
Abstract
Non-vestibular sensorimotor signals modulate the vestibular nucleus neuron to achieve current behavioral goals, and may generate or modulate nystagmus. In central lesions affecting the vestibular nuclei, non-vestibular signals such as mastication or swallowing may induce nystagmus. However, the influence of non-vestibular signals on these types of nystagmus has not been investigated in a systematic way and the underlying mechanisms of the modulation are poorly understood. In this study, several non-vestibular sensorimotor stimuli were applied to evaluate the patterns of nystagmus modulation in a patient with suspected rhombencephalitis or imaging negative small infarction, probably involving the left dorsolateral medulla. The nystagmus was induced or significantly modulated by (1) visual inputs, and (2) combined proprioceptive and efference copy signals (during voluntary motion) unrelated to body or head orientation. In contrast, isolated proprioceptive signal, mental set, or non-proprioceptive somatosensory inputs showed a negligible effect on the induction of nystagmus. Based on these modulations, we suggest that (1) the visually mediated nystagmus is due to a lesion-induced pursuit asymmetry, and (2) the nystagmus induced during voluntary motion is due to erroneous contribution of combined proprioceptive and efference copy signals during integration of non-vestibular signals for ocular motor control. Various non-vestibular sensorimotor stimulations may induce nystagmus due to dysfunction of the central vestibular neural circuity.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The central vestibular system is essential for constructing and maintaining spatial orientation, which is fundamental for motor behaviors such as reflexive eye movements, balance, and locomotion [1]. In addition to primary vestibular inputs, the vestibular nucleus receives non-vestibular sensorimotor inputs such as visual, proprioceptive, and efference copy signals from other brain structures [2]. The functional significance of this convergence of sensorimotor information in the vestibular nucleus is related to the needs for different responses according to the current behavioral goal [e.g., the expected responses are different between the visual cancelation and enhancement tasks of the vestibulo-ocular reflex (VOR)] [2]. Previous experimental studies with animals and humans have shown that sensorimotor information can modulate the neuronal responses in the vestibular nucleus or the nystagmus intensity [3–6]. Thus, the vestibular nucleus is assumed to be an essential structure for these sensorimotor interactions [2].
Visual inputs suppress the nystagmus from peripheral vestibular dysfunction (fixation suppression) [7, 8]. Patients with peripheral vestibular dysfunction can effectively adapt using non-vestibular signals such as vision and proprioception [9, 10]. In contrast, lesions involving the brainstem and vestibulocerebellum may impair this sensorimotor interaction, and visual inputs may fail to suppress the nystagmus [8, 11, 12]. Furthermore, proprioceptive signals can induce vertigo and nystagmus, which have been considered as a form of central vertigo [5, 13, 14]. These findings indicate that dysfunction of the central vestibular system can induce vertigo and nystagmus that originate from non-vestibular sensorimotor signals. However, the modulation patterns and underlying mechanisms of this central nystagmus require further exploration.
In this study, we systematically evaluated induction and modulation of nystagmus by visual, proprioceptive, and efference copy signals in a patient with vertigo and nystagmus that mostly developed during active motion. The purpose of this study was to elucidate the mechanisms of central nystagmus by determining the effects of non-vestibular sensorimotor inputs.
Materials and methods
Case report
A 76-year-old man presented with progressive vertigo and imbalance for 9 days. Examination showed left Horner’s syndrome (ptosis and miosis), mild dysarthria, bilateral limb ataxia, and leftward falling during the Romberg test. Motor and sensory function was intact in facial and extremities. There was no spontaneous or gaze-evoked nystagmus. Smooth pursuit was impaired to the right, but horizontal saccades and bedside head impulse tests were normal. After admission, he noted that the vertigo increased during head motion, limb movements, and even talking. A follow-up examination 2 days later showed spontaneous nystagmus beating rightward, upward, and clockwise during visual fixation. Notably, the nystagmus increased during convergence, talking, hand clapping, and foot tapping (video 1 and 2). Again, gaze-evoked nystagmus was absent, and smooth pursuit was impaired to the right. Without visual fixation in darkness, the spontaneous nystagmus decreased mildly, but then increased with hand clapping. Horizontal head impulse tests were normal, and horizontal head-shaking and positional maneuvers did not change the nystagmus. He also showed hoarseness due to left vocal cord palsy and dysphagia. His symptoms and the nystagmus persisted for five more days, and then slowly improved over the following week.
