
Abstract
Objective
The role of silica in the causation of lung cancer is an ongoing debate. In order to explore whether observed association between silica exposure and lung cancer is confounded by exposure to other occupational carcinogens, we updated a previously nested case-control study among a cohort of male workers in 29 Chinese mines and factories on the basis of an extended follow-up.
Methods
Five hundred and eleven lung cancer cases and 1,879 matched controls were selected. Exposure to respirable silica as well as relevant occupational confounders were quantitatively assessed based on historical industrial hygiene data. The relationship between exposure to silica and lung cancer was analyzed by conditional logistic regression analysis adjusted for exposure to arsenic, polycyclic aromatic hydrocarbons (PAHs), radon, and smoking.
Results
In a crude analysis adjusted for smoking only, a significant trend of increasing risk of lung cancer with exposure to silica was found for tin, iron/copper miners, and pottery workers. But after adjustment for relevant occupational confounders, no relationship between silica and lung cancer can be observed. Instead, there is a significant association between lung cancer mortality and cumulative exposure to inorganic arsenic (OR = 1.86, 95% CI: 1.14, 3.04 for each mg/m3-year increase) and carcinogenic PAHs (OR = 1.35, 95% CI: 1.08, 1.69 for each 100 μg/m3-year increase).
Conclusion
This analysis does not provide any evidence to show that exposure to silica causes lung cancer in the absence of confounding factors.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
The role of silica in the causation of lung cancer is still an ongoing debate. In 1997, a working group of the International Agency for Research on Cancer (IARC) classified respirable silica as a human carcinogen (IARC 1997). However, the working group stated also, that carcinogenicity in humans was not detected in all industrial circumstances. The epidemiological studies reviewed by this working group pointed out important variations in silica associated lung cancer risk by geographic area, type of studies, type of industry, and levels of exposure, with inconsistent dose–response trends. In fact, increased risk of lung cancer was consistently observed among workers reported to have silicosis only (Checkoway and Franzblau 2000; Kurihara and Wada 2004). No increased risk of lung cancer can be observed among workers without silicosis (Checkoway and Franzblau 2000; Kurihara and Wada 2004). The evidence of a direct association between silica exposure and lung cancer is virtually inconsistent (IARC 1997).
In the late 1980s, a mortality follow-up of silica exposed workers in 29 Chinese mines and factories was conducted (Chen et al. 1992). The results of this follow-up did not show an increased risk (standardized mortality ratios) of lung cancer overall, but a significant twofold excess among tin miners. A nested case-control analysis of this cohort found that lung cancer risk increased by cumulative exposure to silica among tin miners and pottery workers, but not among workers in tungsten mines and iron/copper mines (McLaughlin et al. 1992). Relevant occupational confounders [inorganic arsenic in tin mines, polycyclic aromatic hydrocarbons (PAH) in iron/copper mines and potteries] were also noticed, but strong correlations between the various occupational risk factors (silica, arsenic, PAH, and radon) do not allow a separation of these effects in the previous analysis (McLaughlin et al. 1992).
In this present update of the previous case-control analysis, we try to separate the effect of silica from other occupational risk factors on the basis of an extended follow-up of the study cohort (from 1989 until 1994) and with improved individual exposure information.
Methods
Design and study population
Details of the study design and methods, including tracing vital status and cause of death, diagnostic procedures, exposure monitoring data, and follow-up information have been described previously (Chen et al. 1992; McLaughlin et al. 1992; Dosemeci et al. 1993). Briefly, the study design is a retrospective cohort study among workers employed in 29 Chinese mines and factories (ten tungsten mines, six iron/copper mines, four tin mines, eight pottery factories, and one clay mine). All workers who have been employed for at least 1-year and actively employed during the period of January 1, 1972–December 31, 1974 in above mines and factories, were followed for mortality from the data of entry (January 1972–December 1974) until December 31, 1989. The size of the original cohort was 65,285 workers. With the exception of all six iron/copper mines, two tungsten mines, and one pottery factory, follow-up was extended for 20 mines and factories until 1994 for 47,108 workers (the drop of nine mines and factories in the extended follow-up is mainly due to the limited research funding). Information on vital status and cause of death was sought from employment records and from medical and death records at local hospital. In total, vital status and cause of death were assessed for above 95 and 98% of the study cohort, respectively.
