
Abstract
Purpose
To compare visual and anatomical outcomes of half-fluence (HF) and half-dose (HD) photodynamic therapy (PDT) in chronic central serous chorioretinopathy (CSC). Particular focus was given to photoreceptor recovery rate following treatment.
Methods
Retrospective review of 52 chronic CSC patients who underwent HF- or HD-PDT (26 patients per group). Best-corrected visual acuity and spectral-domain optical coherence tomography findings were compared between groups.
Results
Average follow-up for HF- and HD-PDT was 20.7 ± 7.2 and 22.3 ± 6.1 months respectively. Both groups had significant visual acuity improvements, as well as central foveal and subfoveal choroidal thickness reductions. Measured parameters were not significantly different between groups at any time point examined. Complete photoreceptor recovery, defined as a continuous ellipsoid zone with a discernible interdigitation zone, was observed at 12 months in 19 (73 %) and 14 patients (54 %) in the HF- and HD-PDT groups respectively (p = 0.150). Overall photoreceptor recovery rate was not different between groups (p = 0.301, log-rank test). Delayed (>12 months) photoreceptor recovery was significantly associated with baseline external limiting membrane disruption (OR: 21.7, 95 % CI: 1.7–285.4, p = 0.019), disease duration (years, OR: 1.9, 95 % CI: 1.2–3.0, p = 0.005), and fovea-to-PDT spot center distance (100 μm unit, OR: 0.74, 95 % CI 0.56–0.97, p = 0.027). However, delayed photoreceptor recovery was not significantly associated with PDT modality.
Conclusion
Both HF- and HD-PDT are effective in treating chronic CSC. No significant differences in visual or anatomical outcomes were observed.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Central serous chorioretinopathy (CSC) is characterized by serous detachment of the neurosensory retina in the posterior pole, and diffuse decompensation of the retinal pigment epithelium (RPE) [1]. The exact pathophysiology of CSC remains unknown. However, indocyanine green angiography (ICGA) has shown hyperpermeable choroidal vessels [2, 3], and enhanced-depth imaging (EDI) optical coherence tomography (OCT) has shown thickened choroidal tissue [4] in eyes with CSC, which suggests choroidal vasculopathy as a direct cause of CSC.
Photodynamic therapy (PDT), which induces intravascular damage, thrombus formation, and selective vascular occlusion [5], is gaining in popularity as a treatment for CSC [6–8]. To reduce possible PDT-associated complications [6, 9, 10], various modifications have been made to the standard PDT protocol, i.e., halving the laser fluence [11–13] and the photosensitizer dose [14, 15]. Fortunately, both treatment modifications have been shown to be effective in resolving subretinal fluid (SRF) and in improving visual acuity in eyes with CSC. However, few studies have directly compared the efficacy of half-fluence (HF) and half-dose (HD) PDT in eyes with CSC. Nicolo et al. [16] recently found that HD-PDT was more effective than HF-PDT in drying the macula, while no significant differences in visual outcomes were observed. Alkin et al. [17] showed that both HD- and HF-PDT were equally effective in resolving SRF and improving visual acuity. However, both of these studies only examined visual acuity, central foveal thickness, and SRF resolution in a relatively short follow-up period to draw their conclusions.
In the current study, we compared visual and anatomical outcomes of HF- and HD-PDT in eyes with chronic CSC more thoroughly. Serial assessments of spectral-domain optical coherence tomography (OCT) images allowed us to quantitatively (central foveal thickness, subfoveal choroidal thickness) and qualitatively (external limiting membrane [ELM] and ellipsoid zone status) examine the effect of HD- and HF-PDT on CSC. In particular, we focused on photoreceptor recovery rate following PDT and its associated factors.
Materials and methods
We retrospectively reviewed the medical records of patients diagnosed with chronic CSC who underwent PDT at Seoul National University Bundang Hospital (Seongnam, South Korea) between January 2011 and July 2012. This study was approved by the institutional review board (IRB) of Seoul National University Bundang Hospital (Seongnam, South Korea). The need for a study informed consent was waived by the IRB. All study conduct adhered to the tenets of the Declaration of Helsinki.
