
Abstract
Objective
The aim of this study was to test the hypothesis whether ageing workers have a higher need for recovery than younger workers.
Methods
1100 subjects (84.3% participation rate) employed in the public sector participated in a cross-sectional questionnaire study. The subjects were divided into two age groups: older workers (≥45 years) and younger workers (<45 years). The dependent outcome variable was assessed by “The Need for Recovery Scale” questionnaire. A need for recovery score higher than 45 was defined as a high need for recovery. A standardized questionnaire was used to assess psychosocial and physical work strain. Other occupational factors were included: part-time or full-time work, shift work and more than one employment. The following personal and social life and family related factors were also considered: gender, presence of chronic disease, degree of ability to cope with stress, number of children at home, taking care of disabled or elderly people, degree of satisfaction on family and social relationships. Stepwise multiple logistic regression analysis was used to examine the presence of a high need for recovery in older workers.
Results
The mean recovery score was significantly higher in the group of the older workers (40.9) as compared to the younger workers (33.6) (P < 0.005). In the final multivariate logistic regression model the older age group had a significantly higher risk for the presence of a high need for recovery versus the younger group (OR 1.56, 95%CI 1.15–2.11). Gender, presence of musculoskeletal disorder, work pressure, monotonous work, social support from superiors, full time work and unsatisfactory social contacts were also significantly associated with the need for recovery.
Conclusion
The hypothesis that ageing workers have a higher need for recovery than younger workers was confirmed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
There is an economical and political tendency to raise the retirement age. This means that workers will have to work at older age. As age increases changes in health (and its perception) occur (Seitsamo and Klockars 1997). It is also known that several aspects of work capacity change with increasing age (de Zwart et al. 1995; Broersen et al. 1996; Reilly et al. 1997; Ilmarinen 1999; Wegman 1999). An age-related imbalance between workload and work capacity was suggested to result in a chronic overload, increasing the risk of long-term health effects (de Zwart et al. 1995).
In recent research it has been demonstrated that long-term adverse health effects are preceded by short-term effects (Sluiter et al. 1999). These short-term effects are signs of fatigue, which are mostly experienced during or immediately after a day’s work. This is thought not to be a problem if enough recovery time is offered between two periods of work. If there is not enough time to recover from this fatigue in between two periods of work, the cumulated effects of this fatigue will lead to long-term adverse health effects (Sluiter et al. 1999). This is concordant with the cognitive activation theory of stress (CATS), where a sustained response may lead to illness and disease (Ursin and Eriksen 2004). In the CATS stress response is defined as an alarm in a homeostatic system, producing neurophysiological activation. The activation can be reduced by coping mechanisms, triggered by the same alarm. If the coping mechanisms are inadequate to reduce the activation level, a certain aroused activation level remains. If sustained this may lead to adverse health effects (Ursin and Eriksen 2004).
The short-term effects, manifested in feelings of temporary overload after work or subjective need for recovery, are recognizable in the immediate off-work situation and might be a useful indication of the personal psycho-physiological homeostatic balance at that moment (Sluiter et al. 2001). The subjective need for recovery can be measured by “The need for recovery scale”. This scale, used to measure early indications of fatigue at work, proved to be a powerful predictor of experienced health problems (Sluiter et al. 1999, 2003; van Veldhoven and Broersen 2003). This was also confirmed in a study performed in 541 employees working in the public sector where the relationship between work stress and need for recovery was explored. The results showed that the presence of psychosomatic health complaints was significantly associated with the need for recovery (De Meester and Kiss 2002).
In earlier research, also the relationship between short-term effects and high psychosocial work load was demonstrated (Sluiter et al. 1999). More recently, it was shown that subjects who reported more job demands also reported more need for recovery from work (Sluiter et al. 2001).
Studies on the need for recovery where age was included in the analysis showed non-consistent results on the relationship between need for recovery and age. Sluiter et al. (2001) found that age was not significant in the prediction of need for recovery. A more recent study showed a significant association in only two out of six separately considered job categories (Sluiter et al. 2003). However, these results do not answer the question if older workers have a higher need for recovery than younger ones. Therefore, the aim of this study was to test the hypothesis whether ageing workers have a higher need for recovery than younger workers.
To evaluate psychosocial work strain the different components based on the demands-control-support model (Karasek 1979) were included in the study: work pressure, job control, social support from superiors and from colleagues.
Associations between physical demands and need for recovery were found in some occupations (Sluiter et al. 2003). Therefore physical work strain was included in the study.
Since working hours and schedules were found to be associated with need for recovery from work (Jansen et al. 2003), more than one employment, part-time or full-time work and shift work were considered as well.
