
Abstract
Background
To study the demography, various morphological patterns and fluid dynamics of the smokestack leak by fluorescein angiography (FA) in central serous chorioretinopathy (CSC).
Methods
Part I (clinical): review of the medical records and angiographic documents of 69 consecutive cases of CSC with smokestack leak. Part II (experimental): documentation of the movement of various concentrations of fluorescein dye due to convection currents in a laboratory model that roughly represents a closed chamber similar to that of CSC in human eyes.
Results
The clinical study (Part I) revealed that 14.40% of 479 consecutive cases had smokestack leak, of which 70% occurred in first acute episode (p-value: <0.001), 27.14% in acute recurrent episodes (50% fresh leak) and 2.85% in chronic stage. Patients were predominantly male (84.05%) with a median age of 34.00 ± 8.14 years. The median symptom duration excluding the chronic cases was 15 ± 34.28 days. This type of leak was mostly (48.57%) seen in medium-sized CSC, and the majority were in the parafoveal superonasal quadrant (31.42%). The ascending type of leak was predominant (94.28%). In four eyes, an atypical pattern and in two eyes more than one smokestack leak were seen within the same detached area. The experimental study (Part II) demonstrated that fluid containing a low concentration of fluorescein ascended due to convection currents, whereas highly concentrated dye descended.
Conclusions
The clinical study revealed smokestack leaks to be significantly more common in a primary acute episode, and they usually develop in the early part of the acute phase of the disease (average duration 15 ± 34.28 days). Rarely, this type of leak can occur in the chronic stage, and multiple leaks may develop in the same detached space. The various patterns of dye movement due to convection currents in the experimental model resembled the dye movement in certain cases of CSC of the present series. The experimental study also hinted at the probability of drainage of unbound fluorescein molecules along with protein-laden heavy fluid in downward spread of the leak.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Part I: Clinical study
Introduction
In 1961, Novotny and Alvis [1] perfected the technique of fluorescein angiography (FA) to study the human retinal circulation, which led to better understanding of many retinal diseases including central serous chorioretinopathy (CSC). In this particular disease, FA revealed leaks in retinal pigment epithelium (RPE), which are seen in about 95% of all cases of all types of this ailment [2]. Of the varied angiographic manifestations, smokestack leak is considered to be the classic CSC leak. Although Shimizu and Tobari in 1971 [3] drew the attention of the ophthalmic fraternity to this type of leak, interestingly they did not coin this term. They described it as “upward diffusion” of fluorescein dye. In 1973, Wessing [4] described it as “fluorescein flag”, though he found a similarity of this leak with that of smoke arising from a chimney, whereas Burton’s article [5] which was published 1 year earlier had the mention of “smokestack” or “vertical appearing leak”. This type of leak usually manifests itself as a point leak from the RPE at the arterio–venous or early venous phase of the angiography, which gradually increases in size during the mid-phase and begins to ascend; and after reaching a certain height, the dye sometimes extends either nasally or temporally in such a way that it resembles a smokestack. But often the ascending column of the dye on the top level spreads in all directions, resembling a mushroom or umbrella. Some investigators [3, 6] have documented change in direction of the ascending dye on change of posture of the patient. It has also been observed that in general, sensory retinal detachments (SRD) having this type of leak was larger than those with other types of focal leak [7]. Rarely, the dye spreads inferiorly or horizontally [6, 8]. The reported prevalence of smokestack leak in literature varies from 7% to 29% [3, 4, 6, 9, 10]. Review of literature revealed that certain aspects of fluid dynamics of this phenomenon still remain unanswered, and the facts that require attention are:
-
(1)
Why does each and every case of acute CSC not develop “smokestack leak”?
-
(2)
Why does the dye spread in horizontal and downward direction in some cases in spite of patient being in erect posture?
-
(3)
Why, in some cases, does the dye ascend initially vertically, but then move upwards in an irregular pattern?
-
(4)
Why does the speed of entry of dye differ?
-
(5)
What is the role of convection current?
-
(6)
Is it possible to have different concentrations of protein /or different density of fluid within the detached space? If so, how can it be explained?
Keeping these queries in mind, this study (Part I) in addition to the demographic data analysis, aims at understanding the fluid dynamics of the smokestack phenomenon in clinical cases by analyzing the various morphological patterns on FA and the probable risk factors.
Methods and materials
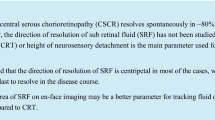
For the present study, we define “smokestack leak” as a stream-like spread of the fluorescein dye on FA in the sub-sensory retinal space through a leaking point in the attached/detached RPE, irrespective of its size, ultimate shape or direction of spread. A leak was considered to be vertical when it initially moved upwards, horizontal when it moved in the horizontal direction away from the upper limit of detachment without any significant vertical spread, and downward when the column of the dye descended from the leaking point. Acute CSC was defined as a blister-like serous detachment usually occurring in the macular area with angiographic evidence of single or multiple leaks in the RPE in absence of any evidence of inflammation, degeneration, or tumor in the choroid, and with signs and symptoms lasting not more than 6 months. Acute CSC could be primary (first acute episode) or recurrent acute episodes. This study has followed the classification of CSC into single resolving, recurrent resolving, recurrent chronic and chronic type based on its clinical course, which had been documented earlier [11]. As regards the size of CSC, Fig. 1 shows the various reference sizes and the geometrical calculations on which these sizes were based. When the detached area had an oval shape or slightly irregular configuration, the longest dimension of the detachment was taken into consideration. Figure 2 shows the empirical division of various quadrants of the central fundus for location of leaks and PEDs. The area within the vascular arcade was empirically divided into four quadrants with the intersecting axes at the foveola, leaving a central circular area covering the foveal avascular zone (FAZ). The four quadrants were again divided into two parts by drawing a circle around the FAZ with a radius of one disc diameter in the horizontal meridian. This zone was considered to be the parafoveal zone (PFZ).