An analysis of cerebrospinal fluid showed elevated protein at 79 mg/dL. Autoimmune serology was negative for anti-nuclear, anti-neutrophil cytoplasmic, anti-Ro and -La, anti-jo-1, anti-ganglioside, and paraneoplastic antibodies (anti-Hu, -Yo, and -Ri). Cranial MRIs with diffusion-weighted imaging and whole body positron-emission tomography findings were also unremarkable. He was assumed to have rhombencephalitis of unknown origin or MR negative small infarction, mostly involving the left dorsolateral medulla.
Study protocols
All study protocols were approved by the Institutional Review Board of Seoul National University Bundang Hospital (B-1109/135-106), and written informed consent was obtained from the patient. The patient had a recording of spontaneous nystagmus with and without visual fixation, gaze-evoked nystagmus, head-shaking nystagmus, vibration-induced nystagmus, positional nystagmus, smooth pursuits and saccades using three-dimensional video-oculography (SensoMotoric Instruments, Teltow, Germany). The protocol for routine video-oculography has been described elsewhere [15–17].
We aimed to determine the influence of non-vestibular sensorimotor inputs such as vision, somatosensation, and efference copy signals on the patient’s spontaneous nystagmus. We also evaluated the effect of the mental set on the nystagmus. Therefore, the following paradigms were presented to the patient (Fig. 1). In paradigm I, we evaluated the influence of visual inputs using two different methods. At first, the patient rested in complete darkness for 60 s, and then, a visual target was presented one meter ahead. In the second condition, the patient was asked to stare at the white textured curtain one meter ahead, which covered the whole visual fields. Afterwards, a visual target was presented on the curtain with the same visual depth as in the first method. The only difference between the two conditions was a textured background that was reported to decrease pursuit gain up to 20 % [18]. Therefore, we were able to evaluate the effect of pursuit eye movement on the nystagmus by comparing the intensity of nystagmus induced during each condition. Paradigm II was adopted to evaluate the influences of the mental set. The patient was asked to perform a simple arithmetic operation with or without verbal responses. Before the experiments, he was fully instructed to calculate a simple arithmetic operation even without verbal responses. Paradigm III was used to determine the influence of somatosensory inputs. The somatosensory inputs were elicited by light touch on both forearms to stimulate the lateral spinothalamic pathway and by repetition of passive joint motion of the right elbow to stimulate the posterior column-medial lemniscus pathway. Finally, during paradigm IV, the patient was asked to clap his hands. Since the self-generated action contains both proprioceptive and efference copy signals, we could define the differential effects of efference copy signals by comparing the results with those of the paradigm III. The paradigms II through IV were performed both with and without a visual cue.

Study protocol
Analyses of nystagmus
The acquired eye position data were analyzed using the MATLAB software (version R2011b, MathWorks, Natick, MA). The baseline eye position data were obtained when the eyes were most stable. The intensity of nystagmus during each stimulus paradigm was determined using the slow phase velocities (SPVs) of nystagmus starting from 10 to 15 s after the onset of stimulus. By averaging the SPVs of 20 consecutive nystagmus, we obtained the mean SPVs of nystagmus during each paradigm. Data were presented as the mean ± standard deviation, and the differences in SPVs were evaluated using the Mann–Whitney’s U test. Statistical analyses were performed using SPSS v.18.0 (IBM Corp., Armonk, NY, USA).
Other laboratory vestibular evaluations
The patient also had bithermal caloric tests, cervical vestibular-evoked myogenic potentials, and tilt of the subjective visual vertical. All tests were performed within 1 day after the evaluation of nystagmus. The method and normative data of each test have been reported [19].
Results
Baseline oculographic findings
In the primary position, the spontaneous nystagmus beat rightward, upward, and clockwise. The vertical and torsional nystagmus decreased during rightward gaze (30°). During leftward gaze (30°), the horizontal and vertical nystagmus was attenuated and the torsional nystagmus reversed into beating counterclockwise. Horizontal saccades were normal in both directions with normal latency, accuracy, and velocity. Rightward smooth pursuit was impaired with a gain of 0.13 (normal = 0.69 ± 0.11) in response to a sinusoidally moving target with a peak velocity at 10°/s while leftward smooth pursuit was intact (gain = 0.73) (Fig. 2a).