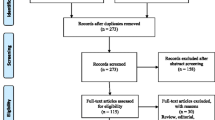
For the nested case-control analysis, 518 male lung cancer cases were identified. Identification of lung cancer cases based primarily on the underlying cause of death noted in the death certificates, their diagnostic information were reconfirmed by medical records in local or regional hospital. Controls were selected randomly among male cohort members by “density sampling,” about 4:1 matched to case (4:1 matched to cases followed until 1989, and 3:1 matched to cases collected during the extended follow-up) by decade of birth and mine or factory. Overall, 1884 male cohort members were selected as controls. The nested case-control analysis was restricted only to men, since the majority of cohort members (85%) were men.
Information on smoking (ever/never smoker, duration of smoking, and average number of cigarettes smoked per day) was acquired by questionnaire from the study subject or his next of kin (for all cases and 30% controls).
Occupational exposure assessment
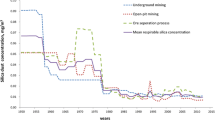
Historical industrial hygiene data were available since the 1950s for total dust, particle size, and percent of free silica. A special monitoring program was designed for this investigation to compare total dust with respirable silica concentrations in work places from 1987. All available monitoring data were used to create a job title/calendar year exposure matrix (JEM) for average total dust. There is a total of 1,090 facility/job tile combinations over 21 calendar periods starting from 1950. More than 60% of facility, job title, and calendar year were estimated based on direct monitoring data (about 2 million measurements since the 1950s). The others were estimated with monitoring data for similar jobs or data for the same job at different time, with adjustment for other historical exposure information and task description for the job title. A detailed description of JEM has been published elsewhere (Dosemeci et al. 1993). For this research, complete individual work histories for each study subject were reconstructed using employment records in personal files of the involved mining companies and factories.
Cumulative exposure to total dust was calculated for each subject by combining the JEM and individual work history (Chen and Chen 2002). The JEM used in previous publication, were updated in this analysis by using exact average values of exposure for each facility, job title, and calendar year combination instead of seven crude exposure categories (<1, 1–1.99, 2–5.99, 6–9.99, 10–14.99, 15–24.99, and ≥25 mg/m3). The individual work history was also improved during the extended follow-up. Exposure information for cohorts from iron/copper mines was not updated in this analysis (75 cases and 277 controls).
Different from previous published case-control analysis (McLaughlin et al. 1992), cumulative exposure to respirable silica was calculated in this analysis by using a conversion factor between total dust and respirable silica, which was developed for various mines and factories (Zhuang et al. 2001).
Exposure to radon-daughters, arsenic, and carcinogenic PAH [including benzo(a)pyrene, benz(a)anthracene, benzo(b)fluoranthene, dibenz(a,h)anthracene chrysene, and indeno(1,2,3-cd)pyrene) was also determined in each of the 29 mines and factories in a special monitoring program during the time between 1987 and 1988 (Wu et al. 1992). Depending on various working conditions, tasks of jobs, and the levels of total dust exposure, relevant sampling points were selected by the USA and Chinese industrial hygienists. In each of the sampling points, 2–6 samples were collected for the assessment of exposure to radon-daughters, arsenic, and carcinogenic PAH, respectively. Based on the monitoring data and expert judgments, a job-exposure matrix was developed independently from the exposure to respirable silica. The cumulative exposure to occupational confounders was calculated by combining the exposure duration and exposure level in various jobs.
Statistical analysis
The association between silica exposure and lung cancer mortality was estimated by conditional logistic regression analysis, a matched-regression method which allows control of residual confounding via regression terms, adjusted for smoking and relevant occupational confounders such as arsenic, PAH, and radon. Cumulative exposure to occupational risk factors among matched controls was truncated at the date of death of the index cases. All analysis was lagged for 15 years. Odds ratios (OR) and their 95% confidence intervals (95% CI) were calculated using PROC PHREG with the statistical software package SAS 8.02.
For the present analysis, only subjects with all information were included, which lead to exclusion of seven cases and five controls, leaving for the analysis 511 cases and 1,879 controls.
Results
Exposure to relevant occupational and non-occupational risk factors among the 511 lung cancer cases and 1,879 matched controls is given in Table 1. In total, 83% of the study populations are current or former smokers. As reported previously, cumulative exposure to respirable silica varies significantly among the different facilities with the highest exposure in tungsten mines and lowest exposure in iron/copper mines. Except respirable silica, exposure to other occupational risk factors in tungsten miners is negligible. However, pottery workers and tin miners exposed to a relatively high level of carcinogenic PAHs (up to 608.4 μg/m3-year) and inorganic arsenic (up to 3,542.4 μg/m3-year), respectively. Although the average cumulative exposure to occupational confounders (arsenic, PAH, and radon) among iron/copper miners is negligible, some of the iron/copper miners exposed to a relatively high level of carcinogenic PAHs (up to 2,000 μg/m3-year) and radon daughter (up to 311 WLM). There is a strong correlation between respirable silica and other occupational risk factors among the Chinese miners and pottery workers (Pearson’s correlation coefficient = 0.57–0.80, 0.83, and 0.55 for PAHs, arsenic, and radon, respectively).