Shows the reference sizes of small (a), medium (b) and big (c) CSCs. d shows the geometric measurements. The ‘small’ detachment had a radius of one disc diameter in the horizontal axis around the geometric centre of the detachment, the ‘medium’ had in between one and two disc diameters, and the ‘big’ had more than two disc diameters

Shows the division of the area between the vascular arcades of the fundus for location of the various types of RPE leaks and PEDs, with the intersecting axes at the foveola, leaving the foveal avascular zone (FAZ). The ultimate divisions are foveal avascular zone (FAZ), parafoveal superior nasal (PFSN), parafoveal superior temporal (PFST), parafoveal inferior nasal (PFIN), parafoveal inferior temporal (PFIT), superior nasal (SN), superior temporal (ST), inferior nasal (IN), and inferior temporal (IT) zones
The cases with smokestack leak in CSC as defined for this study, irrespective of previous laser treatment, were selected for detailed analysis. It total, 479 of 567 cases of CSC attending the “Pragjyoti Eye Care Centre”, Guwahati, India from January 1998 to June 2008 had undergone fluorescein angiography. Of these, 69 cases (14.40%) had been identified with smokestack phenomenon. One of these cases had bilateral smokestack leak. Cases with an old history of CSC without any symptoms related to it, and associated retinal vascular disease that may adversely affect the function of macula, were excluded from the study. Hence, to avoid confusion, one case with diabetic maculopathy having co-incidental CSC with a downward spread of dye was also excluded.
Eyes having smokestack phenomenon were analyzed with special emphasis to age, sex, laterality, primary/recurrent CSC, size of CSC, duration of symptom, location of the leak, leak from undetached RPE or from PED, leak from previously laser treated area, direction of flow of fluid and the varied morphology of the spreading stream of the dye. All the cases had comprehensive ophthalmological examination by slit-lamp biomicroscopy, red-free fundus photography and fluorescein angiography (Kowa RC-XV3, Japan). While doing FA, during the last 4 years of the study period, the cases with smokestack leak were followed up for half an hour.
This study had the approval of the “Ethics Committee” of the Institute.
Statistical analysis
Data were processed using SPSS 11.5 for Windows. Median as a measure of central tendency was preferred to avoid extreme values in case of duration data. The Chi-square statistic was used to test for the significance of proportions for different types of CSC. While analyzing the risk factors, the Z-test for difference of proportions was used, considering only the recorded cases.
Results and observations
The various salient features of smokestack phenomenon and analysis of its probable risk factors are presented in Tables 1, 2, 3. The median age of the patients with smokestack leak was found to be 34 ± 8.14 years. This type of leak was found to be more common in the first acute (primary) episode of the disease (70%) than in the recurrent acute episodes (27.14%). In recurrent acute cases, 50% of the leaks occurred with fresh RPE rent, either from the undetached RPE (25%) or from the previously present non-leaking PED (25%). Most of the leaks were of typical ascending type (94.28%), though the size and extent of the dye spread varied (Fig. 3). As regards the location of smokestack leak, the para-foveal superonasal area as defined for the present study had the maximum number of leaks. The leak was found to arise from PED in 25.71% of affected eyes, and the leakage usually occurred through a micro rent in the detached RPE, or as profuse leakage from all the decompensated cells. (Fig. 4). The smokestack leaks were mostly seen in medium-sized CSC. As regards the risk factors, only the difference of proportion for mental strain was found to be significantly high (Table 3), but it could not be a specific risk factor for smokestack leak, as CSC itself is a stress-related disease.

a A small smokestack leak. b A fairly large column of dye ascending upwards. Both cases had medium sized CSC

a The angiogram of a male patient aged 44 years with recurrent acute CSC of 7 days duration, showing a smokestack leak arising from a rip in the RPE at the margin of a PED. b The angiogram of a female patient aged 30 years having almost identical size of CSC and a PED inside the CSC. All the detached cells of this PED are leaking profusely, whereas the PED outside the detachment is not leaking at all
In this series, we observed two cases of CSC with more than one smokestack leak within the same detached area (Figs. 5 & 6). Both the cases had recurrent acute episodes. In two primary cases, two adjacent point leaks were found to enlarge and coalesce, which then ascended as a single smokestack leak.

Shows the FA findings for a 40-year-old patient on his fifth recurrence of acute CSC in the right eye since 4 days. The main ascending leak is from a PED inside the CSC, and the second leak is from a previously laser treated spot or a point adjacent to it. It started developing after about 10 minutes of dye injection, and by 20 minutes it took the present shape

Shows FA findings of the right eye of a patient aged 43 years having recurrence of CSC 16.50 years after the primary episode. Duration of the recurrent episode was 20 days. He had three adjacent point leaks just below the FAZ. The main ascending leak was from the central point leak, but in late phase, two faint columns of dye ascending from the adjacent spots could be appreciated (arrows). Patient had a smokestack leak from a point above FAZ in the primary episode, which was treated by laser and never recurred in that spot
The morphological variation was seen in four eyes of four patients (5.71%) with smokestack phenomenon. In three eyes, the dye was found to spread upwards in a zig zag manner which appeared to be due to spiraling /twisting of the ascending column (Figs. 7 & 8). In another eye, the ascending column of the dye developed a double umbrella type of spread (Fig. 9) resembling the column of smoke arising from an exploded bomb.

