
Abstract
Purpose
To analyse the long-term functional and morphological response of a specific choroidal neovascular membrane (CNV) phenotype to anti-vascular endothelial growth factor (VEGF) therapy.
Methods
Data from 30 eyes of 30 consecutive patients with subretinal fluid (SRF) and fibrovascular pigment epithelial detachment (PED) due to CNV on spectral-domain optical coherence tomography (SDOCT) with a follow-up of at least 20 months were retrospectively collected. Main outcome measures included change in visual acuity, quantitative and qualitative parameters on SDOCT [photoreceptor layer, outer nuclear layer (ONL), choroid, PED, SRF] and on fluorescein angiography (CNV activity). Subjects were divided into responders and non-responders based on morphological and functional aspects.
Results
An average number of 20.23 ± 9.9 anti-VEGF injections were administered during a mean follow-up of 40.25 ± 13.5 months. Fourteen eyes were categorized as morphological non-responders, 12 as functional non-responders and eight as complete non-responders. Complete non-responders were significantly younger than complete responders (68.5 ± 4.5 vs 74.3 ± 6.8 years; p < 0.05) and presented thinner baseline ONL values (68.43 ± 15.2 vs103.5 ± 32.8 μm; p < 0.05). Intermediate or large drusen as typical features for age-related macular degeneration (AMD) were less frequently present in complete non-responders; however, this was not statistically significant (62.5 % vs 91.7 %; p = 0.25).
Conclusions
Our preliminary findings indicate that eyes with the specific SDOCT phenotype with isolated fibrovascular PED and SRF frequently demonstrate non-response to anti-VEGF therapy, and the underlying disease mechanism may be different from AMD. Larger prospective trials are required to validate those results, and to develop strategies to improve the morphological as well as functional outcome.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Prior to the anti-vascular endothelial growth factor (VEGF) era, age-related macular degeneration (AMD) was the leading cause of legal blindness in patients older than 60 years in the industrialized world [1, 2]. Multiple clinical trials demonstrated that VEGF inhibition improves the prognosis of patients with neovascular AMD [3–6], as well as CNV secondary to other diseases than AMD [7–10]. Despite the success of anti-VEGF treatment across all CNV lesion subtypes, there is a subgroup of patients with decrease in visual acuity (VA) in clinical trials. In the MARINA trial, 8 % to 10 % of patients lost more than 15 letters at month 24, as well as 10 % of patients in the ANCHOR study [3, 11, 12].
Fluorescein angiography (FA) has been used to classify CNV into predominantly classic, minimally classic, and occult CNV lesion subtypes, and to assess the activity of CNV [13]. Within recent years, the noninvasive imaging technique optical coherence tomography (OCT) has become an important diagnostic tool for management of patients with neovascular AMD [14–17]. The spectral-domain OCT (SDOCT) technique provides high-resolution volume scans, allowing to perform detailed qualitative and quantitative analysis of various retinal and subretinal spaces [18–22]. FA and SDOCT images provide complementary information with regard to CNV lesions [22]. Morphological characteristics of active CNV on SDOCT include intraretinal cystoid spaces, SRF, subretinal hyperreflective material, and PED [22].
Many studies have been performed to identify SDOCT lesion characteristics, predicting the response to anti-VEGF therapy [20, 23–25]. Beside other parameters, PED and SRF have been reported to have prognostic value for the functional outcome, as larger PED size is demonstrated to have a negative prognostic value [23], and SRF is reported to be associated with recurrent disease activity [20]. Furthermore, fibrovascular PED lesions have been reported to show less morphological and functional response to anti-VEGF treatment than eyes with other CNV lesion subtypes [26–30]. It was also our clinical impression that eyes with a specific SDOCT phenotype with the isolated presence of fibrovascular PED and SRF frequently show a poor functional as well as morphological response to anti-VEGF injections. Therefore, treatment of these patients represents a challenge.
The purpose of this study was to analyze the morphological and functional response of patients with the specific SDOCT phenotype demonstrating SRF and PED, and to evaluate characteristics for non-response.
Methods
Data collection
For inclusion in the study, eyes were required to show fibrovascular PED (with possible serous component) and SRF due to CNV on SDOCT without evidence for cystoid spaces and subretinal hyperreflective material. The presence of occult CNV was confirmed using FA. Previous treatment for CNV was allowed. Only patients older than 50 years of age were included. Eyes with and without signs for AMD were eligible for this study. Patients with evidence of macular pathology other than AMD on FA (e.g., diabetic retinopathy, Irvine–Gass syndrome, central serous retinopathy, chorioretinitis, vitelliform lesions) were excluded. Our analysis was limited to patients with a minimum follow-up of 20 months.
