
Abstract
Objectives: To investigate the short-term and long-term effectiveness of two, brief, preventive, work stress management programmes. One programme was a cognition-focused programme, the other was a newly developed intervention in which physical exercise and relaxation were combined. It was hypothesised that the newly developed intervention would be more effective in reducing psychological complaints than the cognitive intervention. Both programmes consisted of four sessions in a period of 10 weeks. Methods: From a working population engaged in a periodic health check-up, employees above a minimum stress level (n=396) were invited to participate in a randomised comparative outcome study with pre-trial, post-trial and 6-month follow-up measures. After giving informed consent 130 participants entered the study (response rate 33%). Outcome measures consisted of three self-reported questionnaires on psychological complaints. Results: It was found that both interventions revealed a positive impact on psychological complaints, burnout and fatigue, both at short-term and at 6-month follow-up. No statistical interaction effects between the two interventions were found. Calculation of the clinical significance of the effects indicated that 50% of the employees with psychological complaints who participated in the physical intervention and 60% of the employees who participated in the cognitive intervention improved and returned to functioning within normal range both in the short term and in the long term at 6 months. Conclusion: The data indicate that interventions were equally effective on psychological complaints, burnout and fatigue.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
This paper reports a long-term follow-up assessment of two strategies in relation to their effectiveness in stress management. The specific aim of both interventions, a cognitive intervention versus a combined intervention of physical exercise and relaxation, is to reduce health complaints that result from job stress.
In Western countries job stress is considered a major concern, especially during the past decades. As in other countries (Paoli and Merllie 2000), in the Netherlands, disablement for work as a result of health complaints due to job stress is one of the main political and economical concerns. It is estimated that two-thirds of sick leave may be attributed to job stress (Houtman et al. 1994; Stichting van de Arbeid 2002).
As a result of prolonged job stress, employees may suffer from various health complaints, such as depression symptoms, anxiety, physical symptoms and distress, malaise or burnout (Cooper et al. 2001). Several stress-reducing interventions have been developed over the years to counter these problems. The focus of these job stress interventions can be an individual, an organisational or a combined approach (van der Klink et al. 2001). In this study we consider, especially, the effectiveness of an individual approach.
There is a great diversity concerning the content and duration of individual-focused interventions. Interventions based on a physical approach, such as relaxation and physical exercise, aim at improving mental health by reducing physiological arousal (Salmon 2001). According to Murphy (1996) relaxation is involved in approximately 75% of stress-management programmes. There is good evidence from randomised controlled trials that relaxation techniques can reduce psychological complaints, especially anxiety related symptoms related to stressful situations (Vickers and Zollman 1999).
Another physical approach, physical exercise, may also have a positive effect on psychological complaints, especially for depressive symptoms and the ability to cope with (job) stress (Salmon 2001; Gauvin and Spence 1995; Byrne and Byrne 1993) Recently several studies have consistently associated physical exercise with better mental health (Steptoe and Butler 1996). In a review Salmon (2001) stated that the clearest evidence of improvement of these psychological complaints by exercise training has been found with relatively mildly, non-clinically impaired subjects.
As noted above, employees with job stress report various psychological complaints, including depression and anxiety. Therefore, a combined intervention of relaxation and physical exercise is of special interest. We hypothesise that a combined intervention might have a synergistic effect. To our knowledge outcome studies with a combined intervention of relaxation and physical exercise have not been conducted thus far and are, therefore, one of the aims of the present study.
Individual-focused interventions based on cognitive techniques aim at reducing complaints through changing appraisal processes (cognition) and/or enhancing coping skills (behaviour) (Lazarus and Folkman 1984; Meichenbaum and Deffenbacher 1988). This type of intervention can be described as a time-limited, present-orientated approach that teaches employees cognitive and behavioural coping skills (Heimberg 2002). The positive effects of cognitive interventions have been extensively reported with regard to patients with depressive (Scott 2001) and/or anxiety disorders (Heimberg 2002; Fedoroff and Taylor 2001). Guidelines (Agency for Health Care Policy and Research 1993; American Psychiatric Association 1993) suggest that the best candidates for these interventions are individuals with mild-to-moderate depression as observed in highly distressed employees (Scott 2001).
