
Abstract
Background
Cognitive deficits are common in early multiple sclerosis (MS), however, spatial navigation changes and their associations with brain pathology remain poorly understood.
Objective
To characterize the profile of spatial navigation changes in two main navigational strategies, egocentric (self-centred) and allocentric (world-centred), and their associations with demyelinating and neurodegenerative changes in early MS.
Methods
Participants with early MS after the first clinical event (n = 51) and age-, gender- and education-matched controls (n = 42) underwent spatial navigation testing in a real-space human analogue of the Morris water maze task, comprehensive neuropsychological assessment, and MRI brain scan with voxel-based morphometry and volumetric analyses.
Results
The early MS group had lower performance in the egocentric (p = 0.010), allocentric (p = 0.004) and allocentric-delayed (p = 0.038) navigation tasks controlling for age, gender and education. Based on the applied criteria, lower spatial navigation performance was present in 26–29 and 33–41% of the participants with early MS in the egocentric and the allocentric task, respectively. Larger lesion load volume in cortical, subcortical and cerebellar regions (ß ≥ 0.29; p ≤ 0.032) unlike brain atrophy was associated with less accurate allocentric navigation performance.
Conclusion
Lower spatial navigation performance is present in up to 41% of the participants with early MS. Demyelinating lesions in early MS may disrupt neural network forming the basis of allocentric navigation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Multiple sclerosis (MS) is the most common chronic inflammatory, demyelinating and neurodegenerative disease of the central nervous system in young adults. Cognitive deficits are common in MS and can be detected in 12–57% of individuals after the first clinical event [1, 2]. Cognitive deficits reflect disease-related grey and white matter pathology in the brain [3] and have negative impact on quality of life including but not limited to reduced employment status and poor driving performance [4, 5]. The profile of cognitive impairment in early MS is characterized by predominant slowing of information processing speed and deficits in episodic memory [6]. However, it has not been investigated whether cognitive impairment involves deficits in spatial navigation, the cognitive function essential for our everyday functioning, especially for driving abilities [7].
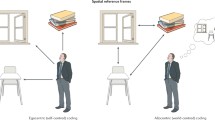
Spatial navigation is a complex and multi-modal cognitive process that involves maintaining a sense of direction and location during the movement and enables us to find our way around an environment. Two basic spatial navigation strategies have been identified, self-centred (egocentric) using the individual’s own position for navigation and world-centred (allocentric) using distal orientation cues for navigation [8]. When navigating our environment a large network of brain areas is activated including the medial temporal lobe region, thalamus and prefrontal cortex in allocentric navigation and posterior parietal lobe and caudate nucleus in egocentric navigation [9]. Disruption of these areas results in spatial navigation impairment in many neurological conditions including Alzheimer’s disease, stroke, epilepsy, Parkinson’s disease, Huntington’s disease and autoimmune encephalitis [10,11,12,13,14,15]. However, it remains unclear whether disruption of these areas by demyelinating and neurodegenerative changes is associated with spatial navigation deficits in individuals with MS.
We used a real-space navigation apparatus and brain MRI with global, regional cortical, subcortical and lesion load volume quantification to characterize a profile of spatial navigation changes in egocentric and allocentric navigational strategies and their associations with demyelinating and neurodegenerative changes in individuals with early MS after the first clinical event. Based on the previous studies showing structural changes in the medial temporal lobe region, thalamus and frontal cortex together with changes in the parietal lobe and caudate nucleus in early MS [16,17,18,19] we hypothesized that participants with early MS would have lower performance in both allocentric and egocentric navigation strategies that would be associated with lesion load and atrophy of brain areas related to spatial navigation.
