
Abstract
Objectives
To assess the extent of exposure to lead, cadmium, and mercury in the Korean general adult population using a representative sample.
Methods
We studied blood concentrations of three heavy metals in a representative sample of 1,997 Koreans as part of the Third Korean National Health and Nutrition Examination Survey (KNHANES III) performed in 2005.
Results
The geometric means of the blood lead, cadmium, and mercury concentrations were 2.61 μg/dL, 1.53 μg/L, and 4.15 μg/L, respectively [95% confidence intervals (CIs), 2.50–2.71, 1.48–1.58, and 3.94–4.36, respectively]. Women had significantly lower blood lead and mercury concentrations in adjusted and unadjusted analyses but no difference between genders was observed in blood cadmium analysis. The geometric means of blood lead and mercury levels were higher in subjects older than 40 years than in those younger than 40 years. Smoking status only affected the blood lead concentration, with this being higher in smokers than in nonsmokers. Blood cadmium levels did not differ with demographic and lifestyle variables after covariate adjustment. Blood mercury concentrations were higher in those who consumed alcohol and also increased with the frequency of fish consumption.
Conclusions
This biomonitoring study of blood heavy metals in the Korean general population as part of KNHANES III provides important reference data stratified by demographic and lifestyle factors that will be useful for the ongoing surveillance of environmental exposure of the Korean general population to heavy metals.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Rapid industrialization and urbanization during the last 3–4 decades has resulted in a considerable amount of chemicals (including heavy metals) accumulating in the environment (Jeong et al. 1991; Lee 1999). In recent years, there have been several nationwide episodes of imported toys contaminated with lead paint and endocrine disrupting chemicals (Korea Consumer Agency 2002), and also cadmium intoxication has occurred due to soil contamination with cadmium from abandoned metal mines in the Kosung area (Korean Ministry of Environment 2004).
Increased awareness of environmental pollution worldwide has led to the establishment of environmental health survey systems in many countries (Batariova et al. 2006; Link et al. 2006; Schulz et al. 2007; Mahaffey et al. 2009). The growing concern about exposure to environmental pollutants in Korea provided the impetus for including human biomonitoring of lead, cadmium, and mercury in the Third Korean Health and Nutrition Examination Survey (KNHANES III). The purpose of the biomonitoring component of the survey was to establish reference values for specific heavy metals across different demographic and lifestyle characteristics (Korean Ministry of Health and Welfare 2005). The implementation of chemical biomonitoring in KNHANES III in 2005 ushered in a new era of ongoing assessment of the exposure of the Korean general population to specific environmental chemicals (Korean Ministry of Health and Welfare 2005).
National surveillance of the exposure to toxic substances is essential for identifying and targeting high-risk groups, evaluating interventions, tracking exposure over time, and monitoring exposure during emergency situations (Guallar et al. 2006; Iqbal et al. 2008; McKelvey et al. 2007). Furthermore, it is necessary to make international comparisons of environmental exposure levels, since they can vary significantly between countries.
Korea is the first country in Asia to incorporate biomonitoring in national health and nutrition surveys. We present data on blood lead, cadmium, and mercury concentrations in a representative national sample of Korean adults, stratified by demographic and lifestyle characteristics.
Methods
Study design and data collection
This study was based on data obtained in KNHANES III, which became officially available in March 2009. KNHANES III is a complex, stratified, multistage, probability-cluster survey of a representative sample of the noninstitutionalized civilian population in South Korea. The survey was conducted by the Korean Ministry of Health and Welfare during April and May in 2005 and consisted of four components: the Health Interview Survey, the Health Behavior Survey, the Health Examination Survey, and the Nutrition Survey.
The survey population included all noninstitutionalized civilian Korean individuals aged 1 year or over. The survey employed stratified multistage probability sampling units based on geographical area, gender, and age, which were determined by household registries of the 2000 National Census Registry (the most recent 5-year national census in Korea at the time). A total of 246,097 primary sampling units, each consisting of approximately 60 households, ultimately constituted the survey sample pool.
In the present study, 600 sampling units were randomly selected from the 246,097 primary sampling units so as to represent the overall Korean population.
From 600 sampling units, 12,001 households were randomly selected. Once selected as a participant of KNHANS III, each subject was interviewed by a qualified interviewer at his or her home. A total of 33,848 participants completed the Health Interview Survey and the Health Behavior Survey, which represents 99.1% of the total population of 34,154. For the Health Examination Survey and the Nutrition Survey, 200 sampling units were randomly selected from the sampling frame of the 600 previously selected sampling units. A total of 7,597 participants (70.2% response rate) who visited mobile health examination unit completed the Health Examination Survey, and 9,047 participants (80.5% response rate) completed the Nutrition Survey (Korean Ministry of Health and Welfare 2005) via individual interviews performed at their homes. A total of 5,501 of the 7,597 participants who completed the Health Examination Survey were 20 years old or older, which constituted another of the inclusion criteria of the present study.
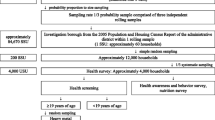
Out of 5,501 adults who received a health examination in the 200 primary sampling units, 10–12 subjects from each sampling unit were randomly selected while maintaining a uniform distribution across gender and five age groups (20–29, 30–39, 40–49, 50–59, and ≥60 years) to yield a total of 2,000 subjects. The data for 3 participants were excluded due to incomplete information, and so 1,997 subjects were included in the final KNHANES III data file (Fig. 1).

