
Abstract
Introduction
The clinical factors predisposing to ischemic stroke in reversible cerebral vasoconstriction syndrome (RCVS) are unclear. In this observational cross-sectional study, we aimed to evaluate the risk factors and clinical outcomes associated with the development of ischemic stroke in patients with RCVS.
Methods
We utilized the Nationwide Readmissions Database 2016–2017 to identify all hospitalizations with RCVS, with or without acute ischemic stroke. Independent predictors of and clinical outcomes associated with ischemic stroke were analyzed using logistic regression.
Results
Among 1065 hospitalizations for RCVS (mean ± SD age 49.0 ± 16.7 years, female 69.7%), 267 (25.1%) had ischemic stroke. Patients with ischemic stroke were more likely to have hypertension (OR 2.33, 95% CI 1.51–3.60), diabetes (OR 1.81, 95% CI 1.11–2.98), and tobacco use (OR 1.64, 95% CI 1.16–2.33) and were less likely to have a history of migraine (OR 0.56, 95% CI 0.35–0.90). Ischemic stroke was associated with higher odds of cerebral edema (OR 3.15, 95% CI 1.31–7.57) and respiratory failure (OR 2.39, 95% CI 1.28–4.44). Patients with ischemic stroke also had longer hospital stay by a mean duration of 6.7 days, P < 0.001, higher hospital charges by a mean of $72,961, P < 0.001, and a higher likelihood of not being discharged to home (OR 3.57, 95% CI 2.39–5.33). They had higher in-hospital mortality rate; however, the difference was not statistically significant.
Conclusion
Ischemic stroke affects nearly 25% of patients with RCVS and is associated with adverse clinical outcomes. RCVS patients with cerebrovascular risk factors might have a higher predisposition for developing ischemic lesions during the disease process.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Reversible cerebral vasoconstriction syndrome (RCVS) is characterized by diffuse, segmental cerebral artery vasoconstriction, usually heralded by severe thunderclap headaches, spontaneously resolving within 3 months [1, 2]. While most patients have a benign clinical course, a significant minority can develop stroke, which is the cause for major morbidity and mortality in this syndrome [3,4,5]. There is increasing evidence to suggest that ischemic stroke in RCVS is associated with proximal vasoconstriction [6]. However, it is still unclear what factors predispose some patients to develop the ischemic lesions. We aimed to evaluate the risk factors and outcomes associated with ischemic stroke in RCVS.
Methods
Study population
Data were obtained from the Nationwide Readmissions Database 2016–2017, developed by the Agency for Healthcare Research and Quality for the Healthcare Cost and Utilization Project [7]. The Nationwide Readmissions Database is an all-payer (Medicare, Medicaid, private insurance, and self-pay) inpatient care database with approximately 36 million discharges per year from short-term hospitals in 22 states in the U.S., representing about 50% of total national hospitalizations. The number of discharges is weighted to estimate the nationally representative statistics. All analyses in this study complied with the Healthcare Cost and Utilization Project data use agreement and the study was exempt from the Institutional Review Board as the Nationwide Readmissions Database is a publicly available database containing deidentified data.
The International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) code I67.841 was used to identify the hospitalizations with the discharge diagnosis of RCVS. Acute ischemic stroke was identified using the ICD-10 codes I63.x, I67.81, I67.82, and I67.89. Only the first RCVS hospitalization of the year for each patient was included and hospitalizations with the diagnosis of hemorrhagic stroke were excluded.
Patient characteristics, covariates, and outcomes
Baseline patient characteristics including age, sex, median household income; hospital characteristics including bed size, ownership/control, location and teaching status; and other hospitalization variables such as the expected primary payer, length of stay, total charges, and discharge disposition were extracted from the data. The ICD-10 diagnosis and procedure codes were used to identify the comorbidities, complications, and interventions performed during the hospital stay. Secondary clinical outcomes included length of stay, hospital charges, discharge disposition, and in-hospital mortality. Disposition at the time of discharge included home, transfer to a short-term hospital, skilled nursing facility, intermediate care or other type of facility, home health care, and against medical advice. Disposition outcomes other than to home were combined and assessed as a clinical outcome.
Statistical analysis
We used the survey design methods to account for data clustering and stratification to generate national estimates. Continuous variables were represented as mean [(standard deviation (SD)] and categorical variables as proportions. Predictors of ischemic stroke were screened using univariate logistic regression with results expressed as odds ratio (OR) and 95% confidence interval (CI). Multivariable analysis was performed using a stepwise backward elimination method starting with all variables from univariate analysis with P < 0.05. Multivariable model was checked for multicollinearity using a variance correlation matrix. Logistic and linear regressions were used to identify the association between ischemic stroke and the clinical outcomes. There were no missing values for variables, except for hospital charge, primary payer, and median household income, which were missing in < 1.5% of the cases. All reported P values were two-sided with P < 0.05 considered significant. All analyses were performed using Stata, version 15.0 (StataCorp, College Station, TX).
