
Abstract
Purpose
The renin-angiotensin system is involved in the pathogenesis of fibrosis in several organs via induction of transforming growth factor (TGF) beta. In the pathogenesis of proliferative vitreoretinopathy (PVR) TGF-beta plays a pivotal role, promoting transition of retinal pigment epithelial (RPE) cells into myofibroblasts. We studied the influence of angiotensin converting enzyme-inhibition (ACEI) on cytokines and growth factors, related to PVR in aqueous humor.
Methods
We performed a post hoc analysis of a prospectively conducted interventional case series. From patients with rhegmatogenous retinal detachment (RRD) aqueous humor was obtained during primary surgery and analyzed using multiplex bead analysis for interferon gamma, tumor necrosis factor alpha, CC-chemokine ligand (CCL) 2 / monocyte chemoattractant protein (MCP)-1, interleukin (IL)-1 beta, IL-2, IL-4, IL-6, IL-8, vascular endothelial growth factor (VEGF)-A, platelet derived growth factor (PDGF)-aa, TGF-beta 1, TGF-beta 2, TGF-beta 3, fibroblast growth factor (FGF)-aa, and FGF-bb. We recorded information about systemic ACEI from the medical history.
Results
In the primary study elevated levels of TGF-beta 1 and 2, IL 6 and 8 and CCL2/MCP-1 were a risk factor for later PVR development. Here, systemic ACEI neither influenced levels of these cytokines and growth factors, nor of any other tested in this study (p ≥ 0.438, respectively). Also the incidence of PVR development was unaffected (p = 0.201).
Conclusion
The systemic intake of ACEI for arterial hypertension does not influence levels of profibrotic cytokines/growth factors in aqueous humor. Further studies need to clarify if relevant levels of ACEI accumulate in the eye, and if direct administration of ACEI in experimental PVR could be beneficial.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Proliferative vitreoretinopathy (PVR) is the leading cause for failure of vitreoretinal surgery [1, 2]. Transforming growth factor (TGF) beta plays a key role in the pathogenesis of PVR [3,4,5,6,7,8,9]. An important step in the development of the characteristic tractional PVR membranes is the epithelial to mesenchymal transition (EMT) of retinal pigment epithelial (RPE) cells into contractile myofibroblasts [9,10,11]. Several groups showed that TGF-beta isotypes 1 and 2 induce EMT in vitro, as well as in vivo [5, 8,9,10, 12, 13].
The same pathomechanism underlies renal fibrosis. Here, TGF-beta induces EMT of renal tubular epithelial cells [14, 15]. Pharmacological inhibition of the angiotensin converting enzyme (ACEI) counteracts the EMT and eventually renal fibrosis [15, 16]. Causative could be that ACEI seems to inhibit the pronounced TGF-beta expression during renal fibrosis [15, 16].
In 2013, we conducted a prospective interventional case series enrolling patients with rhegmatogenous retinal detachment (RRD). We found that elevated aqueous flare values, as well as elevated profibrotic cytokines and growth factors in the aqueous humor constitute a risk factor for later PVR development. TGF-beta 1 but not TGF-beta 2 was one of the factors endangering patients for later PVR.
In this post-hoc analysis of the described population, we aimed to study the influence of systemic ACEI medication for arterial hypertension on aqueous flare and profibrotic cytokines and growth factors, which were formerly identified as risk factors for later PVR.
Materials and methods
In this post hoc analysis of a prospective interventional case series [6], 62 consecutive patients with primary rhegmatogenous RD were included in the analysis. The protocol was approved by the institutional review board of the University of Cologne and followed the tenets of the Declaration of Helsinki.
Exclusion criteria of the primary study were any uncontrolled ocular disease including: active vasculitis, active uveitis, proliferative diabetic retinopathy, diabetic macular edema, neovascular age-related macular degeneration, retinal vein occlusion, and preoperative PVR.
We determined aqueous flare levels in photon counts per millisecond (pc/ ms) preoperatively after pupillary dilatation with 0.5% tropicamide and 5% phenylephrine hydrochloride, using the Kowa FM-500 Laser Flare-Cell Meter (V.1.0; Kowa Company Ltd., Tokyo, Japan). Ten measurements of each eye were averaged. Measurements with artifacts were excluded. We applied the previously defined threshold [17] of 15 pc/ms as cut-off value for elevated flare levels.
Past studies showed that protein levels of the vitreous corresponded well with protein levels in aqueous humor [9]. However, the examination of the aqueous humor instead of investigating the vitreous might be a weakness of our study. We obtained aqueous humor samples using a 1 ml syringe with a 30 gauge needle in the still native eye (before pars plana vitrectomy, scleral buckling or any other manipulation). Samples were stored at −80 °C for a maximum of 3 months. The presence of PVR was evaluated at 6 weeks and 3 months postoperatively.