A CSC diagnosis was based on fundoscopy, fluorescein angiography (FA), ICGA (Heidelberg Retina Angiography, Heidelberg Engineering, Heidelberg, Germany), and OCT (Spectralis OCT, Heidelberg Engineering, Heidelberg, Germany) findings. The CSC was considered chronic if visual disturbances persisted for more than 6 months or if CSC was recurrent. Patients were included in analyses if the following were true: (1) chronic CSC diagnosis, (2) best-corrected visual acuity (BCVA) of 20/200 or better, (3) presence of SRF involving the fovea on OCT, and (4) clinical follow-up of at least 12 months. Patients were excluded from analyses if any of the following were true: (1) presence of choroidal neovascularization or any other chorioretinal disorder that might affect visual acuity and/or foveal structure, (2) history of CSC treatment other than oral medication, or (3) history of intraocular surgery (uncomplicated cataract surgery allowed).
During the study period, two separate retinal outpatient clinics at our hospital used different PDT modifications for CSC patients. Patients underwent either HF-PDT (25 J/cm2, Dr. KHP) or HD-PDT (3 mg/m2 verteporfin [Visudyne, Novartis AG, Switzerland], Dr. SJW) using a 689-nm laser for 83 s. The PDT spot size was defined as the diameter of the smallest circle covering the hyperpermeable choroidal lesion that resulted in subfoveal fluid accumulation, as imaged on mid-phase ICGA. If there were more than two separate areas of choroidal hyperpermeability, they were measured separately and treated separately in the same PDT session. In these cases, overall PDT spot size was defined as the sum of the individual PDT spot sizes.
All SD-OCT images were evaluated quantitatively and qualitatively. Quantitative evaluations included central foveal thickness and subfoveal choroidal thickness measurements. Central foveal thickness was defined as the distance between the internal limiting membrane and the inner border of the RPE, and was measured manually using the built-in calliper tool. Subfoveal choroidal thickness was also manually measured on EDI-OCT images [18], and defined as the distance between the outer portion of the RPE and the inner surface of the sclera beneath the foveal center. To adjust for physiological variation in baseline choroidal thickness, the ratio of follow-up choroidal thickness to baseline choroidal thickness was also evaluated. The distance between PDT spot center and foveal center was also measured manually using the built-in calliper tool. We evaluated the PDT spot coverage over 1-mm foveal subfield zone, i.e., complete, partial, or no involvement.
Qualitative assessments of OCT images included ELM and photoreceptor ellipsoid zone status. These evaluations were made on a line scan that was the average of 50 to 100 horizontal or vertical OCT scans that were centered on the fovea. The presence or absence of subfoveal fluid within the juxtafoveal area was also determined using 20 × 30° volume scan images centered on macula. The ELM was then classified as complete or disrupted (discontinuous) and the photoreceptor ellipsoid zone was classified as disrupted (discontinuous), partial (no gross discontinuity, indiscernible interdigitation zone), or complete (continuous, discernible interdigitation zone). When SRF was present, a precise ellipsoid zone assessment could not be made, thus only ELM status was evaluated. Two independent observers (Y-KK, N-KR) measured and evaluated OCT parameters. The averages of quantitative measurements were used in analyses. When discrepancies in qualitative assessments of the ELM or the ellipsoid zone status arose, the two observers discussed their evaluations and came to an agreement.
Snellen BCVA measurements were converted to the logarithm of the minimal angle of resolution (logMAR) scale for all analyses. Patients were examined 1 month after PDT and every 3 to 4 months thereafter. The final visit was defined as an evaluation performed at the last visit, more than 12 months following PDT. Means of continuous variables were compared using the Mann–Whitney test, and categorical variables were compared using a chi-squared or Fisher’s exact test. Serial changes of visual outcome, central foveal thickness, and subfoveal choroidal thickness were compared between HF- and HD-PDT groups using linear mixed model, with group and time as fixed effects and patients as random effect. Statistical analyses were performed using statistical software (Stata version 13.0; Stata Corp., College Station, TX, USA) and statistical significance was defined as a p < 0.05.