Participants and methods
Participants
51 participants with early MS on interferon-beta treatment were recruited at the Multiple Sclerosis Centre, 2nd Faculty of Medicine, Charles University and Motol University Hospital, Prague, Czech Republic. The participants were 18–55 years old, after the first clinical event, had objective clinical evidence of one lesion, Expanded Disability Status Scale (EDSS) score less than 3.0, 2 or more hyperintensive T2 lesions on brain MRI and 2 or more oligoclonal bands in cerebrospinal fluid. Objective clinical evidence of one lesion was defined as focal neurological dysfunction demonstrated by clinical examination that was typical for acute demyelinating event. The first clinical symptoms included spinal cord (n = 18) and brainstem symptoms (n = 14), retrobulbar neuritis (n = 13) and hemispheric symptoms (n = 6). All participants met the 2017 revised McDonald criteria for relapsing–remitting MS [20]. 7 participants had mild depressive or anxiety symptoms stabilized on selective serotonin reuptake inhibitors. Neuropsychological examination, spatial navigation testing and time-matched experimental brain MRI (within 4 weeks) were performed between 1 and 15 months from the diagnosis of MS (median 4 months). In addition, 42 cognitively normal, age-, gender- and education-matched healthy control participants reporting normal navigation skills were recruited from the hospital staff and their relatives, and underwent the same protocol. Their cognitive performance was within the normal range, they did not score more than 1.5 SDs below the mean of age- and education-adjusted norms in any neuropsychological test. The participants with psychiatric and neurological disorders (except MS in the participants with early MS), cardiovascular diseases, and a history of alcohol or drug abuse were not included in the study. All participants signed an informed consent approved by the local ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Spatial navigation testing
For spatial navigation testing, we used the real-space human analogue of the Morris Water Maze task, a well-established method to evaluate spatial navigation abilities that has been used in many studies and allows separate testing of two important spatial navigation strategies, allocentric and egocentric [12, 15, 21]. This task was performed in a real-space navigational setting, a fully enclosed cylindrical arena 2.8 m in diameter surrounded by a 2.9 m high dark curtain with 8 large digital numerical displays used as distal orientation cues (Fig. 1a), that reliably mimics navigation in the real world [14, 22]. The participants located an invisible goal on the arena floor in 4 different tasks using a start position (egocentric) or 2 distal orientation cues on the wall (allocentric), respectively (Fig. 1b). To begin the task, participants were asked to enter the arena. They were given a long-standing pole with an infrared light-emitting diode on the top and were briefly shown the position of the goal on the arena floor. Before each trial, they were asked to stand at the side of the arena, go directly from their start position to the goal, and to place the pole directly on the presumed goal position. The goal was briefly shown after each trial to facilitate learning (although the goal was not shown any time during the delayed subtask). The allocentric-egocentric task was performed first. It involved locating the goal using its spatial relationship with both the start position and the 2 distal orientation cues on the arena wall. This was considered a training task designed to familiarize participants with the testing procedure. This task was followed by the egocentric task that involved using only the start position to locate the goal with no distal orientation cues displayed. The egocentric task was followed by the allocentric task that involved using only 2 distal orientation cues on the arena wall for navigation to the goal as the start position was unrelated to the goal position. Finally, the delayed task, which was identical to the allocentric task, was administered 30 min after the initial allocentric task was completed. The training (egocentric-allocentric), egocentric and allocentric tasks had 8 trials and the correct position of the goal was shown after each trial to provide the feedback. The delayed task had 2 trials and no feedback through showing the hidden goal was provided. The relative positions (distances and directions) of the goal were stable across all trials relative to (1) the positions of the start location and both orientation cues in the training (allocentric-egocentric) task, (2) positions of the start location in the egocentric task, and (3) positions of both orientation cues in the allocentric and delayed tasks. After each trial, the goal position along with the start position and the positions of 2 distal orientation cues were rotated in a pseudorandom sequence and the participants were instructed to go to the new start position. There was no time limit to find the goal, mainly to reduce bias by differences in sensory and physical functioning and psychomotor speed. All participants were able to complete the spatial navigation task. Spatial navigation performance was recorded automatically by in-house developed software as the distance error between a presumed goal position indicated by the participants and a correct goal position. The distance error in centimetres in each trial or averaged across the trials in each task was used as the main outcome measure.

Human analogue of the Morris Water Maze task. a The real-space navigation setting. b The scheme of the task showing an aerial view of the arena (large white circle) with starting point (red filled circle), orientation cues (red and green lines), and goal (purple circle)
Lower spatial navigation performance for each task was established when the participant with early MS had the average navigational score for a given task more than 1.5 SDs below the mean of the control group. We used the arbitrary criterion of > 1.5 SDs as an analogy with studies on individuals with mild cognitive impairment [23]. In addition, to provide a more conservative estimate of lower spatial navigation performance in participants with early MS, we also calculated values for a more stringent criterion of > 2.0 SDs below the mean of the control group. The score for general spatial navigation performance was expressed as a unit-weighted composite z-score from average navigational scores in the egocentric, allocentric and allocentric delayed tasks. Lower general spatial navigation performance was established using the criterion of > 1.5 SDs below the mean of the control group.
Neuropsychology
The participants underwent a comprehensive neuropsychological assessment covering seven major cognitive domains: (1) verbal memory measured with the Rey Auditory Verbal Learning Test-RAVLT (trials 1–5 and 30-min delayed recall trial), (2) nonverbal memory measured with the Brief Visuospatial Memory Test Revised-BVMT-R (trials 1–3 and 25-min delayed recall trial), (3) information processing speed/attention/working memory measured with the Symbol Digit Modalities Test-SDMT, Paced Auditory Serial Addition Test-PASAT, Digit Span Forward task-DF, Digit Span Backward task-DB and Trail Making Test A-TMT A, (4) executive function measured with the Trail Making Test B-TMT B and Controlled Oral Word Association Test-COWAT, (6) visuo-spatial function measured with the Judgment of Line Orientation Test-JLO and (7) language function measured with the Category Fluency Test-CFT (animals and shopping items) [24]. A self-administered 15-item Multiple Sclerosis Neuropsychological Screening Questionnaire (MSNQ) was used as a self-report screening measure of cognitive functioning. The National Adult Reading Test (NART) was used to estimate premorbid intelligence levels. The Beck Depression Inventory (BDΙ) and the Beck Anxiety Inventory (BAI) were used to measure depressive and anxiety symptoms.
