
Abstract
Objective
To assess long-term variations in arsenic methylation and oxidative DNA lesions of chronic high arsenic-exposed populations.
Methods
A follow-up study was conducted in 64 chronic high arsenic-exposed subjects from 2004 to 2006. Urinary arsenic species and 8-hydroxydeoxyguanine were measured.
Results
Percentages of urinary inorganic arsenic, monomethylarsonate and urinary 8-hydroxydeoxyguanine (8-OHdG) level were significantly higher, but the percentage of dimethylarsinate, the primary methylation index (PMI) and secondary methylation index (SMI) was lower in the ninth year of arsenic exposure compared with the seventh year. Substantial differences in relative arsenic methylation capacity were observed between the seventh and ninth year. Percentages of arsenic species, PMI and SMI were significantly correlated between siblings, and between parents and children.
Conclusions
Arsenic methylation may decrease, but oxidative DNA lesions may increase with the increase of cumulative arsenic exposure level. Both genetic and environmental factors may contribute to variability in arsenic methylation.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Millions of people are exposed to excessive level of arsenic, a documented human carcinogen (IARC 2004), in drinking water all over the world. Long-term exposure to arsenic is associated with various adverse health effects including cancers of the bladder, skin, and lungs, and development of skin lesions, hypertension, and diabetes (Bates et al. 1992; Chen et al. 2005a; Tondel et al. 1999; Tseng et al. 2000; Yoshida et al. 2004). Moreover, the full human costs in terms of diminished quality of life, lost productivity, and other negative effects which result from consumption of arsenic-contaminated water are hardly estimated; however, the mechanism of arsenic poisoning is still not fully understood.
In many organisms, including humans, the biotransformation of arsenic occurs through the methylation process. Though the exact pathway of arsenic methylation is controversial (Aposhian et al. 2004; Hayakawa et al. 2005), inorganic arsenic (iAs) is well-recognized to be methylated in two steps, first to monomethylarsenate (MMA) and then to dimethylarsenate (DMA). The major site for arsenic methylation is the liver (Ford 2002). In humans, abnormal liver functions and transplantation of liver have been linked to the alteration of urinary arsenic metabolites. Thus, differences in the pattern of urinary arsenic metabolites could reflect the variation in the capacity of arsenic methylation in the liver (Hopenhayn-Rich et al. 1996; NRC (National Research Council) 2001).
The average distribution of urinary arsenic metabolites in arsenic-exposed people is generally 10–30% for iAs, 10–20% for MMA, and 60–70% for DMA (Hopenhayn-Rich et al. 1993; Vahter 1999a). However, differences in methylation capacity exist among individuals, even when exposed to the same level of arsenic (Hopenhayn-Rich et al. 1996; Loffredo et al. 2003; Vahter 2000). Low secondary arsenic methylation capacity has been shown to be associated with the incidence of peripheral vascular disease (Tseng et al. 2005), bladder carcinoma (Chen et al. 2003a; Chen et al. 2005b) and skin cancer (Chen et al. 2003b). An investigation carried out in Inner Mongolia found that subjects with arsenic dermatosis had significantly higher levels of urinary MMA than those without dermatosis (Fujino et al. 2005). These data suggest a link between differences in methylation capacity and individual variations in susceptibility to arsenic-induced diseases. Many studies have been conducted to assess these inter-individual differences (Drobna et al. 2004; Hopenhayn-Rich et al. 1996; Loffredo et al. 2003; Vahter 2000). Individual day-to-day fluctuations in arsenic metabolism, and even changes over a 24-h period, have been examined (Concha et al. 2002); however, little is known about long-term variation in arsenic metabolism. Our study was initiated to investigate this question in a population subject to long-term high arsenic exposure. We also report 2-year trends in the urinary levels of 8-OHdG, a potential biological indicator of oxidative DNA lesions in humans that is induced by arsenic exposure.
