately increased risk of depression, while psychological resources, such as job control and social support at work, are related to a lower risk (Stansfeld and Candy 2006; Bonde 2008; Netterstrom et al. 2008).
Work-related stress and long-term health-related outcomes among doctors have become an issue of growing concern (Arnetz 2001; Wallace et al. 2009). However, few studies have examined the specific situation of junior doctors during medical residency (Tyssen et al. 2000). Existing longitudinal studies on doctors remain inconclusive, yet indicate that overtaxing workload, time pressure, and lack of support from senior colleagues might be job-related factors contributing to depression (Tyssen and Vaglum 2002).
In this study, working conditions were conceptualized according to Karasek’s Job Demand-Control (JDC) model (Karasek 1979; Karasek and Theorell 1990). Originally, based on the two dimensions of job demands and job control (Karasek 1979), the model has later been extended to include social support as a third dimension, resulting in the Job Demand-Control-Support (JDCS) model (Johnson and Hall 1988; Johnson et al. 1989). A core assumption of the JDCS model is that a) high job demands, b) low job control, and c) lack of social support are work-related causes of impaired psycho-physical health and well-being. In addition to the direct effects of these three dimensions, the model also postulates interactive effects of working conditions. Job control and support are assumed to provide coping resources that moderate or buffer the potential health-impairing effects of job demands (Karasek and Theorell 1990; Johnson and Hall 1988; Johnson et al. 1989). Specifically, job control and social support are assumed to interact with job demands, such that low levels of control respectively exacerbate support (strain hypotheses), whereas high levels attenuate (buffer hypotheses) the detrimental effects of job demands. Accordingly, the most stressful working situations are characterized by high demands and low levels of both control and support (iso-strain hypothesis).
A large number of studies have used the JDC(S) model to investigate relationships between work characteristics and health-related outcomes. Most have found at least some support for main effects of JDC(S) dimensions on worker well-being. Evidence for interaction effects is less consistent. Out of 41 mostly cross-sectional JDC(S) studies reviewed by van der Doef and Maes (1999), 28 (68%) found support for two-way interactive effects of work characteristics on worker well-being in line with the model’s strain hypothesis. Focussing on high-quality longitudinal research, de Lange et al. (2003) noted that only 8 out of 19 (42%) methodologically rigorous prospective JDC(S) studies reported any significant two-way interactions. Empirical support for a three-way interaction in the sense of the iso-strain hypothesis was practically non-existent. Based on their literature review, de Lange et al. (2003) concluded that evidence for interactive effects of work characteristics is modest and have suggested new directions for research on the JDCS model. These include a stronger emphasis on time-lagged relationships, examination of the cumulative effects of exposure to work characteristics over time, and investigation of specific and contextually relevant health-related outcomes.
Taking into account the outlined developments in research on the JDCS model, the present study focussed on a longitudinal test of the cumulative main effects of job demands, control, and support on depressive symptoms in junior doctors. Mixed results regarding the (iso-)strain hypotheses notwithstanding, the three-dimensional taxonomy of work characteristics in the JDCS model has been shown to provide a fruitful approach to analysing the impact of work on employee well-being in healthcare settings (de Jonge et al. 1999; Söderfeldt et al. 1997) and, in particular, has been previously commended for studies on the aetiology of depressive symptoms (Griffin et al. 2007).
Follow-up studies and measures in research on work–depression relationships
Despite a recent growth in the number of longitudinal studies (e.g. de Lange et al. 2003), a majority of investigations on work stress and depression are still based on cross-sectional data. This limits validity of causal inferences and increases the risk of circular reasoning (Kasl 1998; Zapf et al. 1996). Consequently, follow-up studies are better suited to address the risk of developing depressive symptoms due to psychosocial factors in the working environment and add to the existing evidence regarding the prospective association between work and well-being (Bonde 2008).
The present study used a three-wave longitudinal design to investigate the cumulative impact of working conditions on depressive symptoms in junior hospital doctors over a period of almost 3 years. Repeated measurement of variables allows inferences on the causal relationship between work characteristics and subsequent depressive complaints (Zapf et al. 1996). Controlling for initial depressive problems is important as, after critically reviewing the literature, several authors concluded that observed relationships between work conditions and future depression might be biased due to a lack of control for minor depression at baseline (e.g. Bonde 2008).
As proposed by Netterstrom et al. (2008), job measures were selected to fit the specific working situation of junior doctors. Based on the JDCS model, the following three work characteristics were included: (a) work overload is a well-documented stressor for junior doctors and represents the demand side of the JDCS model (Chapman 2006; Biaggi et al. 2003); (b) autonomy is the core indicator for job control and essential for well-being at work (e.g. Karasek and Theorell 1990; Michie and Williams 2003; Thomas 2004; Bakker et al. 2005); (c) professional support is especially important for junior doctors in their postgraduate training, a phase in which it is crucial to receive performance feedback and develop competences (Arnetz 2001; Prins et al. 2007).
Drawing on core assumptions of the JDCS model, we hypothesize that junior doctors’ risk of developing elevated levels of depressive symptoms increases with the prolonged exposure to work overload and decreases with the enduring extent of job autonomy and availability of professional support. Additionally, the predictive value of interactive effects of work characteristics will be assessed.
