
Abstract
Purpose
To update the mortality experience of employees of a factory that produced cellulose triacetate film base at Brantham in the United Kingdom and generate information on the effects of exposure to methylene chloride, in particular, mortality from cardiovascular disease and cancers of the lung, liver and biliary tract, pancreas and brain.
Methods
All 1,785 male employees with a record of employment at the film factory in 1946–1988 were followed through 2006, including 1,473 subjects exposed to methylene chloride on average for 9 years at a concentration of 19 ppm (8 h time-weighted average).
Results
A total of 559 deaths occurred during the follow-up period. In the subcohort of workers exposed to methylene chloride, substantially reduced mortalities compared with national and local rates were found for all causes, all cancers, and all the principal cancer sites of interest except for brain cancer. There was a small excess of brain cancer deaths (8 observed and 4.4 expected), but no evidence of an association with exposure to methylene chloride. Lung cancer mortality was significantly reduced in exposed workers, even compared to the low mortality rate in the local population (SMR 55). In contrast, mortality from ischaemic heart disease in exposed workers was slightly increased compared with local rates (SMR 102), but was lower in active employees (SMR 94; local rates), where a direct effect of exposure to methylene chloride should be concentrated.
Conclusions
The study provided no indication that employment at the plant, or exposure to methylene chloride, had adversely affected the mortalities of workers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background and objectives
Methylene chloride (dichloromethane) is a volatile organic solvent with many applications including paint stripping, aerosol propellant, food extraction, polyurethane foam manufacturing, triacetate film and fibre manufacturing and metal degreasing (IPCS 1996). The first epidemiological study to evaluate the effects of long-term exposure to methylene chloride on the mortality of workers (Friedlander et al. 1978) focused on cardiac effects based on the observation that methylene chloride is metabolised to carbon monoxide and that it causes a decrease in arterial oxygen content by increasing carboxyhaemoglobin concentrations (Stewart et al. 1972). Interest in methylene chloride as a possible human carcinogen was prompted by animal bioassays reporting an increased incidence of lung and liver tumours in mice, but not rats, exposed to methylene chloride (NTP 1986). Earlier inhalation studies by Burek et al. (1984) in rats and hamsters exposed at similar concentrations had shown no evidence of lung or liver tumours.
Studies of the mortality of five groups of workers exposed to methylene chloride have been conducted, and a critical review of the epidemiology literature has been performed by Dell et al. (1999). Three of these groups of workers worked in plants producing cellulose triacetate photographic film base. Hearne and Pifer (1999) reported on the mortality experience of two overlapping cohorts of workers described as the 1964–1970 Roll Coating and 1946–1970 Methylene Chloride cohorts, who were employed at a plant in Rochester, New York (44% of the total population were in both cohorts). Hearne et al. (1987, 1990) also reported on the mortality experience of the 1964–1970 Roll Coating cohort, and two earlier studies reported on the mortality of the subset of employees who worked during 1964 (Friedlander et al. 1978; Hearne and Friedlander 1981). The first study of the 1964–1970 Roll Coating cohort by Hearne et al. (1987) reported a suggestive excess of pancreatic cancer deaths (8 observed and 3.2 expected), but no more pancreatic cancer deaths have occurred in the cohort and the expected number of deaths has increased to 5.3 (Hearne and Pifer 1999). There was no excess of pancreatic cancer deaths in the second overlapping cohort, and compared with both the general population and a group of employed control subjects, there were reduced mortalities for lung and liver cancer and cardiovascular disease in both cohorts (Hearne and Pifer 1999).
The other cohort of workers engaged in film base manufacturing were employees of a factory owned by ICI that produced cellulose triacetate film base at Brantham in the United Kingdom (Tomenson et al. 1997). Among workers exposed to methylene chloride, substantially reduced mortalities compared with national and local rates were found for all causes, all cancers, and the principal cancer sites of interest at that time (liver and biliary tract cancer, lung cancer and pancreatic cancer). Mortality from ischaemic heart disease in exposed workers was slightly increased compared with local rates, but lower than expected among active employees where a direct effect of exposure to methylene chloride should be concentrated.