Materials and methods
Study population
The high arsenic-exposed subjects come from Koukenban, a Mongolia village in the northwest of China (Inner Mongolia) with elevated arsenic concentration in drinking water (Sun et al. 2007). All residents in the village drink water from the same well. Two investigations were conducted in this village over 2 years. A total number of 108 villagers exposed to high arsenic for 7 years consented to participate in the first investigation of our study from September to October 2004. Because some of the villagers went out for work or study, only 64 of the 108 villagers participated in the second investigation in September 2006. Samples of the public drinking water, collected each time of the two study periods, showed average arsenic concentrations of 162.4 and 166.7 μg/L, all of which were in inorganic form. The low arsenic-exposed subjects with 59 residents were selected from Tianjiaying village where the deep tube-well water is provided by centralized waterworks to community with iAs of 19.8 μg/L. The maximum allowable level for arsenic in drinking water is 50 μg/L in China. Demographics of the study subjects are listed in Table 1. Villagers in the two villages engage in subsistence agriculture, and earn some money by selling their farm products. There is no industry or mining around the villages. No seafood consumption was reported.
All participants gave informed consent. The study was conducted according to the Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects, and approved by the Ethics Committee of China Medical University.
Sample collection
First morning void urine samples (10 ml) were obtained in 15-ml polypropylene tubes (SARSTEDT, Japan) and kept in ice box. Exactly 1 ml of urine was kept separately for 8-OHdG determination. Urine samples collected in villagers’ houses were kept in ice until every night, when the samples were transported to the local center of endemic disease and then kept in −20°C. Then all samples were shipped with dry ice to the laboratory in China Medical University (Shenyang, China) by air to perform further determination.
Determination of urinary arsenic metabolites
Determination of arsenic species, iAs, MMA, DMA, and trimethylated arsenic (TMA) in urine was performed by atomic absorption spectrophotometer (AA-6800, Shimadzu Co. Kyoto, Japan) with an arsenic speciation pretreatment system (ASA-2sp, Shimadzu Co. Kyoto, Japan). The arsenic speciation was based on the well-established hydride generation of volatile arsines, followed by cryogenic separation in liquid nitrogen. The detection limits of the hydride generation and atomic absorption spectrometry (HG–AAS) method for four arsenic species were 1 ng, respectively. Briefly, 1 ml of urine thawed at room temperature from −80°C was digested with 2 N-NaOH solutions at 100°C for 3 h in a 15-ml polymethylpentene test tube followed by dilution with mili-Q water. The assay samples were stirred once every 60 min. This digestion procedure has been shown not to alter the distribution of iAs and methylated arsenicals (Yamauchi and Yamamura 1984). The absorbance of arsenic in the digested urine samples was determined at 193.7 nm. Quality control for arsenic determinations included the analysis of standard reference material of freeze-dried urine (SRM 2670). The certified concentration values for arsenic were 480 ± 100 μg/L. The values measured in present laboratory were 474 ± 20 μg/L. The reliability of arsenic species separation was evaluated by the analytical recoveries of added arsenic species. Spiking urine samples with 10 μg/L of iAs, MMA, DMA, and TMA resulted in recoveries of 81–92, 88–98, 89–103, and 80–95% for iAs, MMA, DMA and TMA, respectively. Because no TMA was detected in urine samples of any subject, we report the total arsenic (TAs) concentrations by summing up the concentrations of iAs, MMA, and DMA. Under our analytical conditions, differentiation of the trivalent forms from the pentavalent forms of arsenic cannot be performed.
Based on the determination of arsenic species in urine, percentages of urinary arsenic metabolites (iAs%, MMA% and DMA%) and two methylation indices, the primary methylation index (PMI) and the secondary methylation index (SMI), were calculated to assess the arsenic methylation capacity. In this study, PMI is defined as (MMA + DMA)/TAs and SMI is defined as DMA/(MMA + DMA).
Analysis of urinary 8-OHdG
To determine the concentrations of 8-OHdG, the urine specimens were centrifuged at 15,000 rpm for 10 min and the supernatants were used for the measurement with an ELISA Kit (Japan Institute for the Control of Aging, Fukuroi, Japan) according to the method of Saito et al. (2000). The determination range was 0.5–200 ng/ml. The levels of urinary 8-OHdG were corrected by the concentrations of urinary creatinine (Cr).
