
Abstract
Purpose
To analyse the mortality and its causes, especially cancer, among French cement production workers.
Methods
A cohort of all workers employed at least 1 year in one of the main four cement companies in France was assembled (9,118 workers, 122,124 person-years of follow-up between 1990 and 2005). A common job titles classification was used to analyse occupational risk factors. We conducted a standardized mortality ratio analysis based on age, gender and calendar-period-specific national mortality rates and explored the combined effect of job titles and duration through an internal Cox regression analysis.
Results
The number of deaths during the follow-up period was 430 (4.7%). Malignant neoplasm was the cause of 48.1% of deaths. Overall, a deficit in all-causes mortality (standardized mortality ratio (SMR): 0.68, 95% confidence interval (CI) 0.61–0.74) and in cancer mortality (SMR: 0.80, CI 0.69–0.92) was observed. Working in the quarry, yard and shipping sectors was associated with a 50% higher all-causes mortality risk in comparison with the administrative sector.
Conclusions
This cohort study does not support previous observations that cement workers are at higher risk of cancer mortality than the general population. The length of follow-up should be increased, and specific exposures deserve analysis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Portland cement is the main process in cement production (78.4% in France in 2007). It is produced by crushing and grinding calcareous materials (mainly limestone, chalk and clay) and additives. The mixture is cooked at high temperature (around 1,500°C) in a rotary kiln heated by different sources of energies (coke, fuel, gas, others). As a result, working in a cement plant involves exposure to cement dust, particulate matters and gaseous pollutants, polycyclic aromatic compounds, silicates, aluminates, chromium VI and other metals such as nickel or cobalt, and asbestos because of the high-temperature process. Many of these substances are considered as definite or possible carcinogens. The carcinogenicity of cement and the risk of cancer associated with working in the cement industry are therefore debated. Several epidemiologic studies have been performed to analyse the carcinogenic risks possibly associated with working in the cement production or utilization. Significant associations have been reported with lung cancer (Milne et al. 1983; Rafnsson and Johannesdottir 1986; Schoenberg et al. 1987; Minder and Beer-Porizek 1992; Swanson et al. 1993; Robinson et al. 1995; Knutsson et al. 2000; Stern 2001; Smailyte et al. 2004; Pukkala et al. 2009; Consonni et al. 2010), laryngeal and upper GI cancer, (Jakobsson et al. 1990; Minder and Beer-Porizek 1992; Robinson et al. 1995; Maier and Tisch 1997; Knutsson et al. 2000; Stern 2001; McDowall 1984; Zagraniski et al. 1986; Dietz et al. 2004; Jansson et al. 2005; Purdue et al. 2006), colorectal cancer, (McDowall 1984; Jakobsson et al. 1990, 1994; Partanen et al. 1994), prostate cancer (Krstev et al. 1998), bladder cancer (Smailyte et al. 2004) and Hodgkin’s lymphoma (Blair et al. 1993). Nevertheless, other showed negative results (Amandus 1986; Brownson et al. 1989; Siemiatycki et al. 1989; Vestbo et al. 1991). Co-exposures to tobacco, asbestos, diesel exhaust and silica and the fact that studies often mixed workers involved in the production of cement with construction workers might represent confounding factors. Another limitation is the low statistical power of many studies.
In 2005, the four main cement companies in France (Ciments Calcia, Holcim France, Lafarge Ciments and Vicat) employing around 5,000 workers in 113 plants, producing annually 22 million tons of cement, decided to initiate the realization of the first French epidemiologic study in that industry via their professional association Association technique de l’industrie des liants hydrauliques (ATILH, Technical Association of Hydraulic Binder Industry). Its objectives were to compare the mortality of the cohort of the cement production workers with the mortality of the general population in France from 1990 to 2005, with a special attention to cancer.
Methods
Cohort definition and data collection
The cohort included all workers employed in cement production for at least 1 year at any plant of the four companies in continental France between the 1st of January 1990 and the 31st of December 2005. Workers employed by service companies or sub-contractors were not included as the information required for mortality study was not available for them. Every employee who worked at least 1 day during the follow-up period was first identified from payrolls. For each identified employee, the following characteristics were extracted from the company administrative files: birth date and place, gender, hiring and end of employment dates, name of the employer, activity status on the 31st of December 2005 and job titles occupied since the hiring (as far back as year 1946). For each job occupied, start and end dates were recorded with the work contract’s type (fulltime, part-time, internship). These data were extracted from digital or paper records kept by the human resources departments of the 113 plant locations.