Methods
Data collection procedure
Based on registration data of the Bavarian Chamber of Medical Doctors, 1,000 junior doctors (482 women, 518 men) in their second or third year of practical training (residency) were selected for inclusion in the study. All were working in direct patient care in hospitals in the wider area of Munich, Germany. Pre-coded questionnaires were mailed directly to prospective participants with self-addressed and stamped envelopes. The study was approved by the University Clinic’s internal review board, and voluntary participants signed a letter of informed consent. A priori, a 12-month time-lag was specified between T1 and T2, and an 18-month lag between T2 and T3. At each measurement point, two reminder letters were sent out and return periods were extended to increase survey participation. Average factual time-lags thus amounted to 14 and 19 months, and the final measurement at T3 took place 33 months after the baseline measurement at T1.
We focussed on junior doctors in their second or third year of medical residency to ensure that at the baseline measurement, all had already gained substantial work experience. The time-lag of the first follow-up was chosen as studies have shown that effects of work strain on depression manifest over a period of about 1 year (Tokuyama et al. 2003; Johnson et al. 1995; Kawakami et al. 1992). The last measurement point was timed to come close to the earliest possible end of junior doctors’ practical training in the hospitals, which takes about 5–6 years or longer, depending on the field of specialization. To assess the consequences of chronic work stress, we examined the cumulative effects of work conditions over a period of 1 year (i.e. T1 and T2 combined) on state depression at T3, that is, on average 2 years later (Cheng et al. 2000). This design and the chosen time-lags correspond with previous recommendations on studying longitudinal effects of work-related determinants on employee well-being (de Lange et al. 2003; Zapf et al. 1996).
Study population
In the first wave (T1), a total of 621 (62.1%) usable questionnaires were returned. The gender distribution (318 female, 303 male doctors) was balanced and did not differ significantly from the sample’s potential participants (χ² difference = 1.39, df = 1, n.s.). In the second wave (T2), 14 months later, identical questionnaires were sent to the same 621 participants. Of those, 561 (90.3%, 289 women and 272 men) were returned completed. At the final assessment (T3), 33 months after T1, questionnaires were sent to all T1-responders. Overall, 507 junior doctors participated in all three surveys repeatedly (247 men, 260 women).
Listwise deletion of missing data in core study variables excluded 42 participants. To obtain a homogeneous sample and address potential confounding influences of reduced working time, we excluded the small number of doctors who held part-time contracts at T1 (N = 19) or T2 (N = 31). Thus, our final sample consisted of N = 415 doctors (218 men, 197 women) working full-time (cf., Fig. 1—flow chart). At T1, the mean age was 30.5 years (SD = 2.7; women: M = 30.1, SD = 3.0; men: M = 30.8, SD = 2.4). Further sample characteristics (e.g. professional tenure, partnership) can be found in Table 1. Participants were employed as resident doctors (T1: 96.1%; T2: 89.6%; T3: 70.6%) or as resident doctors with supervision functions (T1: 3.9%; T2: 10.4%; T3: 29.4%). All medical specialties involved in patient care were represented; largest groups at T1 were internal medicine (28.2%), surgical medicine (13.5%), anaesthesia (11.6%), paediatrics (6.3%), and general medicine (6.0%).

Flow chart of follow-up
Survey measures
Demographic information
Dichotomous items assessed gender (1 = male, 2 = female) and partnership status (“Are you married or do you live with a partner?”; 1 = yes, 2 = no). Age and professional tenure were reported in years.
Working time
Participants were asked to state their average weekly working time (in hours) as well as their average number of free weekends (additionally specified as free Saturday and Sunday) per month.
Work characteristics
Three scales were drawn from an established German self-report instrument for analysing working conditions in hospitals developed by (Büssing and Glaser 2000, 2002). These authors have provided detailed psychometric properties, including convergent validity with objective measures of work characteristics. Work overload measures the extent to which doctors are confronted with excessive amounts of work given the time available. The scale comprises four items: (1) “Even in a constant hurry, the amount of work is frequently too high to complete”, (2) “In this work there is frequently too much to do at once”, (3) “Time pressure to meet short-term deadlines is common here”, and (4) “Short-term deadlines frequently require working under pressure”. Job autonomy refers to possibilities for decision-making and exercising control at work. The scale consists of the following seven items: (1) “This work permits making own decisions on task goals”, (2) “This work offers latitudes to decide which tasks to pursue”, (3) “This work allows using one’s own ideas”, (4) “This work permits being creative in achieving work goals”, (5) “This work offers discretion in processing and scheduling”, (6) “It is possible to make own decisions on how to carry out the work”, and (7) “This work involves choices regarding what methods and tools to use”. Professional support refers to conditions that are instrumental for learning, skill development, and dealing with difficult work problems. Support was measured with three items: (1) “Assistance is available, when a difficult work problem cannot be solved alone”, (2) “The development of knowledge and skills needed to do the work is supported well”, and (3) “Adequate supports for developing the skills required to master challenging tasks are often not provided” (last item reverse-coded). All work characteristics scales use the same 5-point response format (1 = “not at all” to 5 = “yes, indeed”). Scale scores refer to the arithmetic mean of item scores and thus can take on values from 1 to 5 (higher values indicate higher levels of work overload, job autonomy, and professional support, respectively). Cronbach’s alpha coefficients ranged from .71 to .88 across the three scales and measurement points, indicating consistently acceptable reliability.
