
Abstract
Objectives
To determine and characterise the health impacts of extreme heat events on the population in five regions of New South Wales (NSW). Such data provide evidence necessary for the development of policy and programme initiatives designed to reduce the burden of disease due to the impact of climate change.
Methods
A case-only approach was used to analyse 1,497,655 emergency hospital admissions in Sydney East and West, Illawarra, Gosford-Wyong and Newcastle. The distribution of daily minimum and maximum temperatures in each region was used to define extreme heat (≥99th percentile). We investigated the susceptibility of the main causes of emergency hospital admission to extreme heat. We also examined the presence of underlying conditions as a risk modifier of emergency hospital admission on extreme heat. Logistic regression model was used to estimate the effect modifications.
Results
Main causes: On days of extreme heat, the risk of emergency hospital admission due to heat-related injuries, dehydration and other disorders of fluid, electrolyte and acid–base balance increased more than the risk of admission from other causes. Underlying conditions: Those with underlying mental and behavioural disorders, diseases of nervous and circulatory system, especially cardiac, diseases of respiratory system, especially asthma and chronic obstructive pulmonary disease, neoplasms and renal disease, especially renal failure, were more susceptible to an extreme heat event.
Conclusions
In this study, we identified several main diagnoses and underlying conditions for emergency hospital admission that are particularly susceptible to extreme heat events. This knowledge can contribute directly to establishing health programmes that would effectively target those with higher relative risk of emergency hospital admission due to extreme heat.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There is an increasing evidence that extreme heat events have become more prolonged with climate change and that these events will increase in frequency, duration and intensity (Solomon et al. 2007). These extreme heat events have a significant impact on human health both directly through dehydration and heat stroke and indirectly through a number of other health conditions including cardiovascular collapse and respiratory distress (Solomon et al. 2007).
Early warning health systems to detect and reduce morbidity and mortality due to extremes in heat have been shown to be effective (Kilbourne 2002; Bernard and McGeehin 2004; Nogueira 2005). These systems are based on a number of components, including accurate and timely meteorological forecasts, an understanding of the potential health outcomes of heat waves and adequate health intervention strategies (Sheridan and Kalkstein 2004; Smoyer-Tomic and Rainham 2000; Kalkstein et al. 1996; Department of Health 2009).
This study was part of a wider programme on adaptation to climate change undertaken by the New South Wales state health department. Understanding the impacts of climate change on a population is the key to reducing the burden of disease due to climate change. Of those impacts, extremes of temperature, particularly heat, have been shown to have considerable effects on morbidity and mortality (Nogueira 2005; Smoyer-Tomic and Rainham 2000; Stafoggia et al. 2006; Kaiser et al. 2007; Hajat et al. 2006). A number of overseas studies have demonstrated these effects (Filleul et al. 2006; O’Neill et al. 2005; Medina-Ramon et al. 2006). This study focuses on identifying the modifying effect of selected main diagnosis and underlying condition on emergency hospital admission during an extreme heat event. Much of the literature relates to events in the northern hemisphere. This study is a first step in trying to characterise what happens in NSW during an extreme heat event and whether the northern hemisphere results can be generalised for the southern hemisphere.
The objective of the study was to characterise the susceptibility to emergency hospital admission due to extreme heat in five areas of NSW and to identify the temperature index that best predicts increased susceptibility to emergency hospital admission. And further the study aims to identify chronic diseases or other characteristics that modify the risk of hospitalisation due to extreme heat. The outcomes of this study can be used to understand the health impacts of extremes of heat and to provide evidence to develop and support public health interventions to reduce such impacts.
Materials and methods
Study design and population
In Australia, the spring months are September to November, and the summer months are from December to February. We have used a case-only design for studying the susceptibility to extreme heat events using weather, air pollution and emergency hospital admissions for selected disease categories over the total 1,422 spring and summer days, from 1st September to 28th February of each year, in the period 1998–2006. Data from February 2006 were not ready at the time of constructing the dataset so that 1 month was omitted from analysis. The study focussed on five regions in NSW: Sydney East; Sydney West; Gosford-Wyong; Newcastle and Illawarra.