Data from 30 eyes of 30 consecutive patients meeting the inclusion criteria were retrospectively collected from the database of the University of Cologne. Patients were generally treated with three initial monthly anti-VEGF injections using ranibizumab (Lucentis; Novartis AG, Basel, Switzerland) or bevacizumab (Avastin; Roche Pharma AG, Basel, Switzerland), followed by pro re nata (PRN) guided re-injections whenever signs for CNV activity were detected on funduscopy, SDOCT, or FA, or whenever a decrease in VA due to CNV was noted. If morphology and function was stable despite repeated injections, treatment was paused until a recurrent decrease in vision or increase in signs for CNV activity was detected. In eight cases, photodynamic therapy (PDT) with verteporfin (Visudyne; Novartis AG, Basel, Switzerland) was additionally performed during follow-up. At each visit, a comprehensive eye exam and SDOCT imaging (Spectralis SDOCT, Heidelberg Engineering, Heidelberg, Germany) was performed. SDOCT volume scans (4 × 6mm) centered on the fovea were captured with 37 parallel OCT B-Scans using the automated real-time (ART) function with 20 images averaged per B-Scan. FP and FA was obtained at baseline to evaluate the diagnosis, type of CNV, and CNV activity.
Type and date of treatments and best-corrected Snellen visual acuity (BCVA) were recorded for each patient. FP and FA images and SDOCT volume scans were collected at each available follow-up visit.
Image analysis
Trained graders at Cologne Image Reading Center and Laboratory (CIRCL) analyzed FP, FA, and SDOCT images. FP images at baseline were evaluated for the presence, number, and size of drusen. The presence of intermediate (≥63 μm) or large (≥125 μm) drusen within the Early Treatment Diabetic Retinopathy Study (ETDRS) grid was considered as signs for AMD. The CNV lesion subtype and activity was judged on FA at baseline.
SDOCT analysis at all available visits included the presence of SRF and PED, as well as the development of intraretinal cystoid spaces, outer retinal tubulations (ORTs) [31], or retinal pigment epithelial (RPE) tears. Additionally, the presence of a serous component of PED was noted at baseline, as well as a decrease in SRF after the three initial intravitreal injections.
Quantitative analysis was performed using the caliper function of the SDOCT viewer software. The maximum height of PED within the volume scan was measured at all available visits. The foveal center point (FCP) thickness of the outer nuclear layer (ONL), photoreceptor layer (PR), and the choroid was measured at baseline and last follow-up.
Definitions of morphological and functional response
Patients were divided into responders and non-responders based on morphological and functional aspects:
Morphological response was defined as the absence of intra- or subretinal fluid on SDOCT at any time during follow-up. Morphological non-response was considered, if persistent subretinal fluid was present at all available visits.
Functional response was defined as BCVA improvement of at least 2 lines at any time during the entire follow-up period. Patients who never showed a VA increase of 2 lines were classified as functional non-responders.
Patients with functional as well as morphological response were considered “complete responders”. Patients with functional as well as morphological non-response were considered “complete non-responders”.
Statistical methods
Snellen visual acuity was converted to logarithm of minimal angle of resolution visual acuity (logMAR) for the purposes of statistical analyses. Mann–Whitney U test, Fisher’s exact test and chi-squared test were used to compare the groups. All tests were 2-sided, and statistical significance was defined as p < 0.05. Statistical analysis was performed using commercially available software SPSS Version 21.0 (IBM Software and Systems, Armonk, NY, USA).
This study adhered to the tenets set forth in the Declaration of Helsinki.
Results
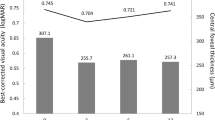
Of the 30 patients included in our analysis, 13 (43.3 %) were female and 17 (56.7 %) were male. The mean age of patients was 70.6 ± 7.3. FA at baseline demonstrated occult CNV in all patients at baseline. Intermediate or large drusen were noted in 25 cases in study eye. Mean BCVA improved from 0.32 ± 0.28 logMAR at baseline to 0.25 ± 0.20 logMAR after the initial three injections to 0.39 ± 0.32 logMAR at last follow-up. Table 1 shows the patient characteristics for responders and non-responders based on morphological and functional outcome parameters. In Table 2, features of “complete responders” and “complete non-responders” are compared.
