
Abstract
Background.
In a previous study it was shown that nimodipine 30 mg twice daily leads to an improvement in the visual field in a subgroup of normal-pressure glaucoma patients. To understand the mechanism of action of nimodipine on the visual system, the aim of this study was to examine the influence of nimodipine on different hemodynamic parameters and contrast sensitivity in healthy subjects.
Methods.
Thirty-two healthy subjects (21–49 years old, mean age 28 years, 10 male, 22 female) received either nimodipine 30 mg twice a day or a placebo according to the same dosage regimen in a double-blind cross-over study design. The ocular blood flow was measured by means of the ocular blood flow system, the optic nerve head blood flow with the continuous laser Doppler flowmeter (Riva), and contrast sensitivity using the MCT 8000 Multivision Contrast Tester. Measurements were taken at baseline (1T0), 120 min after initial dose (1T3) and after 3 days (3T3) of therapy with 150 mg nimodipine or placebo in total.
Results.
Contrast sensitivity improved significantly throughout almost all spatial frequencies in the nimodipine-treated subjects ( P =0.01), whereas there was no change in the placebo group. Ocular blood flow and optic nerve head blood flow increased slightly but not significantly in the nimodipine group (1T0: 706.6 µl/min, 9.33 AU; 3T3: 854.3 µl/min, 9.39 AU) and remained unchanged or were even lower in the placebo group ( P >0.05).
Conclusion.
The results showed a significant increase in contrast sensitivity during treatment with nimodipine in healthy subjects. This increase in visual function, however, was not correlated with an increase in ocular or optic nerve head blood flow. Therefore, another mechanism, e.g., a direct effect on the visual system, might be responsible for the improvement in visual function in healthy volunteers under nimodipine therapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Over the past few years improvement of ocular hemodynamics and neuroprotection have assumed more importance in glaucoma research. Although intraocular pressure (IOP) is still the most important risk factor for the development of glaucomatous optic nerve atrophy, normal-pressure glaucoma demonstrates that other risk factors might play a role in the pathogenesis of this disease [5, 7].
Because of the high coincidence of vasospastic disorders such as Raynaud's syndrome or migraine with normal-pressure glaucoma [6,17], it was postulated that vasospastic disorders might be important in the course of normal-pressure glaucoma [8]. Several studies showed evidence that al least some normal-pressure glaucoma patients with vasospastic risk factors might benefit from treatment with calcium-channel blockers e.g., nimodipine [2, 11, 14, 15,18].
Nimodipine [10, 21] is an antagonist of the 1,4-dihidropyridine class and prevents the influx of calcium ions through the voltage- and receptor-activated "slow" channels of the cell membrane. Nimodipine acts as a smooth muscle cell relaxant. It dilates cerebral arteries and arterioles and increases cerebral blood flow in animals and humans without having any major influence on systemic blood pressure. Because of its lipophil structure nimodipine passes the blood–brain barrier, and for this reason it is commonly used in the treatment of a wide range of cerebrovascular disorders, particularly for prophylaxis and treatment of delayed ischemic neurological deficits resulting from cerebral vasospasm in patients with subarachnoid hemorrhage or acute ischemic stroke and in dementia [1, 21]. For the therapy of cerebrovascular ischemia due to vasospasm a dosage of 60 mg six times a day is used, and a dosage of 30 mg three times a day is recommended for the treatment of dementia.
As the blood vessels of the optic nerve are comparable to those of the central nervous system there have been attempts to use calcium-channel blockers in the therapy of glaucoma. However, even a lower dosage of nimodipine (30 mg twice a day) leads to an improvement in the visual field in a subgroup of normal-pressure glaucoma patients [2].
To help elucidate the mechanism of action of nimodipine on the visual system, the aim of the present study was to examine the influence of nimodipine 30 mg twice a day on contrast sensitivity and on different hemodynamic parameters in healthy subjects.
Patients and methods
Patients
Thirty-two healthy subjects (10 men and 22 women between 21 and 49 years of age, mean 28 years) were examined. They had no visual field defects, glaucomatous cupping of the optic nerve head, ocular hypertension, or history of glaucoma or vasospasm, e.g., migraine, frequent headaches, cold hands or feet, or tinnitus. Each subject received either nimodipine 30 mg twice a day or a placebo according to the same dosage regimen in a double-blind cross-over design. Measurements were taken at baseline and at 120 min and 3 days after the morning dose with 150 mg nimodipine in total or placebo. At each time point, systemic blood pressure, heart rate, IOP, optic nerve head blood flow, ocular blood flow, and contrast sensitivity were measured.