Data analysis
Data analysis was carried out with SPSS software (version 13.0, SPSS Inc., Chicago, IL, USA). Because of the positively skewed distribution of the variables, log-transformation was applied. After the transformation, independent-samples t test was used to test the differences between high and low arsenic-exposed subjects; Paired-samples t test was applied to test the 2-year differences of the high arsenic-exposed subjects, one-way ANOVA and Student–Newman–Keuls (SNK) of post hoc test were employed to test the differences in arsenic methylation capacity of the three high-exposed subgroups. For correlation analysis, Pearson correlation coefficient was reported. All P values were two tailed. Finally, values were transformed back to the arithmetic scale for reporting purposes.
Results
Children and adults exposed to high level of arsenic for 7 years had elevated concentrations of total urinary arsenic (average 529.81 and 579.64 μg/L, respectively), which confirms their high exposure to arsenic in drinking water (Table 2). iAs% and MMA% were significantly increased, but DMA%, PMI and SMI were significantly decreased, in children and adults compared with the low arsenic-exposed subjects (P < 0.01). The mean urinary 8-OHdG levels in high exposed children and adults were 17.77 and 23.67 μg/g Cr, respectively, which were significantly elevated compared with the low-exposed subjects. These results indicate the decreased arsenic methylation capacity and elevated oxidative DNA lesions in the high arsenic-exposed population.
Of 108 subjects exposed to high levels of arsenic in drinking water for 7 years, 64 continued to participate in our study in the ninth year of exposure. As shown in Table 3, for both children and adults, there was no significant variation over the 2 years in the average concentration of urinary TAs (P = 0.977 and P = 0.600), consistent with the stable daily ingestion of arsenic (Table 1); however, there was considerable variation in the relative distribution of urinary arsenic metabolites and the two urine-based arsenic methylation indices, PMI and SMI. On the whole, iAs% and MMA% were elevated, but DMA%, PMI and SMI were decreased in the ninth year of arsenic exposure, compared with the seventh year. In addition, both children and adults had significantly elevated levels of urinary 8-OHdG in the ninth year, compared with the seventh year. These results indicate that, in general, arsenic methylation capacity decreases but oxidative DNA lesions increase as the level of cumulative arsenic exposure increases. Both relative distribution of urinary arsenic species and 8-OHdG altered without change in arsenic exposure in our study subjects. So we investigated the possible relationship between them. It is interesting that all our study groups, including 108 subjects with 7-year-arsenic exposure and 64 subjects with 7- and 9-year exposure, showed most significant correlations of 8-OHdG with urinary MMA and MMA% (Table 4).
To assess the alteration of arsenic methylation capacity in individuals, relative to the whole population, the 64 subjects were divided into three subgroups according to the 30th and 70th percentile distribution of urinary iAs% after 7 years of arsenic exposure (Table 5). In the seventh year of exposure, the average iAs% for each subgroup were significantly different (P < 0.01), 9.50, 15.59 and 21.22, respectively, which reflects the variability in the amount of un-methylated arsenic metabolites. In the ninth year, however, the averages iAs% for the three subgroups were 20.10, 20.54, 19.17, and were not significantly different.
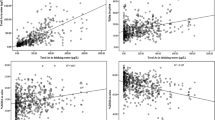
As shown in Fig. 1, the values of iAs%, MMA% and DMA% in urine were plotted for each individual exposed to high level of arsenic for 7 and 9 years. Individuals were listed in the order of urinary iAs% at the seventh year of exposure. On an individual level, the relative distribution of urinary arsenic metabolites (iAs%, MMA%, and DMA%) varied substantially over 2 years. Some subjects with high urinary iAs% in year 7 had relative low iAs% in year 9, and vice versa. The gradual rise in iAs% going from test subject 1 to test subject 64 in year 7 is completely lacking in year 9. These results suggest that an individual’s arsenic methylation capacity can be affected by multiple factors, of which genetic heritage is only one.