Depressive symptoms
The trait scale of the German version of Spielberger’s State-Trait Depression Scales (Form X-1) was used to measure depressive symptoms (STDS; Spielberger 1995; Spaderna et al. 2002). This 10-item scale assesses self-reported cognitive–affective symptoms of depression as a negative emotional state. It has been developed for use in non-clinical populations, and its psychometric properties have previously been validated (e.g. Krohne et al. 2002; Spaderna et al. 2002). Based on two samples of German and American university students (N = 124/251), Krohne et al. (2002) have reported substantial convergent validity between the STD-S and alternative self-report measures of depression (Beck Depression Inventory: r = .63/.58; Zung Self-Rating Depression Scale: r = .60/.66; Center for Epidemiologic Studies Depression Scale: r = .71/.62). Scale instructions asked respondents to indicate how they felt at the present moment on a four-point intensity scale (1 = “not at all” to 4 = “very much so”). Five items capture depressed affect or dysthymia: (1) “blue”, (2) “miserable”, (3) “downhearted”, (4) “sad”, and (5) “gloomy”; the other five items refer to the absence of positive affect or euthymia: (6) “strong”, (7) “alive”, (8) “safe”, (9) “healthy”, and (10) “hopeful about the future”. Euthymic items were reverse-coded and summed up with dysthymic items; thus, scale scores can take on values of 10–40 points, with higher scores indicating more intensive depressive symptoms. Cronbach’s alpha coefficients of .88 (T1), .90 (T2), and .90 (T3) indicated reliable measurement.
Statistical analysis
Analyses were performed using the software package SPSS 18.0. Data were independently entered into the database twice and checked for correctness and plausibility. To explore potential selection bias, we compared baseline data of doctors included in the sample (N = 415) and those who dropped out or were excluded (N = 206) using χ 2 tests (categorical) and t-tests (continuous variables). A difference was found for gender (χ 2 difference = 3.94, p = .05), indicating that the drop-out rate was higher for female than for male participants. No dissimilarities were found for partnership (χ 2 difference = .07, n.s.), age (M = 30.7 years, SD = 2.7, t(596) = .81, n.s.), professional tenure (M = 2.7 years, SD = .90, t(595) = .44, n.s.), weekly working time (M = 51.67 h, SD = 11.22, t(587) = .84, n.s.), or number of free weekends per month (M = 2.16, SD = .76, t(590) = −1.48, n.s.). Panel drop-outs also reported similar work characteristics (work overload: t(596) = −.48, n.s.; job autonomy: t(596) = .50, n.s.; professional support: t(592) = 1.11, n.s.) and intensity of depressive symptoms (t(564) = −1.04, n.s.) as panel responders at baseline.
To investigate the impact of cumulated work-related determinants on depressive symptoms, we used the arithmetic mean of T1 and T2 scores for working time, free weekends, work overload, autonomy, and professional support, respectively. We thus followed Cheng et al. (2000) who have argued that aggregating psychosocial work characteristics over a period of time provides a more stable and valid assessment of exposure to these conditions than single-point measures. Similarly, doctors’ initial depressive symptoms scores were calculated as the arithmetic mean of self-reported depressive symptoms across T1 and T2.
The criterion or outcome variable was a dichotomized measure of depressive symptoms at T3. Based on normative data on the STDS-S for Germany (Spaderna et al. 2002), the cut-off value for dichotomization was set at 24.21 points (normative mean of 18.96 points plus one standard deviation of 5.25 points). Doctors whose depressive symptoms scores exceeded this value were classified as showing “elevated depressive symptoms”. Lacking data on the efficiency of the STDS-S in predicting clinically diagnosed depression notwithstanding, there is reason to assume an elevated likelihood of finding clinically relevant cases predominantly among doctors scoring above the chosen cut-off (Lehr et al. 2008; Spaderna et al. 2002).
To identify prospective associations of predictor variables with the outcome, that is, being classified as having elevated depressive symptoms at the final assessment, a multivariate logistic regression model was calculated. Along with demographic information (gender, partnership, and professional tenure), initial average depressive symptoms scores and cumulated work-related determinants (working time, free weekends, work overload, autonomy, and professional support) were entered en bloc (i.e. simultaneously) as continuous predictor variables into the regression equation. As a recommended procedure to reduce potential problems of multicollinearity in multiple regression, we used z-scores for all non-categorical predictors (Cohen et al. 2002). Strength and direction of the associations between predictor and criterion variables were inferred from the logistic regression coefficients. Reported are odds ratios for the risk of showing elevated depressive symptoms in the last assessment as well as corresponding 95% confidence intervals. Nagelkerke R ² reflects goodness of fit. The regression model was first calculated for the whole sample; in a second step, we analysed only participants, who were not included in the elevated levels of depressive symptoms group at the outset of study (T1). In a last step, we tested for potential interactive effects of work characteristics by entering product terms of work overload, autonomy, and professional support, respectively, as well as their three-way interaction into the first regression equation (Cohen et al. 2002).
Results
Overall, mean scores of depressive symptoms remained stable over the study period (cf., Table 2). However, the proportion of junior doctors classified as showing elevated levels of depression based on mean scores above the applied cut-off of 24.21 points varied between 12.0% (N = 50) at baseline, 10.4% (N = 43) at T2, and 13.3% (N = 55) at T3 (cf., Table 1). In the course of the observation, N = 34 doctors (8.19%) were classified as incident cases, that is, reporting initially non-critical values and eventually scoring above the norm; 29 participants (6.99%) were classified having elevated depressive symptoms at T1 and non-elevated symptoms at T3. Consequently, 21 doctors (5.06%) were included in the elevated depressive symptoms group at T1 as well as T3. The risk of reporting elevated depressive symptoms was higher for doctors living without a partner at T1 and T2, but independent from gender or professional tenure across the study period (cf., Table 1).
