
Abstract
Objectives
Of an estimated 500,000 workers in the USA potentially exposed to perchloroethylene (PCE), the largest share is employed in the dry-cleaning industry. PCE, a non-flammable solvent, has commercial applications as a chemical intermediate, metal degreaser and, since the 1950s, primary solvent in the dry-cleaning industry. The International Agency for Research on Cancer (IARC) currently finds sufficient evidence to designate PCE as carcinogenic in animals, with limited evidence in humans. With regard to occupational exposure through dry-cleaning, PCE is considered to be possibly carcinogenic to humans. This review was conducted to assess the current epidemiological literature on PCE and specific cancers.
Methods
A comprehensive search was conducted to identify all available epidemiological literature pertaining to the carcinogenic effects of PCE. Forty-four papers that provided reasonable data on up to 17 cancer sites were critically reviewed in the context of the available background literature for each cancer site and were assessed on the basis of specified methodological and scientific quality criteria.
Results
While all the epidemiological studies selected for review investigated similar exposure–health outcome relationships, there was a broad diversity of proxy measurements of exposure to PCE, as well as numerous specific cancer outcomes of interest. The widespread lack of valid exposure measurements or other adequate indicators of potential for exposure were consistent limitations. We found no evidence of an association between breast, prostate, skin or brain cancer and exposure to PCE. A relationship between PCE and cancer of the following sites was considered unlikely: oral cavity, liver, pancreas, cervix lung. Scientific evidence was inadequate for laryngeal, kidney, esophageal and bladder cancers.
Conclusions
The current epidemiological evidence does not support a conclusion that occupational exposure to PCE is a risk factor for cancer of any specific site. Priority areas in which additional data are most needed include cancers of the esophagus and bladder.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Perchloroethylene (tetrachloroethylene, PCE), a chlorinated hydrocarbon, is a non-flammable solvent with commercial applications as a chemical intermediate, metal degreaser, and, since the 1950s, primary solvent in the dry-cleaning industry [46]. An estimated 500,000 workers in the USA are potentially exposed to PCE, of whom 119,000 to 278,000 are employed in the dry-cleaning industry [78, 94]. The highest potential for exposure occurs during operation of the machinery, primarily via inhalation and skin contact. In 1991, about one-third of the estimated 28,100 dry-cleaning plants in the USA used an open transfer process in which solvent-wet clothes were moved from washer to dryer by the operator, increasing the potential for exposure. In contrast, in 2000, less than 5% of approximately 30,000 dry-cleaning establishments still employed transfer machines. All other plants used a closed transfer process, which involves less potential for worker exposure [46].
PCE inhaled at high concentrations may be toxic to various human organ systems. Neurological effects include changes in behavior and coordination, as well as damage to the central nervous system. Damage to the liver and kidneys has also been documented [23, 95]. Exposure to PCE has shown a carcinogenic effect in some animal studies; however, the mechanistic processes that occur in some species of animals (e.g., mice) do not occur in humans, and conclusions based on animal models may be inappropriate [23, 46, 95]. The International Agency for Research on Cancer (IARC) currently finds sufficient evidence to designate PCE as carcinogenic in animals, with limited evidence in humans. With regard to occupational exposure through dry-cleaning, PCE is considered to be possibly carcinogenic to humans [46].
Epidemiological research concerning possible human health effects of PCE exposure was initiated when results of National Cancer Institute (NCI) research in 1977 indicated that PCE induced liver tumors in mice [46]. Two epidemiological cohort studies among US dry-cleaners were conducted by NCI and the National Institute for Occupational Safety and Health (NIOSH), with first results published in 1979 by Blair et al. [10] and in 1987 by Brown and Kaplan [21]. With few exceptions, later published risk estimates for PCE exposure (or for dry-cleaners as a surrogate for exposure) were either from population-based case–control studies or from national census-based cancer studies evaluating many different occupations and agents. Though many studies have been conducted mainly among populations that include dry-cleaning workers, several different cancer excesses have been reported, including cancer of the bladder, esophagus, large intestine, kidney (renal cell) and cervix. However, few consistent patterns have emerged. A few studies have evaluated PCE exposure among other occupational cohorts such as aircraft maintenance workers, where exposure is generally to multiple solvents. An assessment of the risks specifically associated with exposure to PCE is difficult or impossible in these studies.
This review is a critical assessment of the epidemiological literature on the possible relationship between PCE and specific cancer sites. The underlying rationale for a critical review is that the quality (inherent or for a specific purpose) of all available published papers is not equal. The synthesizing of evidence for an association between an exposure and a health outcome often leads to interpretations that are not necessarily reduced to a single quantitative result (as is the goal of meta-analysis). Conclusions based on a critical synthesis of the literature can avoid equating consistency with validity and deriving quantitative conclusions beyond what is reasonable, in view of the limitations of the literature.
Materials and methods
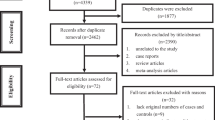
A comprehensive search with MEDLINE was conducted, based on the following main key words: tetrachloroethylene, laundry/dry-cleaning, and degreasing. Searches for relevant synonyms (e.g., PCE), occupations, industries, or authors, were also conducted. Bibliographies from relevant reviews and papers were checked to ensure complete identification of the pertinent literature. Preliminary screening excluded papers according to the following criteria: (1) the paper was not an epidemiological study, e.g., case reports, exposure assessments, reviews of the literature; (2) the outcome of interest was not cancer incidence or mortality; (3) the potential exposure was not occupational, e.g., environmental exposure only; (4) the paper was not in a peer-reviewed publication; or (5) the paper was a death-certificate study that presented only proportionate mortality ratios (PMRs). Seventy-eight papers published between 1963 and 2003 remained for potential inclusion in the critical review.
Two or more epidemiologists independently reviewed each paper for final inclusion. The overall strategy was to include as many studies as possible, and to identify their limitations rather than to exclude studies. Reviewers used a standard critical review instrument to ensure uniformity of evaluation.
The critical review process included the following steps:
-
1.
An assessment of each study as to its quality, and, therefore, its ability to contribute to a critical assessment.
-
2.
Consideration of the study results within the context of the collective literature (consistency).
-
3.
Appraisal of the strength of the evidence for an association.
-
4.
Derivation of conclusions based on a final assessment of all informative results.
An additional 34 papers were excluded from the full critical review for at least one of the following reasons: multiple publications involving the same study population [11, 12, 13, 21, 49, 72, 73, 78]; results of a single study were included as part of a larger multi-center study already included in the critical review [61, 66, 80]; no risk estimate was presented [6, 7, 34, 39, 40, 68, 74, 96]; the probability of any substantial PCE exposure was low or undefined and could not be determined in the study population [15, 29, 32, 35, 36, 50, 77]; PCE was one of many possible exposures without further differentiation [38, 42, 44, 51, 58, 71, 82, 97].
Forty-four articles remained for the critical review and synthesis. Among the studies selected for critical review were some that drew from the same study population, but were retained because they included unique sub-populations or contained pertinent information not otherwise reported; information from these papers was incorporated into discussions of results by study population. The 44 articles provided reasonable data on 17 cancer sites, and were critically reviewed in the context of the available background literature for each cancer site. For some cancer sites (bone, eye, thyroid) too few results were available in these articles to permit critical review.
The quality of each study was individually critiqued, and the quality and strength of evidence for an association was determined. Assessment of overall quality of studies incorporates many factors, some of which are subjective: strength of study design (including the study population definition and time period); quality of exposure assessment; validity of the outcome definition; avoidance of bias, and technical aspects of the design and analysis. The quality of exposure assessment is key to the critical review. Most of the studies included in this review defined exposure using relatively crude occupation or industry codes, either for possible PCE-exposed dry-cleaners or for a combined group of non-PCE exposed launderers and dry-cleaners, generally without information regarding exposure to specific agents. Other studies that tried to assess PCE exposure more directly often included mixtures of a variety of agents. Therefore, it was necessary for us to determine—on the basis of time period of potential exposure, exposure definition or measurement, exposure history, and knowledge of industry practices—the probability and extent for PCE exposure of a specific study population.
PCE exposure was considered "likely" if the assumption of a predominant PCE exposure for a cohort or sub-cohort seemed plausible. PCE exposure was considered "mixed" either if study subjects appeared to have been exposed to a variety of substances or if the study population included different industry or job categories. Within this "mixed" category a partial PCE exposure was considered "likely" if PCE was among the solvents or agents to which the populations or cases were exposed, and "possible" if PCE might have been among the solvents to which populations or cases were exposed, although no specific information with regard to exposure was available.