Urinary arsenic profile of 64 individuals in the seventh year (a) and ninth year (b) of arsenic exposure
Family correlations were conducted to determine whether genetic factors such as genetic polymorphisms may contribute to variations in arsenic methylation. Significant and high correlations were found between siblings for iAs% (r = 0.917, P = 0.010), DMA% (r = 0.825, P = 0.043), and PMI (r = 0.931, P = 0.007) (Table 6). The coefficients of correlation for sibling MMA% and SMI were also high, though not significant (P > 0.05). The parent–child correlations were relatively lower when compared to siblings but significant; the correlation coefficients were 0.530, 0.417, 0.635, 0.446, and 0.530 for iAs%, MMA%, DMA%, PMI, and SMI, respectively. No significant correlations were observed between husband and wife.
Discussion
To confirm the exposure to high level of arsenic, we compared the 108 high arsenic-exposed subjects with the low exposed individuals. Both children and adults had elevated urinary TAs concentrations. The high arsenic-exposed children and adults showed a decrease in arsenic methylation capacity but an increase in oxidative DNA lesions, which were consistent with previous studies. The 64 high arsenic-exposed subjects who participated in both the 2004 and 2006 investigations were not significantly different from the 108 subjects (participated in 2004 investigation) in urinary TAs concentration and arsenic methylation capacity (data not shown), but 8-OHdG levels were lower for the 64 subjects compared with the whole 108 subjects. Further analysis showed that the difference was resulted from 39 adults of the 64 subjects. The study population was required to be resident at the same address for a minimum of 7 years, and thus they were subjected to a stable exposure to arsenic in well water before recruitment. Urinary TAs concentration of the high exposed subjects was found to be consistent over 2 years, reflecting a constant arsenic exposure via drinking water.
It has been suggested that persons with more complete methylation, characterized as greater proportions of DMA and lesser proportions of MMA and iAs in urine, have a lower risk of adverse arsenic-related health problems. In animals, methyl-deficient diets have resulted in reduced arsenic methylation, higher arsenic tissue concentrations and elevated DNA damage (Tice et al. 1997). Although arsenic methylation has been shown to be remarkably stable over a short term (Concha et al. 2002), we found significant variation in arsenic methylation capacity over 2 years. The results indicate that over a certain period when arsenic exposure continues, the capacity of arsenic methylation, as reflected by the relative amounts of different urinary arsenic metabolites, decreases. The significant positive correlations of urinary 8-OHdG with MMA and MMA% found in our study (Table 4) also suggested the possible relationship between arsenic-induced health effects with the urinary arsenic profile and were consistent with previous studies. MMAIII has been found to be the most genotoxic and cytotoxic in vitro (Soto-Reyes et al. 2005; Styblo et al. 2000; Kligerman et al. 2003). Though differentiation of the trivalent from the pentavalent arsenicals cannot be performed under our analytical conditions, it is fairly possible that the content of MMA in urine reflects the level of MMAIII in blood or inside cells to some extent.
Our research also found that the arsenic methylation capacity of individuals within a certain population dramatically changed over 2 years. Some studies suggest that variations in methylation capacity may be caused by inherited genetic traits (Marcos et al. 2006; Schlawicke Engstrom et al. 2007; Vahter 1999b, 2000). The division of the 64 second-study subjects into three subgroups at 7 years of exposure was done according to the value of iAs%, which reflects un-methylated arsenic. The lower the iAs%, the higher the arsenic methylation capacity. If variations in methylation capacity are influenced primarily by inherited factors, subjects in the subgroup with the lowest iAs% may have genetic traits that translate to higher arsenic methylation capacity. If that is the case, then this subgroup should still have the highest methylation capacity of the three subgroups after an additional 2 years of arsenic exposure; however, significant differences in methylation capacity among the three subgroups were not present in the ninth year of arsenic exposure. In addition, the dramatic 2-year variations in arsenic methylation capacity of individuals were observed (Fig. 1). This temporal variation in relative methylation capacity could not be explained by polymorphisms of arsenic metabolism related genes, since an individual’s genetic traits are generally permanent. Other environmental factors such as diet and lifestyle, may be influencing methylation capacity. Nutrition is suggested as a major factor that might affect arsenic methylation (Gamble et al. 2006; Heck et al. 2007). Even minor dietary differences in some nutrients can contribute to variation in the concentration of blood S-adenosyl-methionine (SAM), the methyl donor for arsenic methylation (Poirier et al. 2001). Given the relatively recent evolution of economic systems in most settlements in China, some villagers have seized the opportunity to make substantial improvements in the quality of life. Not everyone, however, has experienced a positive change. People with few financial resources have been found to drink more arsenic-contaminated water because of a higher level of physical labor required on a day-to-day basis as well as lack of accessibility to water of higher quality. In addition, these individuals generally consume less nutritious food which contributes to poorer health. This possibility is supported by other research that has described a negative association between economic status and the prevalence of arsenicosis (Hadi and Parveen 2004).
