
Abstract
Objectives
The neurotoxicity of occupational exposure to aluminium (Al)-containing welding fumes has been discussed with controversial results. The aim of the longitudinal study was to examine a group of Al welders for significant central nervous changes in comparison with a non-exposed cohort.
Methods
A group of 98 Al welders (mean age 37 years) in the car-body construction industry, with a median of 6 years of occupational exposure to Al welding fumes, and an education-matched, gender-matched, age-matched control group of 50 car-production workers (mean age 36 years) at the same plant, were included in this longitudinal study. Two cross-sectional studies were done in 1999 and 2001. In the second cross-sectional study 97 welders and 50 controls could be examined. The examination programme consisted, for example, of a standardised anamnesis, focussing on occupational history, education, illnesses, medication, accidents and current alcohol consumption, a physical examination that included neurological status, and the assessment of Al concentration in plasma and urine. The neurobehavioral methods included a symptom questionnaire, modified Q16, and computerised and non-computerised tests: psychomotor performance (steadiness, line tracing, aiming, tapping), verbal intelligence (WST), simple reaction time, digit span, block design (HAWIE), symbol–digit substitution, digit span, switching attention (European neurobehavioral evaluation system, EURO-NES), and standard progressive matrices. The data were analysed by multivariate analysis of covariance (MANCOVA) for repeated measurements with covariates age, education, and carbohydrate-deficient transferrin in plasma (CDT).
Results
The median Al urine concentration (mean preshift/postshift) was 52.4 μg/g creatinine (2001) and 57.6 μg/g creatinine (1999). Median respirable air dust was 0.67 mg/m3 (2001) and 0.47 mg/m3 (1999). Welders and controls did not report significantly more symptoms in the modified Q16. Furthermore, no significant differences in psychomotor performance and other neurobehavioral tasks, except for reaction time, were seen between welders and non-welders. Regression analyses reveal a significant relationship between reaction time and Al excretion in urine that was confounded by other factors.
Conclusions
At present the outcome for reaction time has to be interpreted as a single result. However, as the modified Q16 questionnaire and the rest of the psychomotor performance showed no significant changes, the next cross-sectional study, in 2003, will provide further information on which a final conclusion can be based.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Aluminium (Al) is abundantly present in our environment and constitutes approximately 8.1% of the earth's crust. Due to its affinity with oxygen Al is found only as compounds. Uptake is most likely in our environment, as Al is present, for example, in drinking water, food and pharmaceuticals. Occupationally, Al can be found in various industries, e.g. the Al-powder industry, the metal industry and in Al foundries.
Al is primarily absorbed from the air via the lungs at the workplace. Ingestion is possible, but according to current scientific knowledge, the inhalation route dominates. Parenteral uptake occurs when medication is administered intravenously. Absorbed Al precipitates in the whole organism and is excreted only by the kidneys. It is not known whether Al can pass the haemato-encephalic barrier. Data on the Al half-times of occupationally exposed persons varies widely in the literature, from days to months, depending on the duration of the exposure. Certainly, the bioavailability of different types of Al has to be considered (Letzel et al. 1999). In non-exposed persons Al levels are <25 μg/l in urine and <10 μg/l in plasma.
The first studies on neurotoxic effects of Al exposure in humans were carried out on patients who had died of dialysis-related encephalopathy. Alfrey et al. (1976) found, for example, elevated levels of Al in the brains of patients that had died of dialysis-related encephalopathy. Other studies in the 1990s associated Al levels in the brain with Alzheimer's disease (AD); however, no conclusive evidence has yet been found that Al contributes to the development of AD (Armstrong et al. 1996; Doll 1993; Savory et al. 1996).
Only few epidemiological studies were conducted on workers occupationally exposed to Al. In Canadian miners who used McIntyre powder by inhalation as prophylaxis against silicosis, Rifat et al. (1990) found a weaker performance in cognitive tests than in the controls. Hosovski et al. (1990) found deficits in performance of foundry workers.
Sjörgen et al. (1996) reported higher frequencies of neurological symptoms in Al welders than in other welders.