Flow chart of sample design and participation rate of KNHANES III
Age was reported at the time of the interview for the Health Interview Survey and categorized into the above-mentioned five categories. Education level was categorized into three groups: less than high school, high school, and college or higher. The area of residence was divided into urban areas (classified as administrative divisions of a city) and rural areas (not classified as administrative divisions of a city). Information about smoking and alcohol consumption was collected during the Health Interview Survey. Smoking status was divided into three categories: current smoker, past smoker, and nonsmoker. Alcohol consumption (henceforth referred to as “drinking”) was assessed by questioning the subjects about their drinking behavior during the month immediately prior to the interview. The subjects were asked about their average frequency of drinking (in days per month) and the average amount consumed on a single occasion (in milliliters). Data on the average amount and number of drinks consumed were converted into the amount of pure alcohol (in grams) consumed per day. The drinking status was categorized into four groups according to the mean daily alcohol consumption: nondrinker, light drinkers (1–15 g), moderate drinkers (15–30 g), and heavy drinkers (>30 g).
To evaluate the association between blood mercury and fish consumption, information about the frequency of fish and shellfish consumption was obtained from the Nutrition Survey of KHNANE III. The Nutrition Survey component of KHNANE III listed the following nine fish- and shellfish-related foods: mackerel, tuna, yellow croaker, pollack, anchovy, seafood paste, squid, clam, and pickled seafood; these are the seafood consumed most frequently in Korea. The consumption frequency was categorized into three groups based on the consumption of at least one type of fish or shellfish on the Nutrition Survey checklist: (1) less than once per week, (2) once per week, and (3) more than once per week during past year.
All participants provided written, informed consent to participate in the study and were reimbursed 10,000 won (approximately US$ 10) for their time and travel expenses incurred visiting a mobile health examination unit.
Determination of heavy metals in whole blood
To assess the levels of heavy metals in whole blood, 3-ml blood samples were drawn into standard commercial evacuated tubes containing sodium heparin (Vacutainer®) during the health examinations. Blood lead and cadmium were measured by graphite furnace atomic absorption spectrometry with Zeeman background correction (SPectrAA-800, Varian Instruments, Australia).
Blood samples were diluted 1:15 and 1:10 for blood lead and cadmium analyses, respectively, with 1% Triton X-100 in 1% nitric acid using ammonium dihydrogen phosphate as a modifier, and 15-μl aliquots of the samples were injected onto the platform of the furnace.
Blood mercury was measured by a cold vapor atomic absorption spectrometric method using a dedicated mercury analyzer (M-6000A, CETAC Technologies, USA). The instrument was operated at a wavelength of 253.7 nm. Whole blood (0.5 mL) was placed in the digestion vessel, and 5.0 mL of HNO3 was added to assist in the dissolution of the sample. After microwave digestion followed by 1 h of cooling in a freezer, the samples were diluted to 50 mL with distilled water for analysis.
Quality assurance and control
All blood heavy-metal analyses were carried out by Seoul Medical Science Institute (SMSI), a laboratory certified by the Korean Ministry of Health and Welfare. For the internal quality assurance and control program, commercial reference materials were obtained from Bio-RAD (Lyphochek® Whole Blood Metals Control), which showed that the coefficients of variation were 8.5% for three blood lead samples (reference values: 4.7, 36.8, and 68.7 μg/dL), 14.5% for three blood cadmium samples (reference values: 0.37, 1.11, and 4.30 μg/L), and 8.3% for three blood mercury samples (reference values: 4.7, 36.8, and 68.7 μg/L). In terms of external quality assurance and control, the SMSI has passed the German External Quality Assessment Scheme operated by Friedrick Alexander University, which is a standard protocol for measuring chemicals at low concentrations. The SMSI also held a certified license from the Ministry of Labor as one of the designated laboratories for special chemicals including heavy metals and certain organic chemicals. Additionally, 30 subsamples were randomly selected and reanalyzed by the Korean Institute of Science and Technology. There were no significant differences in the blood heavy-metal levels measured by the two laboratories.
For the determination of detection limit, a blood sample was obtained from nonexposed person, 3 heavy metal’s concentration were determined in 5 preparations across the 5 different days, and calculation of limit of detection was made according to IUPAC guideline using 3× SD.
The detection limits for blood lead, cadmium, and mercury in the present study were 0.23 μg/dL, 0.30 μg/L, and 0.36 μg/L, respectively. There were 6, 8, and 13 participants with levels below the detection limit for lead, cadmium, and mercury, respectively.
For these participants, we imputed a level equal to the detection limit divided by the square root of 2 (Glass and Gray 2001).
Statistical analysis
Statistical analyses were performed using SAS (Version 9.2, SAS Institute, Cary, NC) and SUDAAN (Release 10.0, Research Triangle Institute, Research Triangle Park, NC), which is a software package that incorporates the sample weights and adjusts the analyses for the complex sample design of the survey. Survey sample weights were used in all analyses to produce estimates that were representative of the noninstitutionalized civilian Korean population.
The levels of all three blood heavy metals were log-transformed since their distributions were skewed, and the unadjusted geometric mean [95% confidence interval (CI)] and selected percentiles were calculated by gender, age group, smoking status, drinking status, area of residence, and educational level using the Proc Descript function in SUDAAN. The blood mercury level was analyzed by adding the frequency of fish consumption as a classification variable.