Findings of a patient with chronic recurrent type of CSC showing a spiraled ascending column of dye (b) arising from a central point leak (a). c The diagrammatic presentation of the ascending column of the dye

a The bifurcation, twist and upward deviation of the column of the dye. b The diagrammatic presentation of the main column of the dye. c The late phase of the angiogram, showing widening of the column of the dye due to diffusion

FA findings for a 37-year-old patient with first acute episode of 3 days duration. a An ascending leak from upper margin of FAZ and a PED below it. b The late-phase findings for the same eye showed no change in the PED, but the upper leak developed a double umbrella type of spread of dye (arrows). This is a late-phase photograph; the dye had already diffused from the main column, making the picture slightly fuzzy
This series had a 52-year-old case who had a profuse dye leakage from all the detached RPE of a PED in CSC on his first visit, and was found to have a smokestack leak from the same PED on his subsequent visit after 65 days.
This series had two cases of CSC, which developed smokestack leak even in the chronic stage. One of them, aged 45 years, had a SRD of 7 months duration. FA revealed a slowly ascending plume of dye which faded away within 8 minutes. The other case was 22 years old, who came to us with CSC of 18 months duration. This case also had a slowly ascending column of dye.
Discussion
As has been mentioned earlier, the prevalence of smokestack leak in CSC in the literature varies from 7% to 29%. Variation in prevalence rate of any condition usually occurs due to lack of uniformity of the definition of that particular condition, or due to geographic environmental factors or ethnic variation. The definition of smokestack leak in the present study encompasses all possible morphological variations of the leak, and the prevalence rate turned out to be 14.40%.
This study has revealed that fresh RPE leaks are usually required for the development of smokestack leak, as the leaks are seen in 70% of the cases with primary episode (p-value: <0.001 — Chi-square statistic). It has also been observed that in recurrent acute cases, 50% of the leaks occur with fresh RPE rent, either from the undetached RPE (25%) or from the previously present non-leaking PED (25%). This finding also deserves attention, as it indicates that the smokestack leak requires a fresh RPE micro-rent, which is likely to be wider than the chronic leaking points. These leaks were mostly seen in the para-foveal superonasal area as defined for the present study. Earlier studies [3, 4, 7, 10] also found a preponderance of all types of RPE leaks in this area. It is difficult to explain why this particular area is vulnerable to the development of RPE leaks. An increased hydrodynamic stress [12] and/or lack of sodium/potassium adenosine triphosphatase (Na/K ATPase) pump in this location [13] might be responsible for it. Friberg and Campagna [7] observed that cases associated with smokestack leak had significantly larger detachments than those with round focal leaks, but they did not specifically mention how big these detachments were. They believed that profuse smokestack leaks were invariably present in extensive serous detachments. One earlier report [5] also had a similar view. The present series found it to be more common in medium-sized CSCs as defined for this study, and also observed that unusually large CSCs were less frequent than medium-sized ones (Table 1). Though rare, this type of leak was also seen in small CSCs. So, it is not necessary that smokestack leak invariably leads to a huge detachment. The present study found this type of leak to occur mostly within 6 weeks of the acute phase of the disease. But amazingly, this phenomenon was also observed in two chronic cases. The presence of smokestack phenomenon beyond the usual period of recovery indicates either continuation of the pathological process in a sub-acute manner, or impending recurrence of the acute episode.
To understand the fluid dynamics of this phenomenon, we will have to explore the basic pathophysiology of CSC. This ailment is now considered to be a condition characterized by an idiopathic choroidal vascular hyperpermeability [14]. Several indocyanine green angiography (ICGA) studies [15–20] have shown presence of multiple hyperpermeable areas in the choroid, and FA leaks have been found to be contiguous with such areas [18–20]. A recent OCT study [21] found PED (91%) and RPE bulge (89%) in the areas of choroidal vascular hyperpermeability.
It is difficult to explain why certain areas in choriocapillaris become hyperpermeable. Several studies [17–20] have observed delayed filling of segments of choriocapillaris prior to the development of hyperpermeability. This had been attributed to a decrease in arterial perfusion in these segments. Decreased arterial perfusion means oxygen deprivation. Experimental studies [22, 23] have shown that oxidative metabolism is critical for the maintenance of retinal adhesions and integrity of cell junctions and barrier. Kitaya et al. [17] were of the opinion that small, localized ischaemic regions caused by non-perfusion or vasoconstriction of the choriocapillaris may induce collateral choriocapillary congestion around this region. However; a decrease in venous outflow of these areas may also have the effect of delaying the observed dye filling. This may create a pressure overload and cause choroidal vascular hyperpermeability [14]. Several ICGA studies [16, 18] noted choroidal venous dilatation, though no explanation was offered for it. One earlier study [24] also suggested the possibility of pathological changes in the choroidal veins, particularly in the intrascleral part, in CSC cases. One experimental study [25] was able to produce posterior pole serous retinal detachment in five out of nine monkey eyes by occluding one or two vortex veins.