Recently, a meta-analysis that assessed the effect sizes of job stress management was conducted (van der Klink et al. 2001). Moderate effect sizes were found for individual-focused programmes (Cohen’s d=0.44). A small but significant effect size was reported for programmes with relaxation techniques across different outcome measures (d=0.35). However, as expected, relaxation was shown to have a large effect size on psychophysiological complaints. For programmes with a cognitive–behavioural approach the effectiveness (d=0.68) across all outcome measures was significantly larger than that of relaxation techniques. This supports the interpretation that cognitive intervention is superior to a physical intervention.
In the meta-analysis a number of gaps in our knowledge is considered with regard to stress-reduction intervention programmes (van der Klink et al. 2001; Murphy 1996; van der Hek and Plomp 1997). Comparative outcome studies on the effectiveness of various interventions are rare. For example, comprehensive programmes that include physical exercise and relaxation techniques have not been compared with a cognitive programme. The aim of this study was to test the hypothesis that the newly developed, combined physical intervention is more effective in reducing psychological complaints than a cognitive intervention. Another issue was the lack of a participant selection criterion in the majority of the studies: participants who applied were included irrespective of their levels of complaints. In only a few studies were participants selected above a minimum stress level. As is argued by Murphy (1996) this may be due to the subclinical levels of stress in a healthy and working population. However, from a preventive point of view, selection of participants may enlarge effectiveness and efficiency (Tallant et al. 1989). Further, from the point of view of efficiency a compact programme that includes a minimum of sessions is of interest. Finally, a very important issue is to perform studies with a long-term assessment, given its relevance for the impact of the intervention.
This study tries to meet the need for studies. by obtaining new data and considering some of these issues. We conducted a trial that compared two four-session interventions. One intervention consisted of a combined programme of physical exercise and relaxation, the other was a cognitive intervention. The participants in the study were included on the condition that they exceeded a certain level of stress complaints. Both short-term and long-term effects were investigated.
Method
Participant selection and design
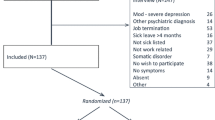
The study was designed as a randomised clinical trial with pre-trial, post-trial and 6-month follow-up measures. Employees working in a telecommunications company in The Netherlands were invited to participate in a screening programme on health experience and perceived work environment. The programme was introduced as a periodic health check-up. From a working population of 7,522 employees, 51% (n=3,852) agreed to participate and filled out a questionnaire (Fig. 1).
This sample comprised 3,497 men and 355 women; their ages ranged from 18 years to 63 years. Of these employees, 396 reported a high rate of distress, which was defined as a distress score above 0.32 on the Four-Dimensional Symptom Questionnaire (4DSQ) (Terluin 1994). This cutoff point is based on data obtained from approximately 700 employees that participated in stress-reducing programmes. Of the most distressed employees, 10% rated higher than 0.32.
After giving informed consent the employees with a score above 0.32 were randomly assigned to one of two conditions: physical and relaxation exercises (FYS) or cognitive intervention (COG). Of the employees, 71 started in the FYS group and 59 in the COG group (time 1 [T1]). The company did not permit dropout research with questionnaires.
After the training period (time 2 [T2]), approximately 10 weeks later, subjects of the intervention groups had to fill out a post-session questionnaire. Six months after the program ended (time 3 [T3]) participants were requested to fill out the follow-up questionnaire (Fig. 1).

Flowchart of subjects participating in the interventions.