Two other groups of workers who worked in plants producing cellulose triacetate fibre have been studied (Ott et al. 1983; Lanes et al. 1990, 1993; Gibbs et al. 1996). Ott et al. (1983) reported no adverse mortality or morbidity experience in a cohort of workers at a plant in Rock Hill, South Carolina. However, mortality updates by Lanes et al. (1990, 1993) reported excess mortality from cancer of the biliary passages and liver, although the excess observed in the most recent update was not statistically significant (4 observed and 1.34 expected). Three of these deaths were due to cancer of the biliary tract. A study of workers employed at a similar plant that produced cellulose acetate and triacetate fibres in Cumberland, Maryland, was conducted to evaluate the consistency of this association (Gibbs et al. 1996), but reported reduced mortality from cancer of the biliary passages and liver (2 observed and 3.71 expected).
Heineman et al. (1994) reported an association between astrocytic brain cancer and exposure to methylene chloride in a case–control study of astrocytic brain cancer and occupational exposure to chlorinated aliphatic hydrocarbons. The risk of astrocytic brain cancer increased with probability and average intensity of exposure and with duration of employment in jobs considered exposed to methylene chloride, and the trends could not be explained by exposures to the other solvents studied.
This report describes an update of the retrospective cohort study conducted by Tomenson et al. (1997) of a cohort of workers employed at a photographic film base plant at Brantham in the United Kingdom and includes a further 12 years of follow-up. The objectives of the study were to generate improved data on the effects of exposure to methylene chloride for one of the five cohorts that contribute the most relevant information to the debate on the safety of the chemical and to better characterise the dose–response relationship with cumulative exposure to methylene chloride. Health effects of a priori interest were cancers of the lung, liver and biliary tract, pancreas and brain and ischaemic heart disease.
Methods
Study population and follow-up
The study population consisted of all male workers employed at a photographic film base plant in Brantham, United Kingdom from 1946 until its closure in 1988. The cohort consists of 1,785 male workers of whom 1,473 had worked in jobs that entailed exposure to methylene chloride. A detailed description of the plant and the methods used to ascertain the cohort are given in the report by Tomenson et al. (1997) which gives results of the earlier investigation into mortality patterns in the cohort with follow-up through 31 December 1994. Female workers were not included because few had worked in production areas and many had job titles that made exposure difficult to assess. The investigation updates follow-up through 31 December 2006, a further 12 years of follow-up. The vital status of the cohort was ascertained using information provided by the UK Medical Research Information Service. The original investigation was approved by ICI’s Medical Research Committee (an institutional review board), and Section 60 support for the update was granted by the UK Patient Information Advisory Group.
Exposure assessment
Workers at the Brantham site have not been exposed to methylene chloride since production of film base ceased and the exposure assessment made for the original investigation has been used for the study update. Estimates of exposure to methylene chloride were generated for 20 distinct work groups during four production periods (before 1960, 1960–1969, 1970–1979, 1980–1988), and estimated exposures (8-h TWA, ppm) for some selected work groups are given by Tomenson et al. (1997). Lifetime cumulative exposure to methylene chloride was calculated by summing the products of mean level of exposure and duration of employment for each job held by a cohort member. The employment histories of 30% of exposed workers (439) were insufficiently precise to calculate a reliable estimate of cumulative exposure. Most of these workers were labourers and maintenance workers whose job histories were not specific enough to determine the time spent in exposed areas.
The non-exposed group consisted of a variety of occupations, but all were unlikely to have been exposed either directly or indirectly through their daily work, although very low concentrations may have existed in the general atmosphere around the works. Most were office workers in the technical and commercial functions. In contrast, the exposed workers were predominantly manual workers.