Family correlation studies were used to determine whether there were genetic polymorphisms in some methylation systems (Weinshilboum 1988). In our family correlation analysis, we found high sibling–sibling and parent–child correlations but no couple correlation of arsenic methylation capacity reflected in the urinary arsenic profile, which suggests that the capacity to metabolize arsenic has a familial component. The results are consistent with a previous study, which reported that methylation patterns aggregate in families and are correlated in siblings (Chung et al. 2002). These data provide evidence of a genetic basis for the variation in arsenic methylation. The alteration of relative arsenic methylation capacity and the family correlation of arsenic methylation reported here provide evidence that variation in arsenic methylation is likely caused by both host factors and environmental effects.
It has been suggested that oxidative stress is involved in arsenic-induced cancer (Kitchin and Ahmad 2003). 8-OHdG in urine is a widely used biomarker of oxidative DNA lesions and indicates cancer risk due to oxidative stress (Kasai 1997). In this study, the assessment of 8-OHdG was completed in the seventh and ninth years of arsenic exposure. For the 64 subjects with two complete data sets (2004 and 2006), the level of urinary 8-OHdG was significantly increased over the 2-year period. Our results indicate that DNA lesions may occur from chronic exposure to inorganic arsenic, and that the lesions elevate as the level of cumulative arsenic exposure increases. Although no patient was diagnosed with cancer in the reported high arsenic-exposed population, the risk of latent adverse health effects, especially carcinogenesis, cannot be ignored.
References
Aposhian HV, Zakharyan RA, Avram MD, Sampayo-Reyes A, Wollenberg ML (2004) A review of the enzymology of arsenic metabolism and a new potential role of hydrogen peroxide in the detoxication of the trivalent arsenic species. Toxicol Appl Pharmacol 198:327–335
Bates MN, Smith AH, Hopenhayn-Rich C (1992) Arsenic ingestion and internal cancers: a review. Am J Epidemiol 135:462–476
Chen YC, Su HJ, Guo YL, Hsueh YM, Smith TJ, Ryan LM, Lee MS, Christiani DC (2003a) Arsenic methylation and bladder cancer risk in Taiwan. Cancer Causes Control 14:303–310
Chen YC, Guo YL, Su HJ, Hsueh YM, Smith TJ, Ryan LM, Lee MS, Chao SC, Lee JY, Christiani DC (2003b) Arsenic methylation and skin cancer risk in southwestern Taiwan. J Occup Environ Med 45:241–248
Chen CJ, Hsu LI, Wang CH, Shih WL, Hsu YH, Tseng MP, Lin YC, Chou WL, Chen CY, Lee CY, Wang LH, Cheng YC, Chen CL, Chen SY, Wang YH, Hsueh YM, Chiou HY, Wu MM (2005a) Biomarkers of exposure, effect, and susceptibility of arsenic-induced health hazards in Taiwan. Toxicol Appl Pharmacol 206:98–206
Chen YC, Su HJ, Guo YL, Houseman EA, Christiani DC (2005b) Interaction between environmental tobacco smoke and arsenic methylation ability on the risk of bladder cancer. Cancer Causes. Control 16:75–81
Chung JS, Kalman DA, Moore LE, Kosnett MJ, Arroyo AP, Beeris M, Mazumder DN, Hernandez AL, Smith AH (2002) Family correlations of arsenic methylation patterns in children and parents exposed to high concentrations of arsenic in drinking water. Environ Health Perspect 110:729–733