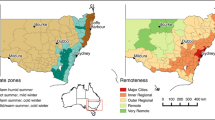
Cooler nights in Sydney West and cooler days in Sydney East provided the rationale for dividing Sydney into East and West. Data from Sydney weather stations were used to define two temperature regions (Sydney West and Sydney East) by maximising the ratio of between groups to within-group temperature variance. Statistical local areas (SLA) within Sydney were then assigned to the west and east regions. SLA of residence was used to assign patients to Sydney East, Sydney West, Illawarra, Gosford-Wyong and Newcastle. The average of weather and air pollution observations from all monitoring stations in each region was used (Fig. 1).

NSW Department of Environment and Climate change air quality monitoring sites and Australian Bureau of Meteorology weather stations overlaying study regions
Morbidity data
We examined current literature on mortality, morbidity and temperature to determine the range of diseases that may modify the risk for hospital admission during extreme heat events (Schwartz 2005; Kovats and Ebi 2006; Medina-Ramon et al. 2006; Johnson et al. 2005; Le Tertre et al. 2006). The diseases selected for the analysis were similar to those described in previously published studies with the addition of cancer.
Daily hospital admissions were obtained from NSW Health, for each of the five regions. Hospitalisation data are routinely assembled by NSW Health, and there is universal coverage of all admissions. For each admission, information on primary diagnosis, secondary diagnosis, sex, referral source, age and SLA of residence was obtained. The following primary diagnoses were retrieved: cardiovascular disease (International Classification of Diseases [ICD]-10 code I00-I99), cardiac arrest (ICD-10 code I00-I52), cerebrovascular disease (ICD-10 code I60-I69), respiratory disease (ICD-10 code J00-J99), asthma (ICD-10 code J45-J46), chronic obstructive pulmonary disease (COPD; ICD-10 code J40-J44 and J47), renal disease (ICD-10 code N00-N39), acute renal failure (ICD-10 code N17-N19), calculus of the kidney and ureter (ICD-10 code N20-N23), injury (ICD-10 code S00-T98), heat-related injuries (ICD-10 code T67), mental and behavioural disorders (ICD-10 code F00-F99), diabetes (ICD-10 code E10-E14), dehydration (ICD-10 code E86) and other disorders of fluid, electrolyte and acid–base balance (ICD-10 code E87.0-E87.8).
Admission data were also reviewed for up to 55 secondary underlying diagnoses: cardiovascular disease (ICD-10 code I00-I99), cardiac arrest (ICD-10 code I00-I52), cerebrovascular disease (ICD-10 code I60-I69), respiratory disease (ICD-10 code J00-J99), asthma (ICD-10 code J45-J46), chronic obstructive pulmonary disease (COPD; ICD-10 code J40-J44 and J47), renal disease (ICD-10 code N00-N39), acute renal failure (ICD-10 code N17-N19), calculus of the kidney and ureter (ICD-10 code N20-N23), diabetes (ICD-10 code E10-E14), mental and behavioural disorders (ICD-10 code F00-F99), diseases of nervous system (ICD-10 code G00-G99) and cancer (ICD-10 code C00-D48).
The analysis was limited to subjects with their status at admission flagged as emergency. All planned and maternity/newborn admissions were excluded. The source of referral was the emergency department for 87.4% of the patients. Nursing homes, psychiatric facilities and general practitioners were amongst other categories of referral.
Environmental data
Daily minimum and maximum temperature, and humidity and wind speed at 9 am and 3 pm from NSW Bureau of Meteorology were obtained for each monitoring station in the five regions. The measurements were averaged over 4 stations in Sydney East, 11 in Sydney West, 1 in Illawarra, 3 in Gosford-Wyong and 2 in Newcastle.
We used four different metrics for temperature (daily maximum temperature, daily minimum temperature, apparent temperature at 9 am and apparent temperature at 3 pm) to investigate which heat indicator has the most influence on modifying admissions to hospital, as some recent studies have suggested that a high minimum temperature (indicating lack of overnight cooling) may be a good predictor of adverse health effects as this may impede the body’s ability to cope with continuing high temperatures the next day (Diaz et al. 2002; O’Neill et al. 2003). The apparent temperature is a measure of relative discomfort due to combined heat, low wind speed and high humidity and was calculated using methods used by the Australian Bureau of Meteorology (http://www.bom.gov.au/info/thermal_stress/).
For each of the temperature metric, extreme heat events were defined as either (a) days when that temperature exceeded the 99th percentile of its distribution in that region (lag0); (b) days for which this criterion was met on the previous day (lag1); and (c) days where the 3-day moving average exceeded its 99th percentile, as some studies have suggested that multiple days with extreme temperature may be more important than a single day of extreme temperature (Kalkstein and Valamont 1986; Saez et al. 1995).