To compare the geometric means of the levels of the three heavy metals in different demographic and lifestyle groups while controlling the covariates [age, gender, smoking status, drinking status, area of residence, and frequency of fish and shellfish consumption (for the analysis of blood mercury)], adjusted geometric means and 95% CIs were calculated using analysis of covariance (ANCOVA) calculated by Proc Regress function.
The Nutrition Survey was carried out separately from the Health Examination Survey, and only 1,749 individuals completed both surveys. Therefore, only 1,749 subjects were included in the analysis of blood mercury with the frequency of fish consumption.
Results
The blood concentrations of lead, cadmium, and mercury in the study participants by general demographic and lifestyle characteristics are listed in Tables 1, 2, and 3, respectively. Unadjusted geometric means of blood heavy metals and adjusted geometric means calculated by ANCOVA are presented with their 95% CI values and selected percentile values. Overall, the geometric means of the blood lead, cadmium, and mercury levels of all participants (n = 1,997), representing Koreans adults aged ≥20 years, were 2.61 μg/dL, 1.53 μg/L, and 4.46 μg/L, respectively (95% CIs, 2.50–2.71, 1.48–1.58, and 3.94–4.36).
The geometric mean of the blood lead level was lower in women (2.29 and 2.35 μg/dL in unadjusted and covariate-adjusted analyses, respectively) than in men (2.98 and 2.90 μg/dL in unadjusted and adjusted analyses, respectively) and was higher in older groups than in younger groups. The geometric mean of the blood lead level was higher in current and past smokers than in nonsmokers (p < 0.05) in adjusted and unadjusted analyses and higher in drinkers than in nondrinkers in the unadjusted analysis but not in the comparison using ANCOVA. The blood lead level was lower in subjects educated to at least college level than in subjects with less than high school education in an unadjusted analysis (p < 0.01) but not in an adjusted analysis.
The geometric mean of the blood cadmium level was lower in women (1.49 μg/L in unadjusted and adjusted analyses) than in men (1.57 and 1.56 μg/L in unadjusted and adjusted analyses, respectively), but the difference was only statistically significant for the unadjusted comparison. The blood cadmium level was significantly lower in women than in men in an adjusted analysis excluding the smoking status and significantly lower in more-educated subjects than in less-educated subjects in an unadjusted analysis (p < 0.05) but not in an adjusted analysis. The blood cadmium level was significantly higher in past and current smokers than in nonsmokers in an unadjusted analysis (p < 0.05), but the difference disappeared in an adjusted analysis.
The geometric mean of the blood mercury level was lower in women (3.67 and 3.81 μg/L in unadjusted and adjusted analyses, respectively) than in men (4.71 and 4.53 μg/L in unadjusted and adjusted analyses, respectively). The blood mercury level differed significantly with drinking status in both adjusted and unadjusted analyses, but it did not differ between smokers and nonsmokers or with the area of residence in adjusted analyses.
The geometric mean of the blood mercury level was significantly higher in subjects who consumed fish and shellfish once per week or more than once per week than in those who consumed fish and shellfish less than once per week (p < 0.05 or p < 0.01, respectively) in unadjusted and adjusted analyses. But the absolute difference between low- and high-consumption groups was only 0.67 and 0.64 μg/L in unadjusted and adjusted analyses, respectively, corresponding to a variation of only 18% with fish consumption (3.71 and 4.38 mg/L in the low- and high-consumption groups, respectively).
Discussion
We used KNHANES III biomonitoring data to establish reference values for the levels of lead, cadmium, and mercury in the Korean general adult population. The overall geometric mean of the blood lead level from KNHANES III was 2.61 μg/dL in all of our 1,997 subjects and was higher in men (2.98 μg/dL) than in women (2.29 μg/dL) in an unadjusted analysis, with similar values being obtained in a covariate-adjusted analysis.
Several previous surveys (Berode et al. 1991; Pirkle et al. 1994; Batariova et al. 2006; Menke et al. 2006; McKelvey et al. 2007; Saraiva et al. 2007) found that the blood lead levels were higher in men than in women due to higher lead exposure and higher blood hematocrit levels, which is due to lead in blood being bound to erythrocytes (WHO 1995; Vahter et al. 2002). We also found that the blood lead level differed significantly with gender, being 30% higher in men than in women. Interestingly, this gender-related difference in blood lead levels in the Korean population is less than that in the United States National Health and Nutrition Examination Survey (US NHANES) survey data, where the blood-lead-level ratio of women to men was 1:1.60–1.83 (Yassin et al. 2004; Muntner et al. 2005). Korean women are less likely than men to have an outdoor job and so would be expected to have much lower blood lead levels. In addition, smoking is known to increase blood lead levels (Berode et al. 1991; Navas-Acien et al. 2004), and our survey also found that the geometric mean of the blood lead level was significantly higher in smokers than in nonsmokers and past smokers. Taking the smoking variable into account when evaluating possible differences in blood lead by gender should result in the blood lead level being lower in Korean women than in women from Western countries, where the prevalence of smoking among women is higher than in Korea (Kim et al. 2006).
The overall geometric mean of the blood lead level of KNHANES III is 2.61 μg/dL, which is less than one-fifth of the blood lead levels in the 1980s of the Korean population exposed to environmental lead (Kim et al. 1992; Kim and Cho 1994). Korea began phasing out leaded gasoline in 1986, since when blood lead levels have steadily declined (Park et al. 2008), with the decline becoming more rapid in the early 2000s (Korean Ministry of Environment 2005). Recent data indicate that the mean blood lead levels in the Korean general population range from 2.0 to 4.0 μg/dL (Park et al. 2006; Kim et al. 2007; Park et al. 2008).