Because of the small number of subjects a normal distribution of the parameters could not be assumed. Therefore, the Wilcoxon test, a non-parametric paired test, was used for the statistical analysis. To correct for multiple testing, the significance level was set to P =0.01. Differences that were not statistically significant were divided between those where P was >0.01 and those where P was >0.05.
Methods
The IOP was measured by applanation tonometry according to Goldmann.
Measurements of the ocular blood flow were performed using the ocular blood flow system (OBF). This instrument is a pneumotonometer and measures the IOP every 30 ms.
With each heart beat a blood bolus enters the eye and causes an increase in intraocular volume. Because of the scleral rigidity each increase in volume causes a corresponding brief increase in IOP. The difference between the maximum and the minimum IOP is the ocular pulse amplitude, which is measured by the instrument (in mmHg). In addition, the instrument calculates the pulsatile ocular blood flow (in µl/min) [12].
Measurements of the blood flow in the optic nerve head were performed by means of the continuous laser Doppler flowmeter according to Riva. This method is based on the optic Doppler effect. A diode laser beam with 160 µm diameter and a wavelength of 670 nm is aimed at the optic nerve head. The laser light is shifted in frequency by the moving red blood cells and the stationary tissue. This broadened mixture of different frequencies is reflected and detected by a photodetector. Using a fast Fourier transformation followed by a power spectral analysis, a Doppler shift power spectrum (DSPS) is calculated. From these data the parameters velocity, volume, and flow are calculated. The parameter velocity represents the relative mean speed of the moving red blood cells and is proportional to the mean Doppler frequency shift. The parameter volume represents the number of moving red blood cells in the sampling volume and is proportional to the area under the curve of the DSPS. The parameter flow is calculated by multiplying volume by velocity. Velocity is expressed in kHz and the parameters volume and flow in arbitrary units (AU) [20].
Measurements of the contrast sensitivity were performed with the MCT 8000 Multivision contrast tester (Vistech), a near vision contrast tester. This instrument is a box (17.5×14 cm) with five rows of nine circles each arranged on the surface. Each circle represents a sinusoidal wave pattern with diminishing spatial frequencies from the upper to the lower row and diminishing contrast levels from left to right. The sinusoidal wave patterns are presented in four different directions: the wave pattern is in either a vertical position or turned 15° to the left or right, or the circle is blank. In this study the test was performed in a dark-adapted and in a light-adapted mode. For each different spatial frequency the last circle correctly identified was determined. The contrast sensitivity is measured in arbitrary units [16].
Results
There was no statistically significant change in systemic blood pressure, heart rate, or IOP either 120 min or 3 days after treatment with either nimodipine or placebo ( P >0.05).
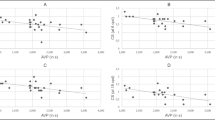
The pulsatile ocular blood flow was 706.6 µl/min at baseline and 833.4 µl/min 120 min and 854.3 µl/min 3 days after treatment with nimodipine. The increase was not statistically significant with P >0.05. The placebo group showed a slight decrease in the pulsatile ocular blood flow from 660.6 µl/min at baseline to 701.5 µl/min at 120 min and 640.2 µl/min at 3 days. These changes were not statistically significant P >0.05 (Table 1, Fig. 1). The parameter pulse volume and pulse amplitudes showed no significant changes ( P >0.05) (Table 1).

Pulsatile ocular blood flow (POBF) under treatment with nimodipine and placebo
The optic nerve head blood flow was 9.33 AU at baseline, 9.47 AU 120 min, and 9.39 AU 3 days after treatment with nimodipine. The slight increase was not statistically significant ( P >0.05). The optic nerve head blood flow was 9.40 AU at baseline, 9.35 AU 120 min, and 9.44 AU 3 days after placebo treatment (Table 2, Fig. 2).The parameters volume and velocity showed no significant change ( P >0.05)(Table 2).

Optic nerve head blood flow under treatment with nimodipine and placebo
Contrast sensitivity showed a significant increase throughout almost all spatial frequencies in the nimodipine-treated subjects after 120 min and after 3 days in dark-adapted (Table 3) and in light-adapted (Table 4) conditions ( P =0.01). The placebo group did not show any statistically significant changes in mean contrast sensitivity ( P >0.05; Table 3, Table 4).
The increase in contrast sensitivity was more pronounced at high spatial frequencies (1.5°, 3° and 6°). For example, at a spatial frequency of 6° the contrast sensitivity increased from 16.8 AU at baseline to 55.1 AU 120 min and to 58.3 AU 3 days after treatment with nimodipine under dark-adapted condition ( P =0.01). The placebo group did not show statistically significant changes under the same conditions (21.6 AU at baseline, 20.0 AU after 120 min, 21.2 AU after 3 days; P >0.05) (Fig. 3).