Results
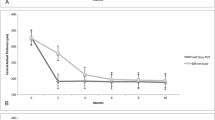
Twenty-six eyes of 26 patients underwent HF–PDT. Another 26 eyes of 26 different patients underwent HD-PDT. The demographics and clinical characteristics of both groups are summarized in Table 1. There were no significant differences between groups in terms of age, sex, chronicity of the disease, and PDT parameters, except for PDT spot size, which was larger in the HD-PDT group (HD-PDT, 3,073 ± 848 μm vs HF-PDT, 2,373 ± 555 μm, p = 0.002). Figure 1 shows changes in BCVA, visual gain, central foveal thickness, and subfoveal choroidal thickness over time for each PDT group. Both groups showed significant improvement of visual acuity and reduction of central foveal thickness and subfoveal choroidal thickness over time (all p < 0.001, linear mixed model), without any significant differences between groups (all p > 0.7, linear mixed model, Fig. 1).

a Best-corrected visual acuity (BCVA), b visual gain, c central foveal thickness, and d relative subfoveal choroidal thickness compared to the baseline value in patients treated with half-fluence (HF) or half-dose (HD) photodynamic therapy. Numbers beneath the graph represent the number of patients included in the analyses at a specific time point. LogMAR logarithm of minimum angle of resolution. Final = last visit more than 12 months following photodynamic therapy
Most patients had complete SRF absorption 1 month after PDT, indicating a prompt effect of PDT in drying the macula. There were no significant differences in SRF absorption rates between the two groups (p = 0.976, log-rank test, Fig. 2). Only one patient (4 %) in the HF-PDT group had persistent shallow SRF, which was present until the last visit 27 months after treatment. Although SRF persisted in this 54-year-old man, ICG leakage was markedly reduced, and no additional PDT was performed (Fig. 3). All other patients had complete SRF absorption within 5 months of PDT.

Absorption rate of subretinal fluid (SRF) under the macula in patients treated with half-fluence and half-dose photodynamic therapy. The bottom portion of the figure is the magnified view of the rectangular area indicated in the top portion

Imaging studies of the left eye of a 54-year-old man with persistent subretinal fluid (SRF) after half-fluence photodynamic therapy (PDT). a Baseline indocyanine green angiography (ICGA) showing leakage. b An ICGA image taken 1 month after PDT showing a decrease in the amount of leakage. c An ICGA image taken 6 months after PDT showing that the leakage remained decreased. d Baseline optical coherence tomography (OCT) revealed subfoveal fluid with a disrupted external limiting membrane (arrowheads). e An OCT image taken 1 month after PDT shows a decrease in subfoveal fluid. f An OCT image taken 6 months after PDT shows an increase in subfoveal fluid, but no active leakage was observed on ICGA (c). No additional treatments were administered to the patient. g–i Subfoveal fluid was present until the last follow up examination 27 months after PDT. Visual acuity (VA) is shown in the lower, left corner of each image
Figure 4 shows a typical photoreceptor recovery following PDT in an eye with CSC. Baseline OCT images revealed subfoveal fluid and a continuous ELM without gross defects (Fig. 4a). One month after PDT, the SRF had been completely absorbed, while the ellipsoid zone was discontinuous (Fig. 4b). Three months after PDT, the ellipsoid zone was continuous without gross defects, but the subfoveal interdigitation zone was indiscernible (Fig. 4c). Six months after PDT, the subfoveal interdigitation zone was visible and distinguishable from the ellipsoid zone and RPE/Bruch’s complex (Fig. 4d). Photoreceptor recovery continued through the last follow-up visit 12 months after PDT (Fig. 4e).

Typical photoreceptor recovery following half-fluence photodynamic therapy (PDT) in a 45-year-old male with central serous chorioretinopathy. a Baseline optical coherence tomography image showing subfoveal fluid. The external limiting membrane (ELM) is continuous with no gross defects (arrowheads). b One month after PDT, the subfoveal fluid has completely absorbed, but discontinuities in the ellipsoid zone (EZ) are visible (arrowheads). c Three months after PDT, the EZ is continuous with no gross defects, but a subfoveal interdigitation zone is not apparent. d Six months after PDT, the subfoveal interdigitation zone is visible (arrows). e Twelve months after PDT, EZ integrity has been maintained and an interdigitation zone is visible (arrows)
The proportion of patients with a complete photoreceptor recovery (continuous ellipsoid zone, discernible subfoveal interdigitation zone) in each group was also examined. By 12 months, 19 of 26 patients (73 %) in the HF-PDT group and 14 of 26 patients (54 %) in the HD-PDT group had a complete photoreceptor recovery (p = 0.150). No significant differences were observed between groups in overall photoreceptor recovery rates (p = 0.301, log-rank test, Fig. 5, Table 1).

