
Abstract
Previous studies using diffusion tensor imaging (DTI) have examined for differences between bulbar- and limb-onset amyotrophic lateral sclerosis (ALS). Findings between studies have been markedly inconsistent, though possibly as a consequence of poor matching for confounding variables. To address this problem, this study contrasted the DTI profiles of limb-onset (ALS-L) and bulbar-onset (ALS-B) in groups that were tightly matched for the potential confounding effects of power, age, cognitive impairment and motor dysfunction. 14 ALS-L and 14 ALS-B patients were selected from a large prospective study so as to be matched on clinical and demographic features. All subjects, including 29 controls, underwent neuropsychological and neurological assessment. Tract-based spatial statistics and region of interest techniques were used to analyse fractional anisotropy (FA), mean diffusivity (MD), radial diffusivity (RD) and axial diffusivity (λ 1). Extensive bilateral FA and RD changes along the corticospinal tract were found in ALS-B compared to controls, p (corrected) <0.05; a similar distribution was seen for ALS-L at a less stringent statistical threshold. ROI analyses also showed more significant changes in ALS-B than ALS-L when each was compared to controls; for FA, MD and RD the changes reached statistical significance in the direct contrast between the two patient groups. With careful matching for confounding factors, the results suggest that ALS-B is associated with greater central white matter degeneration than ALS-L, possibly contributing to the known worse prognosis of ALS-B. The study, however, found no evidence that the spatial distribution of white matter degeneration differs between these groups.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Amyotrophic lateral sclerosis (ALS) can be sub-divided according to the site of onset into limb (ALS-L) or bulbar (ALS-B). ALS-B has a worse prognosis than ALS-L [1, 2]. One possible explanation for this is that when the same disease affects muscles that are more critical for survival, patients succumb more rapidly; another might be that ALS-B represents a biologically more aggressive end of the spectrum. Previous studies have taken advantage of MRI and diffusion tensor imaging (DTI) to probe tissue microstructure and compare degeneration patterns in cerebral white matter between ALS-L and ALS-B cohorts [3–6]. The results of these previous studies are, however, potentially confounded by poor matching of groups for: sample size and, therefore, statistical power [3, 4]; motor disease severity [5]; sex-distribution [3, 4]; and lack of cognitive assessment [3–5]. Some studies were limited to regions-of-interest, and hence unable to describe the full distribution of affected areas [5] while others have attempted whole-brain analyses using the voxel-based morphometry (VBM) technique [3, 4, 6]. The VBM method was never designed for such purposes, however, and lacks the capacity to precisely match individual white matter tracts between subjects to enable like-for-like contrasts [7].
It is not surprising, therefore, that there is considerable inconsistency of results across studies as will be discussed more in detail later. The aim of the present study was to test whether the severity and/or distribution of DTI abnormalities differs between ALS-L and ALS-B using groups that were strictly matched for these confounding factors and using the tract-based spatial statistics [8] approach that was specifically designed to contrast white matter tracts.
Methods
Participants
Patients were recruited through the specialist ALS clinics in Hannover and Magdeburg (Germany) as part of a prospective study that has recruited N = 120 cases to date. Clinical diagnosis of ALS was made according to the revised El Escorial criteria [9]. For the present study only ALS with combined upper and lower motor neuron features were included; primary lateral sclerosis and pure lower motor variants including flail limb were excluded. Concomitant frontotemporal dementia was also an exclusion criterion; this was defined on clinical grounds (including caregiver report) in accordance with proposed diagnostic criteria [10]. Furthermore, there were no cases with primary progressive aphasia in the N = 120 data set. Of the patients meeting these criteria, fourteen ALS-B patients were identified then, from a far larger pool of ALS-L patients (N = 38), 14 cases were selected so as to be matched for statistical power and further matched for sex distribution, age, ALSFRS-R score [11] and cognition using the Montreal Cognitive Assessment [12] (MoCA). ALSFRS-R was assessed by the same experienced, ALS sub-specialised neurologist (SV) in all cases. For imaging comparisons, 29 healthy control subjects were recruited and screened to exclude neurological illness and cognitive performance (Table 1).
Subjects gave their written informed consent prior to their inclusion in the study. The study was approved by the local ethics committee of Otto-von-Guericke University.
Imaging
MRI scans were performed on a Siemens Verio 3T system (Siemens Medical Systems, Erlangen, Germany) equipped with a gradient coil capable of 45 mT/m and 200 T/m/s slew rate. A standard 32-channel phased array imaging head coil (Siemens Medical Systems, Erlangen, Germany) was used in receive mode. A thin pillow was placed on the base of the coil surrounding the sides and the back of the head to minimise motion and increase inter-subject reproducibility in positioning. The field of view was aligned at acquisition in all cases to the anterior commissure–posterior commissure (ac–pc) line.