As the choriocapillaris is fenestrated, the interstitial fluid within the choroid can be expected to have a large range of molecules. Normally resorption of fluid and protein molecules within the choroid primarily occurs by free exchange through this fenestrated choriocapillaris, and some excess amount is also drained through the sclera [14]. In acute CSC, the amount of fluid and solutes are definitely more than the RPE cells normally can cope with. Ultimately, RPE barrier damage occurs in certain areas in CSC, which appears to be secondary to excessive work load of the ionic pumps. Whatever may be the mechanism to jeopardize the normal functioning of RPE cells, some of the cells ultimately decompensate and start leaking fluid which would move towards the retina, as there is less resistance in this direction. Decompensation of the RPE cells could sometimes be visualized while doing FA in cases of CSC with PED. On several occasions, we observed sudden diffuse dye leak from all the RPE cells of the PED about 10 minutes after dye injection, but not all the PEDs leak like this. Several investigators [7, 14, 15, 26–29] have observed that the increase in interstitial hydrostatic pressure in the choroid drives the fluid towards the retina, and leads to the development of PED and microrips at the junction of attached and detached RPE, or along the decompensated RPE cells that cause fluid leak into the subretinal space. The micro-rents usually occur in the parafoveal region, and more so in the superonasal quadrant. This area is probably more hypoxic. Kitaya et al. [17] observed foveal choroidal blood flow in eyes with CSC to be 45% less than in the fellow normal eyes. Several OCT studies [30–33] have noticed thickening of retinal layers in acute CSC. This finding is noteworthy, and it definitely indicates that enough serous fluid enters the retinal stroma in the acute phase of the disease, and this fluid ultimately opens up the potential space between the RPE and the sensory retinal layers. The retinal separation usually occurs in the posterior pole where the leaks develop. Once the detachment occurs, it would be expected to enlarge until sufficient RPE is exposed to allow removal of fluid at a rate equal to the inflow rate through the leak [7]. Thus, the subretinal space has a dynamic environment into which, and from which, there is a continuous flux of water, ions, and protein [34]. Negi and Marmor [35] observed that the presence of protein in serous fluid slows resorption in CSC by raising the oncotic pressure of the subretinal space to a level near that of the choroid. Asayama’s experimental study [36] showed that even 24 hours after injection of human albumin into the subretinal space, most of the protein remained in this space, and only a small amount penetrated the external limiting membrane, which appeared to be the most resistant retinal structure. But albumin was found to cross the iodate-damaged RPE, although slowly [34]. So, in a clinical condition like CSC, in which there is RPE barrier damage, it seems that the protein can move in either direction. In CSC, protein in the subretinal fluid may concentrate as smaller ions are pumped out [35]. Phase boundary between gels or colloids, as well as a liquid, can act as a selective barrier [37]. It can be presumed that the cations attached to the dissolved proteins will also produce some extra osmotic pressure by the Donnan effect.
The presence of fibrin in the detached space itself indicates that there is sufficient alteration in the permeability of the choriocapillaris and the RPE [14]. The fibrin monomers form a gel, which is a colloid system consisting of long colloidal particles forming a ‘brush-heap’ type of structure, in which the liquid is trapped in little pools [38]. Probably this fibrin network, formed inside the detached cavity of CSC, produces pockets of fluid of different density. In the present series, presence of fibrin was clinically suspected in 11.42% of affected eyes.
In FA, the portion of the dye (20%) which is not protein-bound actually fluoresces [39] and, through the RPE functional hole or micro-ent, it enters the detached space along with the fluid due to solvent drag. Shimizu and Tobari [3] believed that the osmotic pressure gradient between the two fluid systems leads to unidirectional fluid flow through the functional hole in the pigment epithelium, that is, a kind of bulk flow occurs. They were of the opinion that the thermal current is not responsible for the smokestack phenomenon. But according to Marmor [40], much of the spread of fluorescein seen angiographically may represent diffusion and convection rather than net fluid influx. The diffusion constants for fluorescein are such that dye merely diffusing through a focal RPE defect could stain a typical serous detachment within minutes to hours without any flow being postulated at all. He also believed that in smokestack leak there is an entry of low-density fluid, but convection currents would move this fluid upwards. According to him, entry of fluid into the serous cavity still does not necessarily mean that there is a net transfer of fluid. A recent study [26] believed that in addition to the role of convection currents and the molecular weight difference between the Fluorescein molecule and the subretinal exudates, a bigger micro RPE rip is needed for the development of smokestack leak. We also believe it to be one of the factors for development of this phenomenon, as all the RPE leaks in the acute phase of the disease are not smokestack leaks. Several OCT studies [31, 41, 42] have shown presence of hyperdense protienaceous material along with clear fluid in the subretinal space in many cases. In the present study, subretinal fibrin clinically seemed to be present in 11.42% of eyes with smokestack leak. So, there are enough supportive data to infer that the subretinal fluid in CSC is hyperdense, which of course may not be uniform through out the detached space. It is quite likely that the oncotic pressure in this hyperdense fluid will be more, and the flow of fluid will reverse at the level of RPE. It appears that the interstitial hydrostatic pressure initiates the process, and as soon as the oncotic pressure, which is also a form of hydrostatic pressure, builds up within the detached space, both the forces act simultaneously, coordinating with each other to maintain the detachment. However, Marmor [40] observed that presence of protein in the sub-retinal space (SRS) does not itself induce or maintain a serous detachment. His opinion was based on the fact that a rapid absorption of fluid occurs in rhegmatogenous retinal detachment after sealing of the retinal hole, and demonstrated a rapid exit of the fluid from the subretinal space in experimental animals, leaving behind the protein. But the biochemical and/or biophysical conditions leading to rhegmatogenous retinal detachment in human eyes and the mechanically induced serous detachment in experimental animals are not exactly the same as that of CSC in human beings, Moreover, presence of protein, although it builds up the oncotic pressure, will probably not prevent the pumping out of the fluid by the normal functioning RPE, or the rate of drainage of protein from the subretinal space will be slower than that of the fluid part.