The interventions
Physical exercise and relaxation
The aim of the physical intervention was to provide awareness and introduction of physical and relaxation exercises in daily work activities. The level and intensity of the exercises were modified in such a way that it met the physical capability of each individual. The sessions took place during working hours, and the participants were supposed to continue their work afterwards. The exercise programme was designed, and the protocol set and conducted, by authorised physical therapists. Four training sessions, each lasting for 1 h, were given over a period of 8 weeks. The intervals between the sessions were 2 weeks, 2 weeks and 4 weeks.
Every session consisted of four main parts: introduction, warming-up and physical exercise, relaxation exercise and an assignment. During the introduction of session 1 the term “stress” and its effects on physical, psychological and behavioural level were clarified. Further, the possibility of coping by physical activities was emphasised. Next, the participant started with warming up and keep fit exercises. The relaxation exercise was designed as progressive muscle relaxation, according to Jacobson (1929). At the end of the session the participant was asked to implement the relaxation exercise during daily stressful situations. The second session started with an assessment of the past 2 weeks and included the implementation of the relaxation exercise. The fitness exercise was focused on the relationship of heart rate and strain and ended with a breathing exercise (Roesel 1928) and muscle stretching. The participant was urged to use the knowledge learned. The third session consisted of an assessment, a keep-fit exercise, a focus on work stress and autogenous training (Schultz 1935). The participants planned their daily exercise and scored their own progression. In the fourth and final session the different physical exercises and relaxation techniques were reviewed, including meditation (Lowenstein 2002). The session ended with advice on the prevention of relapse.
Cognitive intervention
The aim of the cognitive intervention was to restructure irrational beliefs. The theme of the first session was education. The term “stress” was explained by a description of the signals and course of the complaints. The complaints were placed in a positive framework, e.g. backache as body language for heavy stress load. The participants were presented with specific coping techniques, such as focusing on problems and seeking social support. For homework they made a list of (job-related) stressors. The second session started with a discussion of this list. The participants were asked to read a popularised scientific book on rational emotive therapy (RET) (Ellis and Grieger 1986). The theme of the third session was RET: irrational reasoning as a pitfall, and adjustment by rational reasoning. The participants were sent away with the instruction to make themselves familiar with this skill. The fourth and final session was a review of the specific skills and advice on the prevention of relapse. The cognitive interventions were conducted by psychologists and were of the same frequency and duration as the physical exercise programme and conducted during working hours.
Measurements
Psychological complaints
The 4DSQ (Terluin 1994, 2004) measures psychological complaints. It consists of four dimensions: distress (16 items), depression (six items), anxiety (12 items) and somatisation (16 items). The items are scored on a 5-point Likert scale for occurrence during the past week and describe the complaint with five response categories, from no complaints (last week I did not worry) to very often/continuously (last week I worried continuously). The internal consistency (Cronbach’s alpha) of the entire questionnaire in our study was 0.88; for each of the four subscales it was 0.75 for somatisation, 0.70 for distress, 0.71 for depression and 0.79 for anxiety.
Burnout
Burnout, used as an outcome variable, is measured by the UBOS. The UBOS is the Dutch version (Schaufeli and Van Dierendonk 2000) of the Maslach Burnout Inventory–General Survey (MBI-GS) (Maslach et al. 1997). It consists of 16 items, which represent emotional exhaustion (five items), cynicism (five items) and professional efficacy (six items). Each item is rated on a 7-point scale ranging from 0 (working all day is never a strain to me) to 6 (working all day is a strain to me every day). The internal consistency (Cronbach’s alpha) for the three subscales in the present study was 0.84 (exhaustion), 0.72 (professional efficacy) and 0.68 (cynicism).
Fatigue
Fatigue, as an outcome variable, was measured by the Checklist Individual Strength (CIS) (Vercoulen et al. 1994). The CIS is a 20-item multi-dimensional self-report questionnaire that measures fatigue. It consists of four dimensions: the subjective experience of fatigue (eight items), reduction in activity (three items), reduction in concentration (five items) and reduction in motivation (four items). The complete questionnaire consists of 20 statements for which the person has to indicate, on a 7-point scale, to what extent the particular statement applies to him or her. The statements refer to aspects of fatigue experienced during the previous 2 weeks (for example, I feel tired). Cronbach’s alpha for the total CIS was 0.91, and for the scales the α ranged from 0.79 to 0.91, in accordance with results reported in the literature (Beurskens et al. 2000).