The blood lead levels in Koreans are still twice as high as those in the recent US NHANES data (Muntner et al. 2005) but are similar to those in the Japanese general population (Zhang et al. 1999, 2000; Ikeda et al. 2000a, b) and a little lower than those in some European populations (Becker et al. 2002; Batariova et al. 2006). No convincing explanation is available for the persistent international differences in blood lead levels between the United States and other countries (including some European countries and Korea), where levels remain higher even after the long-standing complete ban on leaded gasoline. Food and other environmental conditions could explain the differences, but this will require further studies that involve ongoing biomonitoring of the general populations.
In the 1999–2002 US NHANES, the geometric mean of the blood lead level was 1.7-fold higher in the oldest group (≥60 years) than in the youngest group (18–39 years) (Muntner et al. 2005). In KNHANES III, we found that the geometric means of the blood lead levels were 1.26- and 1.20-fold higher in older groups (50–59 and ≥60 years, respectively) than in the youngest group (20–29 years). Subjects in the older group would have had a greater exposure to environmental lead due to the presence of leaded gasoline during their lifetime, with the resulting accumulation of lead in bone possibly partially explaining the difference with age. Lead is predominantly stored in the human body in calcified tissues, with 90–95% of the total lead burden contained within bone in nonoccupationally exposed adults (Todd et al. 2001). The long half-life of bone lead means that lead accumulated in bone during childhood is retained throughout most of the adult life.
The other possible explanation for the age-related ratio being smaller in the Korean population than in the US population is that most Koreans would not have been exposed to indoor paint containing lead because they generally use paper decorative surfaces to finish indoor walls. While the geometric mean of the blood lead level was higher in the older groups than in the youngest group, the level was lower in those aged ≥60 years than in those aged 50–59 years. Several recent studies of blood lead levels in the Korean general population have also found that the levels were lower in those aged ≥60 or ≥70 years than in younger groups (Kim et al. 2007; Park et al. 2008, 2009). This could be partially explained by cohort effect of very old age group who were exposed to environmental lead less frequently than next younger age group in their life period.
The geometric mean of the blood cadmium levels of men (1.57 μg/L) and women (1.49 μg/L) in KNHANES III is similar to that found in a 1992 field study of Korean subjects (Yeon et al. 1992): 1.80 and 1.50 μg/L, respectively. Our geometric mean cadmium levels in both genders were slightly lower than those in the Japanese general population (Ikeda et al. 1994, 2000a, b, c; Kurihara et al. 2004) but were two- to fourfold higher than those in the US population (McKelvey et al. 2007; Tellez-Plaza et al. 2008) and other south Asian populations (Zhang et al. 1999).
Diet is the primary source of cadmium in areas that are not contaminated with cadmium (Watanabe et al. 2000; Shimbo et al. 2001). Moon et al. (1995) also found that dietary intake was the main source of cadmium exposure in the Korean general population. Tsukahara et al. (2003a) reported that rice is the main source of cadmium intake among the Japanese general population and explained that 59–69% of the total variation in urine, cadmium was attributable to rice consumption. Ikeda et al. (2004) found that dietary cadmium intakes in both polluted and unpolluted areas in Japan were gradually decreasing but that the current intake level (25–30 μg/day) in unpolluted areas was still higher than the levels in other rice-dependent areas in Asia. They also reported that 30–40% of the dietary cadmium intake in the Japanese population comes from rice consumption. On the other hand, the dietary cadmium intake among Korean women has been reported to be 21.2 μg/day (Moon et al. 1995) and 18.4 μg/day (Moon et al. 2003), values that are somewhat lower than that for Japanese women. The differences in dietary cadmium intakes might explain the differences in blood cadmium levels between Korean and Japanese populations.
Several studies of Asian populations have also found that blood cadmium levels are higher in northeast Asian populations (Korean, Japanese, and Chinese) than in Western countries, which are characterized by a lower rice consumption (Soong et al. 1991; Berglund et al. 1994; Zhang et al. 1997; Ikeda et al. 2000c; Watanabe et al. 2000; Batariova et al. 2006). Reeves and Chaney (2008) suggested that the poor nutritional quality of polished rice in terms of zinc and iron contents is of worldwide concern because marginal deficiencies in these heavy metals enhance cadmium absorption from diets containing low cadmium concentrations by up to tenfold. These results indicate that rice consumption is a possible cause of higher cadmium levels in populations consuming rice-based diets. However, Tsukahara et al. (2003b) reported no significant effect of iron deficiency on the cadmium body burden or kidney dysfunction among the Japanese general female population.
In addition to dietary sources of cadmium affecting the general population, cigarette smoking is also known to be a source of cadmium exposure. Biomonitoring of cadmium in the general population has shown that cigarette smoking can significantly increase blood cadmium levels, with average concentrations being two- to fivefold higher in smokers than in nonsmokers (Jarup et al. 1998; Batariova et al. 2006). However, our analysis of KNHANES III data showed that the blood cadmium level was statistically affected by the smoking status only in an unadjusted analysis and not in an adjusted analysis.
In contrast to the situation for blood lead levels, the blood cadmium level did not differ with gender in KNHANES III. From a study of nonsmoking men and women in Sweden, Olsson et al. (2002) suggested that higher blood cadmium level in women can be explained by higher absorption due to a low iron status, whereas the blood cadmium levels did not differ with gender in Japanese subjects (Kurihara et al. 2004) and adult residents of New York city (McKelvey et al. 2007).
