
Abstract
Background
The aim of the study was to evaluate the vitreous penetration of two commercially available ophthalmic fluoroquinolones: ofloxacin and levofloxacin.
Methods
This prospective, double-blind, randomized clinical trial comprised 16 patients scheduled for vitrectomy surgery of one eye for macular hole or macular pucker. The patients were randomly assigned to receive topical ofloxacin 0.3% (n=9) or levofloxacin 0.5% (n=7) the day before, one drop at noon, 4 p.m., 8 p.m. and midnight. The next morning, patients were given their assigned masked antibiotic every 5 min for four doses starting 1 h before surgery. The vitreous humour samples, at least 0.3 ml each, were collected 1 h after the administration of the last dose, at the beginning of the pars plana vitrectomy with infusion disconnected. Samples were assayed for ofloxacin and levofloxacin concentrations by a method using high-performance liquid chromatography (HPLC) coupled with single mass spectrometry with electrospray ionization (ESI-MS).
Results
Equal topical administration of levofloxacin yielded 2.5 times higher vitreal concentration than ofloxacin. The mean vitreous concentrations of ofloxacin and levofloxacin were 5.30±3.04 (SD) ng/ml and 13.09±5.24 ng/ml, respectively (P=0.002).
Conclusion
Equal dosing with topical administration of levofloxacin 0.5% and ofloxacin 0.3% allows better penetration into the vitreous for levofloxacin, but the levels of mean concentrations of each drug did not exceed the MIC(90) or MIC(50) for most ocular pathogenic bacteria in terms of conventional endophthalmitis therapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ofloxacin is a racemic, fluorinated carboxyquinolone, and its antibacterial activity resides primarily in the L-isomer. Levofloxacin is the L-isomer of this ofloxacin racemate [7, 19]. Both of these fluoroquinolones are well established representative ophthalmic antibiotics with ofloxacin classified in the second- and levofloxacin in the third-generation [18]. Their great efficacy against the most frequent Gram-positive and Gram-negative ocular pathogenic bacteria have made these fluoroquinolones an excellent initial choice for the topical therapy of external ocular infections [2, 5, 14, 20, 21, 23]. Pharmacokinetic characteristics such as low molecular weight, lipophilic properties for better corneal permeability and intraocular uptake [8, 22] have raised interest in using fluoroquinolones for prevention of postoperative endophthalmitis [11, 24].
Although ofloxacin and levofloxacin are nearly identical in molecular weight and lipophilicity and almost equal in corneal permeability, a more than fivefold difference in aqueous solubility of levofloxacin predicts higher concentrations for levofloxacin in aqueous humour [8, 22]. Greater water solubility also makes it possible to formulate eyedrops with a higher concentration of levofloxacin (i.e. 0.5%) than of ofloxacin (0.3%). Two studies on human corneal penetration of ofloxacin and levofloxacin indicated that levofloxacin concentrations were approximately twice as high as those of ofloxacin in aqueous humour after topical administration [10, 13].
Data on intravitreal penetration of ofloxacin and levofloxacin after topical administration in humans are scant, and there are only a few reports on intravitreal concentrations of ofloxacin and none of levofloxacin (Table 1). The purpose of the present study was to compare, as a one-time-point measurement, the penetration of ofloxacin and levofloxacin into the vitreous in uninflamed eyes.
Subjects and methods
Patients
Sixteen patients for vitrectomy surgery of one eye for macular hole or macular pucker were recruited between March and August 2005. The mean age of the seven women and nine men was 67.9±7.7 (SD) years. The study protocol was in compliance with the Declaration of Helsinki, and after approval from the local ethics committees, written informed consent was obtained from the patients enrolled. Included were generally healthy patients of either gender, aged from 40 to 80 years. Exclusion criteria were sensitivity to fluoroquinolones, diabetes, renal disease, liver disease, and infective as well as malignant diseases. From the ophthalmic aspect, excluded were patients with glaucoma, ocular infections or inflammations, previous or other contemporaneous ocular surgery, any corneal pathology and sequelae from ocular traumas. In addition, patients were not allowed to use any systemic antibiotics or topical ophthalmic medications.