By means of multiplex fluorescent bead-based immunoassays (Luminex, Austin, TX, USA) using Human Cytokine Custom Premix Fluorokine MAP Kit A, Human Angiogenesis Custom Premix Fluorokine MAP Kit and Fluorokine MAP 3-plex Kit (R&D Systems, Wiesbaden, Germany) we analyzed the cytokines and growth factors interferon (IFN) gamma, tumor necrosis factor alpha (TNF-alpha), CC-chemokine ligand (CCL) 2 / macrophage chemoattractant protein (MCP)-1, interleukin (IL)-1 beta, IL-2, IL-4, IL-6 and IL-8, vascular endothelial growth factor (VEGF)-A, platelet derived growth factor (PDGF)-aa, transforming growth factor beta (TGF-beta) isoforms 1, 2, 3 and fibroblast growth factor (FGF)-aa and FGF-bb. We used 50 μl of aqueous humor, for each Luminex panel. Analysis was performed according to the manufacturers’ instructions. Results are given in pg/ml.
From the medical history of the patients, we obtained data about accompanying systemic medication with ACEI. The respective patients were treated with ACEI continuously throughout follow-up. The used ACEIs were Ramipril, Enalapril, Lisinopril and Captopril.
Statistical analysis was performed using commercially available software (GraphPad Prism, La Jolla, CA, USA). Significance levels for the frequency of postoperative PVR were performed with the Fisher exact test. Subgroup comparisons of flare, cytokine and growth factor levels were performed with non-parametric tests, not assuming Gaussian distribution.
Results
Baseline characteristics
In this post hoc analysis of a prospective interventional case series we enrolled 62 patients with RRD. Forty patients were male, 22 were female. Mean age was 59 ± 13 years (range, 23–83 years). We estimated the duration of the retinal detachment by anamnestically determined onset of symptoms. Patients described having symptoms 8 ± 12 days (range, 1–60 days) on average before reporting to the clinic. The amount of retinal detachment in quadrants was 2 ± 1 (1–4) on average. The macula was involved in 28 cases. Patients were phakic in 41 cases and pseudophakic in 21 cases. All patients received a preoperative laser-flare analysis. Laser-flare-values were 13.27 ± 12.52 pc/ms (range, 2.60–74.30 pc/ms) on average. We present the mean values of the microbead-analysis of growth factors and cytokines in Table 1. During the follow up of 3 months, nine patients (15%) developed PVR grade CP1, four patients had a tractional retinal re-detachment due to PVR.
Influence of systemic ACEI medication on PVR development
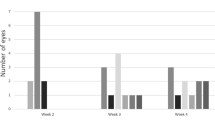
Fifteen of 62 patients (24%) received systemic medication with ACEI. Four of these 15 (27%) developed PVR. Five of the 47 patients (11%) without ACEI developed PVR. This difference was not significant (p = 0.201) (Fig. 1a).

a: Proportion of retinal detachment patients [%] with or without later PVR with or without concomitant systemic ACEI medication did not differ significantly; P-value: 0.201. b: Proportion of retinal detachment patients [%] with Flare values over and under 15pc/ms with or without concomitant systemic ACEI medication did not differ significantly; P-value: 0.088. Abbreviations: ACEI: angiotensin-converting-enzyme-inhibitor; PVR: proliferative vitreoretinopathy
Mean flare values of patients with ACEI medication were 15.95 ± 13.61 pc/ms (range, 5.00–44.50 pc/ms). Mean flare values of patients without ACEI medication were 12.47 ± 12.21 pc/ms (range, 2.60–74.03pc/ms). The difference was not significant (p = 0.309). In our primary results from the study, we found a cut-off 15pc/ms as a good discriminator to determine the risk for later PVR. Four of 15 (27%) patients with ACEI medication had a flare value of over 15pc/ms. Four of 47 (9%) patients without ACEI medication had flare values over 15pc/ms. This difference was also not significant (p = 0.088) (Fig. 1 B).
None of the tested cytokines or growth factors was affected by the systemic ACEI medication. Results are given in Table 1. The levels of IFN gamma, TNF alpha, IL-1 beta, IL-2, IL-4, TGF-beta 3 and FGF-aa and FGF-bb were below detection-threshold.