Mean contrast sensitivity at spatial frequency of 6° under dark-adapted conditions and treatment with nimodipine and placebo
Discussion
In the present study healthy subjects showed a significant increase in contrast sensitivity for almost all spatial frequencies under treatment with nimodipine.
This finding is similar to previously reported results. In a study performed by Bose and coworkers an increase in contrast sensitivity was found in healthy subjects and normal-pressure glaucoma patients 2 h after oral administration of 60 mg nimodipine. The authors hypothesized that the increase in contrast sensitivity might be caused by an increase in blood flow because of a relief of vasospasm or by a direct effect on the retina or the optic nerve [3]. In the present study we did not find a significant increase in any hemodynamic parameters e.g., blood flow of the optic nerve head or ocular blood flow measured by OBF. In addition, Piltz and coworkers did not find a change in macular hemodynamics 90 min after oral administration of 60 mg nimodipine despite an increase of contrast sensitivity in normal-pressure glaucoma patients and healthy controls [19]. Therefore, it seems unlikely that an increase in parameters of ocular hemodynamics is responsible for the increase in contrast sensitivity in healthy subjects.
In patients with vasospastic normal-pressure glaucoma, however, an increase of ocular pulse volumes during 18 months treatment with 30 mg nimodipine twice a day was shown. Normal-pressure glaucoma patients without vasospasm did not show significant changes [2]. This suggests that if vasospasm is present, the relaxation of the ocular vessels leads to an increase in ocular hemodynamics, which could contribute to the increase in contrast sensitivity. However, if no vasospasm is present, like in healthy subjects, the increase in ocular hemodynamics seems to be of minor importance.
Studies dealing with other calcium-channel blockers also detected changes in ocular hemodynamics in healthy subjects and animals. Netland and coworkers showed a decrease in the resistance index of the central retinal artery in healthy subjects after a single drop of verapamil [15]. Harino and coworkers reported an increase in optic nerve head blood flow in the cat after intravenous administration of nicardipine [9].
In the present study we used instruments similar to the ones employed in those studies to evaluate the ocular hemodynamics. Firstly, we used a laser Doppler flowmeter resembling the one used in the study by Harino [9, 20]. This instrument measures the optic nerve head blood flow. It has a penetration depth of up to 1000 µm and measures the blood flow of the superficial nerve fiber layer and the deeper capillary bed of the prelaminar and laminar region of the optic nerve head.
Secondly, we used the OBF to measure the pulsatile ocular blood flow of the whole eye[12]. As the choroid represents almost 85% of the vascular bed of the eye this parameter seems to represent mainly the choroidal circulation. The OBF measures a parameter similar to the oculo-oscillo-dynamography that was used in the study performed by Böhm and Pillunat, where an increase in the ocular pulse amplitude was shown in vasospastic normal-pressure glaucoma patients [2, 12]. However, in the present study we were not able to detect changes after oral administration of nimodipine in healthy subjects with either technique.
This leads to the hypothesis that in healthy subjects other factors may be responsible for improvement of visual function under treatment with nimodipine.
Nimodipine is a centrally acting calcium-channel antagonist. Binding at specific dihydropyridine receptors, nimodipine prevents the influx of calcium ions through voltage- and receptor-activated channels of the cell membrane. This effect is observed at two different locations. Firstly, at the membrane of smooth muscle cells nimodipine acts as a relaxant. The vessels dilate and the blood flow increases. Secondly, the calcium antagonism is present at the neuron and influences its electrical activity and the neurotransmitter system [10]. As no study, including the present one, has yielded any evidence that nimodipine leads to an increase in ocular hemodynamics in healthy subjects, it seems likely that the vessel-dilating effect of nimodipine is negligible in healthy subjects with presumable intact autoregulation. Therefore, the modulating effect of nimodipine on the neuronal system might be the reason for the increase in contrast sensitivity in healthy subjects [4, 10, 13,22].
In conclusion, calcium-channel blockers lead to an improvement in contrast sensitivity in healthy subjects and normal-pressure glaucoma patients. There is evidence that some calcium-channel blockers improve ocular hemodynamics in normals and normal-pressure glaucoma patients. However, with regard to nimodipine, no study has shown an increase in any hemodynamic parameter under treatment with nimodipine in healthy subjects. In our study no increase in either optic nerve head blood flow or ocular blood flow could be shown. Therefore, it seems likely that other than hemodynamic mechanisms, e.g., modulation of the neuronal activity, are responsible for the increase in contrast sensitivity in normal subjects. Further studies are needed to elucidate the mechanism of action of nimodipine on visual function.