Statistical methods
The occupational cohort mortality analysis program OCMAP-PLUS (Marsh et al. 1998) was used to sum person-years within categories of age (5-year intervals) and calendar period (generally 5-year intervals to conform with changes in the ICD) and to compute standardised mortality ratios (SMR). Mortality statistics for England and Wales were used for comparison, and a comparison with local mortalities was also made for selected causes by combining mortality information from four surrounding districts (Tendring, Babergh, Ipswich and Colchester) from 1981 to 2006 and the two surrounding counties (Suffolk and Essex) for 1974–1980. Analyses were performed for the entire cohort and the subcohort of workers who had worked for a minimum of 3 months.
The analysis treated duration of employment, cumulative exposure, and latency as time related variables with the values calculated for each person-year under observation. A subject was allowed to contribute to more than one stratum in each analysis. Cumulative exposure to methylene chloride was categorised as 0, 0–399, 400–799, and ≥800 ppm-years in the original investigation by Tomenson et al. (1997), and the same categories have been used in the update. These cut-off points were chosen to enable comparisons to be made with the studies of Rochester film workers. However, trend analyses were also performed using cut-off points (36.4 and 299.1 ppm-years) which gave equal numbers of deaths from all causes in the 3 cumulative exposure categories. A Poisson trend statistic was used to test for a montonic dose–response relationship in the SMRs (Breslow and Day 1987). A more qualitative assessment of exposure effect was obtained by performing analyses based on duration of exposure.
For selected causes of death, a multivariate regression analysis based on Cox’s proportional hazards model was performed with age as the time variable (Checkoway et al. 2004). The analysis included all workers for whom it was possible to calculate cumulative exposure to methylene chloride (1,034 exposed and 312 unexposed workers). The resultant estimate of hazard ratio can be interpreted as relative risk (RR). Regression models included terms for calendar period (four groups) and cumulative exposure to methylene chloride was treated as a time-dependent variable (both as a continuous variable and grouped by increasing exposure). Analyses were also performed for log-transformed cumulative exposure. Time since hire was included in some models, and analyses were also performed with lagged cumulative exposure (15 years).
Results
Table 1 shows the vital status on 31 December 2006 and the demographic characteristics of exposed and unexposed workers. A total of 59 workers (3.3%) had left the country (49 had emigrated and 10 workers were temporary foreign workers), and a further 10 workers (0.6%) were lost to follow-up. Workers who were not exposed to methylene chloride tended to be older when hired and followed up for fewer years. As noted earlier, workers at Brantham had not been exposed to methylene chloride since the film production plant closed in 1988 and the exposure estimates derived by Tomenson et al. (1997) remain valid. The 1,034 workers for whom it was possible to calculate individual estimates of cumulative exposure to methylene chloride had been exposed on average for 9 years at a concentration of 19 ppm (8 h TWA), and the median, upper quartile and upper decile of cumulative exposure for these workers were 36.0, 149.1 and 545.7 ppm-years, respectively. Tomenson et al. (1997) noted that it was not possible to calculate the cumulative exposure of individual workers in the unassigned group, but on average, they were estimated to have been exposed for 11 years at a concentration of 13 ppm (8 h TWA).
SMRs for the major causes of death and those of initial interest are presented in Table 2, separately for the groups of never exposed workers and exposed workers. SMRs were calculated using England and Wales mortality rates. Among exposed workers, deaths from all causes of death (P < 0.01) and all malignant neoplasms (P < 0.01) were significantly lower than expected. Results for never exposed workers were similar, and deaths from all causes were significantly lower than expected (P < 0.05) and deaths due to malignant neoplasms were reduced (SMR 68). Deaths due to cancers of the lung, pancreas, and liver and biliary tract were all lower than expected in exposed workers. Deaths due to lung cancer were significantly reduced in both exposed (P < 0.01) and unexposed workers (P < 0.05), and there were no deaths due to cancer of the biliary passages and liver in the entire cohort. Deaths due to brain and other CNS cancers were elevated in exposed workers, but the increase was not statistically significant. Deaths due to all heart disease and ischaemic heart disease in exposed and never exposed workers were also lower than expected. Results for workers with more than 3 months of employment were similar and are not presented.
