
Abstract
Purpose
To investigate interocular differences in retrobulbar flow velocities in patients with asymmetric glaucomatous visual field loss.
Methods
Twenty-five patients with primary open-angle glaucoma (POAG) and asymmetric visual field loss were included in this study. Asymmetric visual field loss was defined as a difference of the global index mean deviation (MD) >6 dB between the two eyes. Flow velocities (peak systolic velocity PSV and end-diastolic velocity EDV) and resistive indices (RI) of the ophthalmic artery (OA), central retinal artery (CRA), and nasal and temporal posterior ciliary arteries were measured by means of colour Doppler imaging.
Results
MD of eyes with more severe glaucomatous visual field loss was −18.3±7.8 dB vs −6.8±5.5 dB (p<0.0001) in the less affected eyes. The PSV and the EDV of the CRA and the PSV of the OA were significantly decreased in eyes with more severe glaucomatous visual field loss (CRA PSV: 7.6±2.0 cm/s vs 8.3±1.7 cm/s, p=0.04; CRA EDV: 2.24±0.5 cm/s vs 2.55±0.6 cm/s, p<0.007; OA PSV: 29.7±9.9 cm/s vs 32.7±11.5 cm/s, p<0.02). None of the other differences in velocity or resistive index were significant.
Conclusions
Patients with asymmetric glaucomatous visual field loss exhibit asymmetric flow velocities of the CRA and OA. Patients with more severe damage display reduced flow velocities in retrobulbar vessels in POAG.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Haemodynamic abnormalities of the optic nerve head, the retina, retrobulbar blood vessels, and the choroid have been shown to be present in glaucomatous optic neuropathy [1, 2, 3, 10, 16, 18, 25, 23, 24]. Flow velocities of retrobulbar vessels, i.e. the central retinal artery, the ophthalmic artery, and the short posterior ciliary arteries, can be measured by means of colour Doppler imaging. Colour Doppler imaging is an ultrasound technique combining a B-mode ultrasound image with colour- representing movements based on Doppler frequency shifts [14, 26, 36].
Previous studies investigated blood flow velocities of retrobulbar vessels in patients with open-angle glaucoma. Most of the studies confirmed reduced end-diastolic velocities associated with elevated resistive indices in the central retinal artery and the posterior ciliary arteries. Reduced peak systolic velocities of these vessels tended to be a less obvious phenomenon [ 6, 11–13, 15, 17, 18, 24, 28, 34, 35]. Concerning the ophthalmic artery, the results are less evident. Though reduced blood flow velocities and increased resistive indices have been reported [13, 17, 18, 24, 30], elevated as well as normal peak velocities were found in POAG [5, 35, 37]. Studies comparing retrobulbar haemodynamics of patients with normal-tension glaucoma (NTG) and primary open-angle glaucoma (POAG) confirmed no statistically significant difference [5, 18, 26, 35].
The study presented here aimed to investigate blood flow velocities of retrobulbar vessels in asymmetric glaucoma defined by visual field defects. Interocular asymmetry in glaucomatous visual field loss was compared with interocular blood flow velocity differences.
Patients
Twenty-five patients with POAG and asymmetric glaucomatous visual field loss were included in this prospective study.
All of these 25 individuals had glaucomatous optic nerve head cupping and glaucomatous visual field defects as defined by the European Glaucoma Society [9], in the absence of retinal or neurological disease affecting the visual field. Visual field loss was considered significant when the glaucoma hemifield test was abnormal, three contiguous points were confirmed with p<0.05 probability of being normal, not contiguous with the blind spot, or corrected pattern standard deviation (CPSD) was abnormal with p<0.05. All parameters were confirmed on two consecutive visual fields performed with the Humphrey Visual Field Analyzer (full threshold program 24–2). Patients with POAG had intraocular pressure readings >21 mmHg at least twice in the patient’s medical history. Visual acuity was 20/40 or better and no previous laser or surgical treatment had been performed. Patients with refractive aberrations of more than ±8 diopters, or with diabetic retinopathy were excluded from this study.
To avoid any effect of local treatment on blood flow asymmetry analysis, all patients included in the study had to receive the same local treatment on both eyes.
Based on their medical casenotes, 14 of the 25 patients suffered from systemic arterial hypertension that was treated medically, and 2 patients had a history of peripheral vasospastic disease (i.e. cold hands and feet).