Besides occupational exposures also personal factors could have an influence on the need for recovery. Gender, degree of stress coping and presence of a chronic disease (musculoskeletal disorder, heart disease, chronic renal and surrenal disease) were included in the study. In a study evaluating the association between working hours and need for recovery gender differences were observed (Jansen et al. 2003). Furthermore, according to the CATS (Ursin and Eriksen 2004) coping mechanisms can reduce the activation level and hence influence the need for recovery. Finally, earlier research showed a substantial increase in prevalence rate of musculoskeletal and cardiovascular diseases with increasing age (Seitsamo and Klockars 1997).
Family and social life factors outside work were also included in the study, because it could be expected that these factors have an influence on the need for recovery, as it was shown that family and social life stressors could influence psychosocial health leading to fatigue (Moos et al. 2005; Bernert et al. 2007). Up to now these factors were not studied in relation to the need for recovery.
Methods
This study has been approved by the Ethics Committee Progecov (Commissie voor Medische Ethiek OG 211, Ghent, Belgium).
Subjects
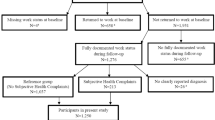
One thousand three hundred and five subjects employed in the public sector were asked to participate in a cross-sectional questionnaire study. All subjects received a standardized self-completed questionnaire at their home addresses by mail. One month later a second data collection was carried out amongst the non-responders. Eventually 1,108 subjects returned the questionnaire (84.9% response rate). Eight subjects with missing values on the outcome variable were excluded from the analyses. This reduced the number of participants to 1,100 subjects (84.3% participation rate). Mean age was 40.4 years (SD 9.8), ranging from 19 to 64 years. To describe the relation between need for recovery and age the subjects were divided into eight age categories (<25, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, ≥55 years). For comparison of older and younger workers the subjects were divided into two age groups: older workers (45 years or older) and younger workers (younger than 45 years), according to the WHO definition (WHO 1993).
Need for recovery
The dependent outcome variable was the experienced need for recovery, which was assessed by “The Need for Recovery Scale” questionnaire. The need for recovery scale was computed by summing up the scores of the 11 constituent dichotomous (yes/no) items, resulting in a score ranging from 0 to 11, which was transformed to a 0 to 100 scale. Reliability of the scale in this study reached 0.88 (Cronbach’s α), which was comparable to the reliability found in earlier studies (Sluiter et al. 1999; van Veldhoven and Broersen 2003; Jansen et al. 2003). A receiver operating characteristic (ROC) analysis in this study population showed that for long term health effects (psychosomatic complaints) a cut-off point for a high need for recovery could be determined at a score of 45 (De Meester and Kiss 2006, unpublished study). A need for recovery score higher than 45 was defined as a high need for recovery, while a score of 45 and lower was defined as a low need for recovery.
Psychosocial work strain
To assess the perception of psychosocial work strain a self-developed questionnaire was used based on the different components of the demands-control-support model (Karasek 1979): job demands were asked for in nine items, job control was asked for in five items and social support by colleagues and superiors was asked for in five items each. After factor analysis the job demand scale was divided into two factors: work pressure (eight items, Cronbach’s α 0.85) and monotonous work (single item). According to the Cronbach’s α the reliability of the job control scale was 0.81. Reliabilities of the scales for social support from superiors and from colleagues were 0.92 and 0.86, respectively. For each separate item a frequency based answer could be given (four possibilities: never, sometimes, often and always), resulting in a score from 0 to 3 for job demands and social support items, and from 1 to 4 in the job control items. All scales were computed by summing up the scores of the constituent items, resulting in a work pressure score ranging from 0 to 24 (highest score concordant with highest job demands), a job control score ranging from 5 to 20 (highest score concordant with highest contribution to a high job control) and scores for social support from superiors and colleagues, each ranging from 0 to 15 (highest score concordant with best social support).
Physical work strain and other occupational factors
Physical work strain was assessed using a three-item physical work load scale, comprising sustained physical efforts, lifting heavy weights and working in awkward positions (Cronbach’s α 0.85). Scoring for each separate item was analogous to scoring for the job demands items. The physical work load scale was computed by summing up the scores of the three constituent items, resulting in a score ranging from 0 to 9, where the highest score was concordant with the highest physical strain. Other relevant occupational factors that could be of influence on the need for recovery were included in the questionnaire: part-time (<38 h a week) or full-time work, shift work and more than one employment.