Discussion
In the primary study, we determined profibrotic cytokines and growth factors, which could serve as a predictor for later PVR in patients with rhegmatogenous retinal detachment. In this post hoc analysis of a prospectively conducted study on patients with retinal detachment [6], we investigated the effect of systemic ACEI medication on profibrotic cytokine and growth factor levels in the aqueous humor of the eye. TGF-beta isotype 1 but not isotype 2 was among these growth factors [6]. The literature provides evidence that inhibition of the renin-angiotensin system prevents fibrosis by down-regulation of TGF-beta [14,15,16]. There is evidence for the presence of the renin-angiotensin system in the eye and its humors [18]. Therefore, it is tempting to analyze the effect of systemic ACEI medication on the incidence of PVR in the eye. However, in this post hoc analysis, we did not find any effect of the systemic ACEI medication on cytokine and growth factor levels including TGF beta isotypes in the aqueous humor. We also did not find any effect on the incidence of PVR.
Angiotensin 2 promotes TGF-beta release and TGF-beta dependent synthesis of collagen IV and extracellular matrix proteins [15, 19, 20]. Consecutively, this system could be at least partly involved in the upregulation of TGF-beta and the formation of tractional retinal membranes during the pathogenesis of PVR. Interestingly, inhibition on angiotensin 2 via systemic ACEI medication affects TGF-beta isotype 1 expression, rather than TGF-beta isotype 2 [15]. Our results from former studies also suggest a pronounced role of TGF-beta isotype 1, rather than isotype 2 [6, 9]. The fact that systemic ACEI medication did not influence cytokine and growth factor levels could be due to a lack of penetration of the ACEI medication into the eye. Alternatively, the systemic levels of ACEI could be too low to inhibit the renin-angiotensin system within the eye. Consecutively, inhibition of the renin-angiotensin system in the eye could be only minor. A major limitation of our study includes the relatively small number of cases. Future and larger studies need to clarify whether systemic ACEI medication leads to relevant levels of ACEI within the eye and to relevant inhibition of the ocular renin-angiotensin system. In this context concentrations of ACE in the aqueous humor need to be analyzed. In addition, direct application of ACEI into the eye in an experimental setting could be a worthwhile attempt to prevent PVR in the future. Inhibition of the renin-angiotensin system could prove beneficial not only to patients at risk for PVR, but also to the large group of patients with Fuchs endothelial dystrophy (FED). This disease is also characterized by EMT of endothelial cells. Similar cytokines have been related to EMT in FED patients as well as in PVR patients [21, 22].
References
Glaser BM, Cardin A, Biscoe B (1987) Proliferative vitreoretinopathy. The mechanism of development of vitreoretinal traction. Ophthalmology 94:327–332
Pastor JC (1998) Proliferative vitreoretinopathy: an overview. Surv Ophthalmol 43:3–18
Bochaton-Piallat ML, Kapetanios AD, Donati G, Redard M, Gabbiani G, Pournaras CJ (2000) TGF-beta1, TGF-beta receptor II and ED-A fibronectin expression in myofibroblast of vitreoretinopathy. Invest Ophthalmol Vis Sci 41:2336–2342
Connor TB Jr, Roberts AB, Sporn MB, Danielpour D, Dart LL, Michels RG, de Bustros S, Enger C, Kato H, Lansing M et al (1989) Correlation of fibrosis and transforming growth factor-beta type 2 levels in the eye. J Clin Invest 83:1661–1666
Gamulescu MA, Chen Y, He S, Spee C, Jin M, Ryan SJ, Hinton DR (2006) Transforming growth factor beta2-induced myofibroblastic differentiation of human retinal pigment epithelial cells: regulation by extracellular matrix proteins and hepatocyte growth factor. Exp Eye Res 83:212–222
Hoerster R, Hermann MM, Rosentreter A, Muether PS, Kirchhof B, Fauser S (2013) Profibrotic cytokines in aqueous humour correlate with aqueous flare in patients with rhegmatogenous retinal detachment. Br J Ophthalmol 97:450–453
Kita T, Hata Y, Arita R, Kawahara S, Miura M, Nakao S, Mochizuki Y, Enaida H, Goto Y, Shimokawa H, Hafezi-Moghadam A, Ishibashi T (2008) Role of TGF-beta in proliferative vitreoretinal diseases and ROCK as a therapeutic target. Proc Natl Acad Sci U S A 105:17504–17509