The above three definitions for extreme heat events were created for each of the five regions as previous studies have shown that the relationship between health-related outcomes and temperature varies across different regions, with the largest heat effect observed in cooler regions (Hales et al. 2000; Keatinge et al. 1997).
Air pollution data from NSW Department of Environment, Climate Change and Water were obtained. The data included daily 1-h maximum of nitrogen dioxide (NO2), daily average of particulate matter less than 10 microns in diameter (PM10) and daily 1-h maximum of ozone (O3). As Gosford-Wyong does not have an air pollution monitoring station, it was assumed that the air pollution level in Gosford-Wyong was similar to that of Newcastle, an area slightly to the north with similar air pollution sources, geography and weather patterns.
For each region (except for Gosford-Wyong), daily average NO2, PM10 and O3 were calculated. The measurements were averaged over 4 stations in Sydney East, 10 in Sydney West, 4 in Illawarra and 3 in Newcastle.
Statistical analysis
Armstrong (2003) introduced the use of the case-only design, originally applied to the study of gene-environmental interactions, for identifying groups susceptible to environmental factors such as air pollution or weather. The author argues that the conventional study design and statistical methods for investigating effect modifications through interaction terms, for example, in time series Poisson regression depends on hard to verify modelling assumptions and complex computation. The case-only approach provides an advantage over other study designs as it requires fewer assumptions and is efficient for detecting precise estimates of interaction and also the analysis is more straightforward. However, there are some limitations to the case-only design particularly that the main effects cannot be estimated (Armstrong 2003). The results from case-only analyses are expressed as relative odds and require careful interpretation (Armstrong 2003; Schwartz 2005).
Since the introduction of the case-only design for environmental health research, it has been used to identify underlying conditions that modify the risk of mortality and morbidity associated with heat waves and ambient air pollution (Schwartz 2005; Medina-Ramon et al. 2006).
Following the methods of Schwartz (2005) and Armstrong (2003), we fitted logistic regression models in Stata (version 9; StataCorp, College Station, TX) in two separate series:
-
1.
Presence or absence of each primary diagnosis as outcome and extreme heat indicator as predictor.
-
2.
Presence or absence of each underlying secondary diagnosis as outcome and extreme heat indicator as predictor.
Separate analyses were conducted for each of the heat indicators: maximum temperature, minimum temperature, apparent temperature at 9 am and apparent temperature at 3 pm. As the daily maximum temperature consistently gave the highest relative odds for each of the primary and secondary diagnoses, further analysis proceeded using only this predictor variable. The analysis was repeated using this temperature indicator on the day of hospitalisation (lag0), the day before hospitalisation (lag1) and for the 3-day average ending on the day of hospital admission.
Schwartz (2005) states that “time varying predictors of risk, such as seasonality should not confound any association with chronic conditions, because such conditions will not fluctuate over time.” However, if the proposed modifier of the effect of extreme temperature is a modifier of seasonality (e.g. if diabetics have a stronger seasonal pattern in morbidity than other persons) or if the morbidity of interest has seasonal pattern (e.g. injuries might be higher at Christmas and on New Year’s Eve), a confounding with the interaction of interest could occur. Therefore, all models also included a sine and cosine term with a 365.24-day period to capture interactions between season and the characteristic being investigated (Medina-Ramon et al. 2006).
The study aimed to estimate the effect modification across the five regions. As noted by Armstrong (2003), this can be either achieved by meta-analytic techniques or by including morbidities from all regions in a case-only logistic regression stratified by region (i.e., in which an indicator for region is included). The second method was chosen as the individual record data were available for all regions so it permits more detailed modelling of the possible effect differences between those regions.
As Armstrong (2003) pointed out, the interaction between a suggested modifier of interest (for example diabetes) and other time-varying factors (for example air pollution) does not cancel out in a case-only method. Therefore, this was taken into account when using air pollution variables (NO2, PM10 and O3) as regressors in the model.
Results
This study included a total of 1,497,655 admissions across the five regions in NSW during the spring and summer periods of 1st September 1998-31st January 2006. Sydney East, with 596,368 admissions (39.82%), had the highest number of admissions during the study period, followed by Sydney West with 545,485 admissions (32.4%). The smaller regions of Illawarra (6.7%), Gosford-Wyong (8.8%) or Newcastle (8.2%) contributed less than 133,000 hospital admissions each. Those aged 65–74 accounted for 12.1%, and those over 75 years of age were 24.4% of the total admissions, with 13.6% of all admissions attributed to those less than 14 years of age. A little over half (50.2%) of admissions were women.