Personal factors
Apart from age, following personal factors were asked for in the questionnaire: gender, presence of chronic musculoskeletal disorder, presence of heart disease, presence of chronic renal and/or surrenal disease and degree of ability to cope with stress. The degree of ability to cope with stress was assessed by a six-item scale (Cronbach’s α 0.73) (Coetsier et al. 1996). Scoring for each separate item was analogous to scoring for the job demands items. The stress coping scale was computed by summing up the scores of the six constituent items, resulting in a score ranging from 0 to 18. A high score was concordant with a high degree of stress coping.
Family and social life factors
Social life and family related matters, which could be of influence on the need for recovery were considered as well. For this study questions were developed about: number of children at home, taking care of disabled or elderly people, degree of satisfaction (“very satisfied”, “fairly satisfied” and “not very satisfied”) on relationships with close relatives and friends and on social contacts (contacts with people in leisure activities, neighbours, hobby clubs, associations,...).
Statistical analyses
All data analyses were performed using SPSS, version 13.0 for Windows (SPSS 2004). The categorical variables (age groups, gender, presence of musculoskeletal disorder, full/part time work, shift work, more than one employment, number of children at home, taking care of ill or old people, contacts with close relatives and friends, social contacts) were described by number and percentage for the total study population and for the younger and older workers separately. The non-categorical variables or scores (stress coping, work pressure, monotonous work, job control, social support from superiors and colleagues, physical work strain) were described by mean and standard deviation for the total study population and for the younger and older workers separately. The mean need for recovery was calculated for each age category. For each category of the categorical variables the mean recovery score and the prevalence of high need for recovery were determined. Since exploring the relationship between age and the need for recovery was the objective of the study only the difference in need for recovery between age groups was tested for significance. Because the need for recovery score did not follow a normal distribution the Mann-Whitney U test and the Kruskal–Wallis test were used to test the difference in need for recovery score. The chi-square test was used to test the difference in the proportion of subjects with a high need for recovery. For testing the differences in other variables between older and younger workers the Mann–Whitney U test and the chi-square test were used appropriately.
Univariate logistic regression analysis was used to calculate the odds ratio and their 95% confidence intervals for the presence of a high need for recovery for each variable separately. To prevent occurrence of multicollinearity, correlations between all exposure variables were checked beforehand and no high collinearity was found (Checkoway et al. 2004). Stepwise forward conditional multiple logistic regression analysis was used to examine the presence of a high need for recovery (dependent variable) in older workers. Apart from age group, following independent variables were entered as well: work pressure, monotonous work, job control, social support from superiors and colleagues, physical work strain, full/part time work, shift work, more than one employment, gender, presence of musculoskeletal disorder, stress coping, number of children at home, taking care of ill or old people, contacts with close relatives and friends, social contacts. For the stepping method criteria, the P value for including a variable was set at 0.05 and the P value for excluding a variable at 0.10. The final multivariate model had the smallest value for −2 Log likelihood and the highest correctly predicted percentage.
Results
Table 1 summarizes the characteristics and the scores of the different personal, work related and family and social factors for the total study population.
The characteristics and the scores of the different personal work related and family and social factors for the younger and older workers separately are shown and compared in Table 2.
The overall mean need for recovery score was 36.1 (SD 29.4), with a proportion of 37.7% of subjects with a high need for recovery. The change in the need for recovery by age is presented in Table 3, which shows the mean need for recovery score for eight different age categories. There was a specific pattern in the mean need for recovery score by increasing age: starting relatively high in the youngest group, decreasing until the age of 34, increasing steadily until the age of 54 and decreasing from the age of 55.
The mean need for recovery score and the prevalence of high need for recovery for each categorical variable is described in Table 4. The mean need for recovery score was significantly higher in the group of the older workers as compared to the younger workers (P < 0.005). In the older age group there was a significantly higher proportion of subjects with a high need for recovery (P < 0.001).
This was confirmed in univariate logistic regression analysis, where the older age group had a significantly higher risk for the presence of a high need for recovery versus the younger group (OR 1.60, 95%CI 1.24–2.06), as shown in Table 5.
Table 5 also shows the results of the final multivariate logistic regression analysis. Age kept its significant association (OR 1.56, 95%CI 1.15–2.11). Of the personal factors gender and presence of a musculoskeletal disorder had a significant influence on the presence of a high need for recovery. Of the work strain factors work pressure and monotonous work increased the risk for the presence of a high need for recovery, while the social support from superiors decreased the risk. Full time work increased the risk for the presence of a high need for recovery. Striking was the very important influence of the degree of satisfaction on social contacts. Not very satisfactory social contacts increased considerably the risk for the presence of a high need for recovery with an OR of 4.12 (95%CI 2.12–7.99).