Statistical analysis
Firstly, a check of the randomisation was conducted by a multivariate analysis of variance (MANOVA) on the pre-test scores. Furthermore, selection effects were checked by dropout analysis. Secondly, we tested the effectiveness of the interventions with repeated measures MANOVA on pre-test to post-test scores, on pre-test, post-test and follow-up scores and post-test to follow-up scores. The intervention was the between-subject factor, whereas time was used as the within-subject factor. Thirdly, to compare our results with that in the literature, we calculated the effect sizes (Cohen’s d) as a standardised measure of change. Finally, conceptualising the process of employees returning to normal functioning, we calculated the clinical significance of the interventions as proposed by the method of Jacobson (Jacobson and Truax 1991). In this method the two steps towards establishing clinically significant change are: establishing a cut-off point between a dysfunctional and a functional population and establishing an index for measuring whether or not the change during the course of the intervention is reliable (McGlinchey and Jacobson 1999). The dysfunctional population is defined as ±1 SD above the mean of the functional (in our case the not stressed) population.
The index to calculate the reliability of change represents the difference of a subject’s post-test score minus the subject’s pre-test score divided by the standard error of difference between the two test scores. An index larger than 1.96 would be unlikely to occur (P<0.05) without actual change.
Results
The results are presented in three sections: the description of characteristics of the participants, a dropout analysis and the analysis of the effectiveness of both programmes.
Participants
At T1 130 employees were participating in the programme. The mean age of this group was 44.2 years (SD=7.4), and the group consisted of 117 (90%) men and 13 (10%) women. On average they had 21.1 years (SD=9.8) of work experience. The work of the employees was diverse and could be divided in four categories: executive, administrative, managerial or advisory. Following the training period, after 2 months [T2], 44 (62%) subjects of the FYS group and 46 (78%) subjects of the COG group filled out the post-session questionnaire. At T3, another 6 months later, 54 (76%) subjects of the FYS group and 46 (78%) subjects of the COG group filled out the follow-up questionnaire.
Of the 130 employees who started the intervention 75 (58%) [COG 36 of 59 (=61%); FYS 39 of 71 (=55%)] completed the intervention and filled out all three questionnaires. Only participants with complete data records were included in the analysis (n=75).
Selection effects
As noted earlier, of the 396 employees who were advised to participate in the intervention programme, 67% dropped out before the first session. The question is whether these dropouts differed significantly from those who continued to participate in this study. To answer this question we conducted two MANOVAs. We compared dropouts and completers on the outcome measures at T1. The self-report measure on psychological complaints (4DSQ) showed no significant differences at the multivariate level: Pillai’s F (4.391)=0.69, P=0.991. No significant differences were found between dropouts and completers on age, work experience and gender (F (1.390)=0.744, P=0.389; F (1.390)=0.101, P=0.751; χ2 (1)=2.327, P=0.127, respectively).
Thus, no selection effects could be demonstrated for the completers. In a next phase the FYS and COG subgroups were distinguished still at T1. We examined possible selection effects by carrying out MANOVAs. For psychological complaints (4DSQ) and burnout (UBOS) there were no significant differences: Pillai’s F was (4.70)=0.185, P=0.945 and (3.69)=2.046, P=0.116, respectively. By contrast, for fatigue (CIS) we found a difference: Pillai’s F (4.68)=4.667, P=0.002. All scales of the CIS differed significantly: fatigue, P=0.001, motivation, P=0.011, activity, P=0.014, concentration, P=0.003.
In conclusion, a difference in fatigue between the groups resulted as a side effect from a randomised procedure to fill up the groups. Employees who were selected in the FYS group experienced more fatigue.