Photoreceptor (PR) recovery rates in patients treated with half-fluence or half-dose photodynamic therapy. Complete PR recovery was defined as a continuous ellipsoid zone and a discernible interdigitation zone on spectral domain optical coherence tomography images. The overall PR recovery rate was not significantly different between the half-fluence and half-dose photodynamic therapy groups (log-rank test, p = 0.301)
We evaluated clinical factors associated with photoreceptor recovery rate, including the type of PDT administered. The cut-off point between an early and delayed photoreceptor recovery was arbitrarily chosen as 12 months, and clinical characteristics were compared between two groups (Table 2). Multiple logistic regression analysis was performed to determine factors associated with a delayed photoreceptor recovery. The following parameters were examined: age, sex, CSC disease duration, distance from fovea-to-PDT spot center, PDT spot size, PDT modality, and baseline ELM disruption. Three clinical factors were significantly associated with delayed photoreceptor recovery, which were ELM disruption at baseline (OR: 21.7, 95 % CI: 1.7–285.4, p = 0.019), disease duration (years, OR: 1.9, 95 % CI: 1.2–3.0, p = 0.005), and fovea-to-PDT spot center distance (100 μm, OR: 0.74, 95 % CI: 0.56–0.97, p = 0.027). Interestingly, PDT modality was not significantly associated with a delayed photoreceptor recovery (HD-PDT, OR: 4.5, 95 %: CI 0.8–25.4, p = 0.093, Table 3).
One patient (4 %) in each group had CSC recurrence during the follow-up period after complete disease resolution. A 46-year-old male patient underwent HF-PDT in his left eye (1,500 μm spot, 800 μm inferior to the fovea). Subfoveal fluid had completely absorbed 1 month after treatment. However, a small amount of SRF beneath the previous area of leakage recurred 22 months after treatment. The SRF did not extend into the subfoveal region (Fig. 6). Another 46-year-old male patient underwent HD-PDT in his left eye (2,400 μm spot, 400 μm temporal to the fovea). Subfoveal fluid had completely absorbed 1 month after PDT, but recurred 26 months after treatment. The amount of leakage present on late-phase ICGA images was less severe than that present before PDT. Interestingly, the amount of subfoveal fluid spontaneously reduced 2 months later (Fig. 7).

A 46-year-old male patient who underwent half-fluence photodynamic therapy (PDT) had recurrent subretinal fluid. The PDT spot size was 1500 μm and was centered approximately 800 μm inferior to the fovea. The left column shows fovea-centered optical coherence tomography (OCT) images and the right column shows PDT spot-centered OCT images. Subretinal fluid was apparent at baseline (top row), both under the fovea and under the PDT lesion center. One month after PDT (second row), the subretinal fluid had completely resolved. Five months after PDT (third row), the subfoveal photoreceptor layer was completely restored. Unfortunately, 22 months after PDT (bottom row), a small amount of subretinal fluid was again present under the center of the PDT lesion. The subfoveal region remained unaffected

A 46-year-old male patient who underwent half-dose photodynamic therapy (PDT) had recurrent subretinal fluid (SRF). The PDT spot size was 2400 μm, and was centered approximately 400 μm temporal to the fovea. a, b Early- (a) and late-phase (b) indocyanine green angiography images. Hyperpermeable choroidal vessels and late leakage are observed. c At baseline, an optical coherence tomography (OCT) image shows a large amount of subfoveal fluid, along with a small pigment epithelial detachment. d One month after PDT, an OCT image shows complete subfoveal fluid absorption. e An OCT image taken 26 months after PDT shows a large amount of subfoveal fluid. f, g Early- (f) and late-phase (g) indocyanine green angiography images obtained 3 weeks after SRF recurrence. Hyperpermeable choroidal vessels are present, but the amount of leakage is less severe than it was before PDT. h Two months after SRF recurrence, the amount of SRF has spontaneously decreased
Discussion
In this study, we compared long-term visual and anatomical outcomes following HF- and HD-PDT for chronic CSC, and found that both modalities are effective in treating the disease. Both treatments resulted in a significant improvement in visual acuity and reductions in central foveal and subfoveal choroidal thickness measurements. On average, these benefits were maintained for more than a year. Additionally, all but one patient in the HF-PDT group had complete SRF absorption by 5 months, mostly within 1 month. This result is comparable with those of previous studies. Chan et al. [14] evaluated the efficacy of HD-PDT in chronic CSC patients, and reported that 89.6 % of eyes had complete SRF resolution at 12 months, and that 95.8 % of eyes had stable or improved vision after treatment. Smretschnig et al. [13] examined HF-PDT for chronic CSC. They observed a significant improvement in visual acuity, a decrease in central foveal thickness, and complete resolution of SRF one month after treatment.