Analysis based on morphological response
Sixteen patients demonstrated morphological response as defined above. A mean of 5.44 ± 2.80 injections (range 3–10) were required in this group before SRF completely disappeared. Fourteen patients showed persistent SRF during a mean follow-up of 38.49 ± 15.05 months and despite a mean of 7.05 ± 2.56 intravitreal injections per year.
Patients in the non-responder group were significantly younger than patients in the responder group (p < 0.05). There was a statistically significant difference between morphological responders and non-responders with regard to the number of patients with reduced SRF after the three initial anti-VEGF injections (p < 0.05, OR = 7.8, 95 % confidence interval 1.48–41.22), with most eyes in the responder group (13 out of 16 eyes, 80.2 %) showing reduced SRF after three initial injections, compared to only five out of 14 eyes (35.7 %) of non-responders.
Patients with morphological response showed more frequently intermediate or large drusen as typical AMD features (15 out of 16 eyes, 93.8 %) than patients with persistent SRF (ten out of 14 eyes, 71.4 %); however, this difference was not statistically significant (p = 0.16). Additionally, there was a trend for a higher number of mean injections per year (p = 0.09), thinner baseline ONL thickness (p = 0.11), greater baseline PED thickness (0.19), and a stronger decrease in choroidal thickness from baseline to the end of follow-up (p = 0.17) in the group of morphological non-responders.
None of the other baseline parameters showed significant differences between the group of morphological responders and non-responders. The incidence of RPE tears, development of intraretinal cystoid spaces, and ORTs were very few and uniformly distributed between both groups.
Analysis based on functional response
Eighteen patients were considered functional responders, with a BCVA increase of at least 2 lines at any time during follow-up. Mean baseline VA in this group was 0.36 ± 0.29 logMAR. During the mean follow-up of 41.15 ± 12.71 months, VA remained stable (mean VA at last visit 0.36 ± 0.28). Twelve patients never showed an increase in VA of at least 2 lines. Mean VA at baseline (0.25 ± 0.18) decreased by 1.8 ± 3.0 lines over a mean follow-up of 38.89 ± 15.08 months.
The number of injections needed to achieve absence of SRF was higher for functional non-responders (mean 8.00 ± 3.36) than for functional responders (mean 4.58 ± 2.11); however, this difference did not reach statistical significance (p = 0.08). Eyes in the responder group had higher PED thickness values at baseline compared to non-responders (p < 0.05), and non-responders demonstrated stronger decrease in PED height after the initial three injections (p < 0.05). None of the other parameters showed significant differences between both groups, although there was a trend for greater baseline choroidal thickness values (p = 0.07), lower baseline ONL thickness values (p = 0.07), and a stronger decrease in choroidal thickness between baseline and last follow-up (p = 0.10) in the non-responder group.
Characteristics of morphological and functional non-responders
There were eight patients without morphological and functional response as defined above. These patients were treated with a mean of 24.25 ± 15.43 injections over 41.78 ± 16.70 months follow-up. Mean injection rate was 6.74 ± 2.90 injections per year. Mean BCVA was 0.31 ± 0.29 logMAR at baseline, 0.31 ± 0.30 logMAR after the initial three injections, and 0.49 ± 0.37 logMAR at the end of follow-up. Twelve patients demonstrated morphological as well as functional response. BCVA in these patients was 0.35 ± 0.31 logMAR at baseline, 0.25 ± 0.19 logMAR after the three initial injections, and 0.38 ± 0.34 logMAR at the end of follow-up. Follow-up of one typical patient is presented in Fig. 1.

Patient with morphological and functional non-response. a + b Baseline fluorescein angiography shows low active occult choroidal neovascularisation with retinal pigment epithelium disturbance. c Baseline spectral-domain optical coherence tomography (SDOCT) with pigment epithelial detachment (PED) and subretinal fluid (SRF). Best-corrected visual acuity is 20/32 (Snellen). d SDOCT after 42 months following treatment with 30× ranibizumab, 1× bevacizumab, 1× photodynamic therapy with verteporfin. Best-corrected visual acuity is 20/63 (Snellen). * Outer nuclear layer (ONL) thickness measurement
Absolute non-responders were significantly younger than absolute responders (68.5 ± 4.5 versus 74.3 ± 6.8 years; p < 0.05). Baseline ONL was significantly thinner in absolute non-responders (103.5 ± 32.8 versus 68.43 ± 15.2 μm; p < 0.05).