After the quality of each study had been assessed, the weight of evidence across studies was synthesized and assessed. The following were considered: number of studies of reasonable quality that were available, the general magnitude of effect, if any, and whether the results across studies were consistent. Finally, the weight of epidemiological evidence was determined to be either positive or negative, arguing for or against an association, or considered inadequate for any conclusion to be to drawn with regard to the relationship in question.
Results
The literature that was critically reviewed consisted of 12 cohort and 32 case–control studies. Of the twelve cohort studies, only four were of well-defined occupational cohorts: two dry-cleaner cohorts [16, 79] and two cohorts of aircraft workers exposed to multiple solvents [19, 89]. The two dry-cleaner cohorts were considered the most likely studies to elucidate the health effects of PCE, for, despite their limited characterization of individual exposure, they had the greatest opportunity for PCE exposure. On the other hand, they did not measure or control for behavioral risk factors (e.g., smoking, alcohol consumption), even though these are the main risk factors for some of the cancers evaluated. Details of these studies follow, and key characteristics of the cohort studies are included in Table 1.
Study summaries
Researchers at the NCI conducted a cohort study of dry-cleaners, including more than 5,000 members of a dry-cleaners' union in the state of Missouri [10, 12, 16]. The cohort was followed from 1 January 1948 or entry into the union (whichever came later) until 1 January 1979. Vital status of the cohort was updated through 31 December 1993 [16]. Using the available job titles as a surrogate for PCE exposure, the investigators made a qualitative exposure assessment. They assigned cohort members an exposure index based on job title and other external data in order to approximate exposure. Confounding due to race, gender, age, and calendar period was controlled in the analysis. Additional analyses were conducted of workers entering the union after 1960, because PCE was the predominant solvent used in the majority of shops after that time. The results of this analysis were similar to results based on all exposure groups combined for most cancer sites.
NIOSH also conducted a cohort study among members of a dry-cleaners' union [21, 49], using union records to identify 1,703 dry-cleaners (65% female) from four US states (New York, California, Illinois, and Michigan). Vital status has been updated twice by Ruder et al. [78, 79]. Cohort members exposed primarily to PCE before 1960 were followed for 56 years (1940–1996). Exposure was qualitative, indicated by union membership. Within the cohort, a subgroup primarily exposed to PCE was identified for additional analysis. This sub-cohort consisted of workers who (at the time of cohort definition) had worked only in shops where PCE was the predominant solvent. Observed mortality was compared with national death rates, and was controlled for gender, race, and calendar period.
Spirtas et al. [89] and Boice et al. [19] studied aircraft maintenance employees and manufacturing workers, respectively. Both cohorts included employees almost certainly exposed to PCE; however, they were also likely exposed to other solvents. Exposure, defined by job title, was to mixed solvents, primarily trichloroethylene in the Spirtas cohort [89]. A sub-cohort of 851 employees also exposed to PCE was examined, but results were only presented for non-Hodgkin's lymphoma and multiple myeloma [91]. Blair and colleagues [15] recently published an update of this cohort through 1990, but no results specific to PCE were reported.
Boice et al. [19] identified a sub-cohort of employees routinely exposed to PCE within a large cohort of aircraft manufacturing workers exposed to a variety of compounds and estimated that 30% of these workers also had prior exposure to trichloroethylene (TCE). They reported that analyses of subgroups exposed to PCE but not TCE displayed similar patterns of mortality. Exposure assessment in this study was qualitative, based on potential for exposure in a specific job.
Several northern European studies were record-linkage studies based on census data linked with cancer registry information. Occupation or industry classification at one point in time was used as a surrogate of exposure [2, 24, 54, 55, 59, 63, 64]. These reports presented results for the combined group of laundry and dry-cleaning workers and, therefore, likely included a large proportion of subjects not exposed to PCE. The Finnish cohort [3] consisted of workers who had been biologically monitored for occupational exposures at the Finnish Institute of Occupational Health. However, the occupation or industry of these workers is not reported, no information regarding duration of exposure is available, and at least a part of the cohort was additionally exposed to other halogenated hydrocarbons.
Thirty-two case–control studies of PCE exposure and cancer incidence or mortality were critically reviewed, and details of the studies are included in Table 2. Most available case–control studies were population-based or hospital-based, not from any specific occupational groups, and evaluated the association between PCE exposure and one specified cancer site. A small number of studies evaluated multiple cancer sites.
The exposure definition in the majority of the case–control studies was self-reported employment in the laundry and dry-cleaning industries or self-reported exposures to dry-cleaning solvents, which served as surrogates for PCE exposure. Exposure prevalence for population-based study subjects was likely to be quite low, limiting study power.
The adjustment for potential confounders varied among studies, although most studies controlled for age and smoking and, depending on the specific cancer site studied, other potential risk factors as well.
Cancer summaries
Oral cancer (ICD-9:140–149)
The strongest risk factors for oral cancers (mouth, tongue, lip, pharynx) are tobacco products and alcohol. Some evidence for a dietary relationship exists, with low intake of fruits and vegetables associated with increased risk. Occupational factors contributing to cancers of the oral cavity are limited [18]. Because the association is strong between oral cancers and tobacco products and alcohol, estimates of risk that do not adequately control for these risk factors were interpreted with caution.
One of the US dry-cleaner cohorts [79], reported excess buccal and pharyngeal cancer, based on nine cases; the standardized mortality ratio (SMR) was 2.07 (95% confidence intervals (CI) 0.94–3.93). Five of the cases were cancer of the tongue among those first employed 20 or more years prior to diagnosis (SMR 5.0, 99% CI 1.62–11.68). Short-term workers (<5 years duration) were at significantly higher risk (P<0.01) than long-term workers. Blair et al. [12, 16] did not observe excess oral cancer mortality among dry-cleaners followed through 1993. Among the workers considered routinely exposed to PCE at an aircraft manufacturing facility, there were fewer oral cancer deaths than expected, based on two cases (SMR 0.55, 95% CI 0.07–1.99) [19].
In an early Swedish study excess risk of oral cancer was reported among laundry or dry-cleaning workers that were followed from 1961–1973 [59]. The only excess reported in a later study, for the period 1971 to 1989, was among Swedish women for cancer of the lip, based on five cases (standardized incidence ratio (SIR) 3.52, P< 0.05) [2]. The authors note, however, that cancer of the lip is generally associated with ultraviolet radiation (in the form of sunlight) and smoking. The authors did not observe excess cancer for any site within the oral cavity in the total Nordic population or in individual country populations and found only one case of tongue cancer (SIR 0.18, P<0.05).
One case–control study found decreased risk of oral cancer for men and women ever employed in the job or industry category for laundry or dry-cleaning workers [45]. The adjusted odds ratio (OR) for men who ever worked in a laundry or dry-cleaning job showed the strongest negative effect (OR 0.39, 95% CI 0.17–0.88), based on eight cases. Analyses by duration of employment in another case–control study indicated decreased risk of oral cancer for those employed for 10 or more years in dry-cleaning (OR 0.4, 95% CI 0.0–31.6), based on one case; however, a small increased risk was found among those who had "ever worked" in the industry (OR 1.2, 95% CI 0.3–4.6, based on seven cases) [98]. Among those with a "probable" exposure to PCE there was a small increase in risk (OR 1.5, 95% CI 0.2–9.5).
These studies varied in their ability to assess the role of known risk factors for cancers of the oral cavity and pharynx. The cohort studies, by nature of their design, did not control for the use of tobacco and alcohol, which for this cancer site limit the quality of the evidence. Risk estimates in the study by Vaughan et al. [98] were adjusted for smoking and alcohol; Huebner et al. [45] also controlled for tobacco and alcohol, as well as length of employment, and observed a reduced risk of cancer, though the study population included laundry and dry-cleaning workers. Because of the strength of the association between smoking and alcohol use and cancers of the oral cavity and pharynx, estimates that do not account for these risk factors must be interpreted with caution. Further, in view of the risk estimates and associated confidence intervals observed in the studies reviewed, it is unlikely that control of other risk factors would have generated positive results.
The quality of evidence available for one to understand the relationship between PCE and oral cancer is limited. Some of the study populations were likely exposed to PCE, even though the quality of the exposure information was poor. The possibility of an association between PCE exposure and oral cancer appears unlikely, given that the two case–control studies that adequately adjusted for important potential confounders found no, or only minimal, excess risk. Further, the lack of strong effects and inconsistent results in the populations restricted to dry-cleaning workers lessen support for an association between PCE and oral cancer. Other explanations for these cancers appear more likely, such as tobacco and alcohol consumption.
Digestive-tract cancers
The literature reviewed showed no evidence for cancer of the stomach or rectum. A statistically significant excess for intestinal cancer in the study by Ruder et al. [79] was restricted to the sub-cohort exposed to PCE and other solvents; all cases of rectal cancer were in this sub-cohort.