The most common primary diagnoses for hospital admission in the five regions during the study period were injury (17.8%), diseases of circulatory system (12.3%) and diseases of respiratory system (10.5%).
Of those admitted during the study period, the most common underlying conditions were diseases of circulatory system (26.1%) specifically cardiac, followed by mental and behavioural disorders (12.3%), diseases of the respiratory system (9.7%), diabetes mellitus (8.5%) diseases of the renal system (7.9%) and the nervous system (6.8%) and cancers (4.8%).
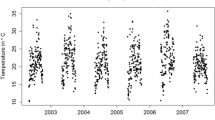
The mean daily maximum temperature was higher in Sydney West (27°C) compared to Sydney East (25°C) whereas the mean daily minimum temperature was higher in Sydney East (16°C) compared to Sydney West (14°C). The temperature distributions during the year have been used for calculating the 99th percentile. Temperature metrics by region in spring and summer of 1998–2006 are presented in Table 1.
Descriptive analysis shows that for some main diagnosis and also for some underlying conditions, number of emergency hospital admissions on extreme heat days was higher than that on not extreme heat days. Results are not shown here for all except for emergency admission due to heat-related injuries as an example to show the relative increase on emergency admission (Table 2).
Table 3 shows the association between the primary causes of emergency hospitalisation to extreme heat events, defined either for the same day (lag0), the day before (lag1) or as a 3-day moving average. The association of emergency hospital admission due to mental health and behavioural disorders with extreme heat events increased significantly only during the prolonged heat events (OR = 1.07; 95% CI: 1.00–1.15). During extreme heat events, the association between emergency hospital admission due to heat-related injuries (OR = 5.87; 95% CI: 4.33–7.95), dehydration (OR = 1.56; 95% CI: 1.30–1.88); and other disorders of fluid, electrolyte and acid–base balance (OR = 1.29; 95% CI: 1.05–1.58) increased significantly.
Table 4 shows the results of the analysis looking at modification by underlying conditions during extreme heat events, defined either for the same day (lag0), the day after (lag1) or a 3-day moving average. The majority of these modifiers were most pronounced in their effect on emergency admissions after 3 days of high temperatures. Those who have asthma showed the greatest evidence of effect modification, with an odds ratio of 1.57 (95% CI: 1.40–1.76).
Patient characteristics
Individual characteristics that could increase subject susceptibility to extreme heat were also examined including: “more than 75 years old”, “more than 65 years old”, “less than 4 years old”, “male” and “living at nursing home”. None of the above characteristics significantly modified the overall risk of emergency admission to hospitals (results not shown).
With regard to individual susceptibility for each main condition, emergency admission risk for men was significantly increased when the main diagnosis was renal disease (OR = 1.22; 95% CI: 1.04–1.44). Men over 75 years of age were more likely to be admitted with a primary diagnosis of heat-related illness and children less than 4 years of age with dehydration.
When the underlying condition was cerebrovascular disease, emergency admission risk was significantly modified for those older than 65 years (OR = 1.59; 95% CI: 1.09–2.31). Cancer as an underlying condition also modified the risk for subjects older than 65 years (OR = 1.17; 95% CI: 1.00–1.37) and for those older than 75 years (OR = 1.21; 95% CI: 1.03–1.42).
Discussion
A feature that distinguishes this study from some previous investigations is the use of the case-only analysis to identify susceptible groups for the adverse health effects of air pollution or weather. The case-only approach provides an advantage over Poisson modelling, as it is simpler and relies on reduced assumptions when the focus is to identify effect modification.
For this study, case-only analysis is useful in determining which groups of patients may be more susceptible to extreme heat events; however, it does not provide quantitative estimates of the overall increase in demand for health services during such events. The odds ratios estimated here represent the relative increase in emergency admissions due to different primary diagnosis or underlying cause, not an absolute estimate of the expected increase in overall hospital utilisation.