Medications
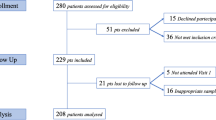
The patients were randomly assigned to receive masked topical ofloxacin 0.3% (Exocin, Allergan, Westport, County Mayo, Ireland) (n=9) or levofloxacin 0.5% (Oftaquix, Santen, Tampere, Finland) (n=7) one drop at a time and eight drops in all before surgery (Fig. 1).

Time schedule for instillation of examination drops
Before the procedure the pupil was maximally dilated with a combination of phenylephrine 5% (Oftan Metaoxedrin, Santen) and tropicamide 0.8% (Oftan Tropikamid, Santen), as well as cyclopentolate 1% (Oftan Syklo, Santen).
Surgery and samples
All the operations were performed under general anaesthesia. The eye was washed using povidone-iodine 5% ophthalmic solution. At the initiation of the surgery, a pars plana sclerotomy was done with a V-Lance Knife (20G, Alcon Surgical, Huntington, WV, USA). Vitreous humour samples of at least 0.3 ml each were collected 1 h after the administration of the last dose, at the beginning of the pars plana vitrectomy with infusion disconnected. For obtaining the vitreous fluid, a vitrector (Accurus, Alcon Laboratories, TX, USA) was used with a suction tube connected to a manually adjusted 2 ml aspiration syringe. The sample was placed into a cryogenic Eppendorf tube (Eppendorf Nordic, Horsholm, Denmark), and then immediately taken to the laboratory to be stored at a temperature below −20°C until analysis was performed. Each tube was marked with a patient identification number and a code which indicated the antibiotic that had been randomly assigned to the patient. The analyses of the concentrations of ofloxacin and levofloxacin in the vitreous humour were performed at Santen Oy Analytical Development Laboratory in Tampere, Finland.
Quantitation analysis
Levofloxacin/ofloxacin and added internal standard (lomefloxacin) were determined in vitreous humour samples by using high-performance liquid chromatography (HPLC) coupled with single quad mass spectrometry with electrospray ionization (ESI-MS). Positive mode ionization and selected ion monitoring (SIM) was used for the sample analysis. Mass ions of m/z 318 ([M+H−CO2]+) and m/z 352 ([M+H]+) were monitored for levofloxacin/ofloxacin and internal standard, respectively. Antibiotics were separated at ambient temperature on a 2.0 mm ID×50 mm length, 3.0 μm particle size Gemini C18 column (Phenomenex, Torrance, CA, USA). A flow rate of 0.2 ml/min was used in isocratic separation. Mobile phase contained 30% methanol and 70% 10 mM ammonium acetate and 0.07% glacial acetic acid. A 200 μl aliquot of vitreous humour to be assayed was spiked with internal standard and diluted with 300 μl of acidic solution. The sample was then placed in a multitube vortexer for 5 min (2600 rpm) and centrifuged for 10 min (3000 rpm). A 20-μl aliquot of supernatant was injected into HPLC/MS system. The ratio of the intensities of the chromatographic responses for levofloxacin/ofloxacin and the internal standard were used to calculate the levofloxacin/ofloxacin concentrations in unknown vitreous humour samples using calibration curve. The calibration curve was generated from the analysis of a drug-free, pig-origin, vitreous humour matrix fortified with various amounts of levofloxacin/ofloxacin and a fixed amount of the internal standard. The calibration curve range for levofloxacin/ofloxacin is from 0.5 ng to 25 ng per millilitre of vitreous humour.
The analytical method used is not enantioselective and is therefore incapable of separating L- and D-isomers of ofloxacin. L- and D-isomers are seen as a single peak in the chromatogram when ofloxacin sample is analysed. Intensities of chromatographic responses for levofloxacin and ofloxacin are identical, as is their chromatographic behaviour, when the current HPLC system with MS detection is used for the sample analysis. This means that equal results are achieved for the levofloxacin and ofloxacin samples containing equivalent concentrations.