Measurements of total mercury in whole blood include both the inorganic and organic forms. In the general population, the total blood mercury concentration is due mostly to the dietary intake of organic forms, particularly of methylmercury (World Health Organisation 1995; Mahaffey et al. 2004). Total blood mercury levels are known to increase with fish consumption (Jarup 2003; Mahaffey et al. 2004; Mozaffarian and Rimm 2006). A health and nutrition examination survey of residents of New York city found that the crude weighted geometric mean level of blood mercury was 2.73 μg/L, with the levels in men (2.67 μg/L) and women (2.78 μg/L) being more than threefold higher than those in the 2001–2002 US NHANES (0.83 μg/L). However, Hightower et al. (2006) reported that blood mercury levels are significantly higher in Asian, Pacific Islander, Native American, and multiracial groups than in the other groups included in the US NHANES. This was also confirmed by a survey of New York city residents, in which the blood mercury level was highest (at 4.11 μg/L) in the Asian population, and very similar to the value in the present study (4.15 μg/L).
Fish consumption is highly influenced by cultural and socioeconomic factors (Sanzo et al. 2001; Bjornberg et al. 2005; Vahter et al. 2007; Karouna-Renier et al. 2008; Mozaffarian and Rimm 2006). The geographical characteristics of islands mean that the Japanese and Taiwanese populations consume more fish than the populations of inland countries. Blood mercury levels of women were recently found to be significantly higher in Japan and Taiwan than in Korea (Hsu et al. 2007; Sakamoto et al. 2007), while geometric means of the blood mercury levels in both genders were higher in our Korean population than in the general populations of European countries (Seifert et al. 2000; Vahter et al. 2000; Berglund et al. 1994; Batariova et al. 2006; Schulz et al. 2007). Moreover, the mean blood mercury level was more than twofold higher in our Korean population than in a Swedish population with a higher consumption of fish (Ask et al. 2002; Bjornberg et al. 2005).
Mahaffey et al. (2004) and Schrober et al. (2003) found that the blood mercury level increases with the frequency of fish and shellfish consumption in an analysis of 1999–2000 US NHANES data. Similar findings were obtained for residents of New York city (McKelvey et al. 2007) and in an EPIC cohort study of the Spanish population (Sanzo et al. 2001). All of the above-mentioned papers reported that the blood mercury level varied by at least 100% with the fish consumption. As expected, our analysis of KNHANES III data revealed an association between the frequency of fish consumption and blood mercury level, but the difference between the low- and high-consumption groups was not as great as that reported for Western countries, being only 18%. Similar findings were reported for pregnant women in Korea (Kim et al. 2005), Taiwan (Hsu et al. 2007), and Japan (Yaginuma-Sakurai et al. 2009). The reason for these large differences between different regions worldwide is unclear, but it is obvious that Korean blood mercury concentrations are high irrespective of the level of fish consumption.
The mercury levels in the most frequently consumed fish are lower in Korea than in Japan and United States, because Koreans generally do not consume high-mercury-content fish and shellfish such as sharks, swordfish, walleye, and lobster (Mahaffey et al. 2004). Therefore, the reason for the blood mercury level being higher in Korea than in the United States and European countries remains to be determined but this might be due to other environmental sources such as soil, water, and air. Further research is needed into why the blood mercury concentration is high in the Korean general population, with a particular focus on Korean women of child-bearing age.
There are inconsistencies in the gender differences in blood mercury levels. Although two general population studies from the Czech Republic (Batariova et al. 2006) and New York city (McKelvey et al. 2007) found that the blood mercury concentrations were higher in women than in men, the present study and a Quebec study (Mahaffey and Mergler 1998) found the opposite result.
In our study, age, smoking, and area of residence exerted no significant effects on the geometric mean of the blood mercury level, but it was higher in heavy drinkers than in nondrinkers.
Our finding of higher blood mercury levels in those aged 40–59 years is consistent with biomonitoring data from New York city (McKelvey et al. 2007).
Our findings are subject to some limitations. We only measured total blood mercury without measuring methylmercury and inorganic mercury concentrations in the whole blood. Unlike the high correlation between total blood mercury and frequency of fish consumption found in Western countries, our data revealed that only a small proportion of the blood mercury concentration was attributable to a high frequency of fish consumption. A future study should thus analyze the organic and inorganic portions of total blood mercury to clarify the proportion of methylmercury that comes mainly from fish. Inorganic mercury has been found to represent a marginal proportion of the total mercury concentration in many Western studies (Sanzo et al. 2001; Mahaffey et al. 2004), but we did not consider the possible contribution of inorganic mercury sources, such as tooth amalgam treatments.
Only a few metals were included in the first set of KNHANES data, and more chemicals are expected to be included in future surveys. Also, the survey schedule of KNHANES was changed from a time-framed design to an ongoing annual survey program, which includes the biomonitoring of chemicals as an important part of the Health Examination Survey.
Future KNHANESs should include not only the adult population but also subjects younger than 18 years who are eligible for health examination programs. This would make it more consistent with the US NHANES, which covers all members of the population aged from 1 year upwards in order to monitor all groups who might be susceptible to environmental chemicals.
The KNHANES is an important source of information about the health of the Korean general population. Furthermore, the inclusion of biomonitoring in the KNHANES is a very encouraging and promising step toward evaluating possible associations between the environment and health.