When local rates were used to calculate expected deaths, the expected number of deaths due to all causes fell by 10.4% and those due to all malignant neoplasms fell by 7.4% (exposed and unexposed workers). For the conditions of a priori interest, local mortality rates were only higher for brain cancer (3.8% increase in expected deaths) and were especially low for lung cancer and ischaemic heart disease (reductions in expected deaths of 13.8 and 13.6%, respectively). Deaths among exposed workers from all causes of death (SMR 88), all malignant neoplasms (SMR 75) and lung cancer (SMR 55) remained significantly lower than expected (P < 0.01). Results for cancers of the pancreas, liver and biliary tract and brain were similar whether local or national mortality rates were used for comparison. However, mortalities due to ischaemic heart disease were elevated in both exposed workers (SMR 102) and unexposed workers (SMR 111) when compared to local mortality rates.
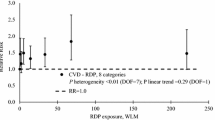
Table 3 presents the results of the SMR analysis for three cumulative dose groups, the group of exposed but unassigned workers, and the never-exposed group. Findings are presented for all causes of death, all malignancies, all causes of death initially of interest except for liver and biliary tract cancer from which there were no deaths, and deaths from all malignancies other than lung cancer because of the very low level of lung cancer mortality in the cohort. There was no evidence of an association between exposure to methylene chloride and all causes of death, all malignancies, and the cancers initially of interest. The test for trend ischaemic heart disease was not significant, but mortality from ischaemic heart disease increased over the three categories of cumulative exposure. However, the SMR for all exposed workers (SMR 88) was lower than that for unexposed workers (SMR 95). The results of trend analyses were similar when restricted to workers with more than 3 months employment.
Table 4 shows the results of Cox regression models with cumulative exposure to methylene chloride as a continuous variable. Results are displayed as relative risks (RR) for exposure to 1,000 ppm-years estimated from Cox regression analyses. Analyses were performed with and without the unexposed group and gave similar results. Time since hire was only significant in models for ischaemic heart disease and was not included in models for other causes of death. No Cox regression coefficients were statistically elevated. Similar findings were obtained for analyses of log-transformed cumulative exposure to methylene chloride and are not presented here.
Discussion
The cohort of Brantham film base production workers is one of the five cohorts totalling 7,270 subjects which provide most of the information currently available about the human health effects of methylene chloride. The other cohorts include two overlapping cohorts of workers who were also exposed to methylene chloride during the manufacture of cellulose triacetate film base (Hearne and Pifer 1999) and two groups of workers who incurred exposure to methylene chloride in the production of cellulose triacetate fibres (Lanes et al. 1993; Gibbs et al. 1996). Table 7 of Hearne and Pifer (1999) summarises the exposure characteristics of workers in the different cohorts. The mean exposure of workers in the present investigation was 19 ppm compared with a workplace exposure limit in the UK of 100 ppm (8 h TWA). Mean exposure was lower than in the other cohorts of photographic workers (26 and 39 ppm), and the mean duration of exposure (9 years) was also shorter (23 and 17 years). Levels of exposure in the two cohorts of fibre workers were considerably higher. The three cohorts of photographic film workers include only male subjects, but a large proportion of the fibre workers were women.