Pursuit eye motion and modulation of nystagmus during study paradigm I. a Rightward pursuit eye motion was impaired in response to a sinusoidally moving target at a peak velocity of 10°/s. Upward deflection indicates rightward eye motion. Age-matched normal gain is 0.69 ± 0.11. b Influence of visual inputs on spontaneous nystagmus beating rightward, upward, and counterclockwise (paradigm I); Upper In darkness, only slowly roving eye motion is observed, but visual fixation induces nystagmus; Lower During staring at a textured curtain covering the whole visual fields, presentation of a visual target augments the spontaneous nystagmus. The nystagmus is attenuated immediately after elimination of the visual target (inserted figure)
Modulation of spontaneous nystagmus
The mean SPVs of nystagmus are presented in Table 1. During the evaluation in complete darkness, we could assess only the horizontal and vertical components due to noises in the torsional recording. Therefore, the compound SPVs of nystagmus were calculated only during the recordings with visual inputs.
Effects of visual inputs (paradigm I)
In darkness, only slowly roving eye movements were observed without apparent jerky nystagmus. Presentation of a visual target evoked jerky nystagmus (Fig. 2b). The horizontal and vertical mean SPVs of the nystagmus were 4.9 ± 1.0 and 2.8 ± 1.4°/s, respectively. After the visual input was eliminated, the induced nystagmus slowly dissipated over about 15 s. While staring at a textured background in the light, the spontaneous nystagmus beat rightward, upward, and clockwise, and the mean SPVs of each component were 2.5 ± 0.7, 1.6 ± 0.7, and 2.1 ± 0.8°/s, respectively. The mean compound SPVs of nystagmus was 3.8 ± 0.6°/s. The intensities of horizontal and vertical components were lower than those during visual fixation in darkness. Then, presentation of a target significantly increased the nystagmus (p < 0.001) (Fig. 2b). The augmented responses disappeared immediately with elimination of the target. During visual fixation in darkness and on the textured background, the mean SPVs of horizontal nystagmus were similar while the vertical nystagmus was about 1.3-fold stronger during visual fixation on the textured background.
Effect of mental set (paradigm II)
In darkness, there was no evoked nystagmus during the mental tasking without verbal responses. However, when the patient was asked to answer verbally, prominent nystagmus was generated. With visual fixation in darkness, the nystagmus was similar between resting and mental tasking without verbal responses (p > 0.05). When the patient answered the questions with a verbal response, the intensity of nystagmus increased significantly (p < 0.001).
Effects of somatosensory cues (paradigm III)
In darkness without a visual target, repeated light touches on the forearm did not evoke nystagmus. In contrast, the passive joint motion began to generate nystagmus 7 s after the stimulation was initiated. The induced nystagmus slowly dissipated over about 50 s despite continued stimulation (Fig. 3a). During visual fixation in darkness, the intensities of the induced nystagmus were similar between the resting and light touch conditions (p > 0.05). However, passive joint motions significantly increased the nystagmus (p < 0.001) (Fig. 3a).

Modulation of nystagmus during study paradigm III and IV. a The nystagmus during passive joint motion (paradigm II); Upper In darkness, the evoked nystagmus starts approximately 7 s after initiating the passive joint motion. The nystagmus slowly decays even with continued passive joint motion; Lower During visual fixation, the spontaneous nystagmus increases with the passive joint motion. b The nystagmus during voluntary action (hand clapping, paradigm III); Upper In darkness, the voluntary action immediately generates the nystagmus. The evoked nystagmus decays over 40 s after ceasing the action. Lower During visual fixation, the nystagmus is augmented with the voluntary action
Effects of voluntary motions (paradigm IV)
In darkness without a visual target, self-generated hand clap induced strong nystagmus, and the induced nystagmus dissipated over about 30 s after the clapping was discontinued (Fig. 3b). During fixation of a target in darkness, the hand clapping markedly augmented the nystagmus (p < 0.001) (Fig. 3b).