Hänninen et al. (1994) and Akila et al. (1999) reported effects on the cognitive function of Al welders. Sjörgen et al. (1996) showed a poorer performance by Al welders than stainless steel welders on four different tests of motor functions. Bast-Pettersen et al. (2000) demonstrated effects on hand tremor and a reduced reaction time in 20 long-term exposed Al welders. Iregren et al. (2001) studied effects on the nervous system in a group of potroom and foundry workers, Al welders and a small group of flake-powder production workers. In the potroom and foundry workers no effects on the nervous system related to Al exposure were detected, whereas the welders, who had been exposed to high levels of Al, showed a reduced performance, though not significant, in four tests of motor function and one pegboard test. However, in the highly exposed flake-powder production workers, no effect on the central nervous system was seen. Letzel et al. (2000) showed no measurable cognitive decline in 32 dust-exposed workers in a German Al-powder plant.
Altogether, occupational exposure to Al seems to have different effects on workers in different industries. The measurable effects on the central nervous system might only develop after a protracted exposure, and the intellectual domain, mainly affected, varies. The following study presents neurobehavioral and exposure data of a cohort of Al welders in comparison with non-exposed controls across the first two examinations of a longitudinal study.
Materials and methods
Study design
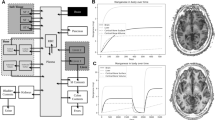
The design of the longitudinal study comprises three cross-sectional studies (e.g. with three neurobehavioral and three Al-exposure examinations of two cohorts, Al welders and controls). The presented data result from the first two examinations carried out with an interval of 2 years (Fig. 1).

Design of the longitudinal study
All human studies were reviewed by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in an appropriate version of the 1964 Declaration of Helsinki. All persons gave their informed consent prior to their inclusion in the study. Details that might disclose the identity of the subjects have been omitted. Essential results have not been and will not be published elsewhere.
Groups
The two cohorts comprise employees of a car manufacturer. In the first examination 98 male Al welders and a demographically similar control group of 50 non-exposed car-production workers from the same plant were investigated. In exposed employees the median exposure to welding fumes was 6 years (mean 4.7). Ninety-seven exposed and 50 non-exposed employees of these cohorts (identical individuals, participation rate: 99% for welders, 100% for controls) were examined again in the second examination. The inclusion criterion was an Al-welding time of at least 2 years. Exclusion criteria were neurological diseases not due to the exposure, cerebrovascular diseases, diabetes, head injuries, insufficient knowledge of the German language and exposure to neurotoxic solvents. Table 1 shows that exposed workers and controls with repeated measurements are similar in age, level of education (four categories: 0–3, 0 = low level), and level of carbohydrate-deficient transferrin in plasma (CDT), which was used as a biomarker of alcohol consumption. For temporal reasons some tests could not be performed with the whole control group at examination 2. In these cases the control sample is reduced to 38 subjects. However, the reduced control group shows values that are nearly identical to the total control group in demographic parameters, with no significant differences from the exposed group. The study participants were three-shift workers (morning, afternoon and night shift) and were examined during the day shift between 0800 and 1300 h only if they had worked on the morning or afternoon shift the week before, in order for us to prevent undue fatigue at testing in either group.
Of the welders and controls, 83.7% and 84.0%, respectively, were German by nationality; 61% of the subjects had German as their mother tongue, which is a precondition for the administration of a German verbal intelligence test.
Exposure assessment
Exposure was measured by plasma and urinary Al concentrations in pre-shift and post-shift samples and by personal air sampling at selected work places. The monitoring was done 3 months in advance of the neurobehavioral testing. Furthermore, a questionnaire aimed at working conditions, working hours, and individual free-time exposure, was applied.
The quantitative determination of Al in serum and urine samples was carried out by graphite furnace-atomic absorption spectrometry. For calibration the standard addition technique was used. The determinations were performed under a strict internal and external quality assessment scheme (Lehnert et al. (1999).
Medical examination
The examination programme consisted of a standardised anamnesis that focused on occupational history, education, illnesses, medication, accidents, current alcohol consumption and a physical examination that included neurological status.
Neurobehavioral methods
We used neurobehavioral methods to evaluate the level of neurotoxic symptoms, pre-morbid intelligence, and deficits in the domains of motor performance, logical thinking, short-term and working memory, perceptual speed, and switching attention.