Awareness of the importance of international cooperation for environmental protection is growing. The analyses of biomonitoring data from the Korean general population reported here have provided new and useful information about one Asian population for use in international comparisons in environmental health research and other related scientific areas.
References
Ask K, Akesson A, Berglund M, Vahter M (2002) Inorganic mercury and methylmercury in placentas of Swedish women. Environ Health Perspect 110:523–526
Batariova A, Spevackova V, Benes B, Cejchanova M, Smid J, Cerna M (2006) Blood and urine levels of Pb, Cd and Hg in the general population of the Czech Republic and proposed reference values. Ind J Hyg Environ Health 209:359–366
Becker K, Kaus S, Krause C, Lepom P, Schulz C, Seiwert M, Seifert B (2002) German Environmental Survey 1988 (GerES III): environmental pollutants in blood of the German population. Int J Hyg Environ Health 205:297–308
Berglund M, Akesson A, Nermell B, Vahter M (1994) Intestinal absorption of dietary cadmium in women depends on body iron stores and fiber intake. Environ Health Perspect 102:1058–1066
Berode M, Wietlisbach V, Richenback M, Guillemin MP (1991) Lifestyle and environmental factors as determinants of blood lead levels in a Swiss population. Environ Res 55:1–17
Bjornberg KA, Vahter M, Grawe KP, Berglund M (2005) Methyl mercury exposure in Swedish women with high fish consumption. Sci Total Environ 341:45–52
Glass DC, Gray CN (2001) Estimating mean exposure from censored data: exposure to benzene in the Australian petroleum industry. Ann Occup Hyg 45:275–282
Guallar E, Silbergeld EK, Navas-Acien A, Malhotra S, Astor BC, Sharrett AR, Schwartz BS (2006) Confounding of the relation between homocysteine and peripheral arterial disease by lead, cadmium, and renal function. Am J Epidemiol 163:700–708
Hightower JM, OHara A, Hernandez GT (2006) Blood mercury reporting in NHANES: identifying Asian, Pacific Islander, Native American, and multiracial groups. Environ Health Perspect 114:173–175
Hsu CS, Liu PL, Chien LC, Chou SY, Han BC (2007) Mercury concentration and fish consumption in Taiwanese pregnant women. BJOG 114:81–85
Ikeda M, Moon C-S, Shimbo S, Watanabe T (1994) Dietary cadmium intake among Japanese people: annual trends and regional difference. Jpn J Hyg 49:176
Ikeda M, Zhang ZW, Moon CS, Shimbo S, Watanabe T, Nakatsuka H, Matsuda-Inoguchi N, Higashikawa K (2000a) Possible effects of environmental cadmium exposure on kidney function in the Japanese general population. Int Arch Environ Health 73:15–25
Ikeda M, Zhang ZW, Shimbo S, Watanabe T, Nakatsuka H, Moon CS, Matsuda-Inoguchi N, Higashikawa K (2000b) Exposure of women in general populations to lead via food and air in east and Southeast Asia. Am J Ind Med 38:271–280
Ikeda M, Zhang ZW, Shimbo S, Watanabe T, Nakatsuka H, Moon CS, Matsuda-Inoguchi N, Higashikawa K (2000c) Urban population exposure to lead and cadmium in East and Southeast Asia. Sci Total Environ 249:373–384
Ikeda M, Ezaki T, Tsukahara T, Morguchi J (2004) Dietary cadmium intake in polluted and non-polluted areas in Japan in the past and in the present. 2004. Int Arch Occup Environ Health 77:227–234
Iqbal S, Muntner P, Batuman V, Rabito FA (2008) Estimated burden of blood lead levels 5 micro g/dl in 1999–2002 and declines from 1988 to 1994. Environ Res 107:305–311
Jarup L (2003) Hazards of heavy metal contamination. Br Med Bull 68:167–182
Jarup L, Berglund M, Elinder CG, Nordberg G, Vahter M (1998) Health effects of cadmium exposure-a review of the literature and a risk estimate. Scand J Work Environ Health 24(Suppl 1):1–51
Jeong HS, Lee DB, Cho YC (1991) A study on the blood lead and cadmium concentration levels of rural residents. Res Rep Env Sci Tech Chungnam Univ 9:61–73
Karouna-Renier N, Rao KR, Lanzai JL, Rivers SD, Wilson PA, Hodges DK (2008) Mercury levels and fish consumption practices in women of childbearing age in the Florida Panhandle. Environ Res 103:320–326
Kim H, Cho SH (1994) Estimation of the geometric means and the reference values of blood lead levels among Koreans. J Kor Med Sci 9:304–312
Kim DI, Kim YK, Kim JM, Jung KY, Kim JY, Chang HS, Lee YH, Choi AH (1992) The levels of blood lead and zinc protoporphyrin for healthy urban population in Korea. Korean J Prev Med 25(3):5–22
Kim EK, Ki KI, Kwon JY, Koo JS, Hwang HS, Kim SK, Park YW, Noh JH, Lee DH (2005) The effect of fish consumption on blood mercury level in pregnant women. Korean J Obstet Gynecol 48:2527–2534
Kim SM, Han JH, Park HS (2006) Prevalence of low HDL-cholesterol levels and associated factors among Koreans. Circ J 70:820–826
Kim NS, Choi SW, Kim JH, Ham JO, Park HY, Ahn KD, Lee BK (2007) Bone and blood lead levels of middle aged Korean not occupationally exposed to lead. Korean J Occup Environ Med 19:285–292