Nassar K, Grisanti S, Tura A, Luke J, Luke M, Soliman M, Grisanti S (2014) A TGF-beta receptor 1 inhibitor for prevention of proliferative vitreoretinopathy. Exp Eye Res 123:72–86
Hoerster R, Muether PS, Vierkotten S, Hermann MM, Kirchhof B, Fauser S (2014) Upregulation of TGF-ss1 in experimental proliferative vitreoretinopathy is accompanied by epithelial to mesenchymal transition. Graefes Arch Clin Exp Ophthalmol 252:11–16
Lee H, O’Meara SJ, O’Brien C, Kane R (2007) The role of gremlin, a BMP antagonist, and epithelial-to-mesenchymal transition in proliferative vitreoretinopathy. Invest Ophthalmol Vis Sci 48:4291–4299
Nassar K, Luke J, Luke M, Kamal M, Abd El-Nabi E, Soliman M, Rohrbach M, Grisanti S (2011) The novel use of decorin in prevention of the development of proliferative vitreoretinopathy (PVR). Graefes Arch Clin Exp Ophthalmol 249:1649–1660
Hatanaka H, Koizumi N, Okumura N, Kay EP, Mizuhara E, Hamuro J, Kinoshita S (2012) Epithelial-mesenchymal transition-like phenotypic changes of retinal pigment epithelium induced by TGF-beta are prevented by PPAR-gamma agonists. Invest Ophthalmol Vis Sci 53:6955–6963
Parapuram SK, Chang B, Li L, Hartung RA, Chalam KV, Nair-Menon JU, Hunt DM, Hunt RC (2009) Differential effects of TGFbeta and vitreous on the transformation of retinal pigment epithelial cells. Invest Ophthalmol Vis Sci 50:5965–5974
Miyajima A, Chen J, Lawrence C, Ledbetter S, Soslow RA, Stern J, Jha S, Pigato J, Lemer ML, Poppas DP, Vaughan ED, Felsen D (2000) Antibody to transforming growth factor-beta ameliorates tubular apoptosis in unilateral ureteral obstruction. Kidney Int 58:2301–2313
El Chaar M, Chen J, Seshan SV, Jha S, Richardson I, Ledbetter SR, Vaughan ED Jr, Poppas DP, Felsen D (2007) Effect of combination therapy with enalapril and the TGF-beta antagonist 1D11 in unilateral ureteral obstruction. Am J Physiol Renal Physiol 292:F1291–F1301
Sun N, Zhai L, Li H, Shi LH, Yao Z, Zhang B (2016) Angiotensin-converting enzyme inhibitor (ACEI)-mediated amelioration in renal fibrosis involves suppression of mast cell degranulation. Kidney Blood Press Res 41:108–118
Schroder S, Muether PS, Caramoy A, Hahn M, Abdel-Salam M, Diestelhorst M, Kirchhof B, Fauser S (2012) Anterior chamber aqueous flare is a strong predictor for proliferative vitreoretinopathy in patients with rhegmatogenous retinal detachment. Retina 32:38–42
Ramirez M, Davidson EA, Luttenauer L, Elena PP, Cumin F, Mathis GA, De Gasparo M (1996) The renin-angiotensin system in the rabbit eye. J Ocul Pharmacol Ther 12:299–312
Wolf G, Zahner G, Schroeder R, Stahl RA (1996) Transforming growth factor beta mediates the angiotensin-II-induced stimulation of collagen type IV synthesis in cultured murine proximal tubular cells. Nephrol Dial Transplant 11:263–269
Gomez-Garre D, Ruiz-Ortega M, Ortego M, Largo R, Lopez-Armada MJ, Plaza JJ, Gonzalez E, Egido J (1996) Effects and interactions of endothelin-1 and angiotensin II on matrix protein expression and synthesis and mesangial cell growth. Hypertension 27:885–892
Heindl LM, Schlotzer-Schrehardt U, Cursiefen C, Bachmann BO, Hofmann-Rummelt C, Kruse FE (2011) Myofibroblast metaplasia after descemet membrane endothelial keratoplasty. Am J Ophthalmol 151:1019–1023 e1012
Matthaei M, Gillessen J, Muether PS, Hoerster R, Bachmann BO, Hueber A, Cursiefen C, Heindl LM (2015) Epithelial-mesenchymal transition (EMT)-related cytokines in the aqueous humor of Phakic and Pseudophakic Fuchs’ dystrophy eyes. Invest Ophthalmol Vis Sci 56:2749–2754
Acknowledgements
RH received support within the Köln Fortune study program from the University of Cologne. None of the authors has any conflicts of interest to declare regarding the content of this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Author statement
ᅟ
Funding
The University of Cologne provided financial support within the Köln Fortune study program in the form of funding personnel costs of RH and laboratory materials for the study. The sponsor had no role in the design or conduct of this research.
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Hoerster, R., Fauser, S., Cursiefen, C. et al. The influence of systemic renin-angiotensin-inhibition on ocular cytokines related to proliferative vitreoretinopathy. Graefes Arch Clin Exp Ophthalmol 255, 1721–1725 (2017). https://doi.org/10.1007/s00417-017-3707-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-017-3707-9