Psychomotor performance tests, simple reaction (time) test and the European neurobehavioral evaluation system (EURO-NES) were administered by computer. All other tests were non-computerised. Most neurobehavioral examinations were performed repeatedly in examinations 1 and 2: symptom questionnaire, psychomotor performance test battery, simple reaction-time test, recall of digits, block design test, and trail making. The standard progressive matrices test was performed at examination 1 only. The EURO-NES and the test of verbal intelligence were introduced at examination 2 for the first time.
Q16
A German version of the well-known Swedish questionnaire Q16 (Hogstedt et al. 1984) was used. Three questions were modified and two were added to improve the sensitivity of the questionnaire (Ihrig et al. 2001). The added questions were related to signs of peripheral neuropathy. The questionnaire is designed for the screening of workers for psychological and neuropsychological symptoms of neurotoxic exposure.
Verbal intelligence
We administered a German multiple-choice vocabulary test (WST, Schmidt and Metzler 1992) to estimate pre-morbid intelligence. It could only be used for workers with the German mother tongue.
Psychomotor performance
Manual-dexterity functions of all participants were examined by a computerised test battery for motor performance (MLS). We used the five sub-tests 'steadiness', 'line tracing', 'aiming', 'tapping', and 'peg board' to screen for static and dynamic changes in psychomotor performance of the upper limbs. Precision and speed were measured for the dominant and non-dominant hand.
Simple reaction time
Simple reaction time is part of the motor performance test system (MLS). The subject had to respond with a quick movement from a home key to a target key whenever a yellow dot appeared on the screen. Reaction time, motoric time and errors were recorded.
Recall of digits
Recall of digits is part of the Hamburg Wechsler Intelligence Scale for Adults (German HAWIE). In this short-term-memory test the subject had to recall series of increasing length. The maximum achievable points were 14 (2×7 series of different lengths) for forward recall as well as for backward recall.
Block design
The block design test is also part of the HAWIE. The subject had to arrange nine different geometric patterns with 12 cubes at maximum speed. The scores consider the combination of accuracy and speed. A maximum total score of 42 could be achieved (Thomas and Dahl 1969).
Standard progressive matrices
The standard progressive matrices test (SPM, Raven) was administered as a German version (Heller et al. 1998). The task requires the subject to recognise the rules of an incomplete matrix of signs and to fill in the missing sign. It is a test of inductive thinking and general intelligence independent of speech. The test score indicates the number of correct solutions of 60 matrices.
Trail-making test
The German form of the trail-making test (TMT; Zahlenverbindungstest, ZVT, Oswald and Roth (1997) consists of connecting numbers from 1 to 90 in four series. The series are presented on four sheets of paper in different random distributions. Scores represent the time it takes in average for the subject to complete one series and the mean number of errors.
EURO-NES
The EURO-NES (e.g. Gilioli 1993) comprises elements from the neurobehavioral evaluation system (NES), Letz et al. 1996) and the Swedish performance evaluation system (SPES), Iregren et al. 1996). The following three tests were administered:
-
Symbol–digit substitution. The test measures perceptual speed, working memory, motor planning and speed. The task asks the subject to perceive a combination of symbols and digits and to complete a new scheme of symbols with the corresponding digits.
-
Digit span. The test measures short-term memory. It is adaptive in difficulty and requires the reproduction of digit sequences of increasing lengths displayed on the screen via keyboard. In the first part the sequences have to be reproduced forward, in the second part, backward.
-
Switching attention. The test measures the response speed and the switching of attention toward different features of a complex design. The sign varies in complexity and is displayed on varying sides of the screen compatible or incompatible with the response keys. The test consists of three parts of increasing difficulty for which reaction time and error measures were obtained.
Statistical analyses
The data were generally analysed by multivariate analyses of covariance (MANCOVA) for repeated measurements. Factors enclosed in the model for multivariate analyses were Al exposure (welders vs controls), examination (second measurement as repetition factor) and the covariates age, education and CDT. The repeated-measurements model allows one to test the hypothesis of whether exposed subjects and controls differ in changes from examination 1 to 2 (interaction term: exposure × examination).