Magnetic resonance imaging acquisition and analysis
Brain scans were performed at 1.5 T scanner (Siemens AG, Erlangen, Germany) using (1) T1-weighted 3-dimensional high resolution magnetization-prepared rapid acquisition with gradient echo (MP-RAGE) sequence with the following parameters: TR/TE = 12/4.605 ms, flip angle 15°, 150 continuous partitions and slice thickness 1.0 mm for volumetric measurement and (2) fluid-attenuated inversion recovery (FLAIR) sequence with the following parameters: TR/TE/TI = 11,000/140/2600 ms, flip angle 90°, 100 continuous partitions, and slice thickness 1.5 mm for lesion load measurement. The scans were visually inspected by a neuroradiologist to ensure appropriate data quality. The experimental protocol was available for all participants with early MS and 32 control participants. 10 control participants were not willing to undergo the MRI protocol.
Brain tissue volume normalized for participants’ head size was estimated with SIENAX, part of FSL (http://fsl.fmrib.ox.ac.uk/fsl/fslwiki/SIENA) [25, 26]. Normalized brain parenchymal (nBP) volume and separate estimates of normalized grey matter (nGM), white matter (nWM) and peripheral (cortical) grey matter (npGM) volumes were calculated. Volumes of subcortical grey matter structures were estimated with FIRST, part of FSL (http://fsl.fmrib.ox.ac.uk/fsl/fslwiki/FIRST) [27]. Subcortical structural volumes were normalized to total intracranial volume to control for variation in head size using a covariance approach [28].
Voxel-based morphometry (VBM) was used to assess differences in regional cortical grey matter. VBM was performed with masking of the registration cost function with lesion masks to reduce the impact of white matter lesions on brain segmentation and creation of grey matter template. Lesions masks were obtained by lesion segmentation tool (LST) toolbox version 2.0.15 (www.statistical-modelling.de/lst.html) for SPM (http://www.fil.ion.ucl.ac.uk/spm/). The algorithm segmented the T1 images into the three main tissue classes (cerebrospinal fluid, grey matter and white matter). This information was then combined with the coregistered FLAIR intensities to calculate lesion probability maps. A lesion filling algorithm implemented in LST toolbox was adopted [29]. The algorithm uses previously generated lesion masks registered to the image to fill the lesions with intensities matching the surrounding normal appearing white matter. An optimized VBM approach was adopted with all processing steps carried out using openware FSL version 5.0.7 (http://fsl.fmrib.ox.ac.uk/fsl/fslwiki/FSLVBM). Anatomical localization of significant clusters was established using the Harvard–Oxford Structural Atlas. Lesion load for each brain lobe and subcortical structure was obtained by coregistration of lesion masks to standard MNI brain using FLIRT and establishing anatomical localization of lesions using the MNI Structural Atlas [30].
Statistics
The Students’ independent two-sample t test evaluated mean between-group differences in demographic variables. The χ2 test evaluated differences in proportions (gender). The analysis of covariance (ANCOVA) evaluated mean between-group differences in cognitive variables, brain tissue volumes derived from SIENAX and subcortical grey matter volumes derived from FIRST. A general linear model (GLM) implemented in FSL was used to compare voxel-wise between-group differences in regional cortical grey matter volumes derived from VBM. Repeated measures (RM) ANCOVA with trials 1–8 as the within-subject factor (learning) evaluated between-group navigational differences in the egocentric and allocentric tasks. ANCOVA evaluated between-group navigational differences in the mean scores of the allocentric delayed task. Age, gender and years of education were controlled in the ANCOVA, RM ANCOVA and GLM analyses to provide more conservative estimates of the hypothesized differences. In addition, the RM ANCOVA and ANCOVA with RAVLT and BVMT-R delayed recall scores sequentially entered into the model as covariates were conducted to address the possibility that between-group navigational differences may be explained by memory deficits. Navigational data were log transformed prior to the analyses because of their right-skewed distribution. This was driven by non-normal distribution of data in the early MS group, while the data in the control group were normally distributed.