No changes across measurement points were found for weekly working time. Free weekends per month dropped significantly from T1 to T2. Work overload increased from T2 to T3, whereas professional support was stable throughout the study; reported job autonomy at T2 was significantly lower than at T1 and T3 (cf., Table 2).
As this might be an issue of practical interest, we also compared working conditions at the baseline measurement between the three major medical specialties in our sample. Significant differences existed in weekly working time (F(df = 2) = 14.59; p < .00) and number of free weekends (F(df = 2) = 4.53, p = .01), such that surgeons worked the longest hours (M = 56.37 h, SD = 9.54 h) and had the lowest number of free weekends (M = 2.02, SD = 0.57), followed by their colleagues in internal medicine (M = 51.38 h, SD = 8.02, and M = 2.4, SD = 0.54) and anaesthesia (M = 48.16 h, SD = 8.24, and M = 2.27, SD = 0.63). Work overload (F(df = 2) = 10.72, p < .01) was lowest for anaesthetists (M = 2.90, SD = 0.73), but higher in internal medicine (M = 3.37, SD = 0.71) and surgery (M = 3.38, SD = 0.78). Job autonomy (F(df = 2) = 8.13, p < .01) was highest among internists (M = 2.72, SD = 0.59) and comparably lower in surgery (M = 2.47, SD = 0.55) and anaesthesia (M = 2.42, SD = 0.54). Finally, the highest levels of professional support (F(df = 2) = 6.59; p < .01) were reported by anaesthetists (M = 3.61, SD = 0.57), compared to surgery (M = 3.36, SD = 0.63) and internal medicine (M = 3.29, SD = 0.61). Despite these dissimilarities, however, no significant differences in initial depressive symptoms (F(df = 2) = 1.16; n.s.) were observed.
Effects of persistent work characteristics on future depressive symptoms were investigated in a logistic regression model. First, the full cohort of N = 415 junior doctors was examined. Aggregated mean scores before (T1) and after the first year of observation (T2) of four variables were significant predictors of the dichotomized outcome: higher initial depressive symptoms scores increased (OR 1.37; p < 0.01), whereas longer professional tenure (OR 0.54; p < 0.05), a higher number of monthly free weekends (OR 0.52; p < 0.05), and higher job autonomy (OR 0.35; p < 0.01) decreased the risk of inclusion into the elevated depressive symptoms group at T3. The negative association of partnership (OR 1.92, p < 0.07) and positive relationship of weekly working time (OR 0.96; p < 0.09) with elevated levels of depressive symptoms were non-significant, yet, with p-values below the 10% level, might be interpreted as potentially noteworthy tendencies. Contrary to our expectations, work overload and professional support possessed no predictive value. Fit of the model to the data was satisfactory (Nagelkerke R ² = .77).
In order to test the robustness of our findings, we applied the same regression model to the subgroup of doctors with initially non-elevated depressive symptoms (N = 365), that is, we excluded participants, who had scored above the cut-off for elevated depressive symptoms at baseline. Results were largely similar (cf., Table 3), such as initial depressive symptoms were positively and job autonomy negatively related to elevated levels of depressive symptoms in the final assessment. In this subgroup, working time was a significant predictor (OR 0.93; p < 0.02).
Additional analyses assessed interactive effects of work characteristics. However, neither one of the two-way interaction terms (Work Overload × Job Autonomy; Work Overload × Professional Support) nor the three-way interaction (Work Overload × Job Autonomy × Professional Support) had any predictive value for the outcome.
Discussion
Findings from this well-defined doctors’ cohort provide evidence that specific work characteristics in the hospital may influence future depressive symptoms in junior doctors. The study’s context was a three-wave panel study among 415 young German hospital doctors undergoing postgraduate training. Based on the JDCS model, we examined effects of relevant work characteristics during the first year on the incidence of elevated depressive symptoms almost 1.5 years later. Three major work characteristics were tested: (a) work overload (excessive quantitative workload); (b) job autonomy (decision authority and control on the job); and (c) professional support (assistance for skill development and difficult work tasks).
After controlling for initial depressive symptoms, demographic variables, and working time, only job autonomy had a significant effect in reducing the risk of developing elevated levels of depressive symptoms. Contrary to assumptions of the JDCS model, work overload and professional support did not predict changes in depressive symptoms. Additional analyses provided no support for interactive effects of work characteristics.
Comparison with previous studies
The rate of junior doctors who reported elevated levels of depressive symptoms varied from 12.0% (T1) to 10.4% (T2) to 13.3% (T3). These ratios are considerably higher than the 6.3% (CI 5.5–7.1%) reported by Wittchen et al. (1999) based on 4-week prevalence data of affective disorders in the general population in Germany. Mean scores for depressive symptoms in our sample, however, were comparable to the normative data for the STDS-D in a non-clinical population (Spaderna et al. 2002). Doctors classified as showing elevated depressive symptoms, therefore, should not be misinterpreted as clinical cases of depression. Although previous studies have suggested that doctors are a high-risk group for developing depressive symptoms, prevalence data on clinical depression in junior doctors are lacking (Tyssen and Vaglum 2002; Dyrbye et al. 2006). Moreover, differences in the definition and measurement of depressive symptoms demand great caution in comparing scores across studies.