A common job titles classification was especially created for the purpose of this study. In the four companies, around 3,800 job titles were listed. A harmonization process was carried out by a work group including members from the four human resources departments and the industrial hygienists. It resulted in 142 job titles that were classified into seven job categories according to the type of work performed throughout the whole process of cement production from the extraction of raw materials to the shipment, namely: quarry, yard, production, shipping (and packing), maintenance, laboratory and administration. To perform the multivariate analysis, production and maintenance, shipping and yard were further collapsed into two categories.
The vital status, till 31 December 2005, was obtained throughout link-search on the database available from the Institut National de la Statistique et des Etudes Economiques (INSEE National Institute of Statistical and Economic Studies National Institute of Statistics). Individuals were matched by last name, first name, date of birth and place of birth. The obtained information was the vital status, and the date and place of death for the deceased subjects. The cause of death was obtained via anonymous record linkage with the database of the Institut National de la Santé et de la Recherche Médicale (INSERM National Institute of Health and Medical Research)—Centre d’Epidémiologie sur les Causes Médicales de Décès (CEPIDC Centre for the Epidemiology of Medical Causes of Death), using date of birth, date and place of death for matching. The database registered all deaths that occurred in France during the study period, including death of foreigners that happened in France, but excluding those who died abroad (data available at: http://www.cepidc.vesinet.inserm.fr/).
The causes of death were coded according to the ninth revision of the International Classification of Diseases (ICD) for the period 1990–1999 and the 10th revision after 1999 (this change was inconsequential for this study). We used the principal cause of death with three levels of groups of causes: the 17 main categories of the ICD (three digit codes), the distinction between benign and malignant tumours at the second level and the site of the tumour at the third level. A consent to get access to personal data was sought through a personalized letter sent by the General Directors to all current and past workers; only one worker refused to participate.
Since it was not possible to get information on tobacco at the individual level, we carried out an ancillary descriptive study to assess the prevalence of tobacco smoking in cement industry. Overall, 27 of the occupational physicians in charge of the medical surveillance of cement workers volunteered to study smoking prevalence. They randomly selected 268 medical files active in 2005 for male workers.
Required authorizations were obtained from the national commission in charge of the protection of privacy of computerized information Commission Nationale pour l’Informatique et les Libertés (CNIL National Commission of Computer Science and Liberty, agreement # 906013), and approval was obtained from the Comité Consultatif sur le Traitement de l’Information en Matière de Recherche dans le Domaine de la Santé (CCTIRS Consultative Committee of the Data Analysis in Health Research).
Statistical analysis
A ‘prevalent cohort’ was defined as including workers already employed at the onset of the observation period (1st of January 1990). An ‘incident cohort’ was defined as including workers who were hired after the 1st of January 1990 and before the 31st of December 2005. Person-years began accruing on the 1st of January 1991 for the prevalent cohort and 1 year after the date of hiring for the incident cohort. The end of follow-up was defined as the date of death for those who died between 1990 and 2005 or the date of study termination for all others even if they had retired.
The observed mortality in the cohort was compared to the expected mortality of the French general population by computing standardized mortality ratios. Since cement plants are spread all over France, the French continental population was chosen as the reference. For each gender and five-year age group, the expected mortality was calculated by applying the mean national mortality rates for three calendar periods (1990–1994, 1995–1999 and 2000–2005) to the person-years of observation in the respective strata. Confidence intervals (95% CI) were estimated using Byar’s method (Breslow and Day 1987). The analyses were stratified by gender, age in three groups (18–35, 36–64 and 65–80 years), job categories, start date (before 1975, 1975–1989 and 1990–2005), employment duration and for the major causes of death. In the main analysis, the longest occupied job category was used. For 73% of the workers in the cohort, the job category chosen was the only one occupied.
Internal analysis relied on Cox proportional hazards regression, which was employed to investigate the association of the hazard of death with year of hiring (prevalent cohort versus incident cohort), number of jobs occupied (more than 5 vs. less than 5) and job categories (administrative workers as a reference group). All models were adjusted for age (continuous) and gender, using age as the time variable. Analysis were performed with the SAS software (version 9.1), SAS Institute Inc., Cary, NC.