Other laboratory vestibular evaluation
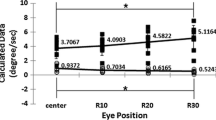
The measured subjective visual verticals during left monocular, right monocular, and binocular viewing were −17.4°, −12.7°, and −8.5°, respectively (normal range = −3.0° to 2.2°; A negative value indicates leftward tilt). Bithermal caloric tests showed no paresis, but showed a directional preponderance of 51 % to the right. Sound-induced cervical vestibular-evoked myogenic potentials showed a mildly decreased amplitude during left ear stimulation with an interaural differences at 23 % (normal <21.5 %).
Discussion
In this study, we evaluated the modulation of nystagmus by non-vestibular sensorimotor signals in a patient with a suspected lesion mostly involving the dorsolateral medulla, probably due to rhombencephalitis or infarction. The main findings of this study were (1) visual inputs and combined proprioceptive and efference copy signals may induce nystagmus; (2) isolated proprioceptive signals are insufficient to generate nystagmus, given the long latency of nystagmus after stimulus initiation (7 s) and dissipation of the nystagmus even during continued stimulation; and (3) mental set and non-proprioceptive somatosensory input do not induce nystagmus.
Because our patient had neurological symptoms and signs indicating dysfunction of the dorsolateral medulla, the findings of this study suggest that dysfunction of the tegmental brainstem structures, especially the vestibular nucleus, produces nystagmus that may be attributed to non-vestibular sensorimotor signals. Though the effect of each sensorimotor signal on nystagmus has been evaluated in different studies, this is the first systematic study that investigated the effects of all possible sensorimotor interactions on the nystagmus.
In the paradigm I, the visual cues generated or augmented the nystagmus. In darkness without a visual target, our patient showed only slowly roving eye movements (dysrhythmia) that may have interrupted apparent nystagmus. It has been suggested that dysrhythmia is a phenomenon to dampen an unwanted VOR [20]. Given that dysfunction of the dorsolateral medulla usually produces a vestibular imbalance, the dysrhythmia in our patient may be a compensatory phenomenon of the central vestibular system. It is of interest, however, that the visual input eliminated the dysrhythmia and generated nystagmus. Prior studies showed that central lesions, especially those involving the cerebellum, eliminate the ability to suppress vestibular nystagmus using visual fixation [8, 11, 12]. In contrast, fixation induced or augmented nystagmus in patients with lesions that involve certain areas of the cerebellum [21, 22], medial longitudinal fasciculus, or paramedian pontine reticular formation [23]. In those studies, the nystagmus augmentation during visual fixation was explained in two ways: One is the enhanced alertness by the visual inputs, and the other is the visually mediated eye position change that enhanced the nystagmus [23]. However, both assumptions cannot be applied to our patient since there was no augmentation of nystagmus during mental tasking without verbal responses. In addition, there was no gaze limitation. In our patient, the visually induced nystagmus attenuated rapidly upon removing the target from the textured background. It should be noted that our patient had prominent rightward pursuit impairment. Visual fixation on the textured background was more effective in generating nystagmus than visual fixation in darkness, which is also suggestive of pursuit asymmetry as a mechanism of nystagmus in our patient [18]. Therefore, we propose that visually mediated nystagmus in our patient may be a form of pursuit paretic nystagmus attributed to dysfunction of the eye–head neurons in the left vestibular nucleus.
The paradigm II evaluated the effects of alertness (mental set) on the nystagmus. Mental arithmetic without verbal responses did not change the intensity of nystagmus, both with or without a visual cue. On the other hand, the same alerting task with verbal responses provoked or augmented the nystagmus in our patient. Therefore, the effects of the mental set on the nystagmus appeared to be minimal, if any, in our patient. According to previous studies, mental alerting tasks intensified the nystagmus during caloric stimulation [24, 25]. Similar effects were noted in patients with peripheral vestibular dysfunction [26]. However, it is not obvious whether the mental tasking was the sole component of stimuli since most of the alerting tasks in those studies included verbal responses. In fact, the mental tasking with verbal responses provides mixed stimuli of both alertness, and combined proprioception and efference copy signals of the tongue and buccofacial structures. Moreover, it was suggested that the active alerting task with verbal responses was more effective than the passive alerting task without verbal responses in augmenting the caloric nystagmus [27]. Therefore, the findings in our patient do not necessarily contradict the previous findings. Based on our observation, mental tasks do not appear to influence the nystagmus from brainstem dysfunction when the patient already maintains an arousal.