We have estimated relative increases in emergency hospital admissions for primary diagnoses ranging from 7% (for mental disorders) to 590% (heat-related injuries including heat exhaustion, heat syncope, sunburn and sunstroke). Those with underlying conditions of asthma and heart disease are expected to be most likely to have an emergency hospital admission after 3 days of very high temperatures (57 and 14% increase, respectively). The conditions identified are affected by temperature independent of the effect of air pollution on health.
The presenting and underlying conditions identified in this study are broadly similar to those identified in other studies of heat and hospital admissions. The only other similar study from Australia found emergency admissions with a primary diagnosis of mental health, renal disease and ischaemic heart disease in the elderly were observed to increase significantly during heat waves (Nitschke et al. 2007).
European studies have generally found increase in extreme heat-related emergency admission is most marked amongst the elderly; however, the role of underlying cardiovascular disease has not been highlighted. In France, presentations for dehydration, hyperthermia, malaise, hyponatraemia, renal colic and renal failure were observed to occur more frequently and the number of elderly patients also increased significantly during heat waves (Josseran et al. 2009). In a study limited to the very elderly in Italy, heat and respiratory disease emergency admissions increased significantly after three or more days above 40°C; however, there was no increase of admissions with a primary diagnosis of circulatory disease (Mastrangelo et al. 2007). A twelve city study also found increased emergency admissions with a primary respiratory cause amongst those over 75 years but no effect for admissions where cardiovascular was the primary cause (Michelozzi et al. 2009). By contrast, heat waves in European cities have been associated with an excess of deaths due to cardiovascular conditions (Mastrangelo et al. 2006; Linares and Diaz 2007; Kovats et al. 2004).
A study that compared emergency hospital admissions during a heat wave in Chicago in 1995 described changes in both primary and underlying conditions. Similar to our findings, increased emergency admissions were due to dehydration, heat stroke and heat exhaustion but also included acute renal failure, and elevated co-morbid conditions were cardiovascular disease, renal disease and nervous system disorders, but also included diabetes. Respiratory disease overall was not noted to be a significant co-morbidity, and only emphysema showed any increase as an underlying respiratory condition during the heat wave period. In this study, the elderly were disproportionately admitted (Semenza et al. 1999).
The increase in emergency admissions for mental and behavioural disorders related to heat has been noted in other studies (Johnson et al. 2005; Garcia-Pina et al. 2008). A relationship with underlying diseases of the nervous system, particularly Alzheimer’s and Parkinson’s disease, was noted during the Chicago heat wave (Semenza et al. 1999). There are likely to be multiple causes behind the observed effect of heat on these conditions, including impaired coping skills. One study observed an increase in emergency admissions and mortality during heat waves for several conditions that commonly use psychotropic drugs and postulated that the interference of these drugs with body temperature regulation exacerbates the impact of heat on the health of those using them (Hansen et al. 2008). There is a need to further investigate the mechanism of such events on mental health patients, and mechanisms for health services to effectively provide this target group with protective measures.
This study identified that any additional risk for the elderly was limited to those with underlying cerebrovascular disease or cancer and that males over 75 years are the most likely to be admitted due to heat-related illness. However, we were not able to determine which factors are most important in increasing the risk. These at risk groups need specific and targeted information in order to reduce their susceptibility to extreme heat events.
Whilst initiating a heat wave plan as early as possible on a day when the maximum temperature, or the 3-day average maximum, is expected to reach extreme levels is desirable this is highly reliant on accurate temperature predictions. However, to initiate a heat wave plan too early, or at too low a threshold, could undermine its effectiveness (Nogueira 2005; Smoyer-Tomic and Rainham 2000; Kalkstein et al. 1996; Department of Health 2009; Kovats and Ebi 2006).
Although this study looked at daily minimum and maximum temperatures and two measures that incorporate humidity and wind speed, the greatest effect was predicted by daily maximum temperature alone. The 3-day moving average of the maximum temperature was a better predictor of risk than the maximum temperature on the same day or the day before. Numerically, the 3-day average is lower than the daily maxima; however, the highest 3-day average periods represent periods of sustained very high temperature. Had we extended our analysis to longer time lags we may have found larger impacts on health. In Italy, four consecutive hot humid days were required before an effect on hospital admissions was observed (Mastrangelo et al. 2007).