Intermediate or large drusen as AMD features were less frequently observed in patients with non-response (five out of eight, 62.5 %) compared to responders (11 out of 12, 91.7 %); however, the difference was not statistically significant. There was a trend for higher baseline choroidal thickness (p = 0.07), stronger decrease in PR thickness (p = 0.07), and a lower rate of patients with decrease in SRF after the initial three injections (p = 0.16) in the group of non-responders. Other baseline parameters were not significantly different between groups.
Discussion
Anti-VEGF therapy has been shown to have a substantial effect on reducing the magnitude of legal blindness and visual impairment by 72 % within 2 years after diagnosis of CNV [6]. Although the prognosis of patients with CNV has dramatically improved, there is a subgroup of patients in all clinical trials with poor response to anti-VEGF therapy [3, 11, 12]. Patients with continuous VA loss and persistent CNV activity despite regular treatments pose a challenge to clinicians. It was our clinical impression that patients with a specific SDOCT phenotype with isolated SRF and PED frequently demonstrate functional as well as morphological non-response. In this study, we analyzed the outcome of these patients, and identified prognostic factors for the response to anti-VEGF therapy.
Twenty-seven percent of patients demonstrated neither functional nor morphological response as defined above over the entire follow-up period. ONL thickness of the complete responder group (mean FCP ONL thickness 103.5 μm) was comparable with the findings of Pappuru et al.[32] in eyes with dry AMD (mean FCP ONL thickness 104.3 μm), while ONL thickness was significantly thinner for complete non-responders (mean FCP ONL thickness 68.4 μm). Thinner ONL values in the non-responder group may indicate damage to the outer retina, possibly due to chronic exudation in the past. In line with this, a thinner ONL at baseline was reported to be a prognostic factor for poorer VA outcome following anti-VEGF therapy [23]. Additionally, there was a trend for a more severe decrease in PR thickness during follow-up in the non-responder group, which may be explained by the continuous presence of SRF in this group. As a result of chronic disease, patients may have developed restricted RPE pump function. Consequently, SRF cannot be resorbed adequately, and may persist despite regular anti-VEGF therapy. Further, multiple minor breaks within the RPE may develop, resulting in a less effective outer retinal barrier.
Morphological non-responders showed intermediate or large drusen on the study eye less frequently than morphological responders, even though this difference did not reach statistical significance, possibly because of the small number of patients. Furthermore, absolute as well as morphological non-responders were significantly younger than responders. These observations may indicate that the underlying disease mechanism for CNV development and persistence of SRF in our non-responsive cases may be different from typical AMD.
Beside neovascular AMD, PED and SRF are also seen in eyes with central serous retinopathy (CSR) and pseudovitelliform lesions [33, 34]. Thus, these diseases may be mistaken for active neovascular AMD, and may be non-responsive to anti-VEGF therapy. Fluorescein angiography may be helpful to distinguish those from CNV. Vitelliform macular dystrophies typically present with subfoveal yellowish lesions, which correspond to areas of blocked fluorescence in the early phase of fluorescein angiography, with staining in the late phase [35]. SD-OCT shows subretinal hyperreflective material [34]. Eventually the subretinal material disappears over time, leaving an empty subretinal hyporeflective space behind [34, 35]. In our study, eyes with subretinal hyperreflective material and eyes with features suggestive for vitelliform lesions have not been included. However, we cannot fully exclude the possibility that some patients have a vitelliform macular dystrophy with complete absence of subretinal material and secondary occult CNV.
CSR frequently occurs in young and middle-aged individuals. In chronic CSR, severe visual loss may occur due to retinal atrophy [36]. In addition, secondary development of occult CNV may occur [37]. In eyes with angiographically occult CNV and PED as well as SRF on SDOCT, it may be difficult to distinguish between AMD and CSR as the underlying disease mechanism. AMD may be more likely in older patients and the presence of drusen, CSR may be more likely in younger patients, and the presence of multifocal areas of RPE disturbance on FA or fluorescein leakage in the typical smoke stack shape. Those FA features of CSR have not been detected in our patients. On SDOCT, eyes with CSR frequently present greater choroidal thickness than eyes with AMD [38–41]. In our study, complete non-responders had a slightly thicker choroid at baseline in comparison to complete responders; however, this did not reach statistical significance. It remains to be shown if SRF in patients with CSR and occult CNV may be less responsive to anti-VEGF therapy than that in eyes with neovascular AMD.