The phenomenon of convection currents definitely plays an important role in the fluid movement inside the detached space. To produce convection currents in the detached space, there would have to be sufficient heat generation in the overlying choroid. Friedman [24], who suspected that CSC might be a manifestation of a failure of the thermoregulatory function of the choroid, felt that the peculiar concurrent pattern of vessels in the posterior choroid, in which the blood in both the short ciliary arteries and vortex veins flow in the same direction (that is, anteriorly) might have some non-nutritional function. According to him, in such a situation heat should be dissipated from the choroid. In CSC, something goes wrong in the thermoregulatory mechanism of choroid, but he did not spell out what exactly could happen. He was probably hinting at a local rise of temperature in the choroid instead of dissipation. Present analysis of the sequence of events in the pathophysiology of the smokestack phenomenon also suggests it. The hyperpermeable areas of the choriocapillaris must be warmer than the rest of the capillary bed. Friedman [24] observed that when heat is introduced into the system in the region of the capillary it tends to be trapped by being short-circuited from a warmer vein to a cooler artery, resulting in a local elevation of temperature. Current movement during convection may be invisibly slow, or it may be obvious and rapid [43]. Application of laboratory fluid dynamics, especially Rayleigh–Bénard convection, to the fluid dynamics of the serous fluid in CSC, would probably explain the various morphological patterns of the smokestack leak. Rayleigh–Bénard convection [44] is the instability of a fluid layer which is confined between two thermally conducting plates, and is heated from below to produce a fixed temperature difference. In CSC, the RPE layer and the detached sensory retina represent the thermally conducting plates with fluid layer in between. When heat is fed into the system from one direction (in the case of CSC it is the choroidal side) at small values, it merely diffuses (conducts) from below upward, without causing fluid flow. As the heat flow is increased, above a critical value of the Rayleigh number, a bulk motion of the fluid due to heat begins. In fluid mechanics, the Rayleigh number [45] for a fluid is a dimensionless number associated with the heat transfer within the fluid. It is defined as the product of the relationship between buoyancy and viscosity within a fluid and the relationship between the momentum diffusivity and thermal diffusivity. Viscous damping in the fluid directly opposes the fluid flow. In addition, the thermal diffusion will suppress the temperature fluctuation by causing the rising plume of hot fluid to equilibrate with surrounding fluid, destroying the buoyant force [43].This is what exactly happens in typical smokestack leak. As the temperature difference between the top and bottom of the fluid becomes higher, the viscosity may begin to significantly vary horizontally across layers of fluid. This breaks the symmetry of the system, and generally changes the pattern of upward- and downward-moving fluid. As the Rayleigh number is increased even further above the value where fluid movements first appear, more complex patterns, such as spirals, may begin to appear. But we do not know yet how much of temperature variation can occur in the choroid due to development of hyperpermeability. If it can really exceed the critical Rayleigh number, this could be a probable explanation for the atypical movement of the stream of dye in certain cases with smokestack phenomenon. If we study the clinical photographs Figs. 7 and 8, it appears that spiralling or twisting movements of the column of the dye occur in the subretinal fluid of CSC cases. The speed of movement of the plume of heated fluid depends upon temperature gradient. This explains the variation in the speed of entry of the dye inside the detached cavity. In some cases, the dye really ascends with considerable speed. This series had two cases of chronic CSC with a slowly rising plume of dye on FA. A slow-rising plume of dye definitely indicates less heat generation in the choroid.
Viscosity of the serous fluid inside the detached area is definitely not uniform; otherwise, we would have seen only the Boussinesq convection [43] as we see it inside the anterior chamber of the eye. It is a known fact that viscosity diminishes as temperature rises. So the fluid freshly entering from the choroid is likely to be less dense than the fluid already existing inside the detached cavity. A very interesting case series was recently reported by Shukla et al. [41]. This small series of CSC cases demonstrated fibrinous deposits in the subretinal space bridging the RPE of PED and the detached sensory retina, and showed some unusual pattern of fluorescein dye leak. In one case, after transpupillary thermotherapy, the fibrinous material disappeared and the PED flattened. Interestingly, the anomalous leaking pattern also changed to typical smokestack leak once the loculation of the serous cavity had gone. It indicates that convection currents definitely plays a role in smokestack phenomenon, and a comparatively homogeneous fluid space is required to develop the typical pattern. It is now quite apparent that the variation in the morphology of this type of leak is due to altered fluid current dynamics in the presence of hyperdense substances such as fibrin in the serous cavity.
Lastly, how to explain the low prevalence of smokestack leak in acute cases of CSC? In addition to the increased tissue hydrostatic pressure in the choroid and the size of the micro-rip in the RPE, a third factor, that is, the temperature gradient in the choroid, definitely plays a role in the production of smokestack phenomenon. It may be that the rise of temperature in the choroid exceeding the critical value of the Rayleigh number may not be there all the time during the acute phase of the disease and FA may miss this critical period, or it may be that the heat generation in the choroid in acute phases of CSC may not be uniform in all the cases.