In participants with early MS, the relationships between demographic and navigational (mean scores in each task) variables, total and regional lesion load volumes, brain tissue volumes and regional subcortical and cortical grey matter volumes were assessed using Pearson’s correlation, point-biserial correlation (gender) and GLM correlation models implemented in FSL (VBM data). VBM results were corrected for family-wise error using a FSL’s tool for nonparametric permutation inference [31]. If a correlational analysis yielded a significant association, a linear regression model adjusted for age, gender, years of education and EDSS score was estimated. Holm–Bonferroni correction for multiple comparisons was used in the statistical analysis. Statistical significance was set at 2-tailed alpha of 0.05. Effect sizes were reported using Cohen’s d for the Student’s t tests, Cramér’s V for the χ2 test and partial eta-squared (η 2p ) for ANCOVA. Partial eta-squared of 0.06 correspond to Cohen’s d of about 0.5. All analyses were conducted with IBM SPSS 25.0 software.
Results
The results are presented in Table 1, Figs. 2 and 3 and Supplementary Tables 1 and 2. The groups did not differ in demographic characteristics, premorbid intelligence level and subjective cognitive functioning. The early MS group reported more depressive and anxiety symptoms, had lower performance in most cognitive tests and lower volumes in most MRI measures. The correlations between variables are presented in Tables 2 and 3, Supplementary Table 3 and Supplementary Figure 1.

Voxels with significant (p < 0.05) grey matter volume reduction in the early MS group compared to controls in rendered brains projected to show: a left side, b right side, c front, d back, e top and f bottom

Voxels with significant (p < 0.05) grey matter volume reduction in controls compared to the early MS group in rendered brains projected to show: a left side, b right side, c front, d back, e top and f bottom.
Spatial navigation
The early MS group had less accurate spatial navigation performance in the egocentric (F[1,88] = 6.85, p = 0.010, η 2p = 0.07), allocentric (F[1,88] = 8.96, p = 0.004, η 2p = 0.09) and allocentric delayed (F[1,88] = 4.45, p = 0.038, η 2p = 0.05) tasks. The results remained significant after Holm–Bonferroni correction for multiple comparisons. The learning effect in the egocentric (F[7,616] = 1.57, p = 0.142, η 2p = 0.02) and allocentric (F[7,616] = 0.53, p = 0.810, η 2p = 0.01) tasks was not significant. There were no significant group-by-trial interactions in the egocentric (F[7,616] = 1.04, p = 0.403, η 2p = 0.01) and allocentric (F[7,616] = 0.33, p = 0.942, η 2p = 0.01) tasks, suggesting no differences in navigational learning between the groups. Controlling for the RAVLT delayed recall score, less accurate spatial navigation performance remained significant in the egocentric (F[1,87] = 4.30, p = 0.041, η 2p = 0.05) and allocentric (F[1,87] = 8.66, p = 0.004, η 2p = 0.09) tasks in the early MS group. The latter also remained significant after controlling for the BVMT-R delayed recall score (F[1,87] = 4.21, p = 0.043, η 2p = 0.05). Exclusion of the participants with mild depressive or anxiety symptoms from the analysis did not affect the results.
The proportion of participants with lower spatial navigation performance was estimated among the early MS group. Using the criterion of 1.5 SDs, lower performance was present in 29.4% of participants in the egocentric task, 41.2% of participants in the allocentric task and 21.6% of participants in the allocentric delayed task. Using a more stringent criterion of 2 SDs, lower performance was present in 25.5% of participants with early MS in the egocentric task, 33.3% of participants in the allocentric task and 13.7% of participants in the allocentric delayed task.
Spatial navigation and MRI measures
In the early MS group, less accurate spatial navigation performance in the allocentric tasks, especially in the allocentric delayed task, correlated with higher lesion load including total lesion volume and lesion volume in the frontal lobe, insula, left temporal lobe, parietal lobe, right occipital lobe, right periventricular region, left cerebellum and left putamen (r ≥ 0.29, p ≤ 0.038). The correlations with lesion load in the right frontal lobe, insula, right occipital lobe, left cerebellum and left putamen remained significant after the correction for multiple comparisons. The results are presented in Tables 2 and 3. The associations between navigational performance in the allocentric tasks, especially in the allocentric delayed task, and higher lesion load including total lesion volume and lesion volume in the frontal lobe, insula, left temporal lobe, parietal lobe, right occipital lobe, left cerebellum and left putamen (ß ≥ 0.29; p ≤ 0.032) remained unchanged in the covariate-adjusted regression models.