Results
Cohort description
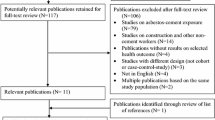
A total of 15,492 employees had worked for at least 1 day in one of the four cement companies during the observation period (Table 1). Among them, 10,010 (64.6%) met the inclusion criteria of having worked for at least 1 year. The basic identifiers were lacking for 502 of these workers, and one refused to participate, leaving 9,507 individual identifiers that were sent to the INSERM—CEPIDC death registry. The registry was able to trace 9,118 of them (95.9%). The proportion of missing data varied among the companies from 2.3 to 5.9%. The examination of the annual mandatory fiscal forms in three of the participating companies showed that the completeness of the cohort was excellent (data not shown).
The characteristics of workers in the cohort are described in Table 2. Men represented 83.7% of the workers (and 86% of the total person-years). The mean age at the end of the observation period is 48 years (39.2 years for women and 49.7 years for men). The prevalent cohort represented 58.5% of the study subjects and 69.8% of the 122,124 person-years of follow-up. Half of the workers had occupied more than 3 jobs, and 60.5% were employed in one of the three sectors production, maintenance and shipping. The mean seniority was 16 years, and 58.7% had seniority higher than 10 years. The mean duration of follow-up was 13.4 years, and the older worker included was recruited in 1946.
By 31 December 2005, 430 workers (4.7% of the cohort) were dead (422 men and 8 women). Most of the deaths had occurred among subjects of the prevalent cohort (91.4%) with an age of death above 60 years for 68.1% of the deceased workers. The cause of death was obtained for all workers with a known deceased status. Malignant neoplasm was the cause of 48.1% of the deaths (N = 207). The main localization of the tumours were the lungs (N = 76), lymphoid and haematopoietic tissues (N = 21), oral cavity and pharynx (N = 13), colon (N = 12), and oesophagus (N = 11).
External comparisons of observed mortality with national death rates
Table 3 presents the observed number of deaths, SMRs and their CI for the main causes of death. The total number of deaths observed in the cohort was 68% of the number expected from the national mortality statistics (SMR 0.68, CI 0.61-0.74). A low mortality was observed for all causes of death, cardiovascular diseases, injuries and for all but three cancer sites (bladder, kidney, and lymphatic and haematopoietic tissues). No statistically significant increase was found for any cancer. The range of the SMRs for individual types of cancers varied from 0.38 (stomach) to 1.38 (lymphatic and haematopoietic tissues). No statistically significant difference in the mortality rates was observed between the four companies (data not shown).
Workers employed before 1975 had a higher SMR, but it remained significantly less than unity (Table 4). Among the seven job categories, all the SMRs were below unity. Workers in quarry, yard, shipping and laboratory had a SMR around 0.8 (not statistically different than unity), while administrative employees had the lowest SMR with 0.53.
Internal analyses within the cohort
Cox regression analysis showed that workers from the quarry, yard and shipping sectors had a 50% higher risk of mortality by all causes compared with the administrative sector (Table 5). For cancer mortality, the risk was about twofold in yard and shipping, and laboratory. Date of hire did not have an effect on the risk of all-causes mortality (prevalent vs. incident cohort Hazard Ratio (HR) 1.24, CI 0.83–1.83), but holding five jobs or more in career was associated with a significantly lower hazard of mortality (HR: 0.61, CI 0.49–0.77).
Smoking
The prevalence of active smoking among male cement workers in activity was estimated to be 32.8% (CI 30.0–35.7), a figure close to what is observed in the general population in France (35.1%) (Beck et al. 2005). Administrative employees smoked less (21.6%, CI 15.8–27.3), and workers involved in the production process smoked more (36.5%, CI 33.0–39.9), laboratory workers being at an intermediary pattern (28.0%, CI 25.9–30.1). The highest prevalence (40.0%) was found in the age group 20–25 years.
Discussion
This study is the first to describe the mortality of the French cement production workers and is one of the largest studies published to this date on this topic. It showed an overall low mortality when compared to national figures.
Because of missing information, 892 workers could not be included, 503 due to insufficient demographic data for identification and 389 who could not be traced by the INSERM registry for mortality data. The proportion of unknown vital status was 2.4% among men and 11.8% among women (p < 0.01). This difference is probably due to the change of family name when women got married. The non-identified workers were older (mean age of 51.1 vs. 48.0 years) and had more seniority on average. These discrepancies should be most considered upon using age and gender standardization in the SMRs calculation.