As the clinical aspect of this study is mostly retrospective, certain drawbacks such as inadequate data for analysis of the various parameters could not be avoided. With the progression of the analysis of the data, we have realized that at times the smokestack phenomenon can develop at a later phase of the angiography. It is likely that we might have missed some cases, as the cases were not followed up for a prolonged period of time while doing FA in the early part of the period chosen for this study. However, in spite of the limitations, the following points emerge from the present study:
-
(1)
Smokestack leaks usually occur in fresh RPE rent and 70% occur in first (primary) acute episode.
-
(2)
They usually develop in the early part of the acute phase of the disease.
-
(3)
The leakage site does not differ from that of other types of RPE leaks.
-
(4)
Convection currents play a major role in the production of smokestack leak.
-
(5)
Temperature gradient in the choroid may not be uniform in all the acute cases of CSC and this may be another important factor for low prevalence of smokestack leak.
-
(6)
Rayleigh–Bénard convection appears to explain its varied morphological manifestations.
-
(7)
Presence of material such as fibrin in the subretinal space alters the fluid dynamics and produces the atypical pattern of the smokestack leak.
-
(8)
Rarely, it can occur in chronic cases and in small-sized detachments, and more than one leak can be seen within the same detached space.
Part II: Experimental study
Introduction
Identical fluorescein to dye leakage that we see in CSC in human eyes has been seen in monkey eyes having serous detachment of the sensory retina produced by repeated intravenous injection of epinephrine and intramuscular corticosteroids [46]. Anatomically, the structure of monkey eyes closely resembles that of human eyes. But if we want to study the fluid dynamics in such an experimental model, it will not differ much from the human eyes. The findings of FA to assess the fluid dynamics will be similar, and the inferences will be mostly hypothetical. As the analysis of the movement of the fluorescein dye in the clinical study has indicated that heat generation in the choroidal side is required for the development of smokestack leak, we contemplated producing this phenomenon in the laboratory model to see whether these findings could be correlated with the findings of clinical cases.
Methods and materials
A small bottle containing diluted fluorescein, the mouth of which was covered by a stretched latex rubber sheet taken from surgical gloves, with a fine hole in its centre made by a 26-gauge needle, was placed horizontally on the bottom of a large beaker containing a solution. After trial with various concentrations of the fluorescein dye and various types of solutions, we settled for three different concentrations (0.10 mg/ml, 10 mg/ml and 40 mg/ml) and two types of solution in the beaker, either 250 ml of isotonic balanced salt solution (‘Irigan’ solution; Manufactured by Klar Sehen Pvt. Ltd., Hyderabad, India) or 250 ml of the same solution mixed with almost the total quantity of the white of an egg weighing 56 gm. As electrolytes are the primary factors in the regulation of the osmotic pressure of plasma, we preferred balanced salt solution, and in one sample egg white was added with the idea of increasing the colloid osmotic pressure further. However, addition of egg white did not make any significant difference to the naked eye, as it was found to settle on the bottom of the beaker even after stirring it well. Assuming that the concentration of injected 3 ml of 20% fluorescein dye (manufactured by “Samarth Life Sciences Pvt. Ltd.”, Mumbai, India) will be around 0.12 mg per ml when it is mixed with 5 liters of circulating blood volume in an adult, the experiment was started with a solution containing 0.10 mg of fluorescein per ml. The beaker was heated by spirit lamp flame just below the horizontally placed bottle, and the changes in the fluid dynamics were photographed.
Our experimental model was practically a copy of Marmor's model [40], in which he tried to show how the dye can enter a closed space without any net accumulation of fluid. However, we placed the small bottle containing the dye horizontally, and tried to immerse it in a solution presumed to be of higher osmotic pressure.
Results and observations
In the experimental study, when the small bottle containing the dye was placed at the bottom of the beaker containing both the types of solution, no bulk flow was observed. When it was heated from below, the dye with low concentrations up to 10 mg/ml ascended. The ascending column of the dye showed various twisting and spiraling patterns (Fig. 10a, b). In contrast, the concentrated dye (40 mg/ml) had descended in spite of heating it for some time (Fig. 10c).

a The horizontally lying bottle with diluted fluorescein dye (0.10 mg/ml) within a beaker with only balanced salt solution. The column of the dye is seen to ascend with a twisting movement. b The same experiment done with a concentrated solution (10 mg/ml) in the bottle. The main column of the dye ascended with a spiraling movement. c The downward spread of the dye from the bottle containing a concentrated solution (40 mg/ml). The column of dye showed a tendency to go up after heating it for some time, but still it could not overcome the gravitational force of the concentrated dye, rather it remained horizontal for some time
Discussion
In the laboratory, if we do not use animals, production of a physiological environment identical to CSC in human beings will never be possible with commonly used equipment. However, the experimental model that we adopted for this study at least demonstrated the change in fluid dynamics of the fluorescein dye due to convection currents, which could be compared with the dye movement in some of the CSC cases of the present series (Figs. 7 & 8). Marmor [40] in his experimental model, by tapping the perforated membrane over a bottle of methylene blue, within a large beaker of water, was able to eject a small puff of dye into the surrounding water, and observing this he inferred that probably vascular pulsations in the choroid or movement of vitreous and sclera during saccades could in this manner force small aliquots of choroidal fluid through an RPE defect without any net inward flow. Our experiment had shown that heat from one side is needed to produce the movement of the column of dye. No doubt, by pressing the perforated covering membrane of the small bottle containing dye, one can produce ejection of the dye, but if choroidal pulsation or saccadic movement of the eye were responsible for leakage of dye in CSC, the RPE leakage, particularly the smokestack leak, would have been pulsatile, or its intensity would have increased or decreased with the movement of the eye. Our crude laboratory experiment also revealed another interesting finding—a downward spread of the concentrated dye in spite of heating it for a considerable period of time (Fig. 10c). This showed that the fluid having the unbound concentrated dye is heavier, and the convection currents could not overcome its gravitational force. Now, does this finding can also explain the downward or horizontal spread of the fluorescein dye in occasional cases of CSC? In that case, the dilution of the fluorescein dye being constant, the fluid containing the unbound dye would have to be heavier. Do these sporadic cases leak more protein-laden heavy fluid? Or is it due to the variation in the viscosity of the subretinal fluid which prevents upward spread of the dye? One clinical study from Japan [47] suspected drainage of protein-rich transudate in inferiorly directed smokestack phenomenon, particularly in the bullous type of detachment.