Esophageal cancer (ICD-9:150)
Risk factors for esophageal cancer include alcohol and smoking, with clear dose–response and interactive effects demonstrated [31, 69]. Estimates of the mortality from esophageal cancer attributed to smoking alone and in combination with alcohol are high, though socio-economic status and nutrition (specifically low intake of fruit and vegetables) are also considered to be important risk factors [30, 69].
Included in Table 3 are the key characteristics and estimates of effect for the studies reviewed for esophageal cancer. For most of the studies there were few cases of esophageal cancer reported. Blair et al. [16] and Ruder et al. [79] reported statistically significant excesses of esophageal cancer. Blair et al. reported a twofold increase, based on 26 deaths; 18 of those deaths occurred among black male workers (SMR 3.1; 95% CI 1.9–5.0). The authors noted that they did not observe increased risk with increased duration or level of exposure. Ruder and colleagues reported excess esophageal cancer for the whole cohort (SMR 2.47, 99% CI 1.35–4.14) and both sub-cohorts, but only the excess among those exposed to PCE and other solvents was statistically significant (SMR 2.4, 95% CI 1.10–4.56) [79]. Risk was elevated for gender and race sub-categories, although none reached statistical significance. When analyses were stratified by latency and duration, all deaths attributed to esophageal cancer were among those in the long-latency group (20 years or more since first employment); ten of the deaths reported were for those workers whose duration of employment was at least 5 years (SMR 5.03, 99% CI 2.41–9.47) [79]. Boice et al. [19] reported a non-significant increase in esophageal cancers among routinely PCE-exposed aircraft manufacturers, based on six cases (SMR 1.47, 95% CI 0.54–3.21).
In contrast, there were fewer cases reported than expected among both men and women for the Nordic countries combined [2]. There were no cases of esophageal cancer reported among "substantially exposed" launderers and dry-cleaning workers in the Siemiatycki study (i.e., 10 or more years of accumulated exposure in the occupation occurring at least 5 years before onset of disease) [83]. Similarly, there were no cases of esophageal cancer reported by Vaughan et al. among dry-cleaning workers with at least 10 years of exposure, however, among those with probable exposure, an increased relative risk estimate was reported (OR 6.4, 95% CI 0.60, 68.9), based on two squamous cell carcinomas. Analysis for adenocarcinomas also showed no increase in risk, based on two cases [98].
The overall evidence was considered inadequate for firm conclusions to be drawn regarding esophageal cancer and exposure to PCE. The potential for estimates to be confounded by alcohol and smoking as well as the possibility for exposure to other solvents undermines the perceived relationship. Nevertheless, elevated risk estimates from the large dry-cleaner cohorts likely to have PCE exposure cannot be dismissed, especially in light of adequate latency and duration.
Liver cancer (ICD-9:155–156)
The known risk factors for liver cancer vary, depending on the type of cancer. Of hepatocellular carcinoma (HCC), 80% is associated with hepatitis B virus (HBV) [53]. Cirrhosis of the liver has also been associated with HCC, but the exact relationship between alcohol and HCC has not been established (i.e., whether alcohol is a tumor initiator or promoter is unclear). Other risk factors for primary liver cancers include aflatoxins, Thorotrast, vinyl chloride, and some steroids [53].
In the literature reviewed, two studies reported a statistically significant excess of liver cancer among workers defined as "exposed" (Table 4). A case–control study by Stemhagen et al. [90] reported an excess risk of primary liver cancers (OR 2.50, 95% CI 1.02–6.14) and a non-significant excess of HCC (OR 2.29, 95% CI 0.85–6.13) among white men in New Jersey who had been diagnosed between 1975 and 1980. Lynge and Thygesen [55] found an excess of liver cancer among female dry-cleaners or launderers that persisted in a follow-up study [54]; however, in a nested case–control study, the excess was restricted to launderers, with no liver cancer observed among dry-cleaning workers [56]. This excess in risk restricted to Danish launderers mostly explains the slight increase found by Andersen et al. [2] for laundry and dry-cleaning workers in the Nordic countries and supports the results from Ruder et al. and Blair and colleagues, which do not suggest an association between PCE exposure and liver cancer mortality [16, 78]. Ruder et al. observed only one case in the full cohort and Blair and co-workers observed fewer cases than expected [16, 78]. Bond et al. reported a slight increase in risk for chemical workers exposed to PCE among other substances (e.g., vinyl chloride) [20], and Boice and colleagues also reported a slight increase in liver cancer, based on seven cases (SMR 2.05, 95% CI 0.83–4.23) [19].
No study was able to control adequately for potential confounding. The cohort studies, by the nature of their design, were unable to control for important confounders. Bond and colleagues [20] reviewed medical department records for alcohol use and hepatitis, but found them of limited use in controlling for confounding. Stemhagen et al. [90] collected information for smoking, alcohol, and medical history, but did not report adjusted risk estimates.
The studies that contribute most to our understanding of PCE and liver cancer are those with risk estimates that pertain to dry-cleaners alone. However, no study that included an analysis of dry-cleaners alone found an increased risk for liver cancer. The epidemiological evidence in the studies reviewed here, on balance, does not support a relationship between liver cancer and exposure to PCE.
Pancreatic cancer (ICD-9:157)
Age is an important predictor of pancreatic cancer, with most cases in the US occurring between 65 and 79 years of age. The epidemiological evidence is strongest for an association between smoking and pancreatic cancer, including evidence of a dose–response relationship [1]. In addition, there is some evidence that diet plays an etiological role, where fat and animal proteins have been implicated in increasing risk. Conversely, a decrease in risk has been observed with high intake of fruit and vegetables, which may be a reflection of a lifestyle that precludes smoking. There is little conclusive evidence of occupational risk factors for pancreatic cancer, though suggested relationships include products of incomplete combustion of petroleum, pesticides, and specific chemicals and processes (not including dry-cleaning or halogenated solvents) [1].
Five cohort studies reported excess mortality due to pancreatic cancer. The excess was not statistically significant in the study by Blair and colleagues [16] (SMR 1.1, 95% CI 0.70-1.50; 28 cases observed), Anttila et al. [3] (SMR 3.08, 95% CI 0.63–8.99), Boice and co-workers [19] (SMR 1.50, 95% CI 0.72–2.76, 10 cases) or Andersen et al. [2] (SIR 1.41, 95% CI 0.98–1.96 for men; SIR 1.02, 95% CI 0.81–1.26 for women). Ruder and colleagues found no excess among those dry-cleaners exposed only to PCE, but did report an excess among the older cohort exposed to PCE and other solvents (SMR 1.89, 95% CI 1.06–3.11), based on 15 deaths [79]. Siemiatycki observed no cases of pancreatic cancer among those in laundry and dry-cleaning occupations or industries [83].
The studies providing information regarding pancreatic cancer and PCE are limited in their results. Effects observed were not large, and all studies were not able to control for confounding, especially by smoking. Ruder et al. observed a significant excess of pancreatic cancer in the sub-cohort believed to have been exposed to PCE and other solvents, but not in the sub-cohort believed to have been exposed only to PCE. In view of the epidemiological data, the authors' inability to control adequately for confounding in the studies, and the previously mentioned limitations in exposure measurements, an association between PCE and pancreatic cancer appears unlikely.
Respiratory cancers
Laryngeal cancer (ICD-9:161)
Squamous cell carcinomas are the most common histological type of cancer found in the larynx and are believed to be caused by long-term smoking. The strongest risk factor for laryngeal cancer, other than smoking, is alcohol consumption. A dose–response effect and an interactive effect have been demonstrated between smoking and alcohol consumption. Studies of diet and laryngeal cancer have demonstrated a protective effect for some nutrients [8].
In most instances results from the studies reviewed were based on few cases, and no study reported statistically significant excess for laryngeal cancer: Boice et al. observed one case and Ruder and colleagues two [19, 79]. Blair and co-workers [16] observed six cases over the extended follow up (SMR 1.7, 95% CI 0.6–3.7). All six cases were in the higher-exposure category, defined for most cohort members by job held at time of enrollment in the union (SMR 2.7, 95% CI 1.0–5.8). However, results of analyses comparing those who entered the union after 1960 with those entering before 1960 were similar. Andersen et al. reported 14 cases among Nordic men (SIR 1.26, 95% CI 0.69–2.12), nine of whom were Swedish, and six cases among female launderers or dry-cleaners (SIR 0.89, 95% CI 0.33–1.94) [2]. The case–control study by Vaughan et al. [98] found a non-significant excess for cancer of the larynx among those who ever worked in the dry-cleaning industry (OR=2.7, 95%CI 0.6–10.9), based on five cases. Vaughan and colleagues also observed an excess among those who reported working in the industry for 10 or more years (two cases). However, when the results were stratified by probability of exposure, no excess among those considered to have a high (>50%) probability of exposure to PCE (one case) was found [98].