In the previous study, Nicolo et al. suggested a greater efficacy of HD-PDT in drying the macula [16]. However, we could not observe similar results, as there were no significant differences in terms of SRF absorption rate or central foveal thickness change between the two PDT modality groups. As it was a retrospective study, we were not able to fully match the baseline characteristics between groups, and PDT spot size was significantly larger in the HD-PDT group. However, even after adjusting with those potential biasing factors on SRF absorption rate after PDT, such as age, sex, disease chronicity, PDT modality, PDT spot size, distance from fovea to PDT spot center, baseline central foveal thickness, and subfoveal choroidal thickness, there were no significant differences in SRF absorption rate between the HF- and HD-PDT groups (data not shown). Further study with prospective design and a large number of patients is needed to draw the conclusion on this issue.
It is well-known that choroidal thickness is reduced following PDT. Compared to laser photocoagulation, standard PDT reduces choroidal thickness and ICG vessel hyperpermeability [19]. A recent study showed significant decrease in the lumen area of abnormal choroidal vessels after HD-PDT [20]. These suggest that PDT induces remodelling of the choroidal vasculature. In the current study, we examined and compared subfoveal choroidal thickness changes over time in patients undergoing HF- or HD-PDT. Subfoveal choroidal thickness measurements were significantly decreased 1 month following treatment in both groups, and persisted until the last follow-up visit. There were no significant differences in choroidal thickness between the HF- and HD-PDT groups. This suggests that choroidal vascular changes induced by PDT are maintained over the long-term (≥12 months), regardless of the modality of PDT.
Photoreceptor recovery after PDT was evaluated using ELM and ellipsoid zone integrity, as determined on OCT images. The ellipsoid zone was considered to have a complete recovery when it was continuous and accompanied by a discernible interdigitation zone. The interdigitation zone, also referred to as the cone outer segment tips line, represents the junction between cone outer segments and apical RPE processes [21, 22]. Interdigitation zone integrity has been shown to be highly correlated with visual acuity in various disorders [23–25]. Additionally, a distinct, sometimes irregular, interdigitation zone is only observed in eyes with an intact ELM and ellipsoid zone [24]. Therefore, ellipsoid zone assessment may be more complete when the interdigitation zone is also evaluated. In a previous study, the ellipsoid zone was clearly detected immediately after the resolution of SRF in 71.6 %, and some of the remaining eyes showed recovery of the ellipsoid zone during follow-up [26]. In studies assessing the ellipsoid zone after HD PDT, 55.2 % of eyes showed continuous ellipsoid zone at 12 months [27], and 76 % of eyes showed ellipsoid zone continuity at 6 months in another study [28]. Additionally, 38 % and 46 % of eyes displayed a fragmented or continuous interdigitation zone 6 and 12 months respectively after treatment [29].