References
Novotny HR, Alvis DL (1961) A method of photographing fluorescence in circulating blood in the human retina. Circulation 24:82–86
Ciardella AP, Guyer DR, Spitznas M, Yannuzzi LA (2001) Central serous chorioretinopathy. In: Ryan S (ed) Retina, 3rd ed., Vol 2. Mosby, St Louis, pp 1153–1181
Shimizu K, Tobari I (1971) Central serous retinopathy dynamics of subretinal fluid. Mod Probl Ophthalmol 9:152–157
Wessing R (1973) Changing concept of central serous chorioretinopathy and its treatment. Trans Am Acad Ophthalmol Otolaryngol 77:275–280
Burton TC (1972) Central Serous Chorioretinopathy. In: Blodi E (ed) Current concepts in ophthalmology. CV Mosby, St Louis, pp 1–28
Yannuzzi LA, Schatz H, Gitter KA (1979) Central Serous Chorioretinopathy. In: The Macula: A Comprehensive Text and Atlas. Williams & Wilkins, Baltimore MD, pp 145–165
Friberg TR, Campagna J (1989) Central chorioretinopathy: an analysis of the clinical morphology using image-processing techniques. Graefes Arch Clin Exp Ophthalmol 227:201–205
Bujarborua D, Nagpal PN (2005) CSR: idiopathic central serous chorioretinopathy. Jaypee Brothers, New Delhi, pp 36–51
How ACSW, Koh AHC (2006) Angiographic characteristics of acute central serous chorioretinopathy in an Asian Population. Ann Acad Med Singapore 35:77–79
Spitznas M, Huke J (1987) Number, shape, and topography of leakage points in acute type I central serous retinopathy. Graefes Arch Clin Exp Ophthalmol 225:438–440
Bujarborua D (2001) Long-term follow-up of idiopathic central serous chorioretinopathy without laser. Acta Ophthalmol Scan 79:417–421
Gass JMD (1967) Pathogenesis of disciform detachment of the neuroepithelium. II. Idiopathic central serous chorioretinopathy. Am J Ophthalmol 63:587–615
Burke JM, McKay BS, Jaffe GJ (1991) Retinal pigment epithelial cells of the posterior pole have fewer Na/K adenosine triphosphatage pumps than peripheral cells. Invest Ophthalmol Vis Sci 32:2042–2046
Spaide RF, Goldbaum M, Wong DWK, Jang KC, Iida T (2003) Serous detachment of the retina. Retina 23(6):820–846
Guyer DR, Yannuzzi LA, Slakter JS, Sorenson JA, Ho A, Orlock D (1994) Digital indocyanine green videoangiography of central serous chorioretinopathy. Arch Ophthalmol 112:1057–1062
Iida T, Kishi S, Hagimura N, Shimizu K (1999) Persistent and bilateral choroidal vascular abnormalities in central serous chorioretinopathy. Retina 19:508–512
Kitaya N, Nagaoka T, Hikichi T, Sugawara R, Fukui K, Ishiko S, Yoshida A (2003) Features of abnormal choroidal circulation in central serous chorioretinopathy. Br J Ophthalmol 87:709–712
Prunte C, Flammer J (1996) Choroidal capillary and venous congestion in central serous chorioretinopathy. Am J Ophthalmol 121:26–34
Piccolino FC, Borgia L (1994) Central serous chorioretinopathy and indocyanine green angiography. Retina 14:231–242
Scheider A, Nasemann JE, Lund OE (1993) Fluorescein and indocyanine green angiographies of central serous chorioretinopathy by scanning laser ophthalmoscopy. Am J Ophthalmol 115:50–56
Hirami Y, Tsujikawa A, Sasahara M, Gotoh N, Tamura H, Otani A, Mandui M, Yoshimura N (2007) Alteration of retinal pigment epithelium in central serous chorioretinopathy. Clin Experiment Ophthalmol 35(3):225–230
Kim RY, Yao XY, Marmor MF (1993) Oxygen dependency of retinal adhesion. Invest Ophthalmol Vis Sci 34:2074–2078
Bailey TA, Kanuga N, Romero IA, Greenwood J, Luthert PJ, Cheetham ME (2004) Oxidative stress affects the junctional integrity of retinal pigment epithelial cells. Invest Ophthalmol Vis Sci 45(2):675–684
Friedman E (1977) Central serous chorioretinopathy: pathogenesis and treatment. In: Brockhurst RJ, Boruchoff SA, Hutchinson BT, Lessell S (eds) Controversy in ophthalmology. WB Saunders, Philadelphia, pp 706–709
Gaudric A, Sterkers M, Coscas G (1987) Retinal detachment after choroidal ischemia. Am J Ophthalmol 104:364–372
Eandi CM, Ober M, Iranmanesh R, Peiretti E, Yannuzzi LA (2005) Acute central serous chorioretinopathy and fundus autofluorescence. Retina 25:989–993