Statistical analysis
Statistical comparison of the mean concentrations of the two groups was performed using a two-sided t test with Levene’s test for equality of variances. The analysis was based on a non-normal distribution of the data. The level of statistical significance was set at P<0.05.
Results
Equal topical administration of levofloxacin yielded a concentration of fluoroquinolone in the vitreous approximately 2.5 times higher than that of ofloxacin (P=0.002). The mean vitreous concentrations of ofloxacin and levofloxacin were 5.30±3.04 (SD) ng/ml and 13.09±5.24 ng/ml, respectively (Fig. 2). All the samples exceeded the lowest detectable level in the quantitation assay.

Mean (SD) vitreous concentrations of ofloxacin and levofloxacin achieved after topical administration
Discussion
Ofloxacin and levofloxacin as representatives of the second and the third generation of fluoroquinolones have an established position in the therapy of external ocular infections and perioperative infection prophylaxis. It has been demonstrated that ofloxacin is effective in sterilizing the external ocular adnexa by eliminating bacteria in the conjunctiva and lids [1, 12], which strengthens the usefulness of fluoroquinolones as perioperative antibiotics reducing the risk of infections following intraocular surgery [11, 15, 16, 24]. In addition, on the basis of their good water solubility and lipophilicity [8, 22], many fluoroquinolones are prone to penetrate intraocularly. As it has been shown that levofloxacin penetrates into the aqueous at approximately twice the concentration of ofloxacin [10, 13], one can assume that levofloxacin penetrates similarly into the vitreous. Furthermore, because levofloxacin consists of only the active L-isomer of the D- and L-racemate ofloxacin, all of the levofloxacin antibiotic found in the anterior chamber is in an active form. Therefore, the actual aqueous concentration of levofloxacin in active compound can be 3.5–4 times that of ofloxacin. The difference in aqueous concentrations is partly due to a higher antibiotic content of the commercially available levofloxacin eyedrop (0.5% vs 0.3%) [13]. The higher antibiotic concentration in the aqueous fluid may be the cause of a higher concentration in the vitreous humour. It has been also shown that multiple and tightly repeated or pulse dosing results in higher intraocular levels of fluoroquinolone antibiotics [3, 4, 6]. Although inside the eye the aqueous flow takes place from the posterior chamber to the anterior one, diffusion of the drug into the vitreous body correlates positively with the concentration gradient.
To the best of our knowledge, there are no published data on levofloxacin penetration into the human vitreous from a 0.5% ophthalmic solution. The dosing of the fluoroquinolones we used in the present study is in accordance with the regimen we follow in routine practice to eradicate microbes from the external parts of the eye preoperatively. The laboratory measurements showed that the amounts of each antibiotic penetrating into the vitreous are very slight, measured in nanograms rather than micrograms. Notwithstanding, the determined concentrations in the vitreous humour clearly showed a 2.5 times higher level for levofloxacin than for ofloxacin. The concentrations were, however, relatively low and well under the MIC(90) and MIC(50) values of most ocular pathogenic bacteria. The higher vitreous ofloxacin levels after topical instillation reported by Donnenfeld et al. may be due in part to the fact that all the 10 study patients had been previously operated on for cataract and had a defect of the posterior capsule [6], and in part to a pulse-type dosing of antibiotic. A relatively high concentration of ofloxacin determined by Yalvac et al. from the vitreous samples obtained during cataract surgery with accidental vitreous loss may also relate to a contamination of vitreous samples with aqueous [25] (see also Table 1).
In a report by Hariprasad et al., topical application of moxifloxacin, a fourth-generation fluoroquinolone, every 6 h for 3 days yielded the levels of 0.88±0.88 μg/ml and 0.06±0.06 μg/ml in the aqueous and the vitreous humour, respectively [9]. In the same report, when the instillation interval was shortened to 2 hours, mean±SD moxifloxacin concentrations achieved 2.28±1.23 μg/ml and 0.11±0.05 μg/ml in the aqueous and the vitreous humour, respectively.