Methods
Each of the 25 patients underwent a detailed ophthalmological examination, visual field testing and colour Doppler imaging of their retrobulbar blood vessels.
Visual field examinations were performed with the Humphrey Visual Field Analyzer (Model 750, Humphrey–Zeiss, San Leandro, California) using the white-on-white 24–2 full threshold program. The visual field global indices mean deviation (MD) and pattern standard deviation (PSD) were used for statistical analysis. Asymmetric visual field loss was defined using interocular asymmetry in MD due to glaucomatous visual field damage. An interocular difference in MD >6 dB was regarded as asymmetric glaucomatous visual field loss. This threshold was used following in part the criteria of the European Glaucoma Society defining early, moderate and advanced glaucomatous visual field loss [9].
Blood flow velocities of retrobulbar vessels of both eyes were measured by means of colour Doppler imaging (CDI) using a 7.5-MHz linear phased-array transducer (Siemens Sonoline Sienna, Germany). The transducer was gently placed on the closed upper eyelid using a coupling gel, taking care to minimise pressure on the globe. All subjects were in the supine position during the examination. CDI permits blood velocity measurements of the ophthalmic artery (OA), the central retinal artery (CRA), and the temporal and nasal short posterior ciliary arteries (TPCA and NPCA). The peak systolic velocity (PSV) and the end-diastolic velocity (EDV) were obtained from the velocity waves of each artery. The resistive index (Pourcelot’s ratio) was calculated [(PSV–EDV)/PSV] to characterise peripheral vascular resistance of the vessels studied [26, 36]. The operator was blinded to the asymmetry of the disease.
Before CDI was performed, intraocular pressure was measured by applanation tonometry (Goldmann) and systolic (SBP) and diastolic (DBP) blood pressure and heart rate were measured after a resting time of 5 min. Mean arterial pressure (MAP) and ocular perfusion pressure were calculated from this data [MAP: DBP +1/3 (SBP−DBP)]; perfusion pressure: 2/3 MAP−IOP) [16].
Adherence to the Declaration of Helsinki for research involving human subjects is confirmed. Informed consent was obtained from all individuals including the analysis of the data. All investigators had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
For the statistical analysis of this study, retrobulbar blood velocities of both eyes were used. A paired non-parametric test (Wilcoxon signed rank test) was applied for comparisons of eyes with more advanced glaucomatous visual field loss versus earlier visual field loss. In all analyses, p<0.05 was regarded as statistically significant.
Results
Patients with POAG and asymmetric visual field loss (mean age 63±12 years) showed significant differences in cup-to-disc-ratios between the two eyes. There was no significant difference in intraocular pressure measured before colour Doppler imaging and ocular perfusion pressure. SBP was 139±16 mmHg, DBP 80±10 mmHg, and MAP 99±10 mmHg. The clinical data are listed in Table 1.
The PSV of the OA and the PSV and EDV of the CRA were significantly lower in the eyes with more advanced glaucomatous visual field loss than in the less affected eyes. No significant differences were found for the resistive indices of the OA, CRA, or PCAs. The PCAs did not show any significant difference between eyes. In Table 2 the results are presented and previously acquired normative data are provided as a reference for each parameter.
No significant interaction was found for the diagnosis of arterial hypertension on asymmetry findings in blood flow velocities of retrobulbar vessels (PSV of the OA: p=0.09; EDV of the OA: p=0.32; PSV of the CRA: p=0.16; EDV of the CRA: p=0.16).
Discussion
Reduced blood flow velocities of retrobulbar vessels are a well-known phenomenon in glaucomatous optic neuropathy [17, 24, 26].
Several studies investigated the association of retrobulbar flow velocities with the extent of functional defects in glaucomatous optic neuropathy. Flow velocities of the CRA and PCAs tended to be decreased in advanced disease and were correlated to global indices in glaucoma [7, 20, 24, 27]. The eyes with glaucoma were divided into early and late glaucoma based on visual field criteria, but no interocular comparisons were made in these studies [7, 20]. Interocular comparisons of ocular blood flow parameters in asymmetric glaucoma may yield more insight in perfusion alterations primarily related to glaucomatous optic neuropathy, as systemic factors will influence both eyes similarly in chronic vascular disease.