An association between PCE and laryngeal cancer cannot be confirmed from the current body of epidemiological research: the number of cases in each study was extremely small, exposure assessments were limited, and other risk factors were either not controlled for or were self-reported. The available evidence, therefore, is not adequate for firm conclusions to be to drawn regarding an association between PCE exposure and laryngeal cancer.
Lung cancer (ICD-9:162)
Smoking is the primary risk factor for lung cancer [17]. A strong dose–response relationship has been documented. Established occupational risk factors include specific arsenic compounds, asbestos, hexavalent chromium, bis(chloro)methyl ethers, and polycyclic aromatic hydrocarbons. Other discussed risk factors include radon, silica, ionizing radiation, and prior non-malignant lung disease (e.g., silicosis). Consumption of fruits and vegetables has been suggested to have a protective effect [17].
Slightly increased relative risks for lung cancer were found in all of the cohort studies (Table 5). Andersen et al. [2] reported a significant excess of lung cancer for both men and women classified as launderers and dry-cleaners for the Nordic countries combined. Ruder et al. [79] reported a significant increase in risk for the whole cohort of dry-cleaners. Most of the excess was found among those with 20 or more years' latency who worked for less than 5 years (SMR 1.80, 95% CI 1.23–2.55), and in the group exposed to PCE and other solvents (SMR 1.46, 95% CI 1.07–1.95). The sub-cohort exposed to PCE only, showed a small and non-significant increase in risk (SMR 1.17, 95% CI 0.71–1.83). Blair and colleagues [16] reported a small increased risk based on 125 cases (SMR 1.4, 95% CI 1.1–1.6). Stratified results based on duration or exposure were similar. No statistically significant excess of lung cancer was found in the remaining studies by Anttila et al. [3] and Boice and colleagues [19]. In a further analysis of routinely or intermittently PCE-exposed lung cancer cases from the Boice cohort, using internal referents, the risk estimates showed a negative trend with duration of exposure and were lowest in the category with 5 years or more of exposure (relative risk (RR) 0.71, 95% CI 0.49–1.02).
A significant increase of lung cancer among female never-smokers (OR 2.1, 95% CI 1.2–3.7) was reported from one case–control study, where exposure was reported as employment in the dry-cleaning industry [22]. Brownson et al. defined exposure as employment in dry-cleaning and conducted analyses that incorporated duration of employment ("high" exposure defined as more than 13.5 months of employment), but did not conduct this analysis for the lifetime non-smokers [22]. Few cases were included in the case–control studies by Siemiatycki [83] and Muscat et al. [70]; therefore, the results are difficult to interpret. Jahn et al. [47] reported results of a pooled analysis of two case–control studies in Germany. An excess risk for women in the laundry and dry-cleaning industry was found that was not significant after controlling for smoking (OR 2.0, 95% CI 0.94–4.29). The authors reported a poor response rate among controls in the larger of the studies, with an under-representation of people from the lower social class among the controls. Pohlabeln et al. [76] found a non-significant excess among non-smoking women (OR 1.83, 95% CI 0.98–3.40) in a multi-center case–control study in Europe. This study also included launderers in the exposed group, and the non-smoking cases and controls of the Jahn et al. [47] study were part of this study.
As noted before, cohort studies were not able to provide estimates of effect controlling for important confounders, specifically smoking. The case–control studies reviewed were able to control for confounding by smoking, though not by occupational factors. However, for some studies, information on potential confounders was collected from surrogates, generally next of kin, which may be susceptible to reporting bias and less accurate than information from respondents.
Small excesses of lung cancer as observed in the cohort studies reviewed are often seen in occupational cohorts and may indicate differences in smoking behavior between dry-cleaners (or launderers and dry-cleaners) and the respective reference population. Lack of control for confounding by smoking might have generated or contributed to these results. Additionally, where reported, excesses were found in groups with shorter durations of employment. The excesses observed for women in the case–control studies by Brownson et al. [22], Jahn and colleagues [47], and Pohlabeln and co-workers [76] must be considered against the background of a low prevalence of dry-cleaning occupation in the populations from which controls were drawn, and low response rate for controls in the latter two studies, as well as the limited level of exposure assessment.
Overall, the quality of epidemiological evidence for studies evaluating PCE exposure and lung cancer is limited. Because no strong excesses were observed, and not all studies reviewed had the ability to control adequately for confounding by smoking or other occupational risk factors, the results must be interpreted within the context of the known risk factors for lung cancer. In view of this and the imprecision of exposure assessment in these studies, a strong association between lung cancer and PCE or employment in dry-cleaning shops seems unlikely.
Cervical cancer (ICD-9:180)
Cervical cancers are generally squamous cell carcinomas, though some are adenocarcinomas [37]. Established risk factors for cervical cancer include multiple sex partners, early sexual activity, sexually transmitted diseases (human papilloma viruses (HPVs) in particular) and low socio-economic status (SES). Smoking is considered to be a co-factor for cervical cancer [37].
All five studies with cervical cancer data reported elevated cervical cancer risk estimates, except for Boice et al. [19]. Three of the studies with elevated risk found a borderline-statistically significant association: Blair et al. [16] among dry-cleaners (SMR 1.6, 95% CI 1.0–2.3, 27 cases observed); Andersen and colleagues [2] for launderers and dry-cleaners in the Nordic countries combined (SIR 1.18, 95% CI 1.01–1.38); Ruder et al. [79] for the total cohort of dry-cleaners (SMR 1.95, 95% CI 1.0–3.4), based on ten cases. The study by Anttila et al. produced a moderately elevated risk estimate (SIR 3.2, 95% CI 0.39–11.6) but only two cases were reported [3].
Although the majority of studies reported excess cervical cancer risk, and the results appear to be consistent, there was no adjustment for potential confounders in all the studies reviewed. This lack of control for known risk factors such as HPV, sexual behavior, and SES, provide too great an opportunity for alternative explanations of the results. The mechanism and biological plausibility for a relationship between PCE and cervical cancer are weak, in view of the established risk factors for cervical cancer. Overall, the quality of epidemiological evidence for an association between cervical cancer and PCE is limited, and an association seems unlikely.
There was no evidence of an association for uterine cancer and exposure to PCE or occupation in the dry-cleaning industry.
Urinary system cancers
Bladder cancer (ICD-9:188, 189.3–189.9)
Smoking is a well-established risk factor for bladder cancer, with estimated RRs ranging from 2 to 3 [31, 87]. The main occupations or industries and exposures that have been identified as high risk include rubber and dye manufacturing, the leather industry, painting, truck drivers, aluminum, and aromatic amines [87].
Excess bladder cancer mortality was observed in both the cohort studies of dry-cleaners that were reviewed (Table 6). An excess of bladder cancer was reported by Ruder et al. [79], which was seen in the subgroup of dry-cleaning workers exposed to PCE and other solvents (SMR 3.15, 95% CI 1.51–5.79), for workers with 20 years' latency and who had worked for 5 or more years (SMR 4.31, 95% CI 1.85–8.76) and for non-white male workers (SMR 4.15, 95% CI 1.1–10.6). However, there were no cases of bladder cancer among those union members exposed only to PCE. The small increase in bladder cancer mortality observed in the Blair et al. study [16] was not statistically significant (SMR 1.3, 95% CI 0.7–2.4), nor was the excess related to PCE exposure dose-indicators (little/no vs medium/high). Boice et al. observed no excess risk for aircraft manufacturers routinely exposed to PCE, based on two cases [19]. Andersen et al. reported a slight excess among male, but not among female, laundry and dry-cleaning workers [2].
The case–control studies reviewed collected information on cigarette smoking as a potential confounder. In addition, five of the studies collected information on employment in other high-risk industries and occupations.
All the case–control studies found an excess of bladder cancer; Silverman reported a statistically significant excess (RR 2.8, 95% CI 1.1–7.4), based on 11 exposed cases (non-white, male dry-cleaners) [85]. When analyzed by duration of employment, the results showed that those with fewer than 5 years of employment showed a higher risk (RR 5.3) than those employed more than 5 years (RR 1.8) [85]. Silverman notes in the discussion section that an earlier report from the same study for white men found no excess bladder cancer risk. Pesch et al. [75] reported a significant excess of urothelium cancer among German men in the highest PCE exposure categories ("substantial" exposure: OR 1.4, 95% CI 1.0–1.9; OR 1.8, 95% CI 1.1–3.1; depending on whether job-exposure matrix (JEM) or job–task exposure matrix (JTEM) was used, both based on interview information and expert ranking). It is likely that at least part of the defined PCE-exposed population was also exposed to other agents (which were not controlled for in analysis). The case–control study by Swanson et al. [92] observed an excess of bladder cancer among women who had ever worked in dry-cleaning (OR 2.0, 95% CI 0.7–6.2). The other study that looked specifically at women was the 1990 report from Silverman [86], where a small increase in risk was observed for women who had ever worked in dry-cleaning (RR 1.4, 95% CI 0.8–2.5).