The present study reinforces the postulated crucial role of job autonomy in clinical practice. For instance, a previous study on US doctors in mid-career found an inverse association between work control and social support and psychological distress 1 year later (Johnson et al. 1995). Regarding the relationship between work hours and subsequent impaired well-being, a thorough consideration of country-specific legal regulations and working time restrictions is advised (e.g. recent Implementation of European Working Time Directive compared to US working-hour limitations imposed by the Accreditation Council for Graduate Medical Education in 2003). Reviewing longitudinal studies on doctors in their first postgraduate years, Tyssen and Vaglum (2002) could not confirm a clear influence of work load or number of working hours on depression. This is in accordance with the results of our study. Nevertheless, studies indicate that overwork and long working hours may serve as contextual risk factors for depressive symptoms: in British doctors, a relationship was observed between overwork, or relationships to senior specialists, and depressive symptoms (Firth-Cozens 1987). Within a recent prospective study in US interns, work hours were predictive of depressive symptoms (Sen et al. 2010). Within our study, the associations of free weekends and reduced risks of later depressive symptoms might serve as a proxy estimation of the relationship of exceeding work hours with subsequent depressive symptoms.
Professional support did not reduce the risk of developing elevated depressive symptoms, which contradicts previous results and merits further discussion (Netterstrom et al. 2008). Partly, this result may be attributable to our conceptualization of professional support, which was defined as instrumental conditions for learning and skill development in the immediate work environment. Accordingly, the wording of our measure was quite general and did not explicitly include notions of emotional support from colleagues or a supportive supervisor relationship. Thus, semantic differences between our measure of professional support and other studies may potentially limit the external validity of our results. Moreover, some authors have suggested that there needs to be a match between the form and source of support and the most relevant work stressors in order for effects to be observed (cf., van der Doef and Maes 1999; de Jonge et al. 1999).
In terms of methodological rigour, our study compares favourably with mainstream research on the JDC(S) model, which typically is based on cross-sectional data (van der Doef and Maes 1999). Corresponding with the majority of longitudinal studies, we did not find any interactive effects of work characteristics on depressive symptoms (de Lange et al. 2003). That only one of the three main effects was significant was contrary to our hypotheses, yet is not limited to our study. De Lange et al.’s (2003) review revealed that out of 16 high-quality longitudinal studies including indicators for all three JDCS dimensions, only 3 (19%) found simultaneous main effects of all of them. Overall, the results of our study thus are largely in accordance with previous research. Yet, to our knowledge, this is the first study corroborating the important role of job autonomy for the psychological well-being of junior doctors.
Limitations of the study
Despite our longitudinal design, we acknowledge the limitations of survey studies for establishing causality. However, in our case of work characteristics and depressive symptoms, randomized control trials are difficult to establish in applied hospital settings. Therefore, methodologically rigorous studies, based on long-term observational data, provide the best source for causal making inferences. Cumulated work characteristics in our study were operationalized in terms of mean scores across 1 year and two measurement points. Although this should provide a more stable assessment than single-point estimates, we note that an aggregation over a longer observation period and multiple measurement points would be preferable to capture the long-term effects of enduring work characteristics on depressive symptoms (e.g. Cheng et al. 2000).
Our taxonomy of work characteristics was based on the JDCS model and thus limited in scope. The lack of confirming results might partly be attributed to the model’s limits to capture the complexities of working in human care jobs (cf., Söderfeldt et al. 1997; de Jonge et al. 1999). Working with patients and clients comprises multifaceted demands such as emotional labour, dealing with difficult patients, and mastering different roles. All these facets were not captured by the JDCS model. Therefore, comparison to and incorporation of alternative work design models is recommended for further research (Netterstrom et al. 2008).
The postal survey involved junior doctors of more than one hundred hospitals. Although our findings are based on data obtained by a validated standard questionnaire, information about working conditions and affective symptoms was based on self-report. The associations reported here may therefore be affected by common method bias (Zapf et al. 1996), since self-reported data on perceived stressors as well as depressive symptoms were not independent (Kasl 1998). In this study, we relied on self-report because we had no access to independent information (e.g. medical records, absence data, or turnover). Further research may potentially benefit from the use of robust objective data on potential depression-related outcomes (e.g. records of sickness absence).
Depressive symptoms were assessed with the STDS-S, which has been developed to measure depressive symptoms in non-clinical populations. Judging from its convergent validity with survey instruments commonly applied in clinical contexts, high scores on the STD-S may indicate clinically relevant levels of depressive symptoms (Krohne et al. 2002). However, we found no studies on the sensitivity and specificity of the STDS-S in predicting clinical depression. One study by Lehr et al. (2008) used the trait-version of the scale (STDS-T) in a sample of 104 healthy and 50 clinically depressed subjects. It determined a test efficiency of 87.6% for a cut-off ≥25 points (sensitivity: 76.0; specificity: 93.3). Corresponding with the cut-off in our study, this value lies almost exactly one standard deviation above the mean of the normative data for the STDS-T (M = 19.69; SD = 5.25) by Spaderna et al. (2002). Trait and state subscales of the STDS are nearly identically worded (the STD-T asks how respondents feel in general, the STD-S, how they feel at the present moment) and highly interrelated; Krohne et al. (2002) report latent variable correlations from r = .48 to r = .80 for dysthymia and euthymia. For our study, where the focus was work-related determinants, however, the STD-S was conceptually more appropriate than the operationalization as a stable personality trait. Even so, the limited number of validation studies on the STDS-S poses a further limitation.