Unfortunately, few studies have evaluated photoreceptor recovery after HF-PDT. Our results showed a recovered ellipsoid zone 12 months following treatment in 73 % and 54 % of eyes treated with HF-and HD-PDT respectively. Although the HF-PDT group showed relatively rapid recovery of the ellipsoid zone compared to the HD-PDT group after 12 months, there were no significant differences in overall recovery rate. Moreover, the follow-up interval was not tight enough to precisely detect the exact time point of photoreceptor recovery after 1 year, and the PDT spot size was even larger in the HD-PDT group. Thus, it is likely that there are no significant differences in the rate of photoreceptor recovery after HF- and HD-PDT. In contrast to the results of a previous study, where the ellipsoid zone had not appeared at 6 months and still could not be seen at 1 year [28], our results suggest continued recovery of the ellipsoid zone even after a year. Complete ellipsoid zone recovery was observed in 23 of 26 eyes (88 %) in the HF-PDT group and 20 of 26 eyes (77 %) in the HD-PDT group at the last visit. Multiple logistic regression analysis result showed that chronicity of the disease and baseline ELM status was significantly associated with photoreceptor recovery after PDT. This is in accordance with a previous study, which showed that changes in the foveal photoreceptor layer in CSC may predict visual recovery after foveal reattachment [30]. In addition, distance between fovea and PDT center was also related to photoreceptor recovery rate. However, the modality of PDT, i.e., HF or HD, did not significantly affect the rate of photoreceptor recovery.
Long-term recurrence results have typically been reported for standard PDT protocols. Vasconcelos et al. [31] reported that two of 17 eyes (11.8 %) underwent a second round of PDT due to SRF recurrence during ≥5 years follow up. Silva et al. [32] showed a 93.4 % SRF resolution rate 4 years after standard PDT, with four of 46 eyes (8.7 %) requiring a second PDT for persistent (three eyes) or recurrent (one eye) SRF. However, long-term recurrence results following HF- and HD-PDT remain to be fully characterized. In our study, mean follow-up time was 21 and 22 months in the HF- and HD-PDT groups respectively. One eye (4 %) in each group had recurrent SRF, and the recurrent SRF was less severe than that originally observed prior to PDT. However, because of the small number of cases and the relatively short follow-up period, our findings remain inconclusive.
Study limitations include the small case numbers and its retrospective design, which led to a lack of randomization and irregular follow-up intervals. However, our direct comparison of quantitative and qualitative assessments of visual and anatomical outcomes following HF- and HD-PDT offers some insight. Prospective studies with a longer follow-up are needed to draw more concrete conclusions.
In summary, there were no significant differences in visual or anatomical outcomes following HF- and HD-PDT for chronic CSC. In both treatment groups, a steady photoreceptor recovery was observed following PDT, which was significantly dependent upon baseline photoreceptor damage severity, disease duration, and fovea–to-PDT spot distance. The PDT modality used did not significantly affect photoreceptor recovery rates.
References
Gass JD (1967) Pathogenesis of disciform detachment of the neuroepithelium. Am J Ophthalmol 63(Suppl):1–139
Prunte C, Flammer J (1996) Choroidal capillary and venous congestion in central serous chorioretinopathy. Am J Ophthalmol 121:26–34
Spaide RF, Hall L, Haas A, Campeas L, Yannuzzi LA, Fisher YL, Guyer DR, Slakter JS, Sorenson JA, Orlock DA (1996) Indocyanine green videoangiography of older patients with central serous chorioretinopathy. Retina 16:203–213