Almost all the studies that were reviewed reported an excess of bladder cancer cases, though few of these risk estimates reached statistical significance. Many of the studies reporting an excess of bladder cancer included both laundry and dry-cleaning workers. The absence of any bladder cancer cases in the Ruder et al. sub-cohort exposed primarily to PCE is inconsistent with the other findings, suggesting that some factor other than PCE had contributed to the excess bladder cancer observed in the full Ruder et al. cohort [79]. The inconsistency in effect by duration of exposure observed in the Silverman study may be due to differential exposures for short-term workers or that other uncontrolled exposures or risk factors for bladder cancer contributed to the slight excesses observed.
The imprecision of exposure measurements and the lack of control for potential confounders, specifically smoking in the cohort studies but also other occupational risk factors, precludes a clear understanding of the relationship between bladder cancer and PCE exposure. The available evidence is inadequate for one to draw a conclusion on the relationship between bladder cancer and PCE.
Renal cancer (ICD-9:189.0–189.2)
Smoking is recognized as a risk factor for renal cancer [64]. Analgesics (specifically phenacetin) have been associated with renal-pelvis tumors and more recently with renal-cell cancer. Obesity has been consistently related to increased risk of renal-cell cancer; however, the mechanism is unclear and the effect is more pronounced among women. Other exposures that have been associated with renal-cell cancer are diet, radiation, coffee, tea, socio-economic status and genetic susceptibility [64], and results are conflicting for many occupational exposures [65, 66].
Only the multi-center case–control study by Mandel et al. [60], of men and women exposed to dry-cleaning solvents, found a statistically significant increased risk for renal-cell or kidney cancer (Table 7). Slightly elevated but not statistically significant risks were found by Ruder et al. in the full cohort and sub-cohorts, by Anttila and colleagues [3] for PCE-exposed employees from different occupations and by Blair and co-workers [16] among those considered to have higher exposure. Ruder's stratified analysis showed no evidence of increased risk with increasing latency or duration of exposure for the total cohort [79]. Six of the eight kidney cancers in the Blair et al. [16] study occurred among black workers. Boice et al. observed fewer cases than expected among workers exposed to PCE [19].
With the exception of the study by Mandel et al. [60], which reported a statistically significant increased risk for men exposed to dry-cleaning solvents (OR 1.4, 95% CI 1.10–1.70) but not for men ever employed as dry-cleaners (OR 0.9, 95% CI 0.30–2.40), all other studies that reported risk estimates by gender [2, 5, 16, 28, 56, 79] showed either a decreased or a slightly increased risk for men. However, exposure in most of these studies was not limited to either dry-cleaners or PCE exposure, and not all these studies controlled for smoking and weight.
Elevated risks for women were statistically significant in one study that presented results by gender. Mandel et al. [60] reported an increased risk for women exposed to dry-cleaning solvents (OR 1.4, 95% CI 1.0–2.7), although results for women employed as dry-cleaners were not reported. Non-significant elevated risks for female dry-cleaners were reported in the case–control study by Asal et al. [5] (OR 2.8, 95% CI 0.80–9.80) in Oklahoma, where the predominant solvent used was Stoddard solvent; in the total cohort by Ruder et al. in the report from 1994 [78] (SMR 2.41, 0.50–7.03; not reported in the 2001 update); and among black but not white women (based on three and two cases, respectively) in the study by Blair et al. [16]. There is some suggestion in the literature [28] that the effects of PCE or other solvents may be different for women than for men, based on body-fat content and renal function among other anatomical and physiological factors. Specifically, Dosemeci et al. [28] suggest that these differences may be the result of a longer "internal" exposure to solvents for women than for men; however, no increased risk was found among women exposed to PCE alone (OR 0.82, 95% CI 0.30–2.10). Additionally, Lynge et al. [56] found no cases of renal-cell cancer among female dry-cleaners in the original Danish cohort of laundry and dry-cleaner workers.
Although smoking and obesity, especially in women, have been consistently related to increased risk of renal-cell cancer, most studies did not control for these variables. When such information was collected, not all results or risk estimates were adjusted for these confounders. For example, the results presented by Delahunt et al. [27], specific to dry-cleaners, are unadjusted for smoking, though smoking-adjusted results for other occupations are discussed.
Except for in one study, the results considered in this critical analysis were not statistically significant. Those of borderline significance need to be considered with caution; the P value, in addition to reflecting biological variability, is also dependent on sample size and the accuracy of exposure assessment. Furthermore, the case definition was not uniform. Some studies evaluated the risk of renal-cell cancer specifically (ICD-9:189.0), while others evaluated the risk of all kidney cancers combined.
In view of the differences in case definition, the limited quality of exposure assessments, small numbers of observed cases, the heterogeneity of the results, and inconsistencies in the available literature, it is not possible for one to draw a definitive conclusion regarding the relationship between PCE and renal-cell (or the broader category of kidney) cancer. It seems unlikely that a strong association exists, as a large effect would likely have been apparent, despite the limitations of the studies reviewed. Conclusions reported in a recent review of the epidemiological literature on renal-cell cancer are consistent with these findings [62].
Other cancer sites
In the process of our review we briefly considered the results for five additional cancer sites. There was no evidence of an association for breast, prostate, skin, or brain cancers and exposure to PCE. For most of these sites a relationship between PCE and the cancer is unlikely, if one considers known risk factors and the current body of literature.
Lymphatic/hematopoietic cancers (ICD-9:200–208)
The etiology of leukemia is generally unknown, as there are a large number of recognized leukemia subtypes [52]. The occupational risk factors most commonly associated with leukemia are benzene and ionizing radiation. Other risk factors include certain medical treatments, some viruses and retroviruses, and smoking, due in part to components of cigarette smoke that include benzene and hydrocarbons [52].
Reported results from the reviewed studies include overall estimates for all lymphatic cancer sites and some site-specific results. The overall results do not suggest a relationship between PCE and lymphatic cancers. Similarly, results for leukemia (ICD-9:204–208) and lymphosarcoma or reticulosarcoma (ICD-9:200) are unconvincing. Reported results for non-Hodgkin's lymphoma (NHL) are not so clear, as five studies reported an excess of NHL. Spirtas et al. [89] reported a significant excess among women only (SMR 9.68, 95% CI 1.17–34.96), based on two cases, and Anttila et al. [3], Boice and co-workers [19], and Andersen et al. [2] all observed non-significant excesses (the excess in Andersen et al. was only among men). Ruder et al. [79] reported a non-significant excess based on seven NHL deaths (SMR 1.39, 95% CI 0.56–2.86). Blair et al. [16] found no association (SMR 0.9, 95% CI 0.5–1.6), on the basis of 12 cases.
Any conclusions regarding lymphatic cancer and PCE exposure need to take into account the specific subtype. The current evidence and study limitations preclude a conclusion from being made with regard to an association between PCE and lymphatic/hematopoietic cancers, and specifically with regard to a PCE-NHL association.
Discussion
Limitations of the available literature
A comprehensive search for, and systematic review of, all available epidemiological literature pertaining to the carcinogenic effects of PCE was conducted. Although the total number of published papers that met the preliminary screening criteria was relatively large (78 papers were identified), only about half of these met the more restrictive criteria that are necessary for a critical assessment. However, even among the papers meeting the criteria, no study could be considered very strong and only a few studies could make a contribution, although limited, to our understanding of the role of PCE exposure as a risk factor for cancer.
A consistent limitation among studies of PCE and cancer was the widespread lack of valid exposure measurements or any other adequate indicators of potential for PCE exposure. The majority of studies evaluated relied on crude surrogates of exposure, allowing the inclusion of a substantial number of persons with no exposure to PCE (e.g., laundry workers) or mixed exposures. While quantitative estimates of exposure may not be necessary to demonstrate the presence of an association between being a member of a working group and a cancer outcome, inaccurate classification of study subjects into "exposed" and "not exposed" categories can have a profound impact on the estimate and lead to erroneous conclusions.