Although the workers in the Brantham cohort experienced the lowest cumulative exposure of the five cohorts, the investigation is valuable for human health risk assessment because of its well-characterised exposure and dose–response analyses. Its value has been increased by the addition of 12 years of follow-up that has resulted in the number of deaths among exposed workers increasing from 287 to 479. The expected numbers of deaths from rare endpoints of interest have almost doubled giving much increased power to detect effects e.g. the expected number of deaths due to liver and biliary passages cancer among exposed workers has increased from 1.5 to 2.8. Mortality patterns over the additional period of follow-up were very similar to those observed in the original study. Among exposed workers, mortality from all causes, all malignant neoplasms, cancers of the digestive system, lung cancer, cerebrovascular disease and non-malignant respiratory disease were reported to be statistically significantly reduced by Tomenson et al. (1997), and all except for non-malignant respiratory disease showed similar reductions during the additional period of follow-up. Compared to England and Wales mortality rates, deaths from non-malignant respiratory disease were close to expected during the additional years of follow-up (SMR 105; 95% CI 73–148), but a statistically significant reduction in mortality due to ischaemic heart disease was observed during this period (SMR 73; 95% CI 52–98).
The observation of lung and liver tumours in the mouse (NTP 1986) raised concerns about the possible carcinogenicity of methylene chloride. Since then, much understanding has been obtained about the metabolic pathways that are the most important for dosimetry and risk assessment, in particular the glutathione S-transferase theta-1 (GSTT1) pathway (Starr et al. 2006). Indeed, one section of the population who are homozygotic null (non-conjugators) for the GSTT1 polymorphism (typically 15 to 25%) are predicted to be at no increased cancer risk from exposure to methylene chloride because they show no GSTT1-dependent metabolism and lack the capacity to bioactivate methylene chloride. David et al. (2006) describe how risk assessments using PBPK modelling have become increasingly more refined since the EPA unit risk value of 4.7 × 10−7 per 1 μg/m3 was derived (EPA 1991) and have culminated in a much lower estimate of risk. David et al. (2006) calculated a median unit risk value of 9.33 × 10−10 per 1 μg/m3 for combined liver and lung tumours using their updated PBPK model incorporating improved metabolic and physiological parameters, and the distribution of genetic polymorphisms for metabolism, approximately a factor of 500 lower than the EPA unit risk value.
The unit risk value derived by David et al. (2006) corresponds to an approximate 1 in 10,000 risk of lung and liver tumours for lifetime methylene chloride exposure of 30 ppm and suggests that it is unlikely that excesses of lung and liver tumours would be observed in the epidemiological studies, especially those of the lower exposed film workers. The Brantham film workers cohort, like the other four groups, experienced reduced overall mortality, reduced mortality from cancer and lower mortality than expected for lung cancer. Lung cancer mortality was especially low for exposed workers in this study, even when compared with the low mortality rates in the local population (SMR 55; 95% CI 36–80), but mortality from other types of cancer apart from lung cancer was also reduced compared to local rates (SMR 84; 95% CI 68–102). Thus, the increased incidence of lung cancer seen in the mouse bioassay is not corroborated by the epidemiology studies, although confounding by smoking may have limited the ability of these studies to detect an effect of exposure to methylene chloride on the risk of lung cancer. The current investigation also provided no evidence of an increased risk of liver cancer or support for the excess of biliary cancer reported in one group of cellulose triacetate fibre workers (Lanes et al. 1993). The excess of biliary cancer was not replicated in another highly exposed group of fibre workers (Gibbs et al. 1996) or in the other cohorts of photographic film workers (Hearne and Pifer 1999).
A suggestive excess of pancreatic cancer was reported in the first study of one of the cohorts of Rochester film workers, but Hearne and Pifer (1999) reported no new cases in the most recent update (8 observed and 5.3 expected), and there was no excess in the overlapping cohort of photographic film workers (5 observed and 5.5 expected). The present study and the two studies of highly exposed fibre production workers (Lanes et al. 1993; Gibbs et al. 1996) provide no support for an association between pancreatic cancer and exposure to methylene chloride.