Imamura Y, Fujiwara T, Margolis R, Spaide RF (2009) Enhanced depth imaging optical coherence tomography of the choroid in central serous chorioretinopathy. Retina 29:1469–1473. doi:10.1097/IAE.0b013e3181be0a83
Schmidt-Erfurth U, Hasan T (2000) Mechanisms of action of photodynamic therapy with verteporfin for the treatment of age-related macular degeneration. Surv Ophthalmol 45:195–214
Cardillo Piccolino F, Eandi CM, Ventre L, Rigault de la Longrais RC, Grignolo FM (2003) Photodynamic therapy for chronic central serous chorioretinopathy. Retina 23:752–763
Yannuzzi LA, Slakter JS, Gross NE, Spaide RF, Costa D, Huang SJ, Klancnik JM Jr, Aizman A (2003) Indocyanine green angiography-guided photodynamic therapy for treatment of chronic central serous chorioretinopathy: a pilot study. Retina 23:288–298
Lim JI, Glassman AR, Aiello LP, Chakravarthy U, Flaxel CJ, Spaide RF (2014) Collaborative retrospective macula society study of photodynamic therapy for chronic central serous chorioretinopathy. Ophthalmology. doi:10.1016/j.ophtha.2013.11.040
Colucciello M (2006) Choroidal neovascularization complicating photodynamic therapy for central serous retinopathy. Retina 26:239–242
Chan WM, Lam DS, Lai TY, Tam BS, Liu DT, Chan CK (2003) Choroidal vascular remodelling in central serous chorioretinopathy after indocyanine green guided photodynamic therapy with verteporfin: a novel treatment at the primary disease level. Br J Ophthalmol 87:1453–1458
Reibaldi M, Boscia F, Avitabile T, Uva MG, Russo A, Zagari M, Occhipinti F, Russo V, Reibaldi A, Longo A (2011) Functional retinal changes measured by microperimetry in standard-fluence vs low-fluence photodynamic therapy in chronic central serous chorioretinopathy. Am J Ophthalmol 151:953–960.e952. doi:10.1016/j.ajo.2010.12.007
Shin JY, Woo SJ, Yu HG, Park KH (2011) Comparison of efficacy and safety between half-fluence and full-fluence photodynamic therapy for chronic central serous chorioretinopathy. Retina 31:119–126. doi:10.1097/IAE.0b013e3181e378f2
Smretschnig E, Ansari-Shahrezaei S, Hagen S, Glittenberg C, Krebs I, Binder S (2013) Half-fluence photodynamic therapy in chronic central serous chorioretinopathy. Retina 33:316–323. doi:10.1097/IAE.0b013e318280769c
Chan WM, Lai TY, Lai RY, Tang EW, Liu DT, Lam DS (2008) Safety enhanced photodynamic therapy for chronic central serous chorioretinopathy: one-year results of a prospective study. Retina 28:85–93. doi:10.1097/IAE.0b013e318156777f
Uetani R, Ito Y, Oiwa K, Ishikawa K, Terasaki H (2012) Half-dose vs one-third-dose photodynamic therapy for chronic central serous chorioretinopathy. Eye (Lond) 26:640–649. doi:10.1038/eye.2012.66
Nicolo M, Eandi CM, Alovisi C, Grignolo FM, Traverso CE, Musetti D, Piccolino FC (2014) Half-fluence versus half-dose photodynamic therapy in chronic central serous chorioretinopathy. Am J Ophthalmol 157(5):1033–1037. doi:10.1016/j.ajo.2014.01.022
Alkin Z, Perente I, Ozkaya A, Alp D, Agca A, Aygit ED, Korkmaz S, Yazici AT, Demirok A (2014) Comparison of efficacy between low-fluence and half-dose verteporfin photodynamic therapy for chronic central serous chorioretinopathy. Clin Ophthalmol 8:685–690. doi:10.2147/opth.s58617
Margolis R, Spaide RF (2009) A pilot study of enhanced depth imaging optical coherence tomography of the choroid in normal eyes. Am J Ophthalmol 147:811–815. doi:10.1016/j.ajo.2008.12.008
Maruko I, Iida T, Sugano Y, Ojima A, Ogasawara M, Spaide RF (2010) Subfoveal choroidal thickness after treatment of central serous chorioretinopathy. Ophthalmology 117:1792–1799. doi:10.1016/j.ophtha.2010.01.023
Hua R, Liu L, Li C, Chen L (2014) Evaluation of the effects of photodynamic therapy on chronic central serous chorioretinopathy based on the mean choroidal thickness and the lumen area of abnormal choroidal vessels. Photodiagnosis Photodyn Ther 11(4):519–525. doi:10.1016/j.pdpdt.2014.07.005