The aim of this study was to analyse specific relationships between certain work characteristics and depressive symptoms in an early phase of a doctor’s career. Residency is characterized by an exceptionally high level of occupational stress (Firth-Cozens 1987; Tyssen et al. 2000; Buddeberg-Fischer et al. 2008). Virtually, all doctors who plan a clinical career must go through this training period. Hence, this experience is likely to influence future professional career and personal well-being. However, the results only apply to the first years in the hospital, while in later years, the selection of a specific career or being in a higher position in the medical hierarchy may produce different detrimental work conditions (Johnson et al. 1995).
Despite a high response to the survey at the successive measurements, loss-to-follow-up accumulated over the extended study period, as is inevitable in long-term panel studies. Great efforts were made at each stage of the survey to improve the response rate (i.e. two postal reminders). Yet, the final analyses included only 41.5% of the initial study group of junior doctors. This response rate is comparable to other physician surveys (Linzer et al. 2002; Asch et al. 1997). Additionally, our drop-out analyses show that we may widely assume similarity between the analysed group and the dropped-out doctors. We also note that empirical evidence for bias due to survey non-response and associated selection effects is actually limited and thus may be less pertinent than frequently assumed (Wei and Cowan 2006).
Meaning of the study
Impaired well-being of doctors is critical to the delivery of high-quality care (Wallace et al. 2009). Young doctors are a specially vulnerable professional group that needs professional support in order to prevent depression and its sequelae suffering (Prince et al. 2007), suicide (Schernhammer 2005), or impaired patient safety (Fahrenkopf et al. 2008). The present results indicate twofold implications: First, strengthening job autonomy may help to prevent depressive symptoms in junior doctors. In order to prove a causal relationship and to show that improving work autonomy could in fact lower the burden of depressive symptoms, a controlled intervention trial aiming to improve well-being would be necessary. Since depression is a prominent health problem for young doctors, intervention studies are warranted (Dietrich et al. 2011).
Second, this study may score highly in educational importance in two directions: First, greater attention should be paid to vulnerable doctors at the start of their professional career (i.e. efforts to detect vulnerable doctors; offer of counselling services; teaching of coping skills; tailored programmes for treatment seekers). Higher initial scores were prospectively associated with subsequent depressive symptoms. Since predicting individuals at risk is impossible, a range of services should be made available in this time of professional transition (Tyssen and Vaglum 2002). Second, according to our results, enhancing junior doctors’ autonomy or control at work seems an effective way to reduce the risk of subsequently developing depressive symptoms.
The fact that autonomy seems to be the most crucial resource for junior doctors is likely to be based on both its instrumental and psychological benefits (Bandura 1997; Bakker et al. 2005). Making own decisions on work goals, methods, and processes may help junior doctors to plan and organize their tasks in ways that are less stressful and better suited to their individual work approaches. Moreover, being able to exercise influence over one’s immediate environment has been identified as a basic psychological need, the fulfilment of which contributes to self-efficacy and well-being (Bandura 1997; Ryan and Deci 2000). Conversely, a lack of control may lead to an experience of the working situation as unpredictable and determined by forces beyond one’s own sphere of influence—conditions that have been associated with progressively passive responses in the sense of a learned helplessness and impaired mental health (Peterson et al. 1995). An autonomy-oriented redesign of junior doctors’ work thus seems to be a promising venue to improve psychological well-being and mental health during postgraduate training, yet needs to be carried out with close attention to its implications for clinical outcomes and patient safety.
Unanswered questions
Associations reported here may be influenced by third variables, which should be included in future studies. Potential moderators that contribute to depressive symptoms, for example family history of depression, personality, or previous serious life events, were assumed to be stable during our study (Bonde 2008; Netterstrom et al. 2008). While a more comprehensive assessment of possible influencing factors would have been desirable, practical considerations regarding the trade-off between survey length and response rates had to be taken into account. Further research is needed to clarify the role of junior doctors’ personal histories, life situations, and personality in the examined relationships.
In our case, work overload was not associated with future depressive symptoms. Potential explanations are the character of the applied stressor variables (Podsakoff et al. 2007) or that unmeasured third variables confound that relationship (Dormann and Zapf 2002); for example, junior doctors accept high stress levels as part of their professional self-image. As professional support, as conceptualized in our study, did not seem to be of particular relevance, future research should focus on the relative importance of different sources and types of instrumental, informational, and emotional support for junior doctors’ well-being during specialty training.
Conclusions
As discussed above, little is known about the contribution of work conditions to the development of depression in doctors during doctors’ first years of professional practice. Furthermore, in hospital settings, stressors are often assumed to be almost inevitable. By demonstrating the differential impact of different work characteristics, this study may serve to target workplace interventions. A programme should thus challenge the degree of autonomy junior doctors possess on the job. Focussing on enhanced control at work may be a promising approach since work stressors can be difficult to change, especially in a hospital environment, where time pressure and work overload are often regarded as an integral part of the job.