The size of the population studied (or, in case–control studies, the number of cases and controls) is one of the major determinants of whether a study is able to detect and quantify an association. Larger studies generally have greater statistical power to detect an effect if present, and measures of association based on larger numbers are more precisely estimated. Many of the publications available on PCE are limited by small numbers of cases, especially when the results for specific cancer sites are isolated and examined. In addition, the total epidemiological literature concerning PCE and cancer divides fairly finely across discrete cancer sites, resulting in many small bodies of literature with little evidence for any one site.
The number of apparent publications available for critical review is effectively reduced because of overlapping populations studied, or multiple reports, such as mortality updates, on a previously studied cohort. Among sets of related results, the most recent update or the report encompassing one or more study groups was usually selected for review. Although this decision was motivated by the larger numbers of outcomes of interest in more recent updates, it is not clear that advanced studies of occupational cohorts have the greatest sensitivity to detect an effect. If, for example, an effect, noted as an excess of deaths or cases of a specific outcome, occurs on average 10 years following exposure, then follow-up of the cohort over 20 or 30 years may increase the number of deaths but dilute, or even mask, the exposure-related excess. However, without more information such as dates of actual exposure, the most appropriate period of follow-up cannot be assessed.
The specific literature on PCE-exposed occupational cohorts consists of two categories: dry-cleaners and other workers that use various solvents, including PCE. Although misclassification is likely within both categories, it is possible that dry-cleaners in specific regions during certain periods, if exposed, would be exposed to PCE. Within the dry-cleaning industry actual exposure to PCE would depend on the specific equipment that was being operated and the specific job within the shop, and some individuals would have no relevant exposure to PCE. Apart from the actual exposures, other factors likely influence the health and disease patterns of those employed within the industry. For example, in the US, employees in dry-cleaning shops are not paid well, and individuals taking these jobs are often poorly educated and of lower socio-economic status. These individuals plausibly have risk-factor profiles different from those of the general population (or whatever referent groups are used in the studies), increasing the possible influence of confounding. Specific risk factors of concern within this context include cigarette smoking, alcohol consumption, multiple sex partners, and poor diet, all of which are key risk factors for specific cancers. If these factors are not properly assessed concurrently with valid measurements of exposure within a study, then the study is not able to control for their confounding effects (i.e., separate the effects of the confounding factors from those related directly to PCE) and the results may be invalid. Control for effects of socio-economic factors is very difficult and may differ by disease (e.g., cervical cancer and multiple sex partners; respiratory cancers and smoking). Most studies reviewed, however, failed to consider important potential confounding variables, including those related to social class as well as others, possibly compromising the validity of study results.
We considered the use of meta-analytic techniques to calculate a quantitative summary result for specific cancer sites. However, in addition to the limitations already described, without exception, the heterogeneity was too great or the numbers of results too few to justify any quantitative synthesis.
The search process produced what appeared to be a substantial epidemiological literature on the carcinogenicity of PCE; however, after our critical assessment this impression was weakened and the literature provided limited support for scientific conclusions.
Key results of the critical review
While all the epidemiological studies selected for inclusion in our review investigated similar exposure–health outcome relationships, there was a broad diversity of proxy measurements of exposure to PCE, as well as numerous specific cancer outcomes of interest.
For some cancers (e.g., cervical cancer) an uncritical inspection of the published results might suggest that a consistent association exists across studies where no true association exists. However, one's inability to find homogeneity among the results of the cancer-specific literature cannot be interpreted as lack of effect. From our extensive review and efforts to synthesize the results of the relevant studies on each cancer outcome, it appears that the findings are inconsistent, a characteristic found frequently in recent epidemiological literature on cancer [43].
Although some of the published studies make a limited contribution to our understanding of the role of PCE exposure as a risk factor for cancer, none is adequately strong, nor, is the body of evidence convincingly consistent to draw firm conclusions. It appears that there is little support on which to base a conclusion that occupational exposure to PCE is a strong risk factor for cancer of any site. Further, none of the cohort studies with sub-cohorts primarily exposed to PCE demonstrated any results different from the broader cohorts with mixed exposure. This argues against any PCE-specific association. A relationship between PCE and cancer of the following sites was considered unlikely, in part due to potential confounding: oral cavity, liver, pancreas, cervix, and lung. Scientific evidence was inadequate for laryngeal, kidney, esophageal, and bladder cancer.
Nevertheless, because of a number of positive findings suggested from some of these epidemiological studies (e.g., for esophageal cancer), one cannot definitely rule out the possibility that associations between PCE and some cancers exist in humans. With considerable numbers of workers exposed to PCE, a clearer indication of human carcinogenic risk is needed, which can be seen from the current body of literature. More evidence is needed to elucidate associations, if they exist, or to demonstrate with adequate power that they do not exist. Many of the published studies were conducted under existing conditions, which themselves were inherently limiting: contexts in which no exposure measurements were available; populations in which exposure prevalence was low (compounded for rarer conditions); occupational cohorts with mixed exposures, etc.
Priority areas in which additional data are most needed include cancers of the esophagus and bladder. Such studies must improve on the exposure indicators used, have adequate sample sizes (especially adequate numbers of exposed persons with the cancers of interest), and concurrently consider the role of known risk factors for the cancers, especially those that might be correlated with employment in the industry studied or the exposure itself. As additional, clearer epidemiological evidence is produced, it can be factored into the existing body of evidence, and the conclusions regarding PCE and cancer can be reassessed. However, until such additional epidemiological evidence is available, conclusions, and subsequently decisions, must rely on existing knowledge. The current epidemiological evidence does not support a conclusion that occupational exposure to PCE is a risk factor for cancer of any specific site.
References
Anderson KE, Potter JD, Mack TM (1996) Pancreatic Cancer. In: Shottenfeld D, Fraumeni JF (eds) Cancer epidemiology and prevention. Oxford University Press, New York, pp 725–771
Andersen A, Barlow L, Engeland A, Kjaerheim K, Lynge E, Pukkala E (1999) Work-related cancer in the Nordic countries. Scand J Work Environ Health 25 [Suppl 2]:1–116
Anttila A, Pukkala E, Sallmen M, Hernberg S, Hemminki K (1995) Cancer incidence among Finnish workers exposed to halogenated hydrocarbons. J Occup Environ Med 37:797–806
Aronson KJ, Siemiatycki J, Dewar R, Gérin M (1996) Occupational risk factors for prostate cancer: Results from a case–control study in Montréal, Québec, Canada. Am J Epidemiol 143:363–373