The estimated association between respirable silica exposure and lung cancer mortality is given in Tables 2, 3, and 4. If only smoking is adjusted without consideration of occupational confounders, a clear dose–response relationship between respirable silica exposure and lung cancer mortality is observed among tin miners, iron/copper miners, and pottery workers, but not among tungsten miners (Table 2). However, the observed dose–response relationship disappeared after the relevant occupational confounders were adjusted (Table 3, except tin miners). Among tin miners, adjustment of relevant occupational confounder cannot produce reliable results in the analysis due to the strong correlation (co-linearity) between the cumulative exposure to respirable silica and arsenic (Table 3).
In a pooled analysis of all facilities (Table 4), no effect of silica on the mortality of lung cancer can be observed. Instead, there is a statistical significant association between lung cancer mortality and cumulative exposure to inorganic arsenic (OR = 1.86, 95% CI: 1.14, 3.04 for each mg/m3-year increase) and carcinogenic PAHs (OR = 1.35, 95% CI: 1.08, 1.69 for each 100 μg/m3-year increase).
Discussion
The purpose of the present case-control analysis is to update previous knowledge on dose–response relationship between silica exposure and lung cancer among a cohort of dust exposed Chinese workers on the basis of extended follow-up and improved exposure information. If relevant occupational cofounders were not considered in this analysis, similar dose–response trend between silica exposure and lung cancer can be observed as those published previously for tungsten miners, tin miners, and pottery workers (McLaughlin et al. 1992). However, some minor changes were found for iron–copper miners (no dose–response relationship was reported previously), although the data for iron–copper miners was not updated in this analysis at all. These changes are likely due to the use of different exposure categories and the 15 years lag in the analysis. After adjustment of relevant occupational confounders, the observed dose–response relationship disappeared in both unpooled (Table 3) and pooled analyses (Table 4, for all data and updated data). The results of the present analysis confirm a previous suspicion (Cocco et al. 2001) that the observed excess risk of lung cancer among silica exposed Chinese miners and pottery workers is more likely due to exposure to other well established occupational lung carcinogens, such as arsenic and PAHs, rather than due to exposure to respirable silica.
The relationship between crystalline silica and lung cancer has been the subject of many recent publications, conferences, and regulatory considerations. Experimental evidences demonstrated that silica is not directly genotoxic and has been shown to be a pulmonary carcinogen in only one animal species: the rat (Hessel et al. 2000). The failure of demonstrating pulmonary carcinogenic effect of crystalline silica in mice, hamsters, or guinea pigs (Hessel et al. 2000) indicate that animal model in rat may not be an appropriate model for assessing carcinogenesis in humans, or for demonstrating biological plausibility for observed associations in selected epidemiological studies.
In human, carcinogenic effect of crystalline silica was only consistently observed among persons with (radiographic) silicosis (Checkoway and Franzblau 2000; Kurihara and Wada 2004). Silicosis was often considered as a marker of high silica exposure. Association between silicosis and lung cancer was, therefore, in general considered as an evidence of an association between silica exposure and lung cancer. Epidemiological evidence based on silicosis studies has often-specific methodological limitations. One important limitation is the great potential for misdiagnosis of radiographic assessment of silicosis, which may be due to X-ray film quality and reader variability (Hessel et al. 2000). Population studies on subjects unexposed to dust show that, 0.2–11.7% of subjects without dust expose have small lung opacities, which are likely diagnosed as pneumoconiosis (Meyer et al. 1997). Smoking induced lung appearances, infectious and non-infections granulomas, hamartomas, and lung cancer are often considered to be possible reasons for misdiagnosis of radiographic silicosis (Fletcher 2002). A recent review study shows that radiographic silicosis is generally positively associated with cigarette smoking (Hessel et al. 2003). Although it is unclear whether smoking predisposes to silicosis (due to decreased lung clearance) or that radiographic appearances from smoking were interpreted as silicosis, a positive association between radiographic silicosis and smoking would bias studies of silicosis and lung cancer, and lead to an overestimation of the effect of silicosis (Hessel et al. 2003).