An association between astrocytic brain cancer and exposure to methylene chloride was reported in a case–control study of astrocytic brain cancer and occupational exposure to chlorinated aliphatic hydrocarbons (Heineman et al. 1994), generating interest in this endpoint (Lynge 1999). In the current study of film workers, there was a non-significant excess of brain cancer deaths in exposed workers (8 observed and 4.4 expected). However, four of these workers had minimal exposure to methylene chloride: one employee was an engineering apprentice in the unassigned exposure group who worked for 1 month and three had estimated cumulative exposures ranging from 1 to 27 ppm-years (a draughtsman who worked for just over 1 year, a laboratory assistant for 4 years and an employee who performed estimation work in the engineering department). Another worker was an electrician from the unassigned exposure group whose job title was insufficiently precise to identify the areas worked, but it was estimated that the mean exposure of this worker, who was employed for 21 years, was unlikely to have exceeded 15 ppm (8 h TWA). The cumulative exposure of the three other workers who died of brain cancer was estimated to range from 189 to 572 ppm-years. When the alternative cut-off points of 36.4 and 299.1 ppm-years were used, an excess of brain cancer deaths was only observed in the lowest (SMR = 226; 95% CI 47–663 and 3 observed) and highest cumulative exposure categories (SMR 328; 95% CI 40–1,188 and 2 observed). There was no significant trend with cumulative exposure whichever set of cut-off points were used for analysis. Non-significant excesses of brain cancer were also reported among workers in both of the overlapping cohorts of Rochester photographic film workers cohorts; 6 observed and 2.8 expected in the 1946–1970 Methylene Chloride cohort, and 4 observed and 2.1 expected in the 1964–1970 Roll Coating cohort, but it was noted that two of the subjects had only worked in a methylene chloride environment for a relatively short period, and there was no evidence of a dose-related trend based on cumulative exposure (Hearne and Pifer 1999). Hence, the small and non-significant excesses of brain cancer mortality in the Brantham and Rochester cohorts of film workers do not appear to be related to methylene chloride exposure, and no support for such an association was provided by the studies of more highly exposed textile fibre workers (Lynge 1999; Hearne and Pifer 1999).
Because methylene chloride is metabolised to carbon monoxide and induces the formation of carboxyhaemoglobin, a role for methylene chloride in the induction of ischaemic heart disease is plausible (Stewart et al. 1972). Tomenson et al. (1997) reported higher mortality due to ischaemic heart disease among exposed workers than among unexposed workers, but the reverse was true in this update. In the case of ischaemic heart disease, it has been suggested that the cardiovascular effects of exposure to carbon monoxide may be acute and reversible (Kristensen 1989), and any effect would be concentrated in active employees. The updated study provides no new information about cardiovascular risk in active employees as production had already ceased at the plant when the first study was conducted. The SMR for ischaemic heart disease decreased to 83 (SMR = 94 calculated using local mortality rates) when the analysis was restricted to active exposed employees (including any deaths that occurred within 1 month of the end of employment). A suggestion of a trend in ischaemic heart disease with cumulative exposure was found in the Cox regression for assigned exposure workers, but this was not significant. This was partly due to the very low mortality among workers in the lowest cumulative exposure group (<400 ppm-years), which was lower than among unexposed workers. However, mortality from ischaemic heart disease was also elevated among workers in the highest cumulative exposure group (≥800 ppm-years) in both the first study and the update, although mortality was close to expected during the update period. There was no evidence of an acute effect in workers in the highest cumulative exposure group as Tomenson et al. (1997) reported that no in-service deaths due to ischaemic heart disease occurred in this group. Reduced mortality from ischaemic heart disease was reported among workers in all of the other four cohorts of workers exposed to methylene chloride (Hearne and Pifer 1999). In addition, there have been three investigations into the cardiovascular health of some of the workers in the present cohort and the cohort of Rock Hill fibre workers (Ott et al. 1983; Soden 1993; Cherry et al. 1981), and none reported any evidence of long-term damage that could be attributed to exposure to methylene chloride.