Asal NR, Geyer JR, Risser DR, Lee ET, Kadamani S, Cherng N (1988) Risk factors in renal cell carcinoma. II. Medical history, occupation, multivariate analysis, and conclusions. Cancer Detect Prev 13:263–279
Aupérin A, Benhamou S, Ory-Paoletti, C Flamant R (1994) Occupational risk factors for renal cell carcinoma: a case–control study. Occup Environ Med 57:426–428
Austin H, Delzell E, Grufferman S, Levine R, Morrison AS, Stolley PD, et al. (1987) Case–control study of hepatocellular carcinoma, occupation, and chemical exposures. J Occup Med 29:665–669
Austin DF, Reynolds P (1996) Laryngeal cancer. In: Shottenfeld D, Fraumeni JF (eds) Cancer epidemiology and prevention. Oxford University Press, New York, pp 619–636
Band PR, Le ND, Fang R, Deschamps M, Gallagher RP, Yang P (2000) Identification of occupational cancer risks in British Columbia. A population-based case–control study of 995 incident breast cancer cases by menopausal status, controlling for confounding factors. J Occup Environ Med 42:284–310
Blair A, Decoufle P, Grauman D (1979) Causes of death among laundry and dry-cleaning workers. Am J Public Health 69:508–511
Blair A, Tolbert P, Thomas T, Grauman D (1986) Mortality among dry cleaners (abstract). Med Lav 77:82–83
Blair A, Stewart PA, Tolbert PE, Grauman D, Moran FX, Vaught J, et al. (1990) Cancer and other causes of death among a cohort of dry cleaners. Brit J Ind Med 47:162–168
Blair A, Linos A, Stewart PA, Burmeister LF, Gibson R, Everett G, et al. (1992) Comments on occupational and environmental factors in the origin of non-Hodgkin's lymphoma. Cancer Res 52 [Suppl]:5501s–5502s
Blair A, Linos A, Stewart PA, Burmeister LF, Gibson R, Everett G, et al. (1993) Evaluation of risks for non-Hodgkin's lymphoma by occupation and industry exposures from a case–control study. Am J Ind Med 23:301–312
Blair A, Hartge P, Stewart PA, McAdams M, Lubin J (1998) Mortality and cancer incidence of aircraft maintenance workers exposed to trichloroethylene and other organic solvents and chemicals: extended follow up. Occup Environ Med 55:161–171
Blair A, Petralia S, Stewart P (2003) Extended mortality follow-up of a cohort of dry cleaners. Ann Epidemiol 13:50–56
Blot WJ, Fraumeni JF (1996) Cancers of the lung and pleura. In: Shottenfeld D, Fraumeni JF (eds) Cancer epidemiology and prevention. Oxford University Press, New York, pp 637–665
Blot WJ, McLaughlin JK, Devesa SS, Fraumeni JF (1996) Cancers of the oral cavity and pharynx. In: Shottenfeld D, Fraumeni JF (eds) Cancer epidemiology and prevention. Oxford University Press, New York, pp 666–680
Boice JD, Marano DE, Fryzek JP, Sadler CJ, McLaughlin JK (1999) Mortality among aircraft manufacturing workers. Occup Environ Med 56:581–597
Bond GG, McLaren EA, Sabel FL, Bodner KM, Lipps TE, Cook RR (1990) Liver and biliary tract cancer among chemical workers. Am J Ind Med 18:19–24
Brown DP, Kaplan SD (1987) Retrospective cohort mortality study of dry cleaner workers using perchloroethylene. J Occup Med 29:535–541
Brownson R, Alavanja M, Chang J (1993) Occupational risk factors for lung cancer among non-smoking women: a case–control study in Missouri (United States). Cancer Causes Control 4:449–454
Calabrese EJ, Kenyon EM (1991) Air toxics and risk assessment. Lewis, Chelsea, Michigan, USA
Chow W-H, McLaughlin JK, Malker HSR, Linet MS, Weiner JA, Stone BJ (1995) Esophageal cancer and occupation in a cohort of Swedish men. Am J Ind Med 27:749–757
Clavel J, Mandereau L, Cordier S, Le Goaster C, Hémon D, Conso F, et al. (1995) Hairy cell leukaemia, occupation, and smoking. Br J Haematol 91:154–161
Clavel J, Mandereau L, Conso F, Limasset J-C, Pourmier I, Flandrin G, et al. (1998) Occupational exposure to solvents and hairy cell leukaemia. Occup Environ Med 55:59–64
Delahunt B, Bethwaite PB, Nacey JN (1995) Occupational risk for renal cell carcinoma. A case–control study based on the New Zealand cancer registry. Br J Urol 75:578–582
Dosemeci M, Cocco P, Chow W-H (1999) Gender differences in risk of renal cell carcinoma and occupational exposures to chlorinated aliphatic hydrocarbons. Am J Ind Med 36:54–59
Døssing M, Petersen KT, Vyberg M Olsen JH (1997) Liver cancer among employees in Denmark. Am J Ind Med 32:248–254
Ellis FH, Levitan N, Lo TCM (1991) Cancer of the esophagus. In: Holleb AI, Fink DJ, Murphy GP (eds) American Cancer Society textbook of clinical oncology. American Cancer Society, Atlanta, Georgia, USA, pp 254–262
Ernster VL, Cummings SR (1991) Smoking and cancer. In: Holleb AI, Fink DJ, Murphy GP (eds) American Cancer Society textbook of clinical oncology. American Cancer Society, Atlanta, Georgia, USA, pp 107–124
Fredriksson M, Bengtsson N-O, Hardell L Axelson O (1989) Colon cancer, physical activity, and occupational exposures. Cancer 63:1838–1842
Gallagher RP, Bajdik CD, Fincham S, Hill GB, Keefe AR, Coldman A, et al. (1996) Chemical exposures, medical history, and risk of squamous and basal cell carcinoma of the skin. Cancer Epidemiol Biomarkers Prev 5:419–424
Goldberg P, Leclerc A, Luce D, Morcet J-F, Brugère J (1997) Laryngeal and hypopharyngeal cancer and occupation: results of a case–control study. Occup Environ Med 54:477–482
Greenland S, Salvan A, Wegman DH, Hallock MF Smith TJ (1994) A case–control study of cancer mortality at a transformer-assembly facility. Int Arch Occup Environ Health 66:49–54
Guralnick L (1963) Mortality by occupation and cause of death among men 20 to 64 years of age: United States, 1950. Vital Statistics—Special Reports 53:95–97, 100, 103, 226–228
Gusberg SB, Runowicz CD (1991) Gynecologic cancers. In: Holleb AI, Fink DJ, Murphy GP (eds) American Cancer Society textbook of clinical oncology. American Cancer Society, Atlanta, Georgia, USA, pp 481–497
Hardell L, Eriksson M, Lenner P, Lundgren E (1981) Malignant lymphoma and exposure to chemicals, especially organic solvents, chlorophenols and phenoxy acids: a case–control study. Br J Cancer 43:169–176
Hardell L, Bengtsson NO, Honsson U, Eriksson S, Larsson LG (1984) Aetiological aspects on primary liver cancer with special regard to alcohol, organic solvents and acute intermittent porphyria—an epidemiological investigation. Br J Cancer 50:389–397
Harrington JM, Whitby H, Gray CN, Reid FJ, Aw TC, Waterhouse JA (1989) Renal disease and occupational exposure to organic solvents: a case referent approach. Br J Ind Med 46:643–650
Heineman EF, Cocco P, Gomez MR, Dosemeci M, Stewart PA, Hayes RB, et al. (1994) Occupational exposure to chlorinated aliphatic hydrocarbons and risk of astrocytic brain cancer. Am J Ind Med 26:155–169
Hernberg S, Korkala ML, Asikainen U, Riala R (1984) Primary liver cancer and exposure to solvents. Int Arch Occup Environ Health 54:147–153
Hernberg S (1998) Inconclusive cancer epidemiology. Scand J Work Environ Health 24:161–164
Hernberg S, Kauppinen T, Riala R, Korkala M-L, Asikainen U (1988) Increased risk for primary liver cancer among women exposed to solvents. Scand J Work Environ Health 14:356–365
Huebner WW, Schoenberg JB, Kelsey JL, Wilcox HB, McLaughlin JK, Greenberg RS, et al. (1992) Oral and pharyngeal cancer and occupation: a case–control study. Epidemiology 3:300–309
International Agency for Research on Cancer (1995) IARC monographs on the evaluation of carcinogenic risks to humans. Dry cleaning, some chlorinated solvents and other industrial chemicals. IARC Press, Lyon, France
Jahn I, Ahrens W, Bruske-Hohlfeld I, Kreuzer M, Mohner M, Pohlabeln H, et al. (1999) Occupational risk factors for lung cancer in women: results of a case–control study in Germany. Am J Ind Med 36:90–100
Kaerlev L, Teglbjaerg PS, Sabroe S, Kolstad HA, Ahrens W, Eriksson M, et al. (2000) Occupation and small bowel adenocarcinoma: a European case–control study. Occup Environ Med 57:760–766
Kaplan SD (1980) Dry cleaner workers exposed to perchloroethylene—a retrospective cohort mortality study (PB81-231367). National Technical Information Service, Springfield, Virginia, USA
Kreuzer M, Pohlabeln H, Ahrens W, Kreienbrock L, Bruske-Hohlfeld I, Jockel KH (1999) Occupational risk factors for lung cancer among young men. Scand J Work Environ Health 25:422–429
Lin RS, Kessler II (1981) A multifactorial model for pancreatic cancer in man. JAMA 245:147–152
Linet M, Cartwright R (1996) The leukemias. In: Shottenfeld D, Fraumeni JF (eds) Cancer epidemiology and prevention. Oxford University Press, New York, pp 841–892
London W, McGlynn K (1996) Liver cancer. In: Shottenfeld D, Fraumeni JF (eds) Cancer epidemiology and prevention. Oxford University Press, New York, pp 772–793