Discussion
The high participation rate of our study population (84.3%) is an indication of the good representativeness for our target population. Furthermore, the proportion of older workers in our study population (35.0%) is similar to the one in the general work force in Flanders (37.2%) (Baisier 2004). However, the proportion of women (61.7%) was higher than in the general work force in Flanders (49.4%) (Baisier 2004). This was due to the employment characteristics in the public sector, where our subjects were enrolled.
Apart from the fact that older workers experienced significantly lower support from their colleagues as compared to the younger workers, there were no significant differences between the two age groups for the other components of work strain. Although there was a smaller proportion of older workers who worked in shifts as compared to the younger workers and a larger proportion of older workers who worked part time, these differences turned out to be not significant. Considering these findings, we could conclude that the overall experienced work strain and other occupational factors were about similar in both age groups and certainly not higher in the older workers.
The overall mean need for recovery score of 36.1 found in our study was comparable to the need for recovery score in the 12,095 subjects of the Maastricht Cohort Study on Fatigue at Work (37.1) (Jansen et al. 2003) and markedly higher than the one found by van Veldhoven and Broersen (2003) in their study on 68,775 Dutch workers (27.3). This last difference could be explained by the higher proportion of female subjects in our study (61.7 vs. 41.0%), who had a significantly higher need for recovery score than men. Furthermore, there was a slightly higher proportion of workers of 45 years or older in our study (35.0 vs. 32.0%). The mean need for recovery score (34.9) for the 421 male subjects in our study population was comparable to the one found by Sluiter et al. (2001) in 60 Dutch male workers (33.6). Taking these considerations into account, our results for the need for recovery score were within expectations.
The high need for recovery in the youngest age category (Table 3) could be explained by a lower level of experience in these starting workers. The decrease after the age of 54 could be due to the healthy worker effect.
Although occupational exposures were about similar in both age groups, ageing workers had a significantly higher need for recovery than the younger workers and there were significantly more subjects with a high need for recovery in the group of ageing workers as compared to the group of younger workers. In the final multivariate regression model, taking into account other significant variables, the older workers still had a significantly higher need for recovery.
In this study other personal factors significant for the presence of a high need for recovery were gender (women had a higher need for recovery than men) and presence of musculoskeletal disorder.
Work demands (work pressure and monotonous work) were associated with a high need for recovery, which is in accordance to earlier findings that subjects who reported more job demands also reported a higher need for recovery from work (Sluiter et al. 2001). As could be expected social support from superiors had a positive influence on the need for recovery and full time work had a negative influence.
Striking is the strong association between the presence of a high need for recovery and unsatisfactory social contacts in leisure activities and not with unsatisfactory contacts with close relatives and friends. A possible explanation for this finding is that subjects with a high need for recovery are too exhausted to take part in social and leisure activities. In univariate analysis contacts with close relatives and friends were nevertheless significant factors for the need for recovery.
The cross-sectional design of this study could be subject to a healthy worker effect bias. However, the recruitment by mailing the questionnaire to the home addresses of the subjects, enabled to reach not only the ones at work, but also the subjects that were temporarily not working (for whatever reason). Workers who were forced to terminate employment prematurely because of poor health could not be included in the study. If the underlying reason for their poor health was due to a high need for recovery our results could possibly be underestimated.
Our study population consisted of workers employed in the public sector. The question is if the results can be extrapolated to other sectors. Further studies in other occupational sectors have to be carried out to confirm our results.
Physical work strain and work pressure in our population were rather low: respectively a mean score of 2.2 on a scale from 0 to 9 and a mean score of 9.4 on a scale from 0 to 24. It could be expected that some occupations in the private sector will have higher physical work strain, and due to a higher level of economical competition, also a higher work pressure. For these reasons those factors could be probably of more importance in other working populations.
For dichotomisation of the need for recovery scale we preferred to use the result of a ROC analysis instead of using an arbitrary cut-off point based on quartiles or tertiles of the study population. For this ROC analysis long-term health effects (psychosomatic complaints) were used as external criterion. The optimal cut-off point in our study population was 45 (De Meester and Kiss 2006, unpublished study). A ROC analysis in another study population with possibly other (combinations of) external criteria could eventually lead to a different cut-off point. More studies are needed to determine a general acceptable cut-off point for the need for recovery.