Characteristics of normal and less accurate navigators with early MS
We directly compared early MS participants with normal (n = 37) and less accurate (n = 14) spatial navigation, which was defined as lower general spatial navigation performance averaged across three navigational tasks using the criterion of 1.5 SDs. The groups did not differ in demographic characteristics, EDSS score, premorbid intelligence level, subjective cognitive functioning, depressive and anxiety symptoms and most cognitive tests except for SDMT and TMT B, where the early MS group with less accurate spatial navigation had lower performance (F[1,46] = 4.83, p = 0.034, η 2p = 0.11 and F[1,46] = 6.45, p = 0.015, η 2p = 0.14, respectively), which did not remain significant after the correction for multiple comparisons. The early MS group with less accurate spatial navigation had lower nWM volume (F[1,46] = 4.29, p = 0.044, η 2p = 0.09) and higher lesion volume in the left and right frontal cortex (F[1,46] = 5.82, p = 0.020, η 2p = 0.11 and F[1,46] = 8.43, p = 0.006, η 2p = 0.16, respectively) and the right parietal cortex (F[1,46] = 4.06, p = 0.049, η 2p = 0.08). The results did not remain significant after the correction for multiple comparisons. The results are presented in Table 4.
Discussion
There is increasing evidence that cognitive deficits emerge early in MS and can be detected in individuals after the first clinical event [16, 32, 33]. Cognitive deficits typical for early MS are characterized by predominant slowing of information processing speed and impairment of episodic memory, however, changes in spatial navigation, the cognitive function essential for our everyday functioning, remain poorly understood [5, 6]. This is the first study to characterize a profile of spatial navigation changes in two main navigational strategies, egocentric (self-centred) and allocentric (world-centred), and their associations with demyelinating and neurodegenerative changes in individuals with early MS after the first clinical event. Our results showed that the participants with early MS had on average lower spatial navigation performance in the egocentric, allocentric and allocentric delayed tasks above and beyond demographic characteristics compared to the control group indicating a disease-related weakening of the general spatial navigation abilities. Lower average navigational performance remained significant in the egocentric and allocentric tasks after controlling for verbal memory, the latter also after controlling for nonverbal (visuospatial) memory indicating that lower average navigational performance, especially allocentric, cannot be explained by general memory deficits in individuals with early MS. Navigational performance did not correlate with EDSS score indicating that greater clinical disability is not associated with less accurate spatial navigation in individuals with early MS. The participants with early MS did not demonstrate spatial navigation learning effects analogous to their worse learning in the memory tests (as indicated by the lower RAVLT 1–5 and BVMTR 1–3 scores). It should be noted that the control participants also did not improve their spatial navigation performance across the trials. This unusual finding could be explained by their superior performance, when they located the hidden place very accurately, leading to the ceiling effect in our spatial navigation task. Next, we explored the proportion of individuals with early MS who had lower spatial navigation performance. For this purpose, we defined lower spatial navigation performance using the previously established criterion of > 1.5 SDs and the more stringent criterion of > 2.0 SDs, respectively, below the mean of the control group for a given task. Based on the applied criteria, 22–41 and 14–33% of the participants with early MS had lower spatial navigation performance, especially in allocentric navigational strategy [16, 23]. The results were similar to previous findings of cognitive deficits observed in 14–49% of individuals after the first clinical event and supported the hypothesis that spatial navigation along with other cognitive functions is affected very early in the course of the disease [16, 34]. Further, we investigated the characteristics of the individuals with early MS with less accurate spatial navigation defined by the criterion of 1.5 SDs below the mean of the control group. The less accurate navigators were similar in demographic characteristics, disease severity (measured by EDSS), premorbid intelligence level, subjective cognitive functioning, and depressive and anxiety symptoms indicating that less accurate spatial navigation performance may not be associated with these characteristics. The less accurate navigators were also similar in most cognitive tests, except for lower performance in the test of information processing speed and the test of executive function, which did not withstand correction for multiple comparisons, suggesting that spatial navigation may be distinguishable from other cognitive functions, which, however, does not contradict occurrence of more complex cognitive dysfunction in individuals after the first clinical event [1, 34].
Finally, we explored the link between neurodegeneration and spatial navigation in early MS by comparing differences in global and regional brain tissue loss between normal and less accurate navigators and evaluating the relationships between cortical and subcortical brain volumes and each navigational strategy. The associations between structural changes of navigation-related brain regions and spatial navigation performance were not significant in our study. It is therefore possible that less accurate spatial navigation in early MS may be caused by regional microstructural alterations, disruption of pathways between these regions and altered dynamics of neural networks rather than by extensive brain tissue loss [35, 36]. The assumption of the association between neural network and pathway disruption and navigational performance is in line with our data showing that the less accurate navigators had more extensive demyelinating changes in the frontal and right parietal cortex, the regions that are strongly involved in allocentric and egocentric navigation [9], respectively, and smaller volume of the nWM, which was previously shown to be associated with visuospatial dysfunction [16]. However, these results should be interpreted with caution as they did not withstand the correction for multiple comparisons. This also corresponds with our findings of the relationships between less accurate allocentric navigation and higher lesion load in the frontal lobe and also in the temporal lobe (uncorrected result), the regions important for allocentric navigation [9], in the participants with early MS. Less accurate allocentric navigation was also associated with higher lesion load in the right occipital and insular cortex, left putamen, left cerebellum and also in the parietal cortex (uncorrected result), the regions involved in spatial navigation [37]. However, location and extent of demyelinating lesions did not explain all navigational changes as they were not associated with less accurate egocentric navigation. Previous studies reported similar observations that specific locations of demyelinating lesions could explain cognitive functioning to a limited extent, where the weakest associations were found in the early stages of MS, in those with a low disease burden [38, 39]. Future studies adopting high-resolution, quantitative and functional MRI and diffusion tensor imaging techniques are required to reveal comprehensively all neural substrates of spatial navigation changes in early MS [40].