Given the fact that the difference between groups is mainly caused by the entity “fatigue” we checked the intercorrelations between the outcome variables.
As can be seen in Table 1 the intercorrelations between the subscales of the different questionnaires range from small to moderate, which fits with their conceptual dependence. The conceptual independence of psychological complaints and burnout plus fatigue is exemplified by the low intercorrelations between these variables. Given the randomisation of the intervention groups the selection effect must be a coincidence.
Intervention effects
Means and standard deviations on the outcome measures are presented in Table 2. The data were subjected to repeated measures MANOVA. The results of these analyses are represented in Table 2.
Short-term effects (pre-test to post-test analysis)
Psychological complaints
As can be seen in Table 2, for both groups, a decline in psychological complaints was found. Repeated measures MANOVA indicated a significant main effect for time, but no main effect for group or the interaction of group and time. As for the four subscales, a significant effect for time and not an effect of the intervention type for both groups is on stress reduction. The effect sizes, shown in Table 3, displayed, for the COG group, a large effect size (Cohen’s d) for distress, a medium effect size for somatisation and depression and a small effect size for anxiety. There was a medium effect for the four subscales for the FYS group, except for somatisation. This effect size was small. Depending on the subscales, return to normal functioning varies from 44% to 54% in the FYS group and from 50% to 61% in the COG group (Table 4).
Burnout
For both groups Table 2 indicates a decrease for exhaustion, cynicism and reduced professional efficacy. In time the decrease is significant for exhaustion and reduced professional efficacy but not for cynicism. The groups differ nearly significantly for exhaustion: a decrease in the FYS group and no clear orientation in the COG group. For the two groups there is no significant effect of intervention type for exhaustion, cynicism and reduced professional efficacy. The effect size (Cohen’s d) of FYS and COG on the subscales is small (Table 3). Depending on the subscales, return to normal functioning ranges from 38% to 49% in the FYS group and 31% to 47% in the COG group (Table 4).
Fatigue
The scores on subjective fatigue, reduced motivation, reduced activity and reduced concentration decreased (Table 2). The reduction in time is significant for subjective fatigue and reduced activity, and marginally significant for reduced motivation and reduced concentration. The groups differ significantly for the CIS (fatigue) and the four subscales, but no significant intervention effect can be observed. There was a small effect size (Cohen’s d) in the FYS group for fatigue, with a medium effect size in the COG group (Table 3). Depending on the subscales, return to normal functioning varies from 33% to 51% in the FYS group and 47% to 61% in the COG group (Table 4). The recovery of employees for subjective fatigue in the COG group is significantly better than for the FYS group.
Follow-up effects (effects 6 months later)
Psychological complaints
The positive reduction in psychological complaints remained stable 6 months after the last session (Table 2). Repeated measures MANOVA indicated a significant main effect for time, attributable to short-term effects. After session four the effect of the type of intervention was maintained. There was a large effect size of FYS and COG on distress, and a medium effect on somatisation, depression and anxiety (Table 3, overall). Depending on the subscales, recovery to normal functioning in the FYS group was 49% and higher and in the COG group 56% and higher (Table 4).
Burnout
The FYS group still demonstrated substantially lower levels of exhaustion, cynicism and reduced professional efficacy. The COG group demonstrated an increase for exhaustion and cynicism (Table 2). However, significant differences between both groups in the adjusted means were not found, except for reduced professional efficacy. There was no effect from the type of intervention. There was a small effect size (Cohen’s d) of FYS and COG on the subscales (Table 4). Depending on the subscales, return to normal functioning in the FYS group was 31% and higher and in the COG group 39% and higher. In the FYS group employees relapsed to abnormal for exhaustion and professional efficacy, and in the COG group only for exhaustion (Table 4).