Lynge E (1994) Danish cancer registry as a resource for occupational research. J Occup Med 36:1169–1173
Lynge E, Thygesen L (1990) Primary liver cancer among women in laundry and dry-cleaning work in Denmark. Scand J Work Environ Health 16:108–112
Lynge E, Cartensen B, Andersen O (1995) Primary liver cancer and renal cell carcinoma in laundry and dry-cleaning workers in Denmark. Scand J Work Environ Health 21:293–295
Mabuchi K, Bross DS, Kessler II (1985) Epidemiology of cancer of the vulva. Cancer 55:1843–1848
Mack TM, Peters JM, Yu MC, Hanisch R, Wright WE, Henderson BE (1985) Pancreas cancer is unrelated to the workplace in Los Angeles. Am J Ind Med 7:253–266
Malker HSR, Weiner JA (1984) Cancer environment register. Examples of use of register-based epidemiology in occupational health (in Swedish). Arbete Hälsa 9:1–107
Mandel JS, McLaughlin JK, Schlehofer B, Mellemgaard A, Helmert U, Lindblad P, et al. (1995) International renal-cell cancer study. IV. Occupation. Int J Cancer 61:601–605
McCredie M, Stewart JH (1993) Risk factors for kidney cancer in New South Wales. IV. Occupation. Br J Ind Med 50:349–354
McLaughlin JK, Lipworth L (2000) Epidemiologic aspects of renal cell cancer. Semin Oncol 27:115–123
McLaughlin JK, Malker HSR, Stone BJ, Weiner JA, Malker BK, Ericsson JLE, et al. (1987) Occupational risks for renal cancer in Sweden. Br J Ind Med 44:119–123
McLaughlin JK, Malker HSR, Malker BK, Stone BJ, Ericcson JLE, Blot WJ, et al. (1987) Registry-based analysis of occupational risks for primary liver cancer in Sweden. Cancer Res 47:287–291
McLaughlin J, Blot W, Devesa S, Fraumeni JF (1996) Renal cancer. In: Shottenfeld D, Fraumeni JF (eds) Cancer epidemiology and prevention. Oxford University Press, New York, pp 1142–1155
Mellemgaard A, Engholm G, McLaughlin JK, Olsen JH (1994) Occupational risk factors for renal-cell carcinoma in Denmark. Scand J Work Environ Health 20:160–165
Miligi L, Costantini AS, Crosignani P, Fontana A, Masala G, Nanni O, et al. (1999) Occupational, environmental, and life-style factors associated with the risk of hematolymphopoietic malignancies in women. Am J Ind Med 36:60–69
Morton W, Marjanovic D (1984) Leukemia incidence by occupation in the Portland–Vancouver metropolitan area. Am J Ind Med 6:185–205
Muñoz N, Day N (1996) Esophageal cancer. In: Shottenfeld D, Fraumeni JF (eds) Cancer epidemiology and prevention. Oxford University Press, New York, pp 681–706
Muscat JE, Stellman SD, Richie JP, Jr., Wynder EL (1998) Lung cancer risk and workplace exposures in black men and women. Environ Res 76:78–84
Olsen GW, Hearn S, Cook RR, Currier MF, Allen S (1989) Mortality experience of a cohort of Louisiana chemical workers. J Occup Med 31:32–34
Parent ME, Siemiatycki J, Fritschi L (2000) Workplace exposures and oesophageal cancer. Occup Environ Med 57:325–334
Parent ME, Hua Y Siemiatycki J (2000) Occupational risk factors for renal cell carcinoma in Montreal. Am J Ind Med 38:609–618
Partanen T, Heikkilä P, Hernberg S, Kauppinen T, Moneta G, Ojajärvi A (1991) Renal cell cancer and occupational exposure to chemical agents. Scand J Work Environ Health 17:231–239
Pesch B, Haerting J, Ranft U, Klimpel A, Oelschlagel B, Schill W (2000) Occupational risk factors for urothelial carcinoma: agent-specific results from a case–control study in Germany. MURC Study Group. Multicenter Urothelial and Renal Cancer. Int J Epidemiol 29:238–247
Pohlabeln H, Boffetta P, Ahrens W, Merletti F, Agudo A, Benhamou E, et al. (2000) Occupational risks for lung cancer among nonsmokers. Epidemiology 11:532–538
Pukkala E (1995) Cancer risk by social class and occupation. A survey of 109,000 cancer cases among Finns of working age. In: Wahrendorf J (ed) Contributions to epidemiology and biostatistics. Karger, pp 62–77
Ruder AM, Ward EM, Brown DP (1994) Cancer mortality in female and male dry-cleaning workers. J Occup Med 36:867–874
Ruder AM, Ward EM, Brown DP (2001) Mortality in dry-cleaning workers: an update. Am J Ind Med 39:121–132
Schlehofer B, Heuer C, Blettner M, Niehoff D, Wahrendorf J (1995) Occupation, smoking and demographic factors, and renal cell carcinoma in Germany. Int J Epidemiol 24:51–57
Schoenberg JB, Stemhagen A, Moglelnicki AP, Altman R, Abe T, Mason T (1984) Case–control study of bladder cancer in New Jersey. I. Occupational exposures in white males. J Natl Cancer Inst 72:973–981
Sharpe CR, Rochon JE, Adam JM, Suissa S (1989) Case–control study of hydrocarbon exposures in patients with renal cell carcinoma. CMAJ 140:1309–1318
Siemiatycki J (1991) Risk factors for cancer in the workplace. CRC Press, Boca Raton, Florida, USA
Silverman DT, Hoover RN, Albert S, Graff KM (1983) Occupation and cancer of the lower urinary tract in Detroit. J Natl Cancer Inst 70:237–245
Silverman DT, Levin LI, Hoover RN (1989) Occupational risks of bladder cancer in the United States: II. Nonwhite men. J Natl Cancer Inst 81:1480–1483
Silverman DT, Levin LI, Hoover RN (1990) Occupational risks of bladder cancer among white women in the United States. Am J Epidemiol 132:453–461
Silverman DT, Morrison AS, Devesa S (1996) Bladder cancer. In: Shottenfeld D, Fraumeni JF (eds) Cancer epidemiology and prevention. Oxford University Press, New York, pp 1156–1179
Smith EM, Miller ER, Woolson RF, Brown CK (1985) Bladder cancer risk among laundry workers, dry-cleaners, and other chemically related occupations. J Occup Med 27:295–297
Spirtas R, A SP, S LJ, et al. (1991) Retrospective cohort mortality study of workers at an aircraft maintenance facility. I Epidemiological results. Br J Ind Med 48:515–530
Stemhagen A, Slade J, Altman R, Bill J (1983) Occupational risk factors and liver cancer. A retrospective case–control study of primary liver cancer in New Jersey. Am J Epidemiol 117:443–454
Stewart PA, Lee JS, Marano DE, Spirtas R, Forbes CD, Blair A (1991) Retrospective cohort mortality study of workers at an aircraft maintenance facility. II. Exposures and their assessment. Br J Ind Med 48:531–537
Swanson GM, Brissette Burns P (1995) Cancer incidence among women in the workplace: a study of the association between occupation and industry and 11 cancer sites. J Occup Environ Med 37:282–287
Teschke K, Morgan MS, Checkoway H, Franklin G, Spinelli JJ, van Belle G, et al. (1997) Surveillance of nasal and bladder cancer to locate sources of exposure to occupational carcinogens. Occup Environ Med 54:443–451
US Environmental Protection Agency (1998) Cleaner technologies substitutes assessment: Professional fabric care processes. Environmental Protection Agency, Washington, DC, USA
US Department of Health and Human Services (1997) ATSDR's toxicological profiles (book or CD-ROM). Lewis, CRC Press, Boca Raton, Florida, USA
Vamvakas S, Bruning T, Thomasson B, Lammert M, Baumuller A, Bolt HM, et al. (1998) Renal cell cancer correlated with occupational exposure to trichloroethene. J Cancer Res Clin Oncol 124:374–382
Vasama-Neuvonen K, Pukkala E, Paakkulainen H, Mutanen P, Weiderpass E, Boffetta P, et al. (1999) Ovarian cancer and occupational exposures in Finland. Am J Ind Med 36:83–89
Vaughan TL, Stewart PA, Davis S, Thomas DB (1997) Work in dry cleaning and the incidence of cancer of the oral cavity, larynx, and oesophagus. Occup Environ Med 54:692–695
Acknowledgements
This review was funded by the Halogenated Solvents Industry Alliance (HSIA), Washington, D.C., USA, and was partly based on an earlier report sponsored by the Arbeitsgemeinschaft der Metall-Berufsgenossenschaften, the Arbeitsgemeinschaft der Berufsgenossenschaften der Bauwirtschaft, the Berufsgenossenschaft der Strassen-, U-Bahnen und Eisenbahnen, the Berufsgenossenschaft der Feinmechanik und Elektrotechnik, the Forschung Textilreinigung e.V. and the Textil–und Bekleidungs-Berufsgenossenschaft (all part of the German workers' compensation insurance system). The authors wish to acknowledge Drs. Frank Bochmann, Margaret McDonald, Carol Bigelow, and Diane Mundt who provided assistance with earlier drafts of the review. We also recognize Mr. Louis Bloemen and Drs. Paul Dugard, John Tomenson, and other anonymous HSIA reviewers of the draft manuscript for their thoughtful comments and questions.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mundt, K.A., Birk, T. & Burch, M.T. Critical review of the epidemiological literature on occupational exposure to perchloroethylene and cancer. Int Arch Occup Environ Health 76, 473–491 (2003). https://doi.org/10.1007/s00420-003-0457-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-003-0457-2