References
Biersack K, Rosskopf R, Eckert H, Pasz T (1992) Wirksamkeit und Verträglichkeit von Nimodipin bei Langzeitbehandlung von Patienten mit Hirnleistungsstörungen. Z Ärztl Fortbild 86:451–456
Böhm AG, Pillunat LE (1999) Kalziumantagonisten in der Langzeittherapie des Normaldruckglaukoms. In: Schmidt KG, Pillunat LE (eds) Fortbildung Glaukom, Band 1: Perfusion und Pharmakologie. Enke, Stuttgart, pp 69–83
Bose S, Piltz JR, Breton ME (1995) Nimodipine, a centrally active calcium antagonist, exerts a beneficial effect on contrast sensitivity in patients with normal-tension glaucoma and in control subjects. Ophthalmology 102(8):1236–1241
Caprioli J (1997) Neuroprotection of the optic nerve in glaucoma. Acta Ophthalmol Scand 75:364–367
Drance SM (1972) Some factors in the production of low tension glaucoma. Br J Ophthalmol 56:229–242
Drance SM, Douglas GR, Wijsman K, Schulzer M, Britton RJ (1988) Response of blood flow to warm and cold in normal and low-tension glaucoma patients. Am J Ophthalmol 105:35–39
Flammer J, Haefliger IO, Orgül S, Resink T (1999) Vascular dysregulation: a principal risk factor for glaucomatous damage? J Glaucoma 8:212–219
Gasser P, Flammer J, Guthauser U, Niesel P, Mahler F, Linder HR (1986) Bedeutung des vasospastischen Syndroms in der Augenheilkunde. Klin Mbl Augenheilkd 188:398–399
Harino S, Riva CE, Petrig BL (1992) Intravenous nicardipine in cats increases optic nerve head but not retinal blood flow. Invest Ophthalmol Vis Sci 33:2885–2890
Herrschaft H (1992) Nimodipine. In: Riederer P, Laux G, Pöldinger W (eds) Neuro-Psychopharmaka Bd. 5, Springer, Vienna, pp 261–289
Kitazawa Y, Shirai H, Jin Go F (1989) The effect of Ca2+-antagonist on visual field in low-rension glaucoma. Graefe's Arch Clin Exp Ophthalmol 227:408–412
Langham M (1994) Ocular blood flow and vision in healthy and glaucomatous eyes. Surv Ophthalmol 38 [Suppl]:S161-S168
Liliprandi R, Canella R, Carmignoto G, Schiavo N, Zanellato A, Zanoni R et al. (1992) N-Methyl-D-aspartate-induced neurotoxicity in the adult rat retina. Vis Neurosci 8:567–573
Netland PA, Chaturvedi N, Dreyer EB (1993) Calcium channel blockers in the management of low-tension and open-angle glaucoma. Am J Ophthalmol 115:608–613
Netland P, Grosskreutz C, Feke G, Hart L (1994) Color Doppler ultrasound analysis of ocular circulation after topical calcium channel blocker. Am J Ophthalmol 119:694–700
Neumann AC, McCarty GR, Locke J, Cobb B (1998) Glare disability devices for cataractous eyes: a consumers's guide. J Cataract Refract Surg 14:212–216
Phelps CD, Corbett JJ (1985) Migraine and low-tension glaucoma. A case-control study. Invest Ophthalmol Vis Sci 26, 8:1105–1108
Pillunat LE, Lang GK (1995) Nimodipin in der Therapie des Normaldruckglaukoms. Klin Monatsbl Augenheilkd 207:270
Piltz JR, Bose S, Lanchoney D (1998) The effect of nimodipine, a centrally active calcium antagonist, on visual function and macular blood flow in patients with normal-tension glaucoma and control subjects. J Glaucoma 7(5):336–342
Riva CE, Harino S, Petrig BL, Shonat RD (1992) Laser Doppler Flowmetry in the optic nerve. Exp Eye Res 55:499–506
Wadworth AN, McTavish D (1992) Nimodipine. A review of its pharmacological properties, and therapeutic efficacy in cerebral disorders. In Drugs & Aging 2 (4) Aids International Lim., pp 262–286
Zornow ML, Prough DS (1996) Neuroprotective properties of calcium channel blockers. New Horizons 4:107–114
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Boehm, A.G., Breidenbach, K.A., Pillunat, L.E. et al. Visual function and perfusion of the optic nerve head after application of centrally acting calcium-channel blockers. Graefe's Arch Clin Exp Ophthalmol 241, 34–38 (2003). https://doi.org/10.1007/s00417-002-0592-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-002-0592-6