The potential weaknesses of the study are discussed in more detail by Tomenson et al. (1997) and include the lack of smoking histories, personal monitoring data before 1980 and reliable area monitoring data before 1975. However, good historical information on the casting machines and working conditions was available, and information on the number of incidents where workers were affected by methylene chloride vapours was consistent with the pattern of exposure estimated for jobs and time periods. Another study weakness was the inability to include 30% of exposed workers (the unassigned exposure group) in the dose–response analyses.
Occupational cohort mortality studies are often influenced by ‘the healthy worker effect’ resulting from the employment and retention of relatively healthy individuals when compared with the general population (McMichael 1976). This is a limitation for external mortality comparisons of outcomes that may directly influence workforce selection processes such as cardiovascular diseases, diabetes mellitus and non-malignant respiratory diseases (Monson 1986), but its effect can be overcome by the use of a suitable internal reference group as in this study. A healthy worker effect was observed in this study with deaths among exposed workers from all causes of death significantly lower than in the local population (SMR 88). However, much of the reduction was due to the low mortality from lung cancer (SMR 55) and reduced mortality from other types of malignant neoplasms (SMR 84). Deaths from causes other than malignant neoplasms were not significantly reduced (SMR 93).
In conclusion, this study provides no evidence of increased mortality related to exposure to methylene chloride. An increased SMR for ischaemic heart disease in the highest cumulative exposure group was observed, but there was no evidence that risk was increased while workers were exposed to methylene chloride and potentially experienced decreases in the arterial oxygen content of their blood. Although this study, like others, did not provide any compelling evidence of an increased risk of cardiovascular disease, the restrictions on smoking at workstations may have limited the ability of all of these studies to detect an exposure-related effect on mortality from cardiovascular disease. Overall, there was no evidence of any increased carcinogenic risk in this population. This was not simply due to a reduced incidence of lung cancer resulting from a low prevalence of smoking in the cohort. Mortality from cancers other than lung cancer was less than expected (SMR 84; local rates), consistent with the pattern reported by Hearne and Pifer (1999) for the other four cohorts of photographic film workers and fibre workers (SMR range 83–95). A small excess of brain cancer deaths was observed, but there was no evidence that this was related to methylene chloride exposure.
References
Breslow NE, Day NE (1987) Statistical methods in cancer research. Volume 2: the design and analysis of cohort studies. Oxford University Press, Oxford, pp 96–97
Burek JD, Nitschke KD, Bell TJ, Wackerle DL, Childs RC, Beyer JE, Dittenber DA, Rampy LW, McKenna MJ (1984) Methylene chloride: a two-years inhalation toxicity and oncogenicity study in rats and hamsters. Fundam Appl Toxicol 4:30–47
Checkoway H, Pearce NE, Kriebel D (2004) Research methods in occupational epidemiology, 2nd edn. Oxford Univ Press, New York, pp 274–276
Cherry N, Venables H, Waldron HA, Wells GG (1981) Some observations on workers exposed to methylene chloride. Br J Ind Med 38:351–355
David RM, Clewell HJ, Gentry PR, Covington TR, Morgott DA, Marino DJ (2006) Revised assessment of cancer risk to dichloromethane II. Application of probabilistic methods to cancer risk determinations. Regul Toxicol Pharmacol 45:55–65
Dell LD, Mundt KA, McDonald M, Tritschler JP 2nd, Mundt DJ (1999) Critical review of the epidemiology literature on the potential cancer risks of methylene chloride. Int Arch Occup Environ Health 72:429–442
Environmental Protection Agency (EPA) (1991) Integrated risk information system: Dichloromethane. Available at http://www.epa.gov/iris/subst/0070.html. Accessed on 9 Nov 2010