Interocular comparisons have been performed based on morphological criteria defining asymmetric glaucoma. Nicolela et al. [21] found significant differences in CRA flow velocities, though Costa et al. [8] did not detect significant differences. Both studies refer to a cohort of glaucoma patients including secondary glaucoma due to pigmentary dispersion and pseudexfoliation, and the clinical data on visual field asymmetry are not presented. In a study on interocular comparison in NTG patients, Kondo et al. [19] defined a concordant and a disconcordant group based on ocular perfusion pressure and MD. The authors speculate that haemodynamic abnormalities may be predominant in the disconcordant patient group (i.e. higher ocular perfusion pressures related to a worse MD) as blood flow velocities were significantly lower than in the concordant group. A significant asymmetry was found for the EDV of the CRA in the concordant patient group. O’Brien et al. [22] reported an asymmetry in pulsatility indices and resistance indices of the internal carotid artery in asymmetric POAG based on a visual field scoring system. In contrast, Breil et al. [4] did not detect any significant differences in blood flow velocities between asymmetric OAG and symmetric glaucoma. Differences in biostatistical analysis may account for these findings. The authors used a subtraction of the left and the right eye in the symmetric glaucoma patient group, and the difference between eyes in the asymmetric glaucoma group. Sponsel et al. reported a significant correlation between asymmetry of visual function and asymmetry of retinal leukocyte velocities using the blue field entoptic phenomenon [33].
In the present study, a definition based on visual field asymmetry was applied to perform interocular comparisons in asymmetric glaucoma. A significant difference was found between eyes for the PSV and the EDV of the CRA and for the PSV of the OA. No significant differences were found for the PCAs. In addition, there was no significant difference in intraocular pressure and ocular perfusion pressure between eyes. The findings on EDV of the CRA are in agreement with previous studies by Nicolela et.al. [21] on morphological asymmetry in glaucoma, and Kondo et.al. [19] on perfusion pressure and visual field asymmetry. Studies referring to correlations of visual field and CDI in glaucoma not based on interocular differences confirm the role of the EDV of the CRA [24, 27].
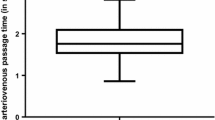
The blood flow velocities of the CRA are influenced by its downstream resistance. A higher downstream resistance in ocular blood flow may be caused by elevated intraocular pressure, vasoconstriction, vasospasm, vasosclerosis or reduced cross section of the vascular bed, e.g. capillary loss. Vasoconstriction of retinal arterioles does not seem to account for reduced flow velocities in asymmetric disease, as Remky et al. did not detect a significant difference in retinal vessel diameters in asymmetric glaucoma [29]. In a previous study on fluorescein filling defects and CDI in NTG, a significant correlation was found between blood flow velocities of the CRA and PCAs and capillary loss of the optic nerve head [24]. In addition, the EDV of the CRA was correlated to the retinal arteriovenous passage time on fluorescein angiography [17]. Simultaneous reductions of PSV and EDV of the CRA may be interpreted as reduced volumetric flow in this vessel [32]. Reduced flow velocities in the CRA of a glaucomatous eye may reflect a chronic decrease in perfusion of the inner retinal layers secondary to nerve fibre loss. Reduced flow velocities have been shown to be predictive for future damage to the nerve fibres in glaucoma [31]. A direct comparison of the extent of flow reduction is based on the detection of vessel diameters that may not be measured by means of CDI. Interestingly, this study could not detect significant differences in flow velocities of the PCAs, i.e. in the vessels primarily relevant for optic nerve perfusion. A higher variability in the measurement of flow in the PCAs may account for this finding [14]. The EDV of the OA was decreased in advanced disease. Various studies reported reduced flow velocities in glaucoma [13, 17, 18, 24, 30], and in asymmetric disease even internal carotid artery flow indices were found to be significantly different. Global ocular perfusion parameters may not be directly related to optic nerve head or retinal microcirculation, but hint that decreased ocular perfusion emphasises vascular disease in glaucoma.
Although calculated ocular perfusion pressure was similar in both eyes in asymmetric glaucoma, reduced retrobulbar blood flow velocities were confirmed in advanced disease. The diagnosis of arterial hypertension showed no statistically significant influence on asymmetry of blood flow velocities in our study. This hints at a decreased ocular perfusion in the more damaged glaucomatous eye not related to systemic blood pressure indices.