The all-causes SMR for the workers who were excluded because they had not work at least 1 year was 0.64, and when these workers were included in the cohort, the resulting SMR was 0.67 instead of 0.68.
The fact that service company workers and employees of sub-contractors could not be correctly identified may have some bearing on the results as these workers frequently occupy some of the most exposed positions. Their exclusion, however, is unlikely to account for a large share of the observed low mortality.
The overall decreased mortality can be interpreted as the result of a ‘Healthy Worker Effect’ (Monson 1990). The observed low mortality is very similar to that reported in other industries in France (Moulin et al. 2000). Although this study is on the whole quite powerful, it lacked statistical power and precision to assess specific causes of death, particularly in view of the average age (48 years old).
Weight of evidence regarding cancers hazards
So far, five descriptive cohort studies of cement workers have already been published (Smailyte et al. 2004; McDowall 1984; Jakobsson et al. 1993; Amandus 1986; Vestbo et al. 1991). Different associations were reported with the mortality for stomach and rectum cancers (McDowall 1984; Smailyte et al. 2004), respiratory cancers (Amandus 1986; Smailyte et al. 2004) and colon cancer (Jakobsson et al. 1993). None of these associations were observed in our study.
The fact that job categories constituted an independent risk factor for mortality in the Cox analysis is hard to interpret in the absence of individual exposure data for occupational pollutants, alcohol or tobacco. Other explanations are the well-known gradient of death between blue collars and white collars and the difference in mortality usually reported according to socio-economic status (Monson 1990). As many factors can differentiate blue collars work and administrative work, our findings justify further research on the relationship between working in different sectors of the cement production and chronic diseases.
No occupational exposures data were available to be used in this epidemiologic study. Therefore, we could not investigate the relationship between exposure to pollutants emitted during the production process and mortality. It seems plausible that during the seventies, technological advances have resulted in decreased levels of dust breathed by the workers. For the same reason, we were not able to assess exposure to asbestos. Among the 430 dead workers, only 2 had been registered with a diagnosis of pleural mesothelioma.
Conclusions
This descriptive study did not support previous observations of risks associated with working in the cement production in France, possibly because of a substantial Healthy Worker Effect. It would be worth prolonging the period of observation in order to improve statistical power and precision. This would be of particular interest in view of the variability of SMRs with regard to cause of death and types of jobs, and the observation of some SMR point estimates being more than unity for a few cancer sites. A study of the effect of dust exposure should also be encouraged in order to shed additional light into the aetiological debate. Finally, this study has demonstrated the feasibility of systematizing the epidemiologic surveillance of workers within different companies in the same sector in France.
References
Amandus HE (1986) Mortality from stomach cancer in United States cement plant and quarry workers, 1950–80. Br J Ind Med 43:526–528
Beck F, Guilbert P, Gautier A (2005) Baromètre santé. Saint-Denis INPES, coll. Baromètres santé. 593 p
Blair A, Linos A, Stewart PA, Burmeister LF et al (1993) Evaluation risks for non-hodgkin’s lymphoma by occupation and industry exposures from a case-control study. Am J Ind Med 23:301–312
Breslow NE, Day NE (1987) Statistical methods in cancer research vol II. The design and analysis of cohort studies. IARC Sci Pub., Lyon, 406 p
Brownson RC, Zahm SH, Chang JC, Blair A (1989) Occupational risk of colon cancer. An analysis by anatomic subsite. Am J Epidem 130:675–687
Consonni D, De Matteis S, Lubin JH et al (2010) Lung cancer and occupation in a population-based case-control study. Am J Epidem 171:323–333
Dietz A, Ramroth H, Urban T, Ahrens W, Becher H (2004) Exposure to cement dust, related occupational groups and laryngeal cancer risk: results of a population based case-control study. Int J Cancer 108:907–911