We used stepwise multiple linear regression analyses to assess the statistical relationships between Al exposure (Al urine, Al plasma, years exposed) and potential confounders (e.g. age, education, CDT) as independent variables, and neurobehavioral performance as dependent variable. For these analyses individual pre-shift and post-shift measurements of Al in urine and plasma were averaged.
The variance analyses for exposed workers and controls were repeated for the subgroups for which verbal intelligence data as covariate were available. Results of these subgroup analyses are not shown because there was no difference from the results of the total sample.
Results
Biomonitoring and ambient monitoring
Table 2 shows a reduction in Al exposure on a group basis in the welders' median concentration of Al in plasma (Al-P) and in urine from examination 1 in 1999 to examination 2 in 2001. Plasma levels decreased from 10.3 μg/l (1999) to 4.3 μg/l (2001) (Al-P pre-shift) and from 8.3 to 4.1 μg/l (2001) (Al-P post-shift). One person exceeded the German BAT value of 200 μg/l for urinary Al. However, respirable-dust exposure increased from a median 0.47 mg/m3 (1999) to 0.67 mg/m3 (2001). This reflects the results of improved instructions on how individuals should use personal protection items.
Q16 symptoms
The mean number of reported neurobehavioral symptoms (Table 3) was small, approximately two symptoms in exposed subjects and controls. No significant difference between both cohorts could be observed (Table 4) with regard to Q16 symptoms. A detail analysis of the number of subjects reporting more than five symptoms, a critical level, did not reveal significant differences between welders and controls.
Psychomotor performance
The data from the motor-performance tests are presented in Table 3 for the dominant and non-dominant hand. The differences between exposed workers and controls are small, and both cohorts show only minor changes from examination 1 to examination 2. For each performance task the speed data were tested, together with the accuracy data for both hands, in one model, by MANCOVA for repeated measurements, with age, education and CDT as covariates (Table 4). The psychomotor performance of exposed and non-exposed workers improved to a comparable extent, from examination 1 to examination 2, in all variables. With the exception of steadiness—in this case one can only suppose an unknown change in the system or procedure—the changes are small. Neither for steadiness nor for line tracing, aiming, and tapping was a significant difference between both cohorts detected. Furthermore, there is no significant trend difference between exposed subjects and controls from examination 1 to examination 2 (interaction term: examination × exposure). However, the covariates show significant relationships with the motor-performance outcomes. CDT is related to line tracing (explained variance 8.0%), and age to aiming (explained variance 12.2%).
Simple reaction time
The MANCOVA of performance in the simple reaction-time task included reaction time (decision time) and motoric movement time in one model. Exposed workers and controls differed significantly in the reaction-time performance (P=0.017, eta2 =0.062) (Tables 3 and 4). Of the covariates, only age (P=0.001, eta2 = 0.11) is related to this performance measure. The trend from examination 1 to examination 2 shows no significant difference between exposed subjects and controls (interaction: examination × exposure, P=0.799; Table 4).
Univariate covariance analysis reveals that the difference between exposed workers and controls in multivariate analysis goes back to differences in reaction time and not in motoric movement time. Figure 2 shows the significant difference in reaction time and Fig. 3 the insignificant difference in motoric time. Figure 2 reveals a small but insignificant increase in the reaction-time difference between both groups from examination 1 to examination 2. However, both groups improved in the motoric time from examination 1 to examination 2, possibly reflecting a learning trend.

Adjusted mean reaction time of exposed workers and controls (adjustment: age, education, CDT)

Adjusted mean motoric time of exposed workers and controls (adjustment: age, education, CDT)
Because of the significance of the exposure variable in simple reaction time, further in-detail analyses on dose–response relationships were performed separately for examination 1 and examination 2. The stepwise multiple linear regression analyses included, as the dependent variable, reaction time and, as predictor variables, Al in plasma, Al concentration in urine, Al concentration in urine referred to creatinine, and years of Al exposure, as well as age, CDT and education. Analyses were performed for the exposed group as well as for the total sample; in the latter case years of exposure were fixed at zero for the control subjects. For the total group the models predicting reaction time included age and the mean Al concentration in urine. The explained variance was, in the first examination, 9% (total R2 =0.090; age: R2 =0.047, Al concentration in urine: R2 =0.043) and, in the second examination, 15% (total R2 =0.150; age: R2 =0.099, Al concentration urine: R2 =0.051). Similar models could be obtained with the urine Al concentration per creatinine, because this variable is highly correlated with Al concentration in urine.