The presented study of asymmetric flow velocities in the CRA and OA included patients with a wide range of visual field defects. Patients with advanced disease may exhibit decreased flow velocities by secondary down-regulation due to the neural tissue loss. Therefore, tissue perfusion could be normal in relation to the loss of ganglion cells. The issue of the temporal relationship between retrobulbar flow velocities and glaucomatous damage accounts for the need for prospective longitudinal studies. In a retrospective study, Satilmis et al. showed that eyes with reduced flow velocities showed greater field progression than those with less reduced or normal flow velocities [31].
To summarise, this study emphasises the importance of reduced flow velocities of the central retinal artery related to a higher downstream resistance in ocular perfusion. There is an association between interocular asymmetry in glaucoma based on functional definition of the disease and blood flow velocities.
References
Arend O, Plange N, Sponsel WE, Remky A (2004) Pathogenetic aspects of the glaucomatous optic neuropathy: fluorescein angiographic findings in patients with primary open-angle glaucoma. Brain Res Bull 62:517–524
Arend O, Remky A, Cantor LB, Harris A (2000) Altitudinal visual field asymmetry is coupled with altered retinal circulation in patients with normal pressure glaucoma. Br J Ophthalmol 84:1008–1012
Arend O, Remky A, Redbrake C, Arend S, Wenzel M, Harris A (1999) Retinale Hämodynamik bei Patienten mit Normaldruckglaukom. Quantifizierung mittels digitaler Scanning-Laser-Fluorescein-Angiographie. Ophthalmologe 96:24–29
Breil P, Krummenauer F, Schmitz S, Pfeiffer N (2002) Verhältnis zwischen retrobulbären Blutflussgeschwindigkeiten und glaukomatösem Schaden: en interindividueller Vergleich. Ophthalmologe 99:613–616
Butt Z, O’Brien C, McKillop G, Aspinall P, Allan P (1997) Color Doppler imaging in untreated high- and normal-pressure open-angle glaucoma. Invest Ophthalmol Vis Sci 38(3):690–696
Cellini M, Possati GL, Caramazza N, Caramazza R (1996) Colour Doppler analysis of the choroidal circulation in chronic open-angle glaucoma. Ophthalmologica 210:200–202
Cellini M, Possati GL, Sbrocca M, Caramazza N (1996) Correlation between visual field and color Doppler parameters in chronic open angle glaucoma. Int Ophthalmol 20:215–219
Costa VP, Sergott RC, Smith M, Spaeth GL, Wilson RP, Moster MR, Katz LJ, Schmidt CM (1994) Color Doppler imaging in glaucoma patients with asymmetric optic cups. J Glaucoma 3 [Suppl 1]:S91–S97
Greve EL et al (eds) (1998) Terminology and guidelines for glaucoma. European Glaucoma Society, Editrice Dogma, Savona, Italy
Flammer J, Orgül S (1998) Optic nerve blood-flow abnormalities in glaucoma. Prog Ret Eye Res 17(2):267–289
Galassi F, Sodi A, Rossi MG, Ucci F, De Saint Pierre F (1997) Ocular haemodynamics in some subgroups of normal pressure glaucoma. Acta Ophthalmol Scand 224 [Suppl]:35–36
Galassi F, Nuzzaci G, Sodi A, Casi P, Vielmo A (1992) Color Doppler imaging in evaluation of optic nerve blood supply in normal and glaucomatous subjects. Int Ophthalmol 16:273–276
Guthoff RF, Berger RW, Winkler P, Helmke K, Chumbley LC (1991) Doppler ultrasonography of the ophthalmic and central retinal vessels. Arch Ophthalmol 109:532–536
Harris A, Kagemann L, Cioffi GA (1998) Assessment on human ocular hemodynamics. Surv Ophthalmol 42:509–533
Harris A, Sergott RC, Spaeth GL, Katz JL, Shoemaker JA, Martin BJ (1994) Color Doppler analysis of ocular vessel blood velocity in normal-tension glaucoma. Am J Ophthalmol 118:642–649
Hayreh SS (1995) The 1994 Von Sallman Lecture: the optic nerve circulation in health and disease. Exp Eye Res 61:259–272