Previous studies have used a range of heat indicators. The other Australian study only looked at periods where the temperature exceeded 35°C for three or more days (Nitschke et al. 2007). A similar approach to defining excess heat was used in Italy (Mastrangelo et al. 2007), whereas other studies have focussed on specific heat wave episodes (Josseran et al. 2009; Semenza et al. 1999; Shiloh et al. 2005). A more exploratory approach similar to the intent of our analysis has been used recently in other studies to try and characterise heat conditions of relevance to health outcomes (Michelozzi et al. 2009; Linares and Diaz 2007; Martin-Latry et al. 2007). To date, no consistency has been found between the most sensitive heat indicators for different locations.
In summary, this study will assist health services to develop programmes and policies to limit the impacts of extreme heat events on the population, particularly those sensitive subgroups.
References
Armstrong BG (2003) Fixed factors that modify the effects of time-varying factors: applying the case-only approach. Epidemiology 14:467–472
Bernard SM, McGeehin MA (2004) Municipal heatwave response plans. Am J Public Health 94(9):1520–1522
Department of Health (2009) Heatwave-plan for England, protecting health and reducing harm from extreme heat and heatwaves Available at: http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_099583.pdf
Diaz J, Jordan A, Garcia R et al (2002) Heat waves in Madrid: 1986–1997: effects on health of the elderly. Int Archiv Occup Environ Health 75(3):163–170
Filleul L, Cassadou S, Medina S et al (2006) The relation between temperature, ozone, and mortality in nine French cities during the heat wave of 2003. Environ Health Perspect 114:1344–1347
Garcia-Pina R, Tobias GA, Sanz NJ, Navarro SC (2008) Effect of weather temperature on hospital emergencies in the Region of Murcia, Spain, throughout the 2000–2005 and its use in epidemiological surveillance. Revista Espanola de Saud Publica 82(2):153–166 Wolfgong Ahrens and Iris Pigeot Handbook of Epidemiology
Hajat S, Armstrong B, Baccini M et al (2006) Impact of high temperatures on mortality: is there an added heat wave effect? Epidemiology 17:632–638
Hales S, Samond G, Town GI, Kjellstrom T, Woodward A (2000) Daily mortality in relation to weather and air pollution in Christchurch, New Zealand. Aust J Public Health 24(1):89–91
Hansen A, Bi P, Nitschke M, Ryan P et al (2008) The effect of heatwaves on mental health in a temperate Australian city. Environ Health Perspect 116:1369–1375
Johnson H, Kovats RS, McGregor G, Stedman J, Gibbs M, Walton H (2005) The Impact of the 2003 heat wave on daily mortality in England and wales and the use of rapid weekly mortality estimates. Eurosurveillance 10:7–9 Jul-Sep
Josseran L, Caillere N, Brun-Ney D, Rottner J et al (2009) Syndromic surveillance and heat wave morbidity a pilot study based on emergency departments in France. BMC Med Inform Decis Mak 9:14
Kaiser R, Le Tetre A, Schwarz J et al (2007) The effect of the 1995 heat wave in Chicago on all-cause and cause-specific mortality. Am J Public Health 97(suppl 1):S158–S162
Kalkstein L, Valamont K (1986) An evaluation of summer discomfort in the United States using a relative climatological index. Bull Am Meteorol Soc 67:842–848
Kalkstein L, Jamason P, Greene J et al (1996) The Philadelphia hot weather-health watch warning system: development and application, Summer 1995. Bull Am Meteorol Soc 77:1519–1528
Keatinge WR, Donaldson GC, Bucher K, Jendritsky G, Cordioli E, Martinelli M et al (1997) Cold exposure and winter mortality from ishaemic heart disease, cerebrovascular disease, respiratory disease, and all causes in warm and cold regions of Europe. Lancet 349(9062):1341–1346
Kilbourne EM (2002) Heat related illness: current status of prevention efforts. Am J of Prev Med 22i:328–329
Kovats RS, Ebi KL (2006) Heatwaves and public health in Europe. Eur J Pub Health 16:592–599
Kovats RS, Hajat S, Wilkinson P (2004) Contrasting patterns of mortality and hospital admissions during hot weather and heat waves in Greater London. Occup Environ Med 61:893–898
Le Tertre A, Lefranc A, Eilstein D, Declercq C, Medina S, Blanchard M, Chardon B, Fabre P, Filleul L, Jusot JL, Pascal L, Prouvost H, Cassadou S, Ledrans M (2006) Impact of the 2003 heatwave on all-cause mortality in 9 French cities. Epidemiology 17:1