Both urine biomarkers showed significant correlations, with the plasma Al biomarkers, between r =0.83 and r =0.15, varying across the two examinations and the samples (total sample, exposed subjects only). However, only the Al urine markers and never the Al plasma markers were significantly correlated with reaction time. Another feature of the urine markers when compared with the plasma markers is that they revealed a stronger relationship with the duration of Al-welding exposure, between r =0.22 and r =0.69 within the total sample, and between r =0.15 and r =0.25 within the exposed workers. Duration of exposure itself was also positively related to reaction time, but if this relationship is controlled for age it becomes insignificant. Furthermore, if we take a one-sided view of the multiple regression models within the exposed group, only age is a significant predictor of reaction time, explaining between 5 and 15% of variance. Compared with the approach with the total group, Al concentration in urine and duration of exposure are no more relevant in the model.
Cognitive performance
Non-computerised tests
The subgroups of exposed and control subjects with German native language were investigated in the second examination with a multiple-choice vocabulary test, an estimate of verbal IQ. The subgroups of exposed subjects and controls did not differ significantly (Table 6) and revealed the same average IQ of approximately 100 (Table 5). The SPM test, a test of logical reasoning and general intelligence, was performed in the first examination with the total samples of exposed and control subjects and led to approximately the same mean values and variances for both groups (Table 5) and, correspondingly, to non-significant statistical results for the group differences (Table 6).
The vocabulary test shows a stronger relationship to education (eta2 =0.08) than the SPM test (eta2 =0.03, Table 6). Because it was not possible for us to use the vocabulary results as covariate for the total group, we used education as covariate to control for intellectual differences. Block design, like SPM a measure of so-called fluent intelligence, did not reveal a general performance difference between exposed and non-exposed subjects (Tables 5, 6). However, the performance increase from examination 1 to examination 2 is stronger in the exposed group, reflected in the significant interaction examination × exposure (P=0.012) (Table 6).
For the trail-making performance we used multivariate analysis to control for possible trade-off effects between accuracy (errors) and speed (time). The performance increased from examination 1 to examination 2 and showed a clear influence of age (eta2 =0.08), a small but significant influence of CDT, but no influence of exposure (Table 6).
Digit span was investigated with a verbal form (HAWIE) and a computerized (EURO-NES, examination two only) form. The performance in the verbal task, forward and backward, were analysed together by multivariate analysis and increased across the examinations significantly (P=0.000, eta2 =0.21) (Table 6). In addition, age, but not exposure, influenced short-term-memory performance.
EURO-NES
The EURO-NES test was used in examination 2 the first time and will be repeated in the last examination of the longitudinal study. The digit-span test in EURO-NES investigates, in a sophisticated adaptive way, the maximum short-term-memory performance of the subject. Exposed subjects and controls could remember, on average, six numbers forward and five numbers backward (Table 5). Symbol–digit substitution contains a strong working-memory component and was, therefore, analysed together with digit–span forward and backward by multivariate analysis. This analysis revealed that exposure did not lead to differences in the domain of short-term-memory performance. Age explained a substantial part of variance, 29%, and CDT 7% (Table 6).
The switching-attention test of the EURO-NES was analysed by multivariate analysis for the three parts of the test, including both reaction time and errors. The analysis did not show exposure effects but did show strong age effects (eta2 =0.26) (Table 6).
Discussion
With regard to comparability the two cohorts were similar for age and educational background. There were no self-reported head injuries in either cohort. Also, both cohorts had worked the morning or afternoon shift the week before the examination took place, so that we could exclude bias due to fatigue among the referents. The similarity of the background variables indicated the suitability of the control cohort.
The median urinary Al concentration of the welders in our study was 57.6 μg/l (1999) vs 52.4 μg/l (2001), which was between the levels reported by other studies on Al welders. The exposed workers in our study had welded for over 6 years (median).