One of the strengths of the present study is the fact that this is the first study to date to assess spatial navigation in MS. We used a well-established method, the real-space human analogue of the Morris Water Maze task, that allows characterizing spatial navigation changes in two main navigational strategies, egocentric and allocentric. In addition, we explored how changes in each navigational strategy are associated with structural brain changes including volume of the cortical and subcortical brain structures and global and regional lesion load. Finally, we used clinically and cognitively well-defined homogeneous cohorts of participants with early MS after the first clinical event and demographically matched healthy controls. This study also has limitations. This was a cross-sectional study, which does not allow tracking spatial navigation changes over time but longitudinal follow-up is ongoing. Also the results may be influenced by interferon-beta treatment that may affect cognitive functions [41]. Next, the group of participants with early MS and lower spatial navigation performance was relatively small and this may influence our results. Some results including the associations between spatial navigation performance and structural brain changes did not surpass the correction for multiple comparisons and therefore should be interpreted with caution. Finally, experimental brain MRI was available only in a subset of the healthy control participants and may not detect subtle structural grey and white matter alterations that could be related to less accurate spatial navigation performance in the participants with early MS.
In conclusion, using the real-space human analogue of the Morris Water Maze task, we demonstrated that the individuals with early MS after the first clinical event had on average lower spatial navigation performance in the egocentric and allocentric navigational strategies compared to the demographically matched healthy controls above and beyond age, gender, education and verbal memory deficits, the latter strategy also above and beyond nonverbal (visuospatial) memory deficits. Based on the applied criteria, lower spatial navigation performance was present in 22–41 and 14–33% of the participants with early MS. Larger cortical, subcortical and cerebellar lesion load volumes were associated with less accurate allocentric navigation performance indicating a disruption of neural network forming the basis of allocentric navigation. Our findings show that spatial navigation deficits can be detected in some individuals with early MS and assessment of navigational strategies along with other cognitive functions may be beneficial when characterizing cognitive performance in early MS. Future studies comparing different spatial navigation tasks in real-space and virtual reality should identify the most appropriate task for spatial navigation assessment in individuals with early MS.
Change history
30 December 2020
The original article can be found online.
References
Brochet B, Ruet A (2019) Cognitive impairment in multiple sclerosis with regards to disease duration and clinical phenotypes. Front Neurol 10:261
Potagas C, Giogkaraki E, Koutsis G, Mandellos D, Tsirempolou E, Sfagos C, Vassilopoulos D (2008) Cognitive impairment in different MS subtypes and clinically isolated syndromes. J Neurol Sci 267:100–106
Daams M, Steenwijk MD, Schoonheim MM, Wattjes MP, Balk LJ, Tewarie PK, Killestein J, Uitdehaag BM, Geurts JJ, Barkhof F (2016) Multi-parametric structural magnetic resonance imaging in relation to cognitive dysfunction in long-standing multiple sclerosis. Mult Scler 22:608–619
Schultheis MT, Weisser V, Ang J, Elovic E, Nead R, Sestito N, Fleksher C, Millis SR (2010) Examining the relationship between cognition and driving performance in multiple sclerosis. Arch Phys Med Rehabil 91:465–473
Honarmand K, Akbar N, Kou N, Feinstein A (2011) Predicting employment status in multiple sclerosis patients: the utility of the MS functional composite. J Neurol 258:244–249
Reuter F, ZaaraouiW Crespy L, Faivre A, Rico A, Malikova I, Confort-Gouny S, Cozzone PJ, Ranjeva JP, Pelletier J, Audoin B (2011) Cognitive impairment at the onset of multiple sclerosis: relationship to lesion location. Mult Scler 17:755–758