Jakobsson K, Attewell R, Hultgren B, Sjöland K (1990) Gastrointestinal cancer among cement workers. A case-referent study. Occup Environ Med 62:337–340
Jakobsson K, Horstmann V, Welinder H (1993) Mortality and cancer morbidity among cement workers. Br J Ind Med 50:264–272
Jakobsson K, Albin M, Hagmar L (1994) Asbestos, cement, and cancer in the right part of the colon. Occup Environ Med 51:95–101
Jansson C, Johansson AL, Bergdahl IA et al (2005) Occupational exposures and risk of esophageal and gastric cardia cancers among male Swedish construction workers. Cancer Causes Control 16:755–764
Knutsson A, Dambler L, Järvholm B (2000) Cancers in concrete workers: results of a cohort study of 33 668 workers. Occup Environ Med 57:264–267
Krstev S, Baris D, Stewart PA, Hayes RB, Blair A, Dosemeci M (1998) Risk for prostate cancer by occupation and industry: a 24-state death certificate study. Am J Ind Med 34:413–420
Maier H, Tisch M (1997) Epidemiology of laryngeal cancer: results of the Heidelberg case-control study. Acta Otolaryng suppl 527:160–164
McDowall ME (1984) A mortality study of cement workers. Br J Ind Med 41:179–182
Milne KL, Sandler DP, Everson RB, Brown SM (1983) Lung cancer and occupation in Alameda county: a death certificate case-control study. Am J Ind Med 4:565–575
Minder CE, Beer-Porizek V (1992) Cancer mortality of Swiss men by occupation, 1979–1982. Scand J Work Environ Health 18(Suppl 3):1–27
Monson RR (1990) Occupational epidemiology. CRC Press, Boca Raton, 291 p
Moulin JJ, Clavel T, Roy B et al (2000) Risk of lung cancer in workers producing stainless steel and metallic alloys. Int Arch Occup Environ Health 73:171–180
Partanen T, Kauppinen T, Degerth R et al (1994) Pancreatic cancer in industrial branches and occupations in Finland. Am J Ind Med 25:851–866
Pukkala E, Martinsen JI, Lynge E et al (2009) Occupation and cancer—follow-up of 15 million people in five Nordic countries. Acta Oncol 48:646–790
Purdue MP, Järvholm B, Bergdahl IA, Hayes RB, Baris D (2006) Occupational exposures and head and neck cancers among Swedish construction workers. Scand J Work Environ Health 32:270–275
Rafnsson V, Johannesdottir SG (1986) Mortality among masons in Iceland. Br J Ind Med 43:522–525
Robinson C, Stern F, Halperin W et al (1995) Assessment of mortality in the construction industry in the United States, 1984–1986. Am J Ind Med 28:49–70
Schoenberg JB, Stemhagen A, Mason TJ et al (1987) Occupation and lung cancer risk among New Jersey white males. J Nat Cancer Inst 79:13–21
Siemiatycki J, Dewar R, Lakhani R et al (1989) Cancer risks associated with 10 inorganic dusts: results from a case-control study in Montreal. Am J Ind Med 16:547–567
Smailyte G, Kurtinaitis J, Andersen A (2004) Mortality and cancer incidence among Lithuanian cement producing workers. Occup Environ Med 61:529–534
Stern F (2001) Mortality among unionized construction plasterers and cement masons. Am J Ind Med 39:373–388
Swanson GM, Lin CS, Burns PB (1993) Diversity in the association between occupation and lung cancer among black and white men. Cancer Epidem Biom Prev 2:313–320
Vestbo J, Knudsen KM, Raffn E et al (1991) Exposure to cement dust at a Portland cement factory and the risk of cancer. Br J Ind Med 48:803–807
Zagraniski RT, Kelsey JL, Walter SD (1986) Occupational risk factors for laryngeal carcinoma: Connecticut, 1975–1980. Am J Epidem 124:67–76
Acknowledgments
We thank A Capmas, the General Delegate of ATIHL, J Duron (Holcim France), JF Jacquet (Lafarge Ciments), J Lumineau (Holcim France), J Prével (Ciments Calcia), A Romi (SFIC), G Rusaouen (Vicat). The study was sponsored by Association technique de l’industrie des liants hydrauliques (ATILH, Technical Association of Hydraulic Binder Industry) that covered the costs of the study, facilitated the work with the human resources department and the industrial hygienists and attended as an observer to the meetings of the scientific committee. It did not interfere in the writing of the protocol, neither in the analysis of data nor in the writing of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dab, W., Rossignol, M., Luce, D. et al. Cancer mortality study among French cement production workers. Int Arch Occup Environ Health 84, 167–173 (2011). https://doi.org/10.1007/s00420-010-0530-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-010-0530-6