Concha G, Vogler G, Nermell B, Vahter M (2002) Intra-individual variation in the metabolism of inorganic arsenic. Int Arch Occup Environ Health 75:576–580
Drobna Z, Waters SB, Walton FS, LeCluyse EL, Thomas DJ, Styblo M (2004) Interindividual variation in the metabolism of arsenic in cultured primary human hepatocytes. Toxicol Appl Pharmacol 201:166–177
Ford M (2002) Arsenic. In: Goldfrank LR, Flomenbaum NE, Lewin NA, Howland MA, Hoffman RS, Nelson LS (eds) Goldfrank’s toxicologic emergencies, 7th edn. McGraw-Hill, New York
Fujino Y, Guo X, Liu J, Matthews IP, Shirane K, Wu K, Kasai H, Miyatake M, Tanabe K, Kusuda T, Yoshimura T (2005) Chronic arsenic exposure and urinary 8-hydroxy-2′-deoxyguanosine in an arsenic-affected area in Inner Mongolia, China. J Expo Anal Environ Epidemiol 15:147–152
Gamble MV, Liu X, Ahsan H, Pilsner JR, Ilievski V, Slavkovich V, Parvez F, Chen Y, Levy D, Factor-Litvak P, Graziano JH (2006) Folate and arsenic metabolism: a double-blind, placebo-controlled folic acid-supplementation trial in Bangladesh. Am J Clin Nutr 84:1093–1101
Hadi A, Parveen R (2004) Arsenicosis in Bangladesh: prevalence and socio-economic correlates. Public Health 118:559–564
Hayakawa T, Kobayashi Y, Cui X, Hirano S (2005) A new metabolic pathway of arsenite: arsenic-glutathione complexes are substrates for human arsenic methyltransferase Cyt19. Arch Toxicol 79:183–191
Heck JE, Gamble MV, Chen Y, Graziano JH, Slavkovich V, Parvez F, Baron JA, Howe GR, Ahsan H (2007) Consumption of folate-related nutrients and metabolism of arsenic in Bangladesh. Am J Clin Nutr 85:1367–1374
Hopenhayn-Rich C, Biggs ML, Smith AH, Kalman DA, Moore LE (1996) Methylation study of a population environmentally exposed to arsenic in drinking water. Environ Health Perspect 104:620–628
Hopenhayn-Rich C, Smith AH, Goeden HM (1993) Human studies do not support the methylation threshold hypothesis for the toxicity of inorganic arsenic. Environ Res 60:161–177
IARC (International Agency for Research on Cancer) (2004) Some drinking water disinfectants and contaminants, including arsenic. IARC Monogr Eval Carcinog Risk Hum 84:269–477
Kasai H (1997) Analysis of a form of oxidative DNA damage, 8-hydroxy-2′-deoxyguanosine, as a marker of cellular oxidative stress during carcinogenesis. Mutat Res 387:147–163
Kitchin KT, Ahmad S (2003) Oxidative stress as a possible mode of action for arsenic carcinogenesis. Toxicol Lett 137:3–13
Kligerman AD, Doerr CL, Tennant AH, Harrington-Brock K, Allen JW, Winkfield E, Poorman-Allen P, Kundu B, Funasaka K, Roop BC, Mass MJ, DeMarini DM (2003) Methylated trivalent arsenicals as candidate ultimate genotoxic forms of arsenic: induction of chromosomal mutations but not gene mutations. Environ Mol Mutagen 42:192–205
Loffredo CA, Aposhian HV, Cebrian ME, Yamauchi H, Silbergeld EK (2003) Variability in human metabolism of arsenic. Environ Res 92:85–91
Marcos R, Martinez V, Hernandez A, Creus A, Sekaran C, Tokunaga H, Quinteros D (2006) Metabolic profile in workers occupationally exposed to arsenic: role of GST polymorphisms. J Occup Environ Med 48:334–341
NRC (National Research Council) (2001) Arsenic in drinking water. Update National Academy Press, Washington DC
Poirier LA, Wise CK, Delongchamp RR, Sinha R (2001) Blood determinations of S-adenosylmethionine, S-adenosylhomocysteine, and homocysteine: correlations with diet. Cancer Epidemiol Biomarkers Prev 10:649–655