Fatigue
As can be seen in Table 2 the decrease found at T2 is maintained and significant. The significant effect of time is still there and can be attributed to short-term effects. The effect of intervention type is not significant. The effect size (Cohen’s d) in the COG group on the four subscales is small, whereas the effect size of FYS on subjective fatigue, reduced activity and reduced concentration remains at a medium level (Table 3). Depending on the subscales, return to normal functioning in the FYS group is 36% and higher and in the COG group 44% and higher, which means that some employees reverted to abnormal functioning (Table 4).
Discussion and conclusions
The aim of the present randomised trial was to investigate whether a physical, combined, intervention of relaxation and physical exercise has a more positive effect on the reduction of psychological complaints than a cognitive intervention. No differential effect between the two conditions was demonstrated. It was found that both interventions revealed a positive impact on psychological complaints, burnout and fatigue, both in the short term and at 6-months’ follow up.
The decrease in psychological complaints, burnout and fatigue for the physical and cognitive intervention is consistent with our expectations and previous research. However, the fact that both programmes were likewise effective, plus the lack of a control group, urged us to assess the clinical significance of the results. Jacobson et al. (1984) introduced the idea that, for psychological interventions, clinically significant change is a good measure of the return to normal functioning. Although the difference between both interventions was not significant, with regard to psychological complaints approximately 50% of the employees that participated in the physical intervention and 60% that participated in the cognitive intervention improved and returned to normal function. On burnout and fatigue the improvement was less. For exhaustion, 31% of the employees in the physical intervention returned to normal functioning and 39% in the cognitive intervention. For subjective fatigue the percentages were 36 and 50, respectively.
As noted above, no (statistical) interaction effect between the two interventions was found. That both interventions were equally effective is remarkable in the light of previous research such as the meta-analysis of van der Klink et al. (2001). Their meta-analysis revealed a small effect for the relaxation techniques on psychological complaints such as anxiety and depression and a significantly larger effect for cognitive interventions on these complaints.
There may be two explanations for this result: the length and duration of the interventions and the content of the interventions. The first explanation for the lack of a differential effect of both intervention types may be attributed to the length and duration of the intervention period necessary to improve psychological complaints. Four sessions may be too short for an intervention to provide a differential effect. How long these interventions should be is subject to debate. For cognitive interventions a large range of results is described in the literature with regard to the length and duration of the intervention. For instance, Mueser et al. (1997) reported poor results of short-term interventions for psychiatric rehabilitation, contrary to Barkham and Shapiro (1990), who reported a reliable and clinically significant improvement for mild depression after two sessions only. Further, van der Klink et al. (2001) stated that the mean number of sessions for the cognitive interventions with a large effect on complaints such as anxiety and depression is seven. Similar effects are found for relaxation programmes and physical exercise (van der Klink et al. 2001; McIntyre et al. 1990; Yeung 1996; Raglin and Wilson 1996; Steptoe et al. 1998).
Summarised, the reduction of psychological complaints, burnout and fatigue, in our study, by four sessions underlines the possibility of success through a brief intervention and confirms the finding of Barkham and Shapiro (1990) with regard to the effectiveness of a brief therapeutic intervention.
The second explanation for the lack of an interaction effect is the content of the interventions. In this study a combined intervention of relaxation and physical exercise was been introduced. The effect size of this combination of relaxation and physical exercise on psychological complaints, especially distress, appears larger than the effect size of relaxation alone in the meta-analysis by van der Klink et al. (2001). However, the effect size of the physical intervention might be overestimated by the lack of a control group. Despite that, relaxation and physical exercise are each known for their positive effect on minor psychological complaints. In accordance with Benson et al. (1975) is the postulation that exercise may also be a form of meditation that triggers a more relaxed state or a form of biofeedback that teaches people to regulate their autonomic arousal. From this point of view a combination of physical exercise and relaxation may have caused the relatively large effect size. To confirm this hypothesis new research with three types of interventions—relaxation, physical exercise and control—is needed.