Friedlander BR, Hearne T, Hall S (1978) Epidemiologic investigation of employees chronically exposed to methylene chloride: mortality analysis. J Occup Med 20:657–666
Gibbs GW, Amsel J, Soden K (1996) A cohort mortality study of cellulose triacetate fiber workers exposed to methylene chloride. J Occup Environ Med 38:693–697
Hearne FT, Friedlander BR (1981) Follow-up of methylene chloride study (letter). J Occup Med 23:660
Hearne FT, Pifer JW (1999) Mortality study of two overlapping cohorts of photographic film base manufacturing employees exposed to methylene chloride. J Occup Environ Med 41:1154–1169
Hearne FT, Grose F, Pifer JW, Friedlander BR, Raleigh RL (1987) Methylene chloride mortality study: dose-response characterisation and animal model comparison. J Occup Med 29:217–228
Hearne FT, Pifer JW, Grose F (1990) Absence of adverse mortality effects in workers exposed to methylene chloride: an update. J Occup Med 32:234–240
Heineman EF, Cocco P, Gomez MR, Dosemeci M, Stewart PA, Haye RB, Zahm SH, Thomas TL, Blair A (1994) Occupational exposure to chlorinated aliphatic hydrocarbons and risk of astrocytic brain cancer. Am J Ind Med 26:155–169
International Program on Chemical Safety (IPCS) (1996) Methylene chloride. Environmental health criteria 164, 2nd edn. World Health Organization, Geneva
Kristensen TS (1989) Cardiovascular diseases and the work environment: a critical review of the epidemiologic literature on chemical factors. Scand J Work Environ Health 15:245–264
Lanes SF, Cohen A, Rothman KJ, Dreyer NA, Soden KJ (1990) Mortality of cellulose fiber production workers. Scand J Work Environ Health 16:247–251
Lanes SF, Rothman KJ, Dreyer NA, Soden KJ (1993) Mortality update of cellulose fiber production workers. Scand J Work Environ Health 19:426–428
Lynge E (1999) Mortality of workers exposed to methylene chloride employed at a plant producing cellulose triacetate film base. Occup Environ Med 56:215
Marsh GM, Youk AO, Stone RA, Sefcik S, Alcorn C (1998) OCMAP-PLUS: a program for the comprehensive analysis of occupational cohort data. J Occup Environ Med 40:351–362
McMichael AJ (1976) Standardized mortality ratios and the “healthy worker effect”: scratching beneath the surface. J Occup Med 18:165–168
Monson RR (1986) Observations on the healthy worker effect. J Occup Med 28:425–433
National Toxicology Program (1986) NTP toxicology and carcinogenesis studies of dichloromethane (methylene chloride) (CAS No. 75–09-2) in F344/N rats and B6C3F1 mice (inhalation studies). Natl Toxicol Program Tech Rep Ser 306:1–208
Ott MG, Skory LK, Holder BB, Bronson JH, Williams PR (1983) Health evaluation of employees occupationally exposed to methylene chloride. Scand J Work Environ Health 9(Suppl 1):1–38
Soden KJ (1993) An evaluation of chronic methylene chloride exposure. J Occup Med 35:282–286
Starr TB, Matanoski G, Anders MW, Andersen ME (2006) Workshop overview: reassessment of the cancer risk of dichloromethane in humans. Toxicol Sci 91:20–28
Stewart RD, Fisher TN, Hosko MJ, Peterson JE, Baretta ED, Dodd HC (1972) Experimental human exposure to methylene chloride. Arch Environ Health 25:342–348
Tomenson JA, Bonner SM, Heijne CG, Farrar DG, Cummings TF (1997) Mortality of workers exposed to methylene chloride employed at a plant producing cellulose triacetate film base. Occup Environ Med 54:470–476
Acknowledgments
The author thanks the European Chlorinated Solvents Association (ECSA) for funding this research and the UK Medical Research Information Service for their assistance.
Conflict of interest
The investigator provides consultancy services to a range of customers including the chemical industry.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tomenson, J.A. Update of a cohort mortality study of workers exposed to methylene chloride employed at a plant producing cellulose triacetate film base. Int Arch Occup Environ Health 84, 889–897 (2011). https://doi.org/10.1007/s00420-011-0621-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-011-0621-z