References
Arnetz BB (2001) Psychosocial challenges facing physicians of today. Soc Sci Med 52(2):203–213
Asch DA, Jedrziewski MK, Christakis NA (1997) Response rates to mail surveys published in medical journals. J Clin Epidemiol 50(10):1129–1136
Bakker AB, Demerouti E, Euwema MC (2005) Job resources buffer the impact of job demands on burnout. J Occup Health Psychol 10(2):170–180
Bandura A (1997) Self-efficacy: the exercise of control. W.H. Freeman, New York
Biaggi P, Peter S, Ulich E (2003) Stressors, emotional exhaustion and aversion to patients in residents and chief residents—what can be done? Swiss Med Wkly 133(23–24):339–346
Bonde JP (2008) Psychosocial factors at work and risk of depression: a systematic review of the epidemiological evidence. Occup Environ Med 65(7):438–445
Buddeberg-Fischer B, Klaghofer R, Stamm M, Siegrist J, Buddeberg C (2008) Work stress and reduced health in young physicians: prospective evidence from Swiss residents. Int Arch Occup Environ Health 82(1):31–38
Büssing A, Glaser J (2000) Work analysis instrument for hospitals (TAA-KH). A method for the psychological assessment of occupational health in hospitals. Work Stress 14:190
Büssing A, Glaser J (2002) Das Tätigkeits- und Arbeitsanalyseverfahren für das Krankenhaus—Selbstbeobachtungsversion (TAA-KH-S) [Work analysis instrument for hospitals—self report version (TAA-KH-S)]. Hogrefe, Göttingen
Chapman C (2006) Health reforms further anger Germany’s striking doctors. Lancet 367(9518):1229–1230
Cheng Y, Kawachi I, Coakley EH, Schwartz J, Colditz G (2000) Association between psychosocial work characteristics and health functioning in American women: prospective study. BMJ 320(7247):1432–1436
Cohen J, Cohen P, West SG, Aiken LS (2002) Applied multiple regression/correlation analysis for the behavioral sciences. Lawrence Earlbaum, Mahwah
de Jonge J, Mulder MJ, Nijhuis FJ (1999) The incorporation of different demand concepts in the job demand-control model: effects on health care professionals. Soc Sci Med 48(9):1149–1160
de Lange AH, Taris TW, Kompier MA, Houtman IL, Bongers PM (2003) “The very best of the millennium”: longitudinal research and the demand-control-(support) model. J Occup Health Psychol 8(4):282–305
Dietrich S, Deckert S, Ceynowa M, Hegerl U, Stengler K (2011) Depression in the workplace: a systematic review of evidence-based prevention strategies. Int Arch Occup Environ Health. doi:10.1007/s00420-011-0634-7
Dormann C, Zapf D (2002) Social stressors at work, irritation, and depressive symptoms: accounting for unmeasured third variables in a multi-wave study. J Occup Organ Psychol 75:33–58
Dyrbye LN, Thomas MR, Shanafelt TD (2006) Systematic review of depression, anxiety, and other indicators of psychological distress among USA and Canadian medical students. Acad Med 81(4):354–373
Fahrenkopf AM, Sectish TC, Barger LK, Sharek PJ, Lewin D, Chiang VW, Edwards S, Wiedermann BL, Landrigan CP (2008) Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ 336(7642):488–491
Firth-Cozens J (1987) Emotional distress in junior house officers. Br Med J (Clin Res Ed) 295(6597):533–536
Frank E, Biola H, Burnett CA (2000) Mortality rates and causes among U.S. physicians. Am J Prev Med 19(3):155–159
Griffin JM, Greiner BA, Stansfeld SA, Marmot M (2007) The effect of self-reported and observed job conditions on depression and anxiety symptoms: a comparison of theoretical models. J Occup Health Psychol 12(4):334–349
Johnson JV, Hall EM (1988) Job strain, work place social support, and cardiovascular disease: a cross-sectional study of a random sample of the Swedish working population. Am J Public Health 78(10):1336–1342
Johnson JV, Hall EM, Theorell T (1989) Combined effects of job strain and social isolation on cardiovascular disease morbidity and mortality in a random sample of the Swedish male working population. Scand J Work Environ Health 15(4):271–279
Johnson JV, Hall EM, Ford DE, Mead LA, Levine DM, Wang NY, Klag MJ (1995) The psychosocial work environment of physicians. The impact of demands and resources on job dissatisfaction and psychiatric distress in a longitudinal study of Johns Hopkins Medical School graduates. J Occup Environ Med 37(9):1151–1159
Karasek R (1979) Job demands, job decision latitude, and mental strain: implications for job design. Adm Sci Q 24:285–308
Karasek R, Theorell T (1990) Healthy work: stress, productivity and the reconstruction of working life. Basic Books Inc., New York
Kasl SV (1998) Measuring job stressors and studying the health impact of the work environment: an epidemiologic commentary. J Occup Health Psychol 3(4):390–401
Kawakami N, Haratani T, Araki S (1992) Effects of perceived job stress on depressive symptoms in blue-collar workers of an electrical factory in Japan. Scand J Work Environ Health 18(3):195–200
Krohne HW, Schmukle SC, Spaderna H, Spielberger CD (2002) The state-trait depression scales: an international comparison. Anxiety Stress Coping 15(2):105–122
Lehr D, Hillert A, Schmitz E, Sosnowsky N (2008) Assessing depressive disorders using the Center for Epidemiologic Studies-Depression Scale (CES-D) and State-Trait Depression Scales (STDS-T): a comparative analysis of cut-off scores. Diagnostica 54(2):61–70