Kloos et al. analyzed the effect of PDT in a small group of non-responders to anti-VEGF treatment with isolated SRF, and demonstrated stabilization in VA following PDT [42]. In some of our patients (n = 5) with morphological non-response, PDT has been performed as an alternative treatment option; however, our study population is too small to draw clear conclusions.
Various anti-VEGF agents may show differences regarding the response of morphological parameters [43]. Possible explanations include differences in binding affinity to VEGF or in molecular size. Further, tachyphylaxis is a possible reason for late non-response to anti-VEGF treatment [21, 44, 45]. Switching to another anti-VEGF drug may be favourable for patients with attenuated response [46]. Recently, the recombinant fusion protein aflibercept, which binds all isomers of the VEGF-A family and placental growth factor, was reported to achieve improved anatomical outcomes in patients with non-response to ranibizumab [47–49], including a rapid response of subretinal and sub-RPE fluid in eyes with PEDs [47, 50]. Thus, non-responsive patients in our group may be favourable for the transition to this anti-VEGF agent. In our study, a decrease in SRF after the initial three anti-VEGF injections was less frequent in patients showing persistence of SRF at some point during follow-up. A lack of initial response of SRF may therefore help to identify patients that may benefit from transition, although there was no difference with regard to functional response in our study.
Various studies have analysed prognostic factors for VA outcome in neovascular AMD [11, 12, 23, 24, 51]. These studies indicate that eyes with lower baseline VA may demonstrate a greater increase in vision, but nevertheless still show lower VA values at last follow-up. In our study, initial VA was not different between responders and non-responders. Larger retinal thickness values at baseline have been reported to be associated with greater increase in VA [23]. In our dataset, eyes with cystoid spaces were excluded, and thus retinal thickness was low. This may partially explain the lack of strong increase in VA during follow-up.
Our study has several limitations, including its retrospective design, the use of Snellen VA, the use of PDT in some cases, the small study population, and the lack of a control group. In addition, our study was not designed to draw conclusions about the frequency of the described SDOCT phenotype. Comparison between our study and results from larger clinical trials such as MARINA are limited, as CNV lesion subtypes in our study are based on SDOCT instead of FA. Whereas occult and minimally classic CNV lesion subtypes were included in the MARINA trial, our study population presents a subtype of occult CNV.
In summary, our results indicate that eyes with the specific SDOCT phenotype with isolated fibrovascular PED and SRF frequently demonstrate non-response to anti-VEGF therapy. Although our study group was small, we could identify younger age and lower ONL thickness as risk factors for morphological as well as functional non-response in this group. A lack of initial decrease in SRF appeared to be more frequent in patients with persistence of SRF during follow-up. The non-response to anti-VEGF therapy may be attributed to several reasons (e.g., persistence of fluid due to restricted RPE pump function or RPE breaks in chronic disease, undertreatment, tachyphylaxis), or may indicate that the underlying disease mechanism is different from neovascular AMD. Possible beneficial effects from switching to other treatment options such as PDT or aflibercept remain to be demonstrated. These preliminary findings should be evaluated in a larger prospective study to elucidate the reason for frequent non-response of eyes with PED and SRF to anti-VEGF therapy, and to develop strategies to improve the morphological as well as functional outcome.