Ruano L, Portaccio E, Goretti B, Niccolai C, Severo M, Patti F, Cilia S, Gallo P, Grossi P, Ghezzi A, Roscio M, Mattioli F, Stampatori C, Trojano M, Viterbo RG, Amato MP (2017) Age and disability drive cognitive impairment in multiple sclerosis across disease subtypes. Mult Scler 23:1258–1267
Lester AW, Moffat SD, Wiener JM, Barnes CA, Wolbers T (2017) The aging navigational system. Neuron 95:1019–1035
Maguire EA, Burgess N, Donnett JG, Frackowiak RS, Frith CD, O’Keefe J (1998) Knowing where and getting there: a human navigation network. Science 280:921–924
Bastiaansen AEM, van Sonderen A, Titulaer MJ (2017) Autoimmune encephalitis with anti-leucine-rich glioma-inactivated 1 or anti-contactin-associated protein-like 2 antibodies (formerly called voltage-gated potassium channel-complex antibodies). Curr Opin Neurol 30:302–309
Schneider CB, Linse K, Schönfeld R, Brown S, Brown S, Koch R, Reichmann H, Leplow B, Storch A (2017) Spatial learning deficits in Parkinson’s disease with and without mild cognitive impairment. Parkinsonism Relat Disord 36:83–88
Majerová V, Kalinčík T, Laczó J, Vyhnálek M, Hort J, Bojar M, Růžička E, Roth J (2012) Disturbance of real space navigation in moderately advanced but not in early Huntington’s disease. J Neurol Sci 312:86–91
Claessen MHG, Visser-Meily JMA, Meilinger T, Postma A, de Rooij NK, van der Ham IJM (2017) A systematic investigation of navigation impairment in chronic stroke patients: evidence for three distinct types. Neuropsychologia 103:154–161
Hort J, Laczó J, Vyhnálek M, Bojar M, Bures J, Vlcek K (2007) Spatial navigation deficit in amnestic mild cognitive impairment. Proc Natl Acad Sci 104:4042–4047
Amlerova J, Laczo J, Vlcek K, Javurkova A, Andel R, Marusic P (2013) Risk factors for spatial memory impairment in patients with temporal lobe epilepsy. Epilepsy Behav 26:57–60
Hyncicova E, Vyhnalek M, Kalina A, Martinkovič L, Nikolai T, Lisý J, Hort J, Meluzínová E, Laczó J (2017) Cognitive impairment and structural brain changes in patients with clinically isolated syndrome at high risk for multiple sclerosis. J Neurol 264:482–493
Henry RG, Shieh M, Okuda DT, Evangelista A, Gorno-Tempini ML, Pelletier D (2008) Regional grey matter atrophy in clinically isolated syndromes at presentation. J Neurol Neurosurg Psychiatry 79:1236–1244
Hyncicova E, Kalina A, Vyhnalek M, Nikolai T, Martinkovic L, Lisy J, Hort J, Meluzinova E, Laczó J (2018) Health-related quality of life, neuropsychiatric symptoms and structural brain changes in clinically isolated syndrome. PLoS One 13:e0200254
Audoin B, Zaaraoui W, Reuter F, Rico A, Malikova I, Confort-Gouny S, Cozzone P, Pelletier J, Ranjeva J (2010) Atrophy mainly affects the limbic system and the deep grey matter at the first stage of multiple sclerosis. J Neurol Neurosurg Psychiatry 81:690–695
Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, Correale J, Fazekas F, Filippi M, Freedman MS, Fujihara K, Galetta SL, Hartung HP, Kappos L, Lublin FD, Marrie RA, Miller AE, Miller DH, Montalban X, Mowry EM, Sorensen PS, Tintoré M, Traboulsee AL, Trojano M, Uitdehaag BMJ, Vukusic S, Waubant E, Weinshenker BG, Reingold SC, Cohen JA (2018) Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol 17:162–173
Laczó J, Andel R, Nedelska Z, Vyhnalek M, Vlcek K, Crutch S, Harrison J, Hort J (2017) Exploring the contribution of spatial navigation to cognitive functioning in older adults. Neurobiol Aging 51:67–70
Laczó J, Vlcek K, Vyhnálek M, Vajnerová O, Ort M, Holmerová I, Tolar M, Andel R, Bojar M, Hort J (2009) Spatial navigation testing discriminates two types of amnestic mild cognitive impairment. Behav Brain Res 202:252–259
Petersen RC (2004) Mild cognitive impairment as a diagnostic entity. J Intern Med 256:183–194
Nikolai T, Stepankova H, Kopecek M, Sulc Z, Vyhnalek M, Bezdicek O (2018) The uniform data set, Czech version: normative data in older adults from an international perspective. J Alzheimers Dis 61:1233–1240
Smith SM, Zhang Y, Jenkinson M, Chen J, Matthews PM, Federico A, De Stefano N (2002) Accurate, robust and automated longitudinal and cross-sectional brain change analysis. NeuroImage 17:479–489
Smith SM, Jenkinson M, Woolrich MW, Beckmann CF, Behrens TE, Johansen-Berg H, Bannister PR, De Luca M, Drobnjak I, Flitney DE, Niazy RK, Saunders J, Vickers J, Zhang Y, De Stefano N, Brady JM, Matthews PM (2004) Advances in functional and structural MR image analysis and implementation as FSL. NeuroImage 23:208–219