The direct association between crystalline silica exposure and lung cancer is, as noted in the IARC monograph (IARC 1997), not detected in human in all industrial circumstances. Heterogeneity in results across studies or industries may reflect chance occurrences or a true biological phenomenon related to different carcinogenic potential of inhaled dust. However, methodological limitations in the study design such as biases, confounding, or possible effect modification may also lead to inconsistent findings of silica-associated lung cancer risks. Although important occupational and non-occupational confounding factors such as radon-daughters, arsenic, PAH, asbestos, diesel exhaust, and smoking have been reported or suspected in many studies or industrial circumstances (McLaughlin et al. 1992; Checkoway et al. 1996; Steenland et al. 2001), these factors have rarely been considered in the analysis of the association between silica exposure and lung cancer. Their possible effect on the association between silica exposure and lung cancer can, therefore, not be ruled out.
In the present case-control analysis of the largest industrial silica cohort world-wide, relevant occupational and non-occupational confounders are for the first time systematically assessed and quantitatively considered. The results of our analysis indicate the importance of adequate adjustment of relevant occupational confounders on the evaluation of the possible association between silica exposure and lung cancer. Although the relatively lower effect of smoking demonstrated in this study indicates some exposure misclassification due to the lack of the information about ex-smoker, this limitation may unlikely have any influence on the demonstrated confounding effect of the relevant occupational factors (Arsenic, PAH). Overall, the results of our analysis do not support the hypothesis that crystalline silica exposure is causally associated with increased risk of lung cancer.
References
Checkoway H, Franzblau A (2000) Is silicosis required for silica-associated lung cancer? Am J Ind Med 37:252–259
Checkoway H, Heyer NJ, Demers PA, et al (1996) Reanalysis of mortality from lung cancer among diatomaceous earth industry workers, with consideration of potential confounding by asbestos exposure. Occup Environ Med 53(9):645–647
Chen J, McLaughlin JK, Zhang JY, et al (1992) Mortality among dust-exposed Chinese mine and pottery workers. J Occup Med 34:311–316
Chen W, Chen J (2002) Nested case-control study of lung cancer in four Chinese tin mines. Occup Environ Med 59:113–118
Cocco P, Rice CH, Chen JQ, et al (2001) Lung cancer risk, silica exposure, and silicosis in Chinese mines and pottery factories: the modifying role of other workplace lung carcinogens. Am J Ind Med 40:674–682
Dosemeci M, Chen JQ, Hearl F, et al (1993) Estimating historical exposure to silica among mine and pottery workers in the People’s Republic of China. Am J Ind Med 24:55–66
Fletcher JW (2002) PET scanning and the solitary pulmonary nodule. Semin Thorac Cardiovasc Surg 14:268–274
Hessel PA, Gamble JF, Gee JB, et al (2000) Silica, silicosis, and lung cancer: a response to a recent working group report. J Occup Environ Med 42:704–720
Hessel PA, Gamble JF, Nicolich M (2003) Relationship between silicosis and smoking. Scand J Work Environ Health 29:329–336
IARC (1997) Monographs on the evaluation of carcinogenic risks to humans, vol 68. Silica, some silicates, coal dust, and para-aramid fibrils. WHO, Lyon
Kurihara N, Wada O (2004) Silicosis and smoking strongly increase lung cancer risk in silica-exposed workers. Ind Health 42:303–314
McLaughlin JK, Chen JQ, Dosemeci M, et al (1992) A nested case-control study of lung cancer among silica exposed workers in China. Br J Ind Med 49(3):167–171
Meyer JD, Islam SS, Ducatman AM, et al (1997) Prevalence of small lung opacities in populations unexposed to dusts. A literature analysis. Chest 111:404–410
Steenland K, Mannetje A, Boffetta P, et al (2001) International agency for research on cancer. pooled exposure-response analyses and risk assessment for lung cancer in 10 cohorts of silica-exposed workers: an IARC multicentre study. Cancer Causes Control 12:773–784
Wu Z, Hearl F, Peng K, et al (1992) Current occupational exposure in Chinese iron and copper mines. Appl Occup Environ Hyg 7:735–743
Zhuang Z, Hearl FJ, Odencrantz J, et al (2001) Estimating historical respirable crystalline silica exposures for Chinese pottery workers and iron/copper, tin, and tungsten miners. Ann Occup Hyg 45:631–642
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chen, W., Bochmann, F. & Sun, Y. Effects of work related confounders on the association between silica exposure and lung cancer: a nested case-control study among Chinese miners and pottery workers. Int Arch Occup Environ Health 80, 320–326 (2007). https://doi.org/10.1007/s00420-006-0137-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-006-0137-0