Korea Consumer Agency (2002) Report on safety of wooden toy for infant education. Korea Consumer Agency, Seoul
Korean Ministry of Environment (2004) Final report on the health effect of closed mine of Kosung area in Kyungnam Province. Korean Ministry of Environment, Seoul
Korean Ministry of Environment (2005) Seoul: report on the study of blood heavy metals of general population. Korean Ministry of Environment, Seoul
Korean Ministry of Health and Welfare (2005) The third Korean National Health and Nutrition Examination Survey. Korean Ministry of Health and Welfare, Seoul
Kurihara I, Kobayashi E, Uetani M, Inaba T, Oishiz M, Kido T, Nakagawa H, Nogawa K (2004) Association between exposure to cadmium and blood pressure in Japanese peoples. Arch Environ Health 59:711–716
Lee BK (1999) The role of biological monitoring in the health management of lead-exposed workers. Toxicol Lett 108:149–160
Link B, Gabrio T, Piechotowski I, Zollner I, Schwenk M (2006) Baden-Wuerttemberg Environmental Health Survey (BW_EHS) from 1996 to 2003: toxic metals in blood and urine of children. Int J Hyg Environ Health 210:357–371
Mahaffey KR, Mergler D (1998) Blood levels of total and organic mercury in residents of the upper St. Lawrence River basin, Quebec: association with age, gender, and fish consumption. Envrion Res 77:104–114
Mahaffey KR, Clickner RP, Bodurow CC (2004) Blood organic mercury and dietary mercury intake: National Health and Nutrition Examination Survey, 1999 and 2000. Environ Health Perspect 112:562–570
Mahaffey KR, Clickner RP, Jeffries RA (2009) Adult women’s blood mercury concentrations vary regionally in the United States: association with patterns of fish consumption (NHANES 1999–2004). Environ Health Perspect 117:47–53
McKelvey W, Gwynn RC, Jeffery N, Kass D, Thorpe LE, Garg RK, Palmer CD, Parsons PJ (2007) A biomonitoring study of lead, cadmium, and mercury in the blood of New York City adults. Environ Health Perspect 115:1435–1441
Menke A, Muntner P, Batuman V, Silbergeld EK, Guallar E (2006) Blood lead below 0.48 μmol /L (10 μg/dL) and mortality among US adults. Circulation 114:1388–1394
Moon CS, Zhang ZW, Shimbo S, Watanabe T, Moon DH, Lee CU, Lee BK, Ahn KD, Lee SH, Ikeda M (1995) Dietary intake of cadmium and lead among the general population in Korea. Environ Res 71:46–54
Moon CS, Paik JM, Choi CS, Kim DH, Ikeda M (2003) Lead and cadmium levels in daily foods, blood and urine in children and their mothers in Korea. Int Arch Occup Environ Health 76:282–288
Mozaffarian D, Rimm EB (2006) Fish intake, contaminants, and human health: Evaluating the risks and the benefits. JAMA 296:1885–1899
Muntner P, Menke A, DeSalvo KB, Rabito FA, Batuman V (2005) Continued decline in blood lead levels among adults in the United States: the National Health and Nutrition Examination Surveys. Arch Intern Med 165(18):2155–2161
Navas-Acien A, Selvin E, Sharrett R, Calderon-Aranda E, Silbergeld E, Guallar E (2004) Lead, cadmium, smoking and increased risk of peripheral arterial disease. Circulation 109:3196–3201
Olsson IM, Bensryd I, Lundh T, Ottosson H, Skerfving S, Oskarsson A (2002) Cadmium in blood and urine-impact of sex, age, dietary intake, iron status, and former smoking- association of renal effects. Environ Health Perspect 110:1185–1190
Park SW, Kim KY, Kim DW, Choi SJ, Kim HS, Choi BS, Choi MK, Park JD (2006) The relation between blood lead concentration and epidemiologic factors and body iron status. J Environ Toxicol 21:153–162
Park JU, Oh SW, Kim SH, Kim YH, Park RJ, Moon JD (2008) A study on the association between blood lead levels and habitual tobacco and alcohol use in Koreans with no occupational lead exposure. Korean J Occup Environ Med 20:165–173
Park RJ, Kim SH, Park JU, Kim YH, Kim MB, Park WJ, Moon JD (2009) Blood lead levels as a predictor of coronary artery disease. Korean J Occup Environ Med 21:38–45
Pirkle JL, Brody DJ, Gunter EW, Kramer RA, Paschal DC, Flegal KM et al (1994) The decline in blood lead levels in the United States. The National Health and Nutrition Examination Surveys (NHANES). JAMA 272(4):284–291
Reeves PG, Chaney RL (2008) Bioavailability as an issue in risk assessment and management of food cadmium: A review. Sci Total Environ 393:13–19
Sakamoto M, Kaneoka T, Murata K, Nakai K, Satoh H, Akagi H (2007) Correlations between mercury concentrations in umbilical cord tissue and other biomarkers of fetal exposure to methylmercury in the Japanese population. Environ Res 103:106–111
Sanzo JM, Dorronsoro M, Amiano P, Amurrio A, Aguinagalde FX, Azpiri MA, The Epic Group of Spain (2001) Estimation and validation of mercury intake associated with fish consumption in an EPIC cohort of Spain. Public Health Nutr 4:981–988