Saito S, Yamauchi H, Hasui Y, Kurashige J, Ochi H, Yoshida K (2000) Quantitative determination of urinary 8-hydroxydeoxyguanosine (8-OH-dg) by using ELISA. Res. Commun Mol Pathol Pharmacol 107:39–44
Schlawicke Engstrom K, Broberg K, Concha G, Nermell B, Warholm M, Vahter M (2007) Genetic polymorphisms influencing arsenic metabolism: evidence from Argentina. Environ Health Perspect 115:599–605
Soto-Reyes E, Del Razo LM, Valverde M, Rojas E (2005) Role of the alkali labile sites, reactive oxygen species and antioxidants in DNA damage induced by methylated trivalent metabolites of inorganic arsenic. Biometals 18:493–506
Styblo M, Del Razo LM, Vega L, Germolec DR, LeCluyse EL, Hamilton GA, Reed W, Wang C, Cullen WR, Thomas DJ (2000) Comparative toxicity of trivalent and pentavalent inorganic and methylated Asals in rat and human cells. Arch Toxicol 74:289–299
Sun G, Xu Y, Li X, Jin Y, Li B, Sun X (2007) Urinary arsenic metabolites in children and adults exposed to arsenic in drinking water in Inner Mongolia, China. Environ Health Perspect 115:647–652
Tice RR, Yager JW, Andrews P, Crecelius E (1997) Effect of hepatic methyl donor status on urinary excretion and DNA damage in B6C3F1 mice treated with sodium arsenite. Mutat Res 386:315–334
Tondel M, Rahman M, Magnuson A, Chowdhury IA, Faruquee MH, Ahmad SA (1999) The relationship of As levels in drinking water and the prevalence rate of skin lesions in Bangladesh. Environ Health Perspect 107:727–729
Tseng CH, Huang YK, Huang YL, Chung CJ, Yang MH, Chen CJ, Hsueh YM (2005) Arsenic exposure, urinary arsenic speciation, and peripheral vascular disease in blackfoot disease-hyperendemic villages in Taiwan. Toxicol Appl Pharmacol 206:299–308
Tseng CH, Tai TY, Chong CK, Tseng CP, Lai MS, Lin BJ, Chiou HY, Hsueh YM, Hsu KH, Chen CJ (2000) Long-term arsenic exposure and incidence of noninsulin-dependent diabetes mellitus: a cohort study inarseniasis-hyperendemic villages in Taiwan. Environ Health Perspect 108:847–851
Vahter M (1999a) Variation in human metabolism of arsenic. In: Abernathy CO, Calderon RL, Chappell WR (eds) Arsenic Exposure and Health Effects, 4th edn. Elsevier Science, New York
Vahter M (1999b) Methylation of inorganic arsenic in different mammalian species and population groups. Sci Prog 82:69–88
Vahter M (2000) Genetic polymorphism in the biotransformation of inorganic arsenic and its role in toxicity. Toxicol Lett 112–113:209–217
Weinshilboum R (1988) Pharmacogenetics of methylation: relationship to drug metabolism. Clin Biochem 21:201–210
Yamauchi H, Yamamura Y (1984) Metabolism and excretion of orally administered dimethylarsinic acid in the hamster. Toxicol Appl Pharmacol 74:134–140
Yoshida T, Yamauchi H, Sun GF (2004) Chronic health effects in people exposed to arsenic via the drinking water: dose-response relationships in review. Toxicol Appl Pharmacol 198:243–252
Acknowledgment
This work was supported by the grant (No. 30530640) from the National Natural Science Foundation of China (NSFC).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Xu, Yy., Wang, Y., Li, X. et al. Variations in arsenic methylation capacity and oxidative DNA lesions over a 2-year period in a high arsenic-exposed population. Int Arch Occup Environ Health 82, 251–258 (2009). https://doi.org/10.1007/s00420-008-0329-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-008-0329-x