In the paradigms III and IV, we evaluated the effects of somatosensory and efference copy signals on the nystagmus. As expected, non-proprioceptive somatosensory inputs did not affect the nystagmus. However, proprioceptive and efference copy signals generated the nystagmus. Interpretation of these results, however, requires caution since the experiment of passive limb movements involved more than the proprioceptive system. Rather, it may have been influenced by the patient’s voluntary actions to some extents. Given the long latency (7 s after initiation of stimulation) and resolution of the nystagmus even during continued stimulation, it appears that isolated proprioceptive cues could not generate the nystagmus in our patient. When the patient voluntarily generated arm movements that contained both the proprioceptive and efference copy signals, however, the nystagmus was generated immediately and decayed gradually over about 40 s, even after cessation of the stimulus. These findings suggest an engagement of the velocity-storage circuit in generating the nystagmus [28]. Taken together, we can conclude that the nystagmus in our patient was generated when both proprioceptive and efference copy signals were simultaneously provided. This assumption is in agreement with a prior experimental study that showed a minimal effect of isolated proprioceptive cues on the response characteristics of the vestibular nucleus neurons [29, 30]. The findings of paradigms III and IV are in contrast to those of prior studies, which showed that proprioceptive inputs augmented or generated nystagmus during the low-frequency VOR [5, 6, 31]. However, the experiments in those studies involved some degree of efference copy signals (grasping the bar or stretching the arm).
Unfortunately, it was not possible to sort out the roles of proprioceptive and efference copy signals in generating the nystagmus in our patient. An experimental study showed that proprioception unmatched to efference copy signals minimally influences the vestibular nucleus neurons [30]. However, the vestibular nucleus neurons enhance their responses to the proprioception in various pathological conditions such as unilateral labyrinthectomy [32]. Thus, there may be a flexible neural circuit that conveys the proprioception and efference copy signals to the vestibular nucleus neuron. A prior study also showed that volitional limb movements modulated per- and post-rotational vestibular responses or self-motion perception [33]. This indicates that the proprioceptive/efference copy signals from/to the limbs are normally integrated into the central vestibular system. These findings are well appreciated given that the limbs usually aid in maintaining the balance. Therefore, the proprioceptive/efference copy signals related to maintaining spatial orientation (e.g., arthrokinetic information from the knee and hip during locomotion, or from the arm during rotation) are normally engaged in the central vestibular system. However, the proprioceptive/efference copy signals involved in verbal responses, finger counting, and clapping, which were adopted in our patient, are not necessary for maintaining spatial orientation. Thus, we suggest that the dorsolateral medullary dysfunction may have changed the property of neural circuits and allowed these unnecessary non-vestibular sensorimotor signals to enter the central vestibular system (Fig. 4). This mechanism might explain other forms of central nystagmus, such as mastication- or swallowing-induced nystagmus, mostly documented in patients with dorsolateral medullary lesions [13, 14].

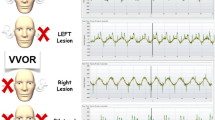
Schematic diagrams for a hypothetical mechanism of central nystagmus caused by combined proprioceptive and efference copy signals. The upper diagram (a) is based on a previous suggestion to explain how proprioceptive/efference copy signals influence the vestibular nucleus neurons in normal conditions [30]. Only the proprioceptive/efference copy signals related to spatial orientation are transferred to the vestibular nucleus. In the low diagram (b), a dorsolateral medullary lesion allows an entry of unnecessary information into the vestibular nucleus
In conclusion, the present study showed that visual inputs or voluntary movements may induce nystagmus in dorsolateral medullary dysfunction. The visually mediated nystagmus can be attributed to lesion-induced pursuit asymmetry. The nystagmus induced by voluntary movements may be due to an erroneous contribution of combined proprioceptive and efference copy signals to the central vestibular system. Dysfunction of the vestibular nucleus and adjacent structures may be essential for induction or modulation of the nystagmus by non-vestibular sensorimotor signals.