Diffusion datasets were acquired using a twice refocused, single-shot, echo-planar imaging pulse sequence using the following parameters: repetition time = 12,700 ms, echo time = 81 ms; matrix = 128 × 128; 72 contiguous axial slices; isotropic voxel resolution of 2 × 2 × 2 mm3; receiver bandwidth of 1,628 Hz/pixel and echo spacing of 0.72 ms. The tensor was computed using 30 non-collinear diffusion directions (b = 1,000 s/mm2) and one scan without diffusion weighting (b = 0 s/mm2) and two averages. We allowed for parallel acquisition of independently-reconstructed images using generalised, autocalibrating, partially-parallel acquisitions or GRAPPA [13], with acceleration factor of 3 and 57 reference lines. The total acquisition time was 14′11″.
A T2-weighted FLASH sequence acquired during the same session (24 slices, slice thickness = 5 mm, distance factor = 20 %, 256 × 256 matrix size, 0.9 × 0.9 mm2) was used to exclude vascular pathology.
Data processing and analysis
The Oxford Centre for Functional MRI of the Brain (FMRIB) software library (FSLv4.1.2) [14] was used to correct for motion and eddy currents, fit the diffusion tensor and compute the parametric maps. Initially, each diffusion-weighted volume was affine-aligned to its corresponding b0 image using the FMRIB’s linear image registration tool (FLIRTv5.4.2) [15] to correct for motion artefacts and eddy-current distortions. In addition, to exclude extra-cerebral voxels, brain masks of each b0 image were generated using the brain-extraction tool (BET v2.1) [16] with fractional threshold, f = 0.1, and vertical gradient, g = 0. FMRIB’s diffusion toolbox (FDT v2.0) was then used to fit the tensor and compute the diagonal elements (λ 1, λ 2 and λ 3) at each brain voxel, from which the derived metrics radial diffusivity (RD), mean diffusivity (MD) and fractional anisotropy (FA) were also inferred.
The tract-based spatial statistics (TBSS) approach [8] was used to perform whole-brain, cluster-based, statistical analyses at white matter tract centres. Spatial normalisation was achieved by warping all FA images to the 1 × 1 × 1 mm3 FMRIB58_FA standard template (FMRIB, University of Oxford, UK) in MNI152 space (Montreal Neurological Institute, McGill University, Canada) using the FMRIB’s non-linear image registration tool (FNIRT v1.0). Following the TBSS data processing pipeline, all patients and controls warped FA maps were averaged to create the mean FA template, from which the mean FA skeleton was derived (FA >0.2). Finally, all spatially normalised FA, axial diffusivity (λ 1), RD and MD data were projected onto the skeleton and fed into voxel-wise statistics, where 10,000 permutations of the data were generated using randomize v2.1 with threshold free cluster enhancement [17] (TFCE) enabled. The TFCE output was corrected for multiple comparisons by controlling the family wise error rate (FWE), using a threshold p < 0.05.
Regional corticospinal analysis
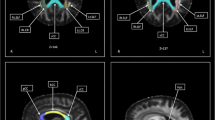
A region of interest (ROI) comprising the left and right corticospinal tracts (CST) was manually delineated in standard space, using the FMRIB58_FA template (Fig. 1a) to specifically compare the severity between ALS-L and ALS-B. Mean values for FA, λ 1, RD and MD resulting from the intersection of the ROI with the mean skeleton mask (N = 43, FA >0.2) were extracted as depicted in Fig. 1a. Regional data were tested for normality using the Lilliefors [18] test, implemented in Matlab v2012a (The Mathworks Inc., Natick, MA, USA). The results of the test at α = 0.05 indicated that for the ALS-B cohort, RD was not normally distributed. Hence for consistency non-parametric Mann–Whitney U tests were used to compare all DTI-derived values from independent sample groups (controls, ALS-B and ALS-L) [19]. The single CST ROI was used because there was no prior hypothesis related to lateralisation of effects, and to limit the number of statistical contrasts.

Corticospinal tract ROI delineation and analysis. a Corticospinal tract ROI (orange) overlaid onto the mean FA skeleton (green) and mean FA map in standard space (background image). b Skeletonised corticospinal ROI analysis. Bars denote means; whiskers are the 95 % confidence interval; and dots the individual data points; *p ≤ 0.05, **p < 0.01 and ***p < 0.001. The y axes were adjusted dynamically for each plot such that the center of the axis represents the control mean and the top and bottom of the axis was defined as the center ±7 control standard deviations
Results
TBSS analysis of ALS-B cohort
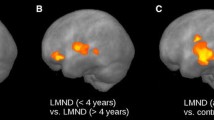
At p < 0.05 corrected for multiple comparisons, bilateral and confluent changes along the CST were found for FA. RD showed less extensive statistical differences mainly restricted to the CST at the thalamic level. No differences were detected for MD or λ 1 at this statistical threshold (Fig. 2a).