There are a number of potential limitations in this study. The first limitation of the present design is the lack of a control group. Therefore, selection effects and effects of regression to the mean cannot be excluded. However, the lack of a control group is a considerable problem in field studies. If an intervention proved to be beneficial, withholding it from employees in need is an important ethical issue (Goldenhar and Schulte 1994). However, an experimental design for field studies is more favourable than semi-experimental designs for the generalisation of the results.
A second limitation for the generalisation of the results concerns a selection effect of the physical intervention. Despite the randomisation procedure the employees in this condition had significantly more complaints about fatigue. It emphasises, again, the need for a controlled study.
In conclusion, the present study is one of the few that has a long-term assessment of two interventions randomly assigned to highly stressed employees. A newly designed physical intervention is compared with a cognitive intervention. Both interventions were equally effective for psychological complaints, burnout and fatigue. Moreover, 50% of the employees with psychological complaints that participated in the physical intervention and 60% that participated in the cognitive intervention improved and returned to scores with normal range. The present study emphasises the importance of the study of effects in a field setting.
References
Agency for Health Care Policy and Research (1993) Depression in primary care: guideline overview. J Natl Med Assoc 85:501–503
American Psychiatric Association (1993) Practice guideline for major depressive disorder in adults. American Psychiatric Association, USA
Barkham M, Shapiro DA (1990) Brief psychotherapeutic interventions for job-related distress: a pilot study of prescriptive and exploratory therapy. Couns Psychol Q 3:133–147
Benson H, Greenwood MM, Klemchuk H (1975) The relaxation response: psychophysiologic aspects and clinical applications. Int J Psychiatry Med 6:87–98
Beurskens AJ, Bultmann U, Kant I, Vercoulen JH, Bleijenberg G, Swaen GM (2000) Fatigue among working people: validity of a questionnaire measure. Occup Environ Med 57:353–357
Byrne A, Byrne DG (1993) The effect of exercise on depression, anxiety and other mood states: a review. J Psychosom Res 37:565–574
Cooper CL, Dewe PJ, O’ Driscoll MP (2001) Organizational stress: a review and critique of theory, research, and applications. Sage Publications, Thousand Oaks
Ellis AE, Grieger RME (1986) Handbook of rational–emotive therapy, vol. 2. Springer, Berlin Heidelberg New York
Fedoroff IC, Taylor S (2001) Psychological and pharmacological treatments of social phobia: a meta-analysis. J Clin Psychopharmacol 21:311–324
Gauvin L, Spence JC (1995) Psychology research on exercise and fitness: current research trends and future challenges. Sport Psychol 9:434–448
Goldenhar LM, Schulte PA (1994) Intervention research in occupational health and safety. J Occup Med 36:763–775
Heimberg RG (2002) Cognitive–behavioral therapy for social anxiety disorder: current status and future directions. Biol Psychiatry 51:101–108
van der Hek HH, Plomp HN (1997) Occupational stress management programmes: a practical overview of published effect studies. Occup Med 47:133–141
Houtman IL, Bongers PM, Smulders PG, Kompier MA (1994) Psychosocial stressors at work and musculoskeletal problems. Scand J Work Environ Health 20:139–145
Jacobson E (1929) Progressive relaxation. University of Chicago Press, Chicago
Jacobson NS, Truax P (1991) Clinical significance: a statistical approach to defining meaningful change in psychotherapy research. J Consult Clin Psychol 59:12–19
Jacobson NS, Follette WC, Revenstorf D (1984) Psychotherapy outcome research: methods for reporting variability and evaluating clinical significance. Behav Ther 15:336–352