Bast-Pettersen et al. (2000) reported a median urinary Al concentration of 40.5 μg/l in 20 Al welders aged 21–52 years with an average exposure time of 8.1 years. Iregren et al. (2001) reported a median urinary Al concentration of 22.0 μg/l in 38 Al welders aged 26–56 years and an average exposure time of 15 years. Hänninen et al. (1994) reported a median urinary Al concentration of 65 μg/l (exposure time 4 years) and Sjörgen et al. (1996) a median urinary Al concentration of 22 μg/l (exposure time >10 years). Altogether, the exposure time and the urinary Al levels were within the range of other studies on Al welders.
The neurobehavioral results suggest that the performance measures that were used are sensitive to age and therefore should also be sensitive to neurotoxic exposures. In contrast to this assumption, neither motor-performance tests nor short-term memory or switching-attention tests showed significant exposure effects. These non-significant results were stable across both examinations and did not change if possible confounders (age, education, CDT) were taken into account. In addition, sub-sample analyses, when verbal intelligence was considered as an estimate of pre-morbid intelligence, did not change the findings.
Welders and controls differed significantly with regard to performance in simple reaction time. However, it could not be shown that the differences between the groups increased during the 2 years of the study and were dependent on the growing number of years of exposure in welders. It is an advantage of the longitudinal study that this hypothesis could be tested. The interaction of exposure × examination is not significant, and the values show that the differences between the groups remained stable across the 2 years. Thus, it might be concluded that the difference is an accidental result that describes possible pre-exposure group differences. It is in line with this assumption that only one test out of many neurobehavioral tests, and only one test out of those that demanded a fast motor reaction (e.g. switching attention), showed significant group differences.
Simple reaction time shows a dose–response relationship with Al exposure, though small. But again, no other performance measure, whether it represented a comparable domain or another intellectual domain, showed a similar relationship. Additionally, regression analysis reveals that urine Al levels are predictors of reaction time only in models with the total sample, not in models with exposed workers alone. This suggests that performance differences between exposed subjects and controls, that might have existed a priori, accentuate the outcome of regression analysis. From regression analysis it is not possible to deduce whether difference between controls and exposed workers is a random a priori difference or an exposure effect because urinary Al level, exposure duration and age are related and confounded. The further follow up of the group difference across the study will show whether exposure is responsible; however, it might need more than 2 years of a longitudinal study to register slow changes in simple reaction-time performance.
Motor performance decrements are more or less indicated in some other studies of Al exposure. The comparability is a problem, as the subjects in our study do not have a mixed exposure to possible neurotoxic substances such as solvents, manganese and other welding fumes. This might possibly be a problem in other studies, as welding wire can contain a low percentage of manganese (Mn). In addition to this previous study, cohorts were rather small.
On the other hand, Dietz et al. (2001) showed no significant group differences in psychomotor performance between workers that were highly exposed to manganese dioxide and non-exposed workers.
The results of our study suggest that reaction time could be a first indicator for possible neurological changes in Al welders, as it is significantly related to exposure and age. However, as the Q16 questionnaire and the rest of the psychomotor performance showed no significant changes, and the examination period was only 2 years, the next cross-sectional study, in 2003, will prove the significance of the results.