Results
Population characteristics
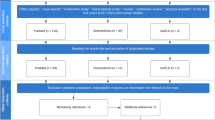
Among 71,451,419 weighted discharges during the study period, 1,938 had a discharge diagnosis of RCVS. Based on the inclusion criteria, 1065 discharges for RCVS were included for further analysis. The baseline characteristics of all patients are shown in Table 1. The mean (SD) age was 49.0 (16.7) years and 69.7% were female. Common comorbidities included hypertension (55.6%), hyperlipidemia (31.9%), migraine (25.1%), depression (23.7%), and diabetes (21.5%). Lumbar puncture (36.4%) and cerebral angiography (25.0%) were the most frequently performed inpatient procedures. Most patients had private insurance (43.6%) and a majority of the hospitalizations were at the large (73.9%), teaching hospitals (88.2%). The mean (SD) length of stay was 7.1 (10.3) days and approximately 26% of patients had discharge disposition other than home.
Predictors of ischemic stroke
Among the total 1065 patients, 267 (25.1%) had occurrence of ischemic stroke at presentation or during the initial hospitalization. Table 2 shows the comparison of baseline characteristics between patients with and without ischemic stroke. After multivariable adjustment, patients with ischemic stroke were more likely to have history of hypertension (OR 2.33, 95% CI 1.51–3.60), diabetes (OR 1.81, 95% CI 1.11–2.98), and tobacco use (OR 1.64, 95% CI 1.16–2.33) and less likely to have a history of migraine (OR 0.56, 95% CI 0.35–0.90).
Clinical outcomes
Table 3 shows different clinical outcomes in patients with ischemic stroke in reference to those without any ischemic stroke. Ischemic stroke was associated with higher odds of cerebral edema (OR 3.15, 95% CI 1.31–7.57) and respiratory failure requiring mechanical ventilation (OR 2.39, 95% CI 1.28–4.44). Patients with ischemic stroke also had longer hospital stay by a mean duration of 6.7 days, P < 0.001, higher hospital charges by a mean of $72,961, P < 0.001, and a higher likelihood of being discharged other than to home (OR 3.57, 95% CI 2.39–5.33). They had higher in-hospital mortality rate, the difference, however, was not statistically significant.
Discussion
This study describes the rate, risk factors, and clinical outcomes of ischemic stroke in one of the largest cohorts of hospitalized patients with RCVS to date. One in four patients in our study had the diagnosis of acute ischemic stroke. The incidence of ischemic stroke in RCVS has been reported to range from 4 to 6% in the studies recruiting patients with acute headaches (and angiographic abnormalities) from the headache clinics or emergency rooms [8, 9] to as high as 39% in a study from tertiary care referral centers based on the inpatient setting [3]. This variation in the rate of ischemic stroke is likely reflective of recruitment bias with a higher disease severity among the hospitalized patients.
Ischemic strokes in RCVS are typically seen in the anterior-middle and middle-posterior cerebral artery watershed territories [6]. Ischemic lesions could be caused by severe vasospasm of medium- and large-sized arteries or could result from cerebral edema in some patients [2]. The only study comparing patients with RCVS with and without ischemic stroke found that the angiographic severity score predicted the occurrence of ischemic infarcts [6]. Although we did not have access to the imaging data, ours is the first study to give a detailed description of the clinical characteristics associated with ischemic stroke in RCVS. We found that hypertension, diabetes, and tobacco use were independently associated with the occurrence of ischemic stroke. These are all major risk factors for intracranial atherosclerosis [10]. We speculate that intracranial atherosclerosis along with the right shift of the cerebral blood flow autoregulation curve in chronic hypertension [11], might be associated with a higher susceptibility to developing ischemic lesions from proximal vasoconstriction in patients with these risk factors. Interestingly, we found that history of migraine was associated with a lower risk of developing ischemic stroke. While the exact reason for this finding is unclear, but the changes in cerebrovascular reactivity and the putative epiphenomenon of vasodilation underlying migraine [12], might potentially be associated with a protective effect against the uncontrolled vasoconstriction associated with ischemic stroke in RCVS.
Stroke is the most severe manifestation of RCVS that can lead to permanent neurologic deficits and even death [9], and is hence the major determinant of the long-term prognosis in RCVS [2]. In this study, we found that patients with ischemic stroke were significantly more likely to develop cerebral edema and respiratory failure requiring mechanical ventilation. They had a longer hospital stay, higher total hospital charges, and were less likely to be discharged home. Patients with ischemic stroke also had a higher all-cause in-hospital mortality; however, the association was not statistically significant because of small number of patients who died.