References
MacNeilage PR, Ganesan N, Angelaki DE (2008) Computational approaches to spatial orientation: from transfer functions to dynamic Bayesian inference. J Neurophysiol 100(6):2981–2996. doi:10.1152/jn.90677.2008
Angelaki DE, Cullen KE (2008) Vestibular system: the many facets of a multimodal sense. Annu Rev Neurosci 31:125–150. doi:10.1146/annurev.neuro.31.060407.125555
Cullen KE, McCrea RA (1993) Firing behavior of brain stem neurons during voluntary cancellation of the horizontal vestibuloocular reflex, I. Secondary vestibular neurons. J Neurophysiol 70(2):828–843
Gauthier GM, Vercher JL (1990) Visual vestibular interaction: vestibulo-ocular reflex suppression with head-fixed target fixation. Exp Brain Res 81(1):150–160
Brandt T, Buchele W, Arnold F (1977) Arthrokinetic nystagmus and ego-motion sensation. Exp Brain Res 30(2–3):331–338
Sugita-Kitajima A, Koizuka I (2009) Somatosensory input influences the vestibulo-ocular reflex. Neurosci Lett 463(3):207–209. doi:10.1016/j.neulet.2009.07.090
Huh YE, Kim JS (2013) Bedside evaluation of dizzy patients. J Clin Neurol 9(4):203–213. doi:10.3988/jcn.2013.9.4.203
Hood JD, Korres S (1979) Vestibular suppression in peripheral and central vestibular disorders. Brain 102(4):785–804
Dieterich M, Bauermann T, Best C, Stoeter P, Schlindwein P (2007) Evidence for cortical visual substitution of chronic bilateral vestibular failure (an fMRI study). Brain 130(Pt 8):2108–2116. doi:10.1093/brain/awm130
Cutfield NJ, Scott G, Waldman AD, Sharp DJ, Bronstein AM (2014) Visual and proprioceptive interaction in patients with bilateral vestibular loss. Neuroimage Clin 4:274–282. doi:10.1016/j.nicl.2013.12.013
Alpert JN (1974) Failure of fixation suppression: a pathologic effect of vision on caloric nystagmus. Neurology 24(9):891–896
Takemori S, Cohen B (1974) Loss of visual suppression of vestibular nystagmus after flocculus lesions. Brain Res 72(2):213–224
Lee SU, Park JH, Kim HJ, Deriu F, Kim JS (2014) Swallowing-induced vertigo and downbeat nystagmus. J Neurol 261(12):2457–2459. doi:10.1007/s00415-014-7539-9
Park SH, Kim HJ, Kim JS, Koo JW, Oh SW, Kim DU, Kim JT, Welgampola M, Deriu F (2014) Mastication-induced vertigo and nystagmus. J Neurol 261(3):480–489. doi:10.1007/s00415-013-7221-7
Yang Y, Kim JS, Kim S, Kim YK, Kwak YT, Han IW (2009) Cerebellar hypoperfusion during transient global Amnesia: an MRI and oculographic study. J Clin Neurol 5(2):74–80. doi:10.3988/jcn.2009.5.2.74
Huh YE, Kim JS (2011) Patterns of spontaneous and head-shaking nystagmus in cerebellar infarction: imaging correlations. Brain 134(Pt 12):3662–3671. doi:10.1093/brain/awr269
Choi JY, Kim JH, Kim HJ, Glasauer S, Kim JS (2015) Central paroxysmal positional nystagmus: characteristics and possible mechanisms. Neurology 84(22):2238–2246. doi:10.1212/WNL.0000000000001640
Collewijn H, Tamminga EP (1984) Human smooth and saccadic eye movements during voluntary pursuit of different target motions on different backgrounds. J Physiol 351:217–250
Choi KD, Oh SY, Kim HJ, Koo JW, Cho BM, Kim JS (2007) Recovery of vestibular imbalances after vestibular neuritis. Laryngoscope 117(7):1307–1312. doi:10.1097/MLG.0b013e31805c08ac
Proctor LR, Lam AP (2002) Dysrhythmia of caloric nystagmus. Laryngoscope 112(10):1730–1736. doi:10.1097/00005537-200210000-00004
Holmes G (1917) The symptoms of acute cerebellar injuries due to gunshot injuries. Brain 40:461–535. doi:10.1093/brain/40.4.461
Aschoff JC, Conrad B, Kornhube HH (1974) Acquired pendular nystagmus with oscillopsia in multiple-sclerosis—sign of cerebellar nuclei disease. J Neurol Neurosurg Psychiatry 37(5):570–577. doi:10.1136/jnnp.37.5.570