van der Klink JJ, Blonk RW, Schene AH, van Dijk FJ (2001) The benefits of interventions for work-related stress. Am J Public Health 91:270–276
Lazarus RS, Folkman S (1984) Stress, appraisal, and coping. Jason Aronson, New York
Lowenstein KG (2002) Meditation and self-regulatory techniques. In: Shannon S (ed) Handbook of complementary and alternative therapy in mental health. Academic, San Diego, pp 159–181
Maslach C, Jackson SE, Leiter MP (1997) Maslach burnout inventory, 3rd edn. In: Zalaquett CP (ed) Evaluating stress. Scarecrow Press, Lanham, pp 191–218
McGlinchey JB, Jacobson NS (1999) Clinically significant but impractical? A response to Hageman and Arrindell. Behav Res Ther 37:1211–1217
McIntyre CW, Watson D, Cunningham AC (1990) The effects of social interaction, exercise, and test stress on positive and negative affect. B Psychonomic Soc 28:141–143
Meichenbaum DH, Deffenbacher JL (1988) Stress inoculation training. Couns Psychol 16:69–90
Mueser KT, Drake RE, Bond GR (1997) Recent advances in psychiatric rehabilitation for patients with severe mental illness. Harv Rev Psychiatry 5:123–137
Murphy LR (1996) Stress management in work settings: a critical review of the health effects. Am J Health Promot 11:112–135
Paoli P, Merllie D (2000) Third European Survey on Working Conditions 2000. Office for Official Publications of the European Communities, Luxembourg
Raglin JS, Wilson M (1996) State anxiety following 20 minutes of bicycle ergometer exercise at selected intensities. Int J Sports Med 17:467–471
Roesel R (1928) Die psychologischen Grundlagen der Yogapraxis [The psychological basis of yoga practice]. In: Osterreich TK (ed) Beitrage zur Philosophie und Psychologie. Kohlhammer, Stuttgart
Salmon P (2001) Effects of physical exercise on anxiety, depression, and sensitivity to stress: a unifying theory. Clin Psychol Rev 21:33–61
Schaufeli WB, Van Dierendonk D (2000) Utrechtse Burnout Schaal (UBOS)- Test Handleiding [Utrecht burnout scale: test manual]. Lisse. Test series
Schultz JH (1935) Uebungsheft fuer das autogene Training [A practice manual of autogenous training]. Thieme, Leipzig
Scott J (2001) Cognitive therapy for depression. Br Med Bull 57:101–113
Steptoe A, Butler N (1996) Sports participation and emotional wellbeing in adolescents. Lancet 347:1789–1792
Steptoe A, Kimbell J, Basford P (1998) Exercise and the experience and appraisal of daily stressors: a naturalistic study. J Behav Med 21:363–374
Stichting van de Arbeid. Nota “Beperking ziekteverzuim en instroom in de WAO [Report “reduction of absenteeism and work incapacitation risk”] (2002) Den Haag: Stichting van de Arbeid, Publicatienummer. 5/9
Tallant S, Rose SD, Tolman RM (1989) New evidence for the effectiveness of stress management training in groups. Behav Modif 13:431–446
Terluin B (1994) Nervous breakdown substantiated: a study of the general practitioner’s diagnosis of surmenage (thesis) (in Dutch). Kerckebosch, Zeist, The Netherlands
Terluin B, Van Rhenen W, Schaufeli WR, De Haan M (2004) The four-dimentional symptom questionnaire (4DSQ): measuring distress and other mental health problems in a working population. Work Stress 18:187--207
Vercoulen JHMM, Swanink CMA, Fennis JFM, Galama JMD, et al (1994) Dimensional assessment of chronic fatigue syndrome. J Psychosom Res 38:383–392
Vickers A, Zollman C (1999) ABC of complementary medicine. Hypnosis and relaxation therapies. BMJ 319:1346–1349
Yeung RR (1996) The acute effects of exercise on mood state. J Psychosom Res 40:123–141
Acknowledgements
This research was supported by grants from Zorg Onderzoek Nederland (ZON) and ArboNed N.V.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Van Rhenen, W., Blonk, R.W.B., van der Klink, J.J.L. et al. The effect of a cognitive and a physical stress-reducing programme on psychological complaints. Int Arch Occup Environ Health 78, 139–148 (2005). https://doi.org/10.1007/s00420-004-0566-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-004-0566-6