Huber K, Plange N, Remky A, Arend O (2004) Comparison of colour Doppler imaging and retinal scanning laser fluorescein angiography in healthy volunteers and normal pressure glaucoma patients. Acta Ophthalmol Scand 82:426–431
Kaiser HJ, Schoetzau A, Stümpfig D, Flammer J (1997) Blood-flow velocities of the extraocular vessels in patients with high-tension and normal-tension primary open-angle glaucoma. Am J Ophthalmol 123:320–327
Kondo Y, Niwa Y, Yamamoto T, Sawada A, Harris A, Kitazawa Y (2000) Retrobulbar hemodynamics in normal-tension glaucoma with asymmetric visual field change and asymmetric ocular perfusion pressure. Am J Ophthalmol 130:454–460
Liu CJ, Chiou H-J, Chiang S-C, Chou JC, Chou Y-H, Liu J-H (1999) Variations in ocular hemodynamics in patients with early and late glaucoma. Acta Ophthalmol Scand 77:658–662
Nicolela MT, Drance SM, Rankin SJ, Buckley AR, Walman BE (1996) Color Doppler imaging in patients with asymmetric glaucoma and unilateral visual field loss. Am J Ophthalmol 121:502–510
O’Brien, Saxton V, Crick RP, Meire H (1992) Doppler carotid artery studies in asymmetric glaucoma. Eye 6:273–276
Plange N, Kaup M, Weber A, Remky A, Arend (2004) Fluorescein filling defects and quantitative morphologic analysis of the optic nerve head in glaucoma. Arch Ophthalmol 122:195–201
Plange N, Remky A, Arend O (2003) Colour Doppler imaging and fluorescein filling defects of the optic disc in normal tension glaucoma. Br J Ophthalmol 87:731–736
Plange N, Remky A, Arend O (2001) Papilläre Füllungsdefekte in Fluoreszein-Angiographien bei Glaukom - Eine retrospektive klinische Studie. Klin Monatsbl Augenheilkd 218:214–221
Rankin SJA (1999) Color Doppler imaging of the retrobulbar circulation in glaucoma. Surv Ophthalmol 43 [(Suppl 1]:S176–S182
Rankin SJ, Drance SM, Buckley AR, Walman BE (1996) Visual field correlations with color Doppler studies in open angle glaucoma. J Glaucoma 5:15–21
Rankin SJ, Walman BE, Buckley AR, Drance SM (1995) Color Doppler imaging and spectral analysis of the optic nerve vasculature in glaucoma. Am J Ophthalmol 119:685–693
Remky A, Plange N, Klok J, Arend O (2004) Retinal arterial diameters in patients with glaucoma. Spektrum Augenheilkd 18:25–30
Rojanapongpun P, Drance SM, Morrison BJ (1993) Ophthalmic artery flow velocity in glaucomatous and normal subjects. Br J Ophthalmol 77:25–29
Satilmis M, Orgül S, Doubler B, Flammer J (2003) Rate of progression of glaucoma correlates with retrobulbar circulation and intraocular pressure. Am J Ophthalmol 135:664–669
Spencer JA, Giussani DA, Moore PJ, Hanson MA (1991) In vitro validation of Doppler indices using blood and water. J Ultrasound Med 10:305–308
Sponsel WE, DePaul L, Kaufman PL (1990) Correlation of visual function and retinal leukocyte velocity in glaucoma. Am J Ophthalmol 109:49–54
Trible JR, Costa VP, Sergott RC, Spaeth GL, Smith M, Wilson RP, Katz LJ, Moster MR, Schmidt CM (1993) The influence of primary open-angle glaucoma upon the retrobulbar circulation: baseline, postoperative and reproducibility analysis. Trans Am Ophthalmol Soc 91:245–265
Vécsei PV, Hommer A, Reitner A, Kircher K, Egger S, Schneider B, Bettelheim HC (1998) Farbduplex der retrobulbären Arterien bei Normaldruck- und Offenwinkelglaukom. Klin Monatsbl Augenheilkd 212:444–448
Williamson TH, Harris A (1996) Color Doppler imaging of the eye and orbit. Surv Ophthalmol 40:225–267
Yamazaki Y, Hayamizu F (1995) Comparison of flow velocity of ophthalmic artery between primary open angle glaucoma and normal tension glaucoma. Br J Ophthalmol 79:732–734
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Plange, N., Kaup, M., Arend, O. et al. Asymmetric visual field loss and retrobulbar haemodynamics in primary open-angle glaucoma. Graefe's Arch Clin Exp Ophthalmo 244, 978–983 (2006). https://doi.org/10.1007/s00417-005-0227-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-005-0227-9