Although MIC(90) values were far exceeded in the aqueous for a wide spectrum of pathogens in both instillation regimens, concentrations of moxifloxacin in the vitreous did not achieve the MIC(90) levels for several organisms [9]. In the present study, the mean vitreous concentrations of both tested fluoroquinolones did not exceed the minimum inhibitory concentrations—MIC(90) or MIC(50)—for most ocular pathogenic bacteria in terms of conventional endophthalmitis therapy [17]. The different dosing schemes used in the study by Hariprasad et al. and in the present study make it difficult to compare exact differences in the ocular penetration of these fluoroquinolones.
References
Barkana Y, Almer Z, Segal O, Lazarovitch, Avni I, Zadok D (2005) Reduction of conjunctival bacterial flora by povidone-iodine, ofloxacin and chlorhexidine in an outpatient setting. Acta Ophthalmol Scand 83:360–363
Bron AJ, Leber G, Rizk SN, Baig H, Elkington AR, Kirkby GR, Neoh C, Harden A, Leong T (1991) Ofloxacin compared with chloramphenicol in the management of external ocular infection. Br J Ophthalmol 75(11):675–679
Bucci FA Jr (2004) An in vivo study comparing the ocular absorption of levofloxacin and ciprofloxacin prior to phacoemulsification. Am J Ophthalmol 137(2):308–312
Cekic O, Batman C, Yasar U, Basci NE, Bozkurt A, Kayaalp SO (1998) Penetration of ofloxacin in human aqueous and vitreous humors following oral and topical administration. Retina 18(6):521–525
Diamond JP, White L, Leeming JP, Bing Hoh H, Easty DL (1995) Topical 0.3% ciprofloxacin, norfloxacin, and ofloxacin in treatment of bacterial keratitis: a new method for comparative evaluation of ocular drug penetration. Br J Ophthalmol 79(6):606–609
Donnenfeld ED, Perry HD, Snyder RW, Moadel R, Elsky M, Jones H (1997) Intracorneal, aqueous humor, and vitreous penetration of topical and oral ofloxacin. Arch Ophthalmol 115(2):173–176
Fujimoto T, Mitsuhashi S (1990) In vitro antibacterial activity of DR-3335, the S-(-)-isomer of ofloxacin. Chemotherapy 36:268–276
Fukuda M, Sasaki K (1995) In vitro topically applied fluoroquinolone penetration into the anterior chamber. Nippon Ganka Gakkai Zasshi 99(5):532–536
Hariprasad SM, Blinder KJ, Shah GK, Apte RS, Rosenblatt B, Holekamp NM, Thomas MA, Mieler WF, Chi J, Prince RA (2005) Penetration pharmacokinetics of topically administered 0.5% moxifloxacin ophthalmic solution in human aqueous and vitreous. Arch Ophthalmol 123:39–44
Healy DP, Holland EJ, Nordlund ML, Dunn S, Chow C, Lindstrom RL, Hardten D, Davis E (2004) Concentrations of levofloxacin, ofloxacin, and ciprofloxacin in human corneal stromal tissue and aqueous humor after topical administration. Cornea 23(3):255–263
Jensen MK, Fiscella RG, Crandall AS, Moshirfar M, Mooney B, Wallin T, Olson RJ (2005) A retrospective study of endophthalmitis rates comparing quinolone antibiotics. A J Ophthalmol 139(1):141–148
Kirsch LS, Jackson WB, Goldstein DA, Discepola MJ (1995) Perioperative ofloxacin vs. tobramycin: efficacy in external ocular adnexal sterilization and anterior chamber penetration. Can J Ophthalmol 30(1):11–20
Koch HR, Kulus SC, Roessler M, Ropo A, Geldsetzer K (2005) Corneal penetration of fluoroquinolones: aqueous humor concentrations after topical application of levofloxacin 0.5% and ofloxacin 0.3% eyedrops. J Cataract Refract Surg 31:1377–1385