Linzer M, Gerrity M, Douglas JA, McMurray JE, Williams ES, Konrad TR, Sa SGIMC (2002) Physician stress: results from the physician worklife study. Stress and Health 18(1):37–42
Michie S, Williams S (2003) Reducing work related psychological ill health and sickness absence: a systematic literature review. Occup Environ Med 60(1):3–9
Netterstrom B, Conrad N, Bech P, Fink P, Olsen O, Rugulies R, Stansfeld S (2008) The relation between work-related psychosocial factors and the development of depression. Epidemiol Rev 30(1):118–132
Peterson C, Maier SF, Seligman MEP (1995) Learned helplessness: a theory for the age of personal control. Oxford University Press, Oxford
Podsakoff NP, LePine JA, LePine MA (2007) Differential challenge stressor-hindrance stressor relationships with job attitudes, turnover intentions, turnover, and withdrawal behavior: a meta-analysis. J Appl Psychol 92(2):438–454
Prince M, Patel V, Saxena S, Maj M, Maselko J, Phillips MR, Rahman A (2007) No health without mental health. Lancet 370(9590):859–877
Prins JT, Gazendam-Donofrio SM, Tubben BJ, van der Heijden FM, van de Wiel HB, Hoekstra-Weebers JE (2007) Burnout in medical residents: a review. Med Educ 41(8):788–800
Ryan RM, Deci EL (2000) Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol 55(1):68–78
Schernhammer E (2005) Taking their own lives—the high rate of physician suicide. N Engl J Med 352(24):2473–2476
Schernhammer ES, Colditz GA (2004) Suicide rates among physicians: a quantitative and gender assessment (meta-analysis). Am J Psychiatry 161(12):2295–2302
Sen S, Kranzler HR, Krystal JH, Speller H, Chan G, Gelernter J, Guille C (2010) A prospective cohort study investigating factors associated with depression during medical internship. Arch Gen Psychiatry 67(6):557–565
Shanafelt TD, Bradley KA, Wipf JE, Back AL (2002) Burnout and self-reported patient care in an internal medicine residency program. Ann Intern Med 136(5):358–367
Söderfeldt B, Söderfeldt M, Jones K, O’Campo P, Muntaner C, Ohlson C-G, Warg L-E (1997) Does organization matter? A multilevel analysis of the demand-control model applied to human services. Soc Sci Med 44(4):527–534
Spaderna H, Schmukle SC, Krohne HW (2002) Report about the German adaptation of the State-Trait Depression Scales (STDS). Diagnostica 48(2):80–89
Spielberger CD (1995) State-Trait Depression Scales (form X-1). Mind Garden, Palo Alto
Stansfeld S, Candy B (2006) Psychosocial work environment and mental health—a meta-analytic review. Scand J Work Environ Health 32(6):443–462
Thomas NK (2004) Resident burnout. JAMA 292(23):2880–2889
Tokuyama M, Nakao K, Seto M, Watanabe A, Takeda M (2003) Predictors of first-onset major depressive episodes among white-collar workers. Psychiatry Clin Neurosci 57(5):523–531
Tyssen R, Vaglum P (2002) Mental health problems among young doctors: an updated review of prospective studies. Harv Rev Psychiatry 10(3):154–165
Tyssen R, Vaglum P, Gronvold NT, Ekeberg O (2000) The impact of job stress and working conditions on mental health problems among junior house officers. A nationwide Norwegian prospective cohort study. Med Educ 34(5):374–384
van der Doef M, Maes S (1999) The job demand-control(-support) model and psychological well-being : a review of 20 years of empirical research. Work Stress 13(2):87–114
Wallace JE, Lemaire JB, Ghali WA (2009) Physician wellness: a missing quality indicator. Lancet 374(9702):1714–1721
Wei LJ, Cowan CD (2006) Selection bias. In: Kotz S (ed) Encyclopedia of statistical sciences. Wiley, New York
West CP, Huschka MM, Novotny PJ, Sloan JA, Kolars JC, Habermann TM, Shanafelt TD (2006) Association of perceived medical errors with resident distress and empathy: a prospective longitudinal study. JAMA 296(9):1071–1078
Wittchen HU, Muller N, Pfister H, Winter S, Schmidtkunz B (1999) Affektive, somatoforme und Angststörungen in Deutschland—Erste Ergebnisse des bundesweiten Zusatzsurveys “Psychische Störungen” [Affective, somatoform and anxiety disorders in Germany—initial results of an additional federal survey of “psychiatric disorders”]. Gesundheitswesen 61 Spec no: S216–S222
Zapf D, Dormann C, Frese M (1996) Longitudinal studies in organizational stress research: a review of the literature with reference to methodological issues. J Occup Health Psychol 1(2):145–169
Acknowledgments
This study was funded in part by the German Medical Association and supported by the Bavarian Chamber of Doctors, Marburger Bund, and Munich Center of Health Sciences. These sponsors had no influence on the collection, analysis, and interpretation of data; on the writing of the report; and on the decision to submit the paper for publication. All authors are independent from the funders and supporters.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Ethics approval
The Committee on Ethics of Human Research of the Medical Faculty, Ludwig-Maximilians University Munich, gave ethical approval for the study (No. 016/04).
Rights and permissions
About this article
Cite this article
Weigl, M., Hornung, S., Petru, R. et al. Depressive symptoms in junior doctors: a follow-up study on work-related determinants. Int Arch Occup Environ Health 85, 559–570 (2012). https://doi.org/10.1007/s00420-011-0706-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-011-0706-8