Gass JDM (1977) Idiopathic central serous choroidopathy (ICSC). In: Brockhurst RJ, Boruchoff SA, Hutchinson BT, Lessell S (eds) Controversy in ophthalmology. WB Saunders, Philadelphia, pp 710–714
Goldstein BG, Pavan PR (1987) “Blow-outs” in the retinal pigment epithelium. Br J Ophthalmol 71:678–681
Carvalho-Recchia CA, Yannuzzi LA, Negrao S, Spaide RF, Freud KB, Rodriguez-Coleman H, Lenharo M, Iida T (2002) Corticosteroids and central serous chorioretinopathy. Ophthalmology 109:1834–1837
Hee NR, Puliafito CA, Wong C, Reichel E, Duker JS, Schuman JS, Swanson EA, Fujimoto JG (1995) Optical coherence tomography of central serous chorioretinopathy. Am J Ophthalmol 120(1):65–74
Iida T, Hagimura N, Sato T, Kishi S (2000) Evaluation of central serous chorioretinopathy with optical coherence tomography. Am J Ophthalmol 129(1):16–20
Moschos M, Brouzas D, Koutsandrea C, Stefanos B, Loukianou H, Papantinosio F, Moschos M (2007) Assessment of central serous chorioretinopathy by optical coherence tomography and multifocal electroretinography. Ophthalmologica 221(5):292–298
Ojima Y, Hangai M, Sasahara M, Gotog N, Inone R, Yasuno Y, Makita S, Yatagai T, Tsujikawa A, Yoshimura N (2007) Three-dimensional imaging of the foveal photoreceptor layer in central serous chorioretinopathy using high-speed optical coherence tomography. Ophthalmology 114(12):2197–2207
Takeuchi A, Kricorian G, Marmor MF (1995) Albumin movement out of the subretinal space after experimental retinal detachment. Invest Ophthalmol Vis Sci 36:1298–1305
Negi A, Marmor MF (1984) Experimental serous retinal detachment and focal pigment epithelial damage. Arch Ophthalmol 102:445–449
Asayama K (1976) In vivo study on the absorption of the subretinal fluid.2. Studies on an absorption of tracers injected between the sensory retina and the pigment epithelium layer. Acta Soc Ophthalmol Jpn 80:598–607
Gibbs–Donnan effect. http://en.wikipedia.org/wiki/Gibbs–Donnan effect (accessed April 16, 2008).
Garrett AB (1987) Colloid. The new book of popular science, Vol. 3. Grolier International Inc., pp 107–117
Schatz H (1989) Fluorescein angiography: basic principles and interpretation. In: Ryan SJ (ed) Retina, vol 2. The C.V. Mosby Company, St. Louis, pp 3–77
Marmor MF (1988) New hypotheses on the pathogenesis and treatment of serous retinal detachment. Graefes Arch Clin Exp Ophthalmol 226:548–552
Shukla D, Aiello LP, Kolluru C, Baddela S, Jager RD, Kim R. (2008) Relation of optical coherence tomography and unusual leakage pattern in central serous chorioretinopathy. Eye 22(4):592–596.58
Fujimoto H, Gomi F, Wakabayashi T, Sawa M, Tsukawa M, Yano Y (2008) Morphologic changes in acute central serous chorioretinopathy evaluated by fourier-domain optical coherence tomography. Ophthalmology 115(9):1494–1500
Convection. http://en.wikipedia.org/wiki/Convection (accessed April 16,2008).
Rayleigh–Bénard Convection. http://physics.ucsd.edu/was-daedalus/convection/rb.html (accessed April 16, 2008).
Rayleigh number. http://en.wikipedia.org/wiki/Rayleigh_Number (accessed April 16, 2008).
Yoshioka H, Katsume Y, Akune H (1982) Experimental central serous chorioretinopathy in monkey eyes: fluorescein angiographic findings. Ophthalmologica, Basel 185:168–178
Watanabe G, Iida T, Takahashi K, Sato T, Kishi S, Shimizu M (2001) Clinical characteristics of bullous retinal detachment manifesting inferiorly-directed smokestack phenomenon. Jap J Ophthalmol 55(6):1217–1220 (English abstract)
Acknowledgements
We are grateful to Dr Nazimul Hussain, Dr Samrat Chatterjee, Dr Wartikar Sharang, Dr Geetanjali Bori, Dr Ankur Rahman, Dr. Aditya Sharma and Dr Kamal Nagpal for their help in various stages of this study, and indebted to Mr Omana Kuttan for his technical assistance.
Author information
Authors and Affiliations
Corresponding author
Additional information
Financial support None.
Rights and permissions
About this article
Cite this article
Bujarborua, D., Nagpal, P.N. & Deka, M. Smokestack leak in central serous chorioretinopathy. Graefes Arch Clin Exp Ophthalmol 248, 339–351 (2010). https://doi.org/10.1007/s00417-009-1212-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-009-1212-5