Linares C, Diaz J (2007) Impact of high temperatures on hospital admissions: comparative analysis with previous studies about mortality (Madrid). Eur J of Pub Health 18(3):3312–3322
Martin-Latry K, Goumy MP, Latry P, Gabinski C et al (2007) Psychotropic drugs use and risk of heat-related hospitalisation. Eur Psy 22(6):335–338
Mastrangelo G, Hajat S, Fadda E, Buja A et al (2006) Contrasting patterns of hospital admissions and mortality during heat waves: are deaths from circulatory disease a real excess or an artefact? Med Hypotheses 66(5):1025–1028
Mastrangelo G, Fedeli U, Visentin C, Milan G et al (2007) Pattern and determinants of hospitalisation during heat waves: an ecologic study. BMC Public Health 7:200
Medina-Ramon M, Zanobetti A, Cavanagh DP, Schwartz J (2006) Extreme temperatures and mortality: assessing effect modification by personal characteristics and specific cause of death in a multi-city case-only analysis. Environ Health Perspect 11:1331–1336
Michelozzi P, Accetta G, De Sario M, D’Ippoliti D et al (2009) High temperature and hospitalizations for cardiovascular and respiratory causes I n12 European cities. Am J Resp Crit Care Med 179(5):383–389
Nitschke M, Tucker GR, Peng B (2007) Morbidity and mortality during heatwaves in metropolitan Adelaide. MJA 187(11/12):662–665
Nogueira PJ (2005) Examples of heat health warning systems: Lisbon’s ICARO surveillance system, summer 2003. In: Kirch W, Menne B, Bertollini R (eds) Extreme weather events and public health responses. Springer, Berlin, pp 141–160
O’Neill MS, Zanobetti A, Schwart J (2003) Modifiers of temperature and mortality association in seven US cities. Am J Epidemiol 157:1074–1082
O’Neill MS, Hajat S, Zanobetti A et al (2005) Impact of control for air pollution and respiratory epidemics on the estimated associations of temperature and daily mortality. Int J Biometeorol 50:121–129
Saez M, Sunyer J, Castellsague J et al (1995) Relationship between weather temperature and mortality: a time series analysis approach in Barcelona. Int J Epidemiol 24:576–582
Schwartz J (2005) Who is sensitive to extremes of temperature? A case-only analysis. Epidemiology 16:67–72
Semenza JC, McCullough JE, Flanders WD, McGeehin MA et al (1999) Excess hospital admissions during the July 1995 heat wave in Chicago. Am J Prev Med 16(4):269–277
Sheridan S, Kalkstein LS (2004) Progress in heat watch-warning system technology. Bull Am Meteorol Soc 85:1931–1941
Shiloh R, Shapira A, Potchter O, Hermesh H et al (2005) Effects of climate on admission rates of schizophrenia patients to psychiatric hospitals. Eur Psy 20:61–64
Smoyer-Tomic KE, Rainham DGC (2000) Beating the heat: development and evaluation of a Canadian Hot Weather Health Response Plan. Environ Health Perspect 109:1241–1247
Solomon S, Qin D, Manning M, Chen Z, Marquis M, Averyt K B, Tignor M and Miller H L (2007) IPCC fourth assessment report (AR4). Climate change 2007: the physical science basis. Contribution of working group I to the fourth assessment report of the intergovernmental panel on climate change. Cambridge University Press, Cambridge, United Kingdom and New York, NY, USA, p. 996
Stafoggia M, Forastiere F, Agostini D et al (2006) Vulnerability to heat-related mortality: multicity, population-based, case-crossover analysis. Epidemiology 17:315–323
Acknowledgments
We would like to acknowledge the support and assistance of the Australian Bureau of Meteorology and the New South Wales Department of Environment, Climate Change and Water. We would like to thank Professor Bin Jalaludin from University of New South Wales and Associate Professor Geoff Morgan from University of Sydney, for reviewing this paper and their comments. We would also like to thank Mr Sina Mavaddati from Department of Planning for preparing the map. This research was part of the NSW Health Department Climate Change Adaptation Programme and funded under the NSW Government’s Climate Change Adaptation Research Fund.
Conflict of interest statement
The authors declare they have no competing financial interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Khalaj, B., Lloyd, G., Sheppeard, V. et al. The health impacts of heat waves in five regions of New South Wales, Australia: a case-only analysis. Int Arch Occup Environ Health 83, 833–842 (2010). https://doi.org/10.1007/s00420-010-0534-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-010-0534-2