In conclusion, this study showed that, taking into account several occupational, personal and social factors, older workers had a higher need for recovery. A sustained high need for recovery will eventually lead to adverse health effects, compromising the good health of older workers. The inevitable policy of keeping workers longer at work can only be successful if the older workers remain in good health. This can be achieved when the employers take into account that older workers have a higher need for recovery. The high prevalence of musculoskeletal disorders in older workers and their major influence on the need for recovery justify more specific ergonomic measures. Measures to reduce work pressure and to facilitate part time work for older workers can also be recommended to employers.
References
Baisier L (2004) De tewerkstelling van de oudere werknemers in de industrie en profitdiensten in het Vlaams Gewest in 2000 [In Dutch: Employment of older workers in industry and profit sector in the Flemish Region in 2000]. SERV—STV—Innovatie & Arbeid, Brussel
Bernert RA, Merrill KA, Braithwaite SR, Van Orden KA, Joiner TE Jr (2007) Family life stress and insomnia symptoms in a prospective evaluation of young adults. J Fam Psychol 21:58–66
Broersen JP, de Zwart BC, van Dijk FJ, Meijman TF, van Veldhoven M (1996) Health complaints and working conditions experienced in relation to work and age. Occup Environ Med 53:51–57
Checkoway H, Pearce N, Kriebel D (2004) Research methods in occupational epidemiology, 2nd edn. Oxford University Press, New York
Coetsier P, De Backer G, De Corte W, Karnas G, Kornitzer M (1996) Onderzoeksdesign en instrumentarium van het Belgisch Jobstress onderzoek [In Dutch: study design and instruments of the Belgian Job stress Study]. Reeks Theoretische en Toegepaste Psychologie no. 6, Infoservice, Deinze
De Meester M, Kiss P (2002) Relationship between work stress and need for recovery. Preliminary results (abstract). Med Lav 93:460
de Zwart BCH, Frings-Dresen MHW, van Dijk FJH (1995) Physical workload and the ageing worker: a review of the literature. Int Arch Occup Environ Health 68:1–12
Ilmarinen J (1999) Ageing workers in the European Union—status and promotion of work ability, employability and employment. Finnish Institute of Occupational Health, Helsinki
Jansen NWH, Kant IJ, van Amelsvoort LGPM, Nijhuis FJN, van den Brandt PA (2003) Need for recovery from work: evaluating short-term effects of working hours, patterns and schedules. Ergonomics 46:664–680
Karasek RA (1979) Job demands, job decision latitude and mental strain: implications for job design. Adm Sci Q 24:285–308
Moos RH, Schutte KK, Brennan PL, Moos BS (2005) The interplay between life stressors and depressive symptoms among older adults. J Gerontol B Psychol Sci Soc Sci 60:199–206
Reilly T, Waterhouse J, Atkinson G (1997) Aging, rhythms of physical performance, and adjustment to changes in the sleep-activity cycle. Occup Environ Med 54:812–816
Seitsamo J, Klockars M (1997) Aging and changes in health. Scand J Work Environ Health 23(Suppl 1):27–35
Sluiter JK, Van der Beek AJ, Frings-Dresen MHW (1999) The influence of work characteristics on the need for recovery and experienced health: a study on coach drivers. Ergonomics 42:573–583
Sluiter JK, Frings-Dresen MH, van der Beek AJ, Meijman TF (2001) The relation between work-induced neuroendocrine reactivity and recovery, subjective need for recovery, and health status. J Psychosom Res 50:29–37
Sluiter JK, de Croon EM, Meijman TF, Frings-Dresen MHW (2003) Need for recovery from work related fatigue and its role in the development and prediction of subjective health complaints. Occup Environ Med 60(Suppl 1):i62–i70
SPSS (2004) SPSS for Windows, version 13.0.1. SPSS, Chicago
Ursin H, Eriksen HR (2004) The cognitive activation theory of stress. Psychoneuroendocrinology 29:567–592
van Veldhoven M, Broersen S (2003) Measurement quality and validity of the “need for recovery scale”. Occup Environ Med 60(Suppl 1):i3–i9
Wegman D (1999) Older Workers. Occup Med 14:537–557
World Health Organization (WHO) (1993) Aging and working capacity: report of a WHO study group WHO technical report series 835. World Health Organization, Geneva
Acknowledgments
The authors wish to acknowledge Mrs. Veerle Veldeman for her meticulous data input and Mr. Patrick De Loof for his useful linguistic advice. They extend special thanks to Lydia Decrans, MD, Director of Progecov, for the support that made it possible to realize this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kiss, P., De Meester, M. & Braeckman, L. Differences between younger and older workers in the need for recovery after work. Int Arch Occup Environ Health 81, 311–320 (2008). https://doi.org/10.1007/s00420-007-0215-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-007-0215-y