Lichtenstein SJ, Rinehart M; Levofloxacin Bacterial Conjunctivitis Study Group (2003) Efficacy and safety of 0.5% levofloxacin ophthalmic solution for the treatment of bacterial conjunctivitis in pediatric patients. J AAPOS 7(5):317–324
Liesegang TJ (2001) Use of antimicrobials to prevent postoperative infection in patients with cataracts. Curr Opin Ophthalmol 12(1):68–74
Masket S (1998) Preventing, diagnosing, and treating endophthalmitis. J Cataract Surg 24(6):725–726
Mather R, Karenchak LM, Romanowski EG, Kowalski RP (2002) Fourth generation fluoroquinolones: new weapon in the arsenal of ophthalmic antibiotics. Am J Ophthalmol 133(4):463–466
Naber KG, Adam D (1998) Classification of fluoroquinolones. Int J Antimicrob Agents 10(4):255–257
Neu HC, Chin NX (1989) In vitro activity of S-ofloxacin. Antimicrob Agents Chemother 33:1105–1107
O’Brien TP, Maguire MG, Fink NE, Alfonso E, McDonnell P (1995) Efficacy of ofloxacin vs cefazolin and tobramycin in the therapy for bacterial keratitis. Report from the Bacterial Keratitis Study Research Group. Arch Ophthalmol 113(10):1257–1265
Prajna NV, George C, Selvaraj S, Lu KL, McDonnell PJ, Srinivasan M (2001) Bacteriologic and clinical efficacy of ofloxacin 0.3% versus ciprofloxacin 0.3% ophthalmic solutions in the treatment of patients with culture-positive bacterial keratitis. Cornea 20(2):175–178
Robertson SM, Curtis MA, Schlech BA, Rusinko A, Owen GR, Dembinska O, Liao J, Dahlin DC (2005) Ocular pharmacokinetics of moxifloxacin after topical treatment of animals and humans. Surv Ophthalmol 50 [Suppl 1]:S32–S35
Schwalb IR, Friedländer M, McCulley J, Lichtenstein SJ, Moran CT; Levofloxacin Bacterial Conjunctivitis Active Control Study Group (2003) A phase III clinical trial of 0.5% levofloxacin ophthalmic solution versus 0.3% ofloxacin ophthalmic solution for the treatment of bacterial conjunctivitis. Ophthalmology 110(3):457–465
Ta CN, Egbert PR, Singh K, Shriver EM, Blumenkranz MS, Miño de Kaspar HM (2002) Prospective randomized comparison of 3-day versus 1-hour preoperative ofloxacin prophylaxis for cataract surgery. Ophthalmology 109(11):2036–2041
Yalvac IS, Basci NE, Bozkurt A, Duman S (2003) Penetration of topically applied ciprofloxacin and ofloxacin into the aqueous humor and vitreous. J Cataract Surg 29:487–491
Acknowledgements
This study was supported financially in part by Santen Oy, Tampere, Finland. J. Lokkila, MSc, is an employee of Santen Oy Analytical Development Laboratory in Tampere. None of the authors has a proprietary or commercial interest in any product mentioned or concept discussed in this article. The authors thank K. Kontra, Mc.Pharm, H. Käsnänen, RN and A. Kaakkola, RN, Kuopio University Hospital, Kuopio, Finland, for their assistance in technical and practical arrangements during the study.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was supported financially in part by Santen Oy, Tampere, Finland.
Rights and permissions
About this article
Cite this article
Puustjärvi, T., Teräsvirta, M., Nurmenniemi, P. et al. Penetration of topically applied levofloxacin 0.5% and ofloxacin 0.3% into the vitreous of the non-inflamed human eye. Graefe's Arch Clin Exp Ophthalmol 244, 1633–1637 (2006). https://doi.org/10.1007/s00417-006-0360-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-006-0360-0