References
Akila R, Stollery B, Riihimäki V (1999) Decrements in cognitive performance in metal inert gas welders exposed to aluminium. Occup Environ Med 56:632–639
Alfrey AC, LeGendre GR, Kaehne WD (1976) The dialysis encephalopathy syndrome. Possible aluminum intoxication. N Engl J Med 294:184–188
Armstrong, RA, Winsper, SJ, Blair JA (1996) Aluminium and Alzheimer's disease: review of possible pathogenic mechanisms. Dementia 7:1–9
Bast-Pettersen R, Skaug V, Ellingsen D (2000) Neurobehavioral performance in aluminium welders. Am J Ind Med 37:184–192
Dietz MC, Ihrig A, Wrazidlo W, Bader M, Jansen O, Triebig G (2001) Results of magnetic resonance imaging in long-term manganese dioxide-exposed workers. Environ Res 85:37–40
Doll R (1993) Alzheimer's disease and environmental aluminium. Age Ageing 22:138–153
Gilioli R (1993) EURONEST (1993) a concerted action of the European community for the study of organic solvents neurotoxicity. Environ Res 62:89–98
Hänninen H, Matikainen E, Kovala T (1994) Internal load of aluminium and the central nervous system function of aluminium workers. Scand J Work Environ Health 20:279–285
Heller KA, Kratzmeier H, Lengfelder A (1988) Matritzen-Test-Manual zu den Standard Progressive Matrices von J.C. Raven. Beltz Test, Göttingen
Hogstedt C, Andersson K, Hane M (1984) A questionnaire approach to the monitoring of early disturbances in central nervous functions. In: Aitio A, Riihimaki V, Vaninio H (eds) Biological monitoring and surveillance of workers exposed to chemicals. Hemisphere, Washington, pp 275–287
Hosovki E, Mastelica Z, Sunderic D (1990) Mental abilities of workers exposed to aluminium. Med Lav 81:119–123
Ihrig A, Triebig G, Dietz MC (2001) Evaluation of a modified German version of the Q16 questionnaire for neurotoxic symptoms in workers exposed to solvents. Occup Environ Med 58:19–23
Iregren A, Gamberale F, Kjellberg A (1996) SPES: a psychological test system to diagnose environmental hazards. Neurotoxicol Teratol 18:485–491
Iregren A, Sjörgen B, Gustafsson K, Hagman M, Nylén L, Frech W, Andersson M, Ljunggren KG, Wennberg A (2001) Effects on the nervous system in different groups of workers exposed to aluminium. Occup Environ Med 58:453–460
Lehnert G, Schaller KH, Angerer J (1999) Report on the status of the external quality-control programs for occupational—medical and environmental—medical toxicological analyses in biological materials in Germany. Int Arch Occup Environ Health 72:60–64
Letz R, Pieper WA, Morris RD (1996) NES test performance in a large US army veteran sample: relationship with both demographic factors and traditional neuropsychological measures. Neurotoxicol Teratol 18:381–390
Letzel S, Schaller KH, Hilla W, Windorfer K, Kraus T (1999) Untersuchung zur biologischen Halbwertszeit der realen Alumiumausscheidung bei Alumiumschweissern: Arbeitsmed Sozialmed Umweltmed 11:456–460
Letzel S, Lang CJG, Schaller KH, Angerer J, Fuchs S, Neundörfer B, Lehnert G (2000) Longitudinal study of neurotoxicity with occupational exposure to aluminium dust. Neurology 54:997–1000
Oswald WD, Roth E (1997) Der Zahlenverbindungstest, ZVT (trail making). Hogrefe, Göttingen
Rifat SL, Eastwood MR, Crapper McLachlan DR, Corey PN (1990) Effects of exposure of miners to aluminium powder. Lancet 336:1162–1165
Savory J, Exley C, Forbes WF, Huang Y, Joshi JG, Kruck T, McLachlan DRC, Wakayama I (1996) Can the controversy of the role of aluminium in Alzheimer's disease be resolved? What are the suggested approaches to this controversy and methodological issues to be considered? J Toxicol Environ Health 48:615–635
Schmidt KH, Metzler P (1992) WST Wortschatztest 1992. Beltz, Weinheim
Sjörgen B, Iregren A, Frech W (1996) Effects on the nervous system among welders exposed to aluminium and manganese. Occup Environ Med 53:32–40
Thomas, Dahl (1969) Zur Validität der Intelligenzdiagnostik im reduzierten Wechslertest (WIP). Psychol Beitr 4:543–550
Acknowledgments
We thank Hauptverband der gewerblichen Berufsgenossenschaften (HVBG) and Vereinigung der Metallberufsgenossenschaften (VMBG) for financial support for the study. Some data were taken from the medical dissertation of A. Kuhlmann.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Buchta, M., Kiesswetter, E., Otto, A. et al. Longitudinal study examining the neurotoxicity of occupational exposure to aluminium-containing welding fumes. Int Arch Occup Environ Health 76, 539–548 (2003). https://doi.org/10.1007/s00420-003-0450-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-003-0450-9