References
Bressler NM, Bressler SB, Congdon NG, Ferris FL 3rd, Friedman DS, Klein R, Lindblad AS, Milton RC, Seddon JM, Age-Related Eye Disease Study Research G (2003) Potential public health impact of age-related eye disease study results: AREDS report no. 11. Arch Ophthalmol 121:1621–1624
Shah AR, Del Priore LV (2009) Natural history of predominantly classic, minimally classic, and occult subgroups in exudative age-related macular degeneration. Ophthalmology 116:1901–1907
Brown DM, Kaiser PK, Michels M, Soubrane G, Heier JS, Kim RY, Sy JP, Schneider S, Group AS (2006) Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med 355:1432–1444
Rosenfeld PJ, Brown DM, Heier JS, Boyer DS, Kaiser PK, Chung CY, Kim RY, Group MS (2006) Ranibizumab for neovascular age-related macular degeneration. N Engl J Med 355:1419–1431
Comparison of Age-related Macular Degeneration Treatments Trials Research G, Martin DF, Maguire MG, Fine SL, Ying GS, Jaffe GJ, Grunwald JE, Toth C, Redford M, Ferris FL 3rd (2012) Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: Two-year results. Ophthalmology 119:1388–1398
Bressler NM, Doan QV, Varma R, Lee PP, Suner IJ, Dolan C, Danese MD, Yu E, Tran I, Colman S (2011) Estimated cases of legal blindness and visual impairment avoided using ranibizumab for choroidal neovascularization: Non-hispanic white population in the United States with age-related macular degeneration. Arch Ophthalmol 129:709–717
Konstantinidis L, Mantel I, Pournaras JA, Zografos L, Ambresin A (2009) Intravitreal ranibizumab (Lucentis) for the treatment of myopic choroidal neovascularization. Graefes Arch Clin Exp Ophthalmol 247:311–318
Lai TY, Chan WM, Liu DT, Lam DS (2009) Intravitreal ranibizumab for the primary treatment of choroidal neovascularization secondary to pathologic myopia. Retina 29:750–756
Mones JM, Amselem L, Serrano A, Garcia M, Hijano M (2009) Intravitreal ranibizumab for choroidal neovascularization secondary to pathologic myopia: 12-month results. Eye (Lond) 23:1275–1280, quiz 1281
Nguyen QD, Shah SM, Hafiz G, Do DV, Haller JA, Pili R, Zimmer-Galler IE, Janjua K, Symons RC, Campochiaro PA (2008) Intravenous bevacizumab causes regression of choroidal neovascularization secondary to diseases other than age-related macular degeneration. Am J Ophthalmol 145:257–266
Boyer DS, Antoszyk AN, Awh CC, Bhisitkul RB, Shapiro H, Acharya NR, Group MS (2007) Subgroup analysis of the MARINA study of ranibizumab in neovascular age-related macular degeneration. Ophthalmology 114:246–252
Rosenfeld PJ, Shapiro H, Tuomi L, Webster M, Elledge J, Blodi B, MARINA and ANCHOR Groups (2011) Characteristics of patients losing vision after 2 years of monthly dosing in the phase III ranibizumab clinical trials. Ophthalmology 118:523–530
Barbazetto I, Burdan A, Bressler NM, Bressler SB, Haynes L, Kapetanios AD, Lukas J, Olsen K, Potter M, Reaves A, Rosenfeld P, Schachat AP, Strong HA, Wenkstern A, Treatment of Age-Related Macular Degeneration with Photodynamic Therapy Study G, Verteporfin in Photodynamic Therapy Study G (2003) Photodynamic therapy of subfoveal choroidal neovascularization with verteporfin: Fluorescein angiographic guidelines for evaluation and treatment—TAP and VIP report No. 2. Arch Ophthalmol 121:1253–1268
Kaiser PK, Brown DM, Zhang K, Hudson HL, Holz FG, Shapiro H, Schneider S, Acharya NR (2007) Ranibizumab for predominantly classic neovascular age-related macular degeneration: subgroup analysis of first-year ANCHOR results. Am J Ophthalmol 144:850–857
Fung AE, Lalwani GA, Rosenfeld PJ, Dubovy SR, Michels S, Feuer WJ, Puliafito CA, Davis JL, Flynn HW Jr, Esquiabro M (2007) An optical coherence tomography-guided, variable dosing regimen with intravitreal ranibizumab (Lucentis) for neovascular age-related macular degeneration. Am J Ophthalmol 143:566–583
Lalwani GA, Rosenfeld PJ, Fung AE, Dubovy SR, Michels S, Feuer W, Davis JL, Flynn HW Jr, Esquiabro M (2009) A variable-dosing regimen with intravitreal ranibizumab for neovascular age-related macular degeneration: Year 2 of the PrONTO study. Am J Ophthalmol 148(43–58):e41