Srinivasan VJ, Monson BK, Wojtkowski M, Bilonick RA, Gorczynska I, Chen R, Duker JS, Schuman JS, Fujimoto JG (2008) Characterization of outer retinal morphology with high-speed, ultrahigh-resolution optical coherence tomography. Invest Ophthalmol Vis Sci 49:1571–1579. doi:10.1167/iovs. 07-0838
Spaide RF, Curcio CA (2011) Anatomical correlates to the bands seen in the outer retina by optical coherence tomography: literature review and model. Retina 31:1609–1619. doi:10.1097/IAE.0b013e3182247535
Gharbiya M, Grandinetti F, Scavella V, Cecere M, Esposito M, Segnalini A, Gabrieli CB (2012) Correlation between spectral-domain optical coherence tomography findings and visual outcome after primary rhegmatogenous retinal detachment repair. Retina 32:43–53. doi:10.1097/IAE.0b013e3182180114
Itoh Y, Inoue M, Rii T, Hiraoka T, Hirakata A (2012) Significant correlation between visual acuity and recovery of foveal cone microstructures after macular hole surgery. Am J Ophthalmol 153:111.e.111–119.e111. doi:10.1016/j.ajo.2011.05.039
Watanabe K, Tsunoda K, Mizuno Y, Akiyama K, Noda T (2013) Outer retinal morphology and visual function in patients with idiopathic epiretinal membrane. JAMA Ophthalmol 131:172–177. doi:10.1001/jamaophthalmol.2013.686
Ojima Y, Tsujikawa A, Yamashiro K, Ooto S, Tamura H, Yoshimura N (2010) Restoration of outer segments of foveal photoreceptors after resolution of central serous chorioretinopathy. Jpn J Ophthalmol 54:55–60. doi:10.1007/s10384-009-0766-4
Ratanasukon M, Thongthong K, Bhurayanontachai P, Jirarattanasopa P (2013) Photoreceptor disruption in central serous chorioretinopathy treated by half-dose photodynamic therapy. Clin Ophthalmol 7:87–92. doi:10.2147/opth.s39584
Shinojima A, Kawamura A, Mori R, Fujita K, Yuzawa M (2011) Detection of morphologic alterations by spectral-domain optical coherence tomography before and after half-dose verteporfin photodynamic therapy in chronic central serous chorioretinopathy. Retina 31:1912–1920. doi:10.1097/IAE.0b013e3182252aa8
Fujita K, Shinoda K, Imamura Y, Matsumoto CS, Mizutani Y, Mizota A, Yuzawa M (2012) Correlation of integrity of cone outer segment tips line with retinal sensitivity after half-dose photodynamic therapy for chronic central serous chorioretinopathy. Am J Ophthalmol 154:579–585. doi:10.1016/j.ajo.2012.03.043
Piccolino FC, de la Longrais RR, Ravera G, Eandi CM, Ventre L, Abdollahi A, Manea M (2005) The foveal photoreceptor layer and visual acuity loss in central serous chorioretinopathy. Am J Ophthalmol 139:87–99. doi:10.1016/j.ajo.2004.08.037
Vasconcelos H, Marques I, Santos AR, Melo P, Pires I, Figueira J, de Abreu JF, Cachulo ML, Silva R (2013) Long-term chorioretinal changes after photodynamic therapy for chronic central serous chorioretinopathy. Graefes Arch Clin Exp Ophthalmol 251:1697–1705. doi:10.1007/s00417-013-2270-2
Silva RM, Ruiz-Moreno JM, Gomez-Ulla F, Montero JA, Gregorio T, Cachulo ML, Pires IA, Cunha-Vaz JG, Murta JN (2013) Photodynamic therapy for chronic central serous chorioretinopathy: a 4-year follow-up study. Retina 33:309–315. doi:10.1097/IAE.0b013e3182670fbe
Financial support
This study was supported by a grant from the Seoul National University Bundang Hospital Research Fund (grant number: 11-2012-017).
Conflicts of interest
No conflicting relationship exists for any author.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kim, YK., Ryoo, NK., Woo, S.J. et al. Comparison of visual and anatomical outcomes of half-fluence and half-dose photodynamic therapy in eyes with chronic central serous chorioretinopathy. Graefes Arch Clin Exp Ophthalmol 253, 2063–2073 (2015). https://doi.org/10.1007/s00417-014-2926-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-014-2926-6