RCVS is a relatively rare and a heterogenous disorder and most of the previous studies are limited to single-center or regional cohorts. So, one of the major strengths of our study includes the utilization of large, nationally representative database, increasing the generalizability of our findings. However, the results of this study should be interpreted in the context of potential limitations. First, we did not have data about the clinical presentation, triggers/precipitants, or radiographic studies, and with the inclusion of cases solely based on the use of ICD-10 codes, the possibility of misdiagnosis of RCVS cannot be completely ruled out. Specifically, intracranial atherosclerosis is a close radiological mimic of RCVS that can potentially confound the association between ischemic stroke and the risk factors analyzed in this study. However, we used a validated ICD-10 diagnostic code for RCVS that was recently shown to have 100% sensitivity and 90% specificity in an administrative claims database [13]. To further enhance the diagnostic specificity of RCVS and eliminate the potential confounding effect of intracranial atherosclerosis, we carried out sensitivity analysis and identified the predictors of ischemic stroke after excluding patients with a concomitant diagnosis of intracranial atherosclerosis either during the initial RCVS hospitalization or during any of the follow-up readmissions in the same calendar year. We found that 28 (2.6%) patients had a secondary diagnosis of intracranial atherosclerosis and we identified similar predictors of ischemic stroke even after excluding these patients. Second, in the general clinical practice, RCVS patients can be seen in the headache clinics, emergency room, or inpatient stroke units. However, the present study was based on the inpatient setting only, which might have led to an overestimation of the neurologic complications. Despite these limitations, this study provides relevant benchmark data on ischemic stroke in RCVS.
Conclusion
In conclusion, we found that ischemic strokes affect nearly 25% of patients with RCVS and is associated with increased rate of other neurologic complications and worse functional outcomes. Patients with traditional cerebrovascular risk factors might have a higher predisposition for developing ischemic lesions.
Data availability
The Nationwide Readmissions Database is a publicly available dataset that can be obtained after completion of the HCUP data use agreement.
References
Ducros A, Bousser MG (2009) Reversible cerebral vasoconstriction syndrome. Pract Neurol 9(5):256–267. https://doi.org/10.1136/jnnp.2009.187856
Ducros A (2012) Reversible cerebral vasoconstriction syndrome. Lancet Neurol 11(10):906–917. https://doi.org/10.1016/s1474-4422(12)70135-7
Singhal AB, Hajj-Ali RA, Topcuoglu MA, Fok J, Bena J, Yang D, Calabrese LH (2011) Reversible cerebral vasoconstriction syndromes: analysis of 139 cases. Arch Neurol 68(8):1005–1012. https://doi.org/10.1001/archneurol.2011.68
Katz BS, Fugate JE, Ameriso SF, Pujol-Lereis VA, Mandrekar J, Flemming KD, Kallmes DF, Rabinstein AA (2014) Clinical worsening in reversible cerebral vasoconstriction syndrome. JAMA Neurol 71(1):68–73. https://doi.org/10.1001/jamaneurol.2013.4639
Garg A, Rocha M, Starr M, Ortega-Gutierrez S (2021) Predictors and outcomes of hemorrhagic stroke in reversible cerebral vasoconstriction syndrome. J Neurol Sci 421:117312. https://doi.org/10.1016/j.jns.2021.117312
Topcuoglu MA, Singhal AB (2016) Hemorrhagic reversible cerebral vasoconstriction syndrome: features and mechanisms. Stroke 47(7):1742–1747. https://doi.org/10.1161/STROKEAHA.116.013136
Overview N (December 2019) Healthcare Cost and Utilization Project (HCUP).
Ducros A, Boukobza M, Porcher R, Sarov M, Valade D, Bousser MG (2007) The clinical and radiological spectrum of reversible cerebral vasoconstriction syndrome. A prospective series of 67 patients. Brain 130(12):3091–3101. https://doi.org/10.1093/brain/awm256
Ducros A, Fiedler U, Porcher R, Boukobza M, Stapf C, Bousser MG (2010) Hemorrhagic manifestations of reversible cerebral vasoconstriction syndrome: frequency, features, and risk factors. Stroke 41(11):2505–2511. https://doi.org/10.1161/STROKEAHA.109.572313
Banerjee C, Chimowitz MI (2017) Stroke caused by atherosclerosis of the major intracranial arteries. Circ Res 120(3):502–513
Ruland S, Aiyagari V (2007) Cerebral autoregulation and blood pressure lowering. Am Heart Assoc 10:13–34
Fabjan A, Zaletel M, Žvan B (2015) Is there a persistent dysfunction of neurovascular coupling in migraine? Biomed Res Int 2:574186. https://doi.org/10.1155/2015/574186
Magid-Bernstein J, Salehi Omran S, Murthy SB, Merkler AE, Kamel H (2020) Abstract WP228: reversible cerebral vasoconstriction syndrome: presenting symptoms, incidence, and outcomes in a multi-state cohort in the USA. Stroke 51(1):AWP228–AWP228
Funding
None.
Author information
Authors and Affiliations
Contributions
All authors were involved in the conception of the study design. Statistical analysis was performed by AG. The first draft of the manuscript was written by AG and SO-G. All authors were involved in the critical revision of the manuscript. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflicts of interest.
Ethics approval
The study was exempt from the Institutional Review Board as we used a publicly available database with deidentified information.
Rights and permissions
About this article

Cite this article
Garg, A., Starr, M., Rocha, M. et al. Predictors and outcomes of ischemic stroke in reversible cerebral vasoconstriction syndrome. J Neurol 268, 3020–3025 (2021). https://doi.org/10.1007/s00415-021-10456-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-021-10456-2