Keane PA, Patel PJ, Liakopoulos S, Heussen FM, Sadda SR, Tufail A (2012) Evaluation of age-related macular degeneration with optical coherence tomography. Surv Ophthalmol 57:389–414
Joeres S, Tsong JW, Updike PG, Collins AT, Dustin L, Walsh AC, Romano PW, Sadda SR (2007) Reproducibility of quantitative optical coherence tomography subanalysis in neovascular age-related macular degeneration. Invest Ophthalmol Vis Sci 48:4300–4307
Witkin AJ, Vuong LN, Srinivasan VJ, Gorczynska I, Reichel E, Baumal CR, Rogers AH, Schuman JS, Fujimoto JG, Duker JS (2009) High-speed ultrahigh resolution optical coherence tomography before and after ranibizumab for age-related macular degeneration. Ophthalmology 116:956–963
Golbaz I, Ahlers C, Stock G, Schutze C, Schriefl S, Schlanitz F, Simader C, Prunte C, Schmidt-Erfurth UM (2011) Quantification of the therapeutic response of intraretinal, subretinal, and subpigment epithelial compartments in exudative AMD during anti-VEGF therapy. Invest Ophthalmol Vis Sci 52:1599–1605
Keane PA, Liakopoulos S, Ongchin SC, Heussen FM, Msutta S, Chang KT, Walsh AC, Sadda SR (2008) Quantitative subanalysis of optical coherence tomography after treatment with ranibizumab for neovascular age-related macular degeneration. Invest Ophthalmol Vis Sci 49:3115–3120
Liakopoulos S, Ongchin S, Bansal A, Msutta S, Walsh AC, Updike PG, Sadda SR (2008) Quantitative optical coherence tomography findings in various subtypes of neovascular age-related macular degeneration. Invest Ophthalmol Vis Sci 49:5048–5054
Ristau T, Hillebrand S, Smailhodzic D, Walsh AC, Kirchhof B (2013) Prognostic factors for long term visual acuity outcome after ranibizumab therapy in patients with neovascular age-related macular degeneration. J Clin Exp Ophthalmol 4:264
Singh RP, Fu EX, Smith SD, Williams DR, Kaiser PK (2009) Predictive factors of visual and anatomical outcome after intravitreal bevacizumab treatment of neovascular age-related macular degeneration: an optical coherence tomography study. Br J Ophthalmol 93:1353–1358
Ritter M, Elledge J, Simader C, Deak GG, Benesch T, Blodi BA, Schmidt-Erfurth UM (2011) Evaluation of optical coherence tomography findings in age-related macular degeneration: A reproducibility study of two independent reading centres. Br J Ophthalmol 95:381–385
Avery RL, Pieramici DJ, Rabena MD, Castellarin AA, Nasir MA, Giust MJ (2006) Intravitreal bevacizumab (Avastin) for neovascular age-related macular degeneration. Ophthalmology 113:363.e365–372.e365
Spaide RF, Laud K, Fine HF, Klancnik JM Jr, Meyerle CB, Yannuzzi LA, Sorenson J, Slakter J, Fisher YL, Cooney MJ (2006) Intravitreal bevacizumab treatment of choroidal neovascularization secondary to age-related macular degeneration. Retina 26:383–390
Heier JS, Antoszyk AN, Pavan PR, Leff SR, Rosenfeld PJ, Ciulla TA, Dreyer RF, Gentile RC, Sy JP, Hantsbarger G, Shams N (2006) Ranibizumab for treatment of neovascular age-related macular degeneration: a phase I/II multicenter, controlled, multidose study. Ophthalmology 113(633):e631–e634
Freeman WR, Kozak I, Yuson RM, Nigam N, Cheng L, Mojana F (2011) Prognosti implications of pigment epithelial detachment in bevacizumab (avastin)-treated eyes with age-related macular degeneration and choroidal neovascularization. Retina 31:1812–1818
Veritti D, Macor S, Menchini F, Lanzetta P (2013) Effects of VEGF inhibition on retinal morphology, neovascular network size, and visual acuity in patients with vascularized pigment epithelium detachment because of occult choroidal neovascularization. Retina 33:982–989
Zweifel SA, Engelbert M, Laud K, Margolis R, Spaide RF, Freund KB (2009) Outer retinal tubulation: A novel optical coherence tomography finding. Arch Ophthalmol 127:1596–1602
Pappuru RR, Ouyang Y, Nittala MG, Hemmati HD, Keane PA, Walsh AC, Sadda SR (2011) Relationship between outer retinal thickness substructures and visual acuity in eyes with dry age-related macular degeneration. Invest Ophthalmol Vis Sci 52:6743–6748
Hee MR, Puliafito CA, Wong C, Reichel E, Duker JS, Schuman JS, Swanson EA, Fujimoto JG (1995) Optical coherence tomography of central serous chorioretinopathy. Am J Ophthalmol 120:65–74
Spaide RF, Noble K, Morgan A, Freund KB (2006) Vitelliform macular dystrophy. Ophthalmology 113:1392–1400