Saraiva MCO, Taichman RS, Braun T, Nriagu J, Eklund SA, Burt BA (2007) Lead exposure and periodontitis in US adults. J Periodont Res 42:45–52
Schrober SE, Sinks TH, Jones RL, Bolger PM, McDowell M, Osterloh J, Garrett ES, Canady RA, Dillon CF, Sun Y, Joseph CB, Mahaffey KR (2003) Blood mercury levels in US children and women of childbearing age, 1999–2000. JAMA 289:1667–1674
Schulz C, Becker CK, Kolossa-Gehring M, Seiwert M, Seifert B (2007) Twenty years of the German Environmental Survey (GerES): Human biomonitoring: temporal and spatial (West Germany/East Germany) differences in population exposure. Int J Hyg Environ Health 210:271–297
Seifert B, Becker K, Helm D, Krause C, Schulz C, Seiwert M (2000) The German Environmental Survey 1990/1992 (GerES II): reference concentrations of selected environmental pollutants in blood, urine, hair, house dust, drinking water and indoor air. J Expo Anal Environ Epidemiol 10:552–565
Shimbo S, Zhang ZW, Watanabe T, Nakatsuka H, Matsuda-Inoguchi N, Higashikawa K, Ikeda M (2001) Cadmium and lead contents in rice and other cereal products in Japan in 1998–2000. Sci Total Environ 281:165–175
Soong YK, Tseng R, Liu C, Lin PW (1991) Lead, cadmium, arsenic, and mercury levels in maternal and fetal cord blood. J Formos Med Assoc 90:59–65
Tellez-Plaza M, Navas-Ancien A, Crainiceanu CM, Guallar E (2008) Cadmium exposure and hypertension in the 1999–2004 national health and nutrition examination survey (NHANES). Environ Health Perspect 116:51–56
Todd AC, Lee BK, Lee GS, Ahn KD, Moshier FL, Schwartz BS (2001) Predictors of DMSA chelatable lead, tibial lead, and blood lead in 802 Korean lead workers. Occup Environ Med 58:73–80
Tsukahara T, Ezaki T, Moriguchi J, Furuki K, Shimbo S, Matsuda-Inoguchi N, Ikeda M (2003a) Rice as the most influential source of cadmium intake among general Japanese population. Sci Total Environ 305:41–45
Tsukahara T, Ezaki T, Moriguchi J, Furuki K, Fukui Y, Ukai S, Okamoto S, Sakurai H, Ikeda M (2003b) No significant effect of iron deficiency on cadmium body burden or kidney dysfunction among women in the general population in Japan. Int Arch Occup Environ Health 76:275–281
Vahter M, Akesson A, Lind B, Bjors U, Schutz A, Berglund M (2000) Longitudinal study of methylmercury and inorganic mercury in blood and urine of pregnant and lactating women, as well as in umbilical cord blood. Environ Res 84(2):186–194
Vahter M, Berglund M, Akesson A, Liden C (2002) Metals and women’s health. Environ Res 88:145–155
Vahter M, Akesson A, Liden C, Ceccatelli S, Berglund M (2007) Gender differences in the disposition and toxicity of metals. Environ Res 104:85–95
Watanabe T, Zhang ZW, Moon CS, Shimbo S, Nakatsuka H, Matsuda-Inoguchi K, Higashikawa K, Ikeda M (2000) Cadmium exposure of women in general populations in Japan during 1991–1997 compared with 1977–1981. Int Arch Environ Health 73:26–34
World Health Organisation (1995) Inorganic lead: environmental health criteria, vol 118. International Programme on Chemical Safety, World Health Organization, Geneva
Yaginuma-Sakurai K, Shimada M, Ohba T, Nakai K, Suzuki K, Kurokawa N, Kameo S, Satoh H (2009) Assessment of exposure to methylmercury in pregnant Japanese women by FFQ. Public Health Nutrition 12:2352–2358
Yassin AS, Martonik JF, Davidson JL (2004) Blood lead levels in U.S. Workers, 1988–1994. J Occup Environ Med 46:720–728
Yeon YY, Ahn KD, Lee BK (1992) Blood and urine cadmium in non-exposed Korean to cadmium. Korean J Occup Environ Med 4(1):70–80
Zhang ZW, Moon CS, Watanabe T, Shimbo S, He FS, Wu YQ, Zhou SF, Su DM, Qu JB, Ikeda M (1997) Background exposure of urban populations to lead and cadmium: comparison between China and Japan. Int Arch Occup Environ Health 69:273–281
Zhang ZW, Shimbo S, Watanabe T, Srianujata S, Banjong O, Chitchumroonchokchai C, Nakatsuka H, Matsuda-Inoguchi N, Higashikawa K, Ikeda M (1999) Non-occupational lead and cadmium exposure of adult women in Bangkok, Thailand. Sci Total Environ 226(1):65–74
Zhang ZW, Moon CS, Shimbo S, Watanabe T, Nakatsuka H, Matsuda-Inoguchi N, Higashikawa K, Ikeda M (2000) Further reduction in lead exposure in women in general populations in Japan in the 1990s, and comparison with levels in east and Southeast Asia. Int Arch Occup Environ Health 73:91–97
Conflict of interest statement
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article can be found at http://dx.doi.org/10.1007/s00420-010-0572-9
Rights and permissions
About this article
Cite this article
Kim, NS., Lee, BK. National estimates of blood lead, cadmium, and mercury levels in the Korean general adult population. Int Arch Occup Environ Health 84, 53–63 (2011). https://doi.org/10.1007/s00420-010-0522-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-010-0522-6