Patenaude B, Smith SM, Kennedy DN, Jenkinson M (2011) A Bayesian model of shape and appearance for subcortical brain segmentation. Neuroimage 56:907–922
Jack CR, Petersen RC, O’Brien PC, Tangalos EG (1992) MR-based hippocampal volumetry in the diagnosis of Alzheimer’s disease. Neurology 42:183–188
Battaglini M, Jenkinson M, De Stefano N (2012) Evaluating and reducing the impact of white matter lesions on brain volume measurements. Hum Brain Mapp 33:2062–2071
Jenkinson M, Bannister P, Brady M, Smith S (2002) Improved optimization for the robust and accurate linear registration and motion correction of brain images. NeuroImage 17:825–841
Winkler AM, Ridgway GR, Webster MA, Smith SM, Nichols TE (2014) Permutation inference for the general linear model. NeuroImage 92:381–397
Feuillet L, Reuter F, Audoin B, Malikova I, Barrau K, Cherif AA, Pelletier J (2007) Early cognitive impairment in patients with clinically isolated syndrome suggestive of multiple sclerosis. Mult Scler 13:124–127
Deloire MS, Ruet A, Hamel D, Bonnet M, Dousset V, Brochet B (2011) MRI predictors of cognitive outcome in early multiple sclerosis. Neurology 76:1161–1167
Glanz BI, Holland CM, Gauthier SA, Amunwa EL, Liptak Z, Houtchens MK, Sperling RA, Khoury SJ, Guttmann CR, Weiner HL (2007) Cognitive dysfunction in patients with clinically isolated syndromes or newly diagnosed multiple sclerosis. Mult Scler 13:1004–1010
Planche V, Ruet A, Coupé P, Lamargue-Hamel D, Deloire M, Pereira B, Manjon JV, Munsch F, Moscufo N, Meier DS, Guttmann CR, Dousset V, Brochet B, Tourdias T (2017) Hippocampal microstructural damage correlates with memory impairment in clinically isolated syndrome suggestive of multiple sclerosis. Mult Scler 23:1214–1224
Lommers E, Simon J, Reuter G, Delrue G, Dive D, Degueldre C, Balteau E, Phillips C, Maquet P (2019) Multiparameter MRI quantification of microstructural tissue alterations in multiple sclerosis. Neuroimage Clin 23:1018–1079
Murias K, Slone E, Tariq S, Iaria G (2019) Development of spatial orientation skills: an fMRI study. Brain Imaging Behav 13:1590–1601
Mollison D, Sellar R, Bastin M, Mollison D, Chandran S, Wardlaw J, Connick P (2017) The clinico-radiological paradox of cognitive function and MRI burden of white matter lesions in people with multiple sclerosis: a systematic review and meta-analysis. PLoS One 12:15
Uher T, Krasensky J, Sobisek L, Blahova Dusankova J, Seidl Z, Kubala Havrdova E, Sormani MP, Horakova D, Kalincik T, Vaneckova M (2017) Cognitive clinico-radiological paradox in early stages of multiple sclerosis. Ann Clin Transl Neurol 5:81–91
Di Filippo M, Portaccio E, Mancini A, Calabresi P (2018) Multiple sclerosis and cognition: synaptic failure and network dysfunction. Nat Rev Neurosci 19:599–609
Penner IK, Stemper B, Calabrese P, Freedman MS, Polman CH, Edan G, Hartung HP, Miller DH, Montalban X, Barkhof F, Pleimes D, Lanius V, Pohl C, Kappos L, Sandbrink R (2012) Effects of interferon beta-1b on cognitive performance in patients with a first event suggestive of multiple sclerosis. Mult Scler 18:1466–1471
Acknowledgements
The authors would like to thank Ms. Přibylová and Ms. Jozsóvá for help with data collection and Dr. Lisý for supervising MRI acquisition. This study was supported by the Grant Agency of the Charles University, Prague (no. 546317); Ministry of Health, Czech Republic–conceptual development of research organization, University Hospital Motol, Prague, Czech Republic (no. 00064203); and Institutional Support of Excellence 2. LF UK (no. 699332).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical standards
All data and materials as well as software application support published claims and comply with field standards.
Additional information
The original online version of this article was revised: The given names and family names were interchanged.
The original version of this article was revised: Modifications have been made to the author’s name, Affiliation, Figures 1,2 and 3 caption, Tables 1 and 4 and also in Acknowledgement. Full information regarding the corrections made can be found in the correction for this article.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

{kind=link}
Cite this article
Němá, E., Kalina, A., Nikolai, T. et al. Spatial navigation in early multiple sclerosis: a neglected cognitive marker of the disease?. J Neurol 268, 77–89 (2021). https://doi.org/10.1007/s00415-020-10079-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-020-10079-z