Takemori S, Aiba T, Shizawa R (1981) Visual suppression of caloric nystagmus in brain-stem lesions. Ann N Y Acad Sci 374:846–854
Barber HO, Wright G (1967) Release of nystagmus suppression in clinical electronystagmography. Laryngoscope 77(6):1016–1027. doi:10.1288/00005537-196706000-00008
Kileny P, McCabe BF, Ryu JH (1980) Effects of attention-requiring tasks on vestibular nystagmus. Ann Otol Rhinol Laryngol 89(1 Pt 1):9–12
McGovern TN, Fitzgerald JE (2008) The effect of mental alerting on peripheral vestibular nystagmus during spontaneous, gaze (30 degrees left, 30 degrees right) and body positional (left and right lateral lying) testing using electronystagmography (ENG). Int J Audiol 47(10):601–606. doi:10.1080/14992020802123579
Davis RI, Mann RC (1987) The effects of alerting tasks on caloric induced vestibular nystagmus. Ear Hear 8(1):58–60
Leigh RJ, Zee DS (2006) The neurology of eye movements, 4th edn. Oxford University Press, New York
Roy JE, Cullen KE (2001) Passive activation of neck proprioceptive inputs does not influence the discharge patterns of vestibular nuclei neurons. Ann N Y Acad Sci 942:486–489
Roy JE, Cullen KE (2004) Dissociating self-generated from passively applied head motion: neural mechanisms in the vestibular nuclei. J Neurosci 24(9):2102–2111. doi:10.1523/JNEUROSCI.3988-03.2004
Bles W, Jelmorini M, Bekkering H, de Graaf B (1995) Arthrokinetic information affects linear self-motion perception. J Vestib Res 5(2):109–116
Sadeghi SG, Minor LB, Cullen KE (2011) Multimodal integration after unilateral labyrinthine lesion: single vestibular nuclei neuron responses and implications for postural compensation. J Neurophysiol 105(2):661–673. doi:10.1152/jn.00788.2010
Guedry FE, Benson AJ (1983) Modification of per- and postrotational responses by voluntary motor activity of the limbs. Exp Brain Res 52(2):190–198
Author contributions
Jeong-Yoon Choi acquired the data, analyzed the data, and drafted the manuscript; Ji-Soo Kim analyzed the data and made critical revisions of the manuscript.
Disclosure
Dr. J-S Kim serves as an Associate Editor of Frontiers in Neuro-otology and on the editorial boards of the Journal of Clinical Neurology, Frontiers in Neuro-ophthalmology, Journal of Neuro-ophthalmology, and Journal of Vestibular Research. The other author has nothing to disclose.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
No conflicting relationship exists for the authors.
Electronic supplementary material
Below is the link to the electronic supplementary material.
415_2016_8032_MOESM1_ESM.avi
Video 1 Effect of passive motion on spontaneous nystagmus in darkness. There was only slow roving eye motion in darkness. The repetitive passive elbow motion generates jerky nystagmus 7 s after the initiation of stimulation. The nystagmus slowly dissipated despite continued stimulation. (AVI 6042 kb)
415_2016_8032_MOESM2_ESM.avi
Video 2 Effect of voluntary motions on spontaneous nystagmus in darkness. The slow roving eye motion was interrupted by jerk nystagmus associated with hand clapping. Of interest, the jerk nystagmus persisted after finishing the clapping. (AVI 4639 kb)
Rights and permissions
About this article

Cite this article
Choi, JY., Kim, JS. Modulation of central nystagmus by vision, proprioception, and efference copy signals: a systematic evaluation. J Neurol 263, 735–742 (2016). https://doi.org/10.1007/s00415-016-8032-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-016-8032-4