Brecher R, Bird AC (1990) Adult vitelliform macular dystrophy. Eye (Lond) 4(Pt 1):210–215
Gass JD (1967) Pathogenesis of disciform detachment of the neuroepithelium. Am J Ophthalmol 63(Suppl):1–139
Loo RH, Scott IU, Flynn HW Jr, Gass JD, Murray TG, Lewis ML, Rosenfeld PJ, Smiddy WE (2002) Factors associated with reduced visual acuity during long-term follow-up of patients with idiopathic central serous chorioretinopathy. Retina 22:19–24
Imamura Y, Fujiwara T, Margolis R, Spaide RF (2009) Enhanced depth imaging optical coherence tomography of the choroid in central serous chorioretinopathy. Retina 29:1469–1473
Kim YT, Kang SW, Bai KH (2011) Choroidal thickness in both eyes of patients with unilaterally active central serous chorioretinopathy. Eye (Lond) 25:1635–1640
Kuroda S, Ikuno Y, Yasuno Y, Nakai K, Usui S, Sawa M, Tsujikawa M, Gomi F, Nishida K (2013) Choroidal thickness in central serous chorioretinopathy. Retina 33:302–308
Chung SE, Kang SW, Lee JH, Kim YT (2011) Choroidal thickness in polypoidal choroidal vasculopathy and exudative age-related macular degeneration. Ophthalmology 118:840–845
Kloos P, Niederberger H, Valmaggia C (2011) Photodynamic therapy in “secondary sick RPE syndrome” after repeated intravitreal injections of VEGF inhibitors in patients with wet age-related macular degeneration. Klin Monatsbl Augenheilkd 228:340–344
Joeres S, Kaplowitz K, Brubaker JW, Updike PG, Collins AT, Walsh AC, Romano PW, Sadda SR (2008) Quantitative comparison of optical coherence tomography after pegaptanib or bevacizumab in neovascular age-related macular degeneration. Ophthalmology 115:347.e342–354.e342
Eghoj MS, Sorensen TL (2012) Tachyphylaxis during treatment of exudative age-related macular degeneration with ranibizumab. Br J Ophthalmol 96:21–23
Forooghian F, Cukras C, Meyerle CB, Chew EY, Wong WT (2009) Tachyphylaxis after intravitreal bevacizumab for exudative age-related macular degeneration. Retina 29:723–731
Gasperini JL, Fawzi AA, Khondkaryan A, Lam L, Chong LP, Eliott D, Walsh AC, Hwang J, Sadda SR (2012) Bevacizumab and ranibizumab tachyphylaxis in the treatment of choroidal neovascularisation. Br J Ophthalmol 96:14–20
Patel KH, Chow CC, Rathod R, Mieler WF, Lim JI, Ulanski LJ 2nd, Leiderman YI, Arun V, Chau FY (2013) Rapid response of retinal pigment epithelial detachments to intravitreal aflibercept in neovascular age-related macular degeneration refractory to bevacizumab and ranibizumab. Eye (Lond) 27:663–667, quiz 668
Yonekawa Y, Andreoli C, Miller JB, Loewenstein JI, Sobrin L, Eliott D, Vavvas DG, Miller JW, Kim IK (2013) Conversion to aflibercept for chronic refractory or recurrent neovascular age-related macular degeneration. Am J Ophthalmol 156(29–35):e22
Bakall B, Folk JC, Boldt HC, Sohn EH, Stone EM, Russell SR, Mahajan VB (2013) Aflibercept therapy for exudative age-related macular degeneration resistant to bevacizumab and ranibizumab. Am J Ophthalmol 156:15.e11–22.e11
Kumar N, Marsiglia M, Mrejen S, Fung AT, Slakter J, Sorenson J, Freund KB (2013) Visual and anatomical outcomes of intravitreal aflibercept in eyes with persistent subfoveal fluid despite previous treatments with ranibizumab in patients with neovascular age-related macular degeneration. Retina 33(8):1605–1612
Hirami Y, Mandai M, Takahashi M, Teramukai S, Tada H, Yoshimura N (2009) Association of clinical characteristics with disease subtypes, initial visual acuity, and visual prognosis in neovascular age-related macular degeneration. Jpn J Ophthalmol 53:396–407
Acknowledgments
Supported in part by Ilse Palm-Foundation, Germany
Conflict of Interest
Lebriz Ersoy: none, Tina Ristau: none, Sandra Liakopoulos served as a consultant for Novartis Pharma and received honoraria from Novartis Pharma, Bernd Kirchhof: none
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ersoy, L., Ristau, T., Kirchhof, B. et al. Response to anti-VEGF therapy in patients with subretinal fluid and pigment epithelial detachment on spectral-domain optical coherence tomography. Graefes Arch Clin Exp Ophthalmol 252, 889–897 (2014). https://doi.org/10.1007/s00417-013-2519-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-013-2519-9