TBSS result for the ALS-B (a) and ALS-L (b) groups compared to controls. a Thresholded (FWE error corrected TFCE, p < 0.05) statistical maps for reduced FA (blue) and increased RD (red) overlaid onto the mean FA skeleton (green) and the mean FA map in standard space. b Thresholded (uncorrected TFCE, p < 0.05) statistical maps for reduced FA (blue) and increased RD (red) overlaid onto the mean FA skeleton (green) and the mean FA map in standard space. On both panels, coronal depths, in MNI space, are given in mm
TBSS analysis of ALS-L cohort
The group comparisons between ALS-L and controls (corrected p < 0.05) showed no significant differences in any diffusivity or anisotropy metric. Reducing the significance threshold to uncorrected p < 0.05 found patchy FA and RD changes in CST (Fig. 2b). No differences were detected for MD or λ 1 at this reduced statistical threshold.
Regions of interest: corticospinal tracts (Fig. 1b)
Significant FA reductions (relative to controls) were found for both ALS groups in the skeletonised CST ROI, although the significance in the control versus ALS-B contrast was considerably more robust (compared to controls, a 3.3 % FA reduction in ALS-L and a 5.8 % reduction in ALS-B). The same pattern was evident for increases in RD in the patients groups (compared to controls, a 4.9 % RD increase in ALS-L and a 7.8 % increase in ALS-B). A statistically significant MD increase for ALS-B compared to controls and a significant decrease in λ 1 for ALS-L compared to controls emerged from the ROI analyses.
Direct contrast of the two patient groups found a statistically significant difference (more abnormal) for FA, RD and MD in ALS-B compared to ALS-L.
Discussion
Using groups that were strictly matched for power, sex-distribution, ALSFRS-R and cognition, the study found that ALS-B is associated with more statistically significant abnormalities than ALS-L. No evidence, however, was identified to suggest that the distribution of abnormalities differs between the two modes of disease onset—in both groups, changes were concentrated on the corticospinal pathways.
Several previous studies have taken advantage of DTI to analyse WM degeneration in ALS [6, 20–25]. These studies indicated that FA values are reduced in ALS particularly in WM structures such as corpus callosum and CST in agreement with past histological findings [26]. The present study went beyond FA, which is a function derived from λ 1 and RD, to exploit the full extent of diffusion information (FA, MD, λ 1, RD) to ascertain the most sensitive DTI metric for ALS. As previously shown in Alzheimer’s disease [27], the present results found that the FA reduction in ALS is predominantly driven by increases in RD. Unlike Alzheimer’s disease [27], however, the FA reduction was also influenced by a decrease in λ 1. This “double hit” suggests that FA is the best metric to study in ALS. These findings offer further evidence that different neurodegenerative diseases can behave differently with respect to the quality of tensor changes [27, 28]. For instance, in contrast to the present findings, increased λ 1 in Alzheimer’s disease makes FA an insensitive metric [27, 29, 30].
Regarding the group contrasts, the results indicated greater CST degeneration in ALS-B compared to ALS-L. Given the matching of the two groups, this suggests that ALS-B might represent a biologically more aggressive form of the disease. The symptom duration also supports this interpretation in that, although there was no significant between-group difference in this measure, the ALS-L group had longer average symptom duration than ALS-B. There are, however, caveats. For instance, at least in theory, if one needed a greater level of neurodegeneration to become symptomatic in the bulbar system compared to the limbs, it is conceivable that ALS-B could have more degeneration for apparently shorter symptom duration. Furthermore, although the groups were matched for disease severity on the ALSFRS-R, this is a composite score and it is theoretically possible that endorsements in bulbar versus limb questions have different sensitivity to the degree of underlying degeneration. A further, and perhaps more plausible caveat, is that ALS-B represents a predominantly central degenerative process whereas disability in ALS-L is more influenced by relatively greater lower motor neuron involvement. Whether such caveats warrant serious consideration or are only theoretical is unclear; definitive proof that central degeneration in ALS-B moves at a faster pace will require longitudinal data. What can be claimed with confidence from the current result is that if ALS-B and ALS-L are matched with ALSFRS-R score, one can expect the ALS-B group to have more central WM degeneration.
Turning to the question of whether ALS-L and ALS-B are associated with differing topographical distributions of degeneration is where previous studies are most inconsistent, and where either confounding factors, or incomplete information about such factors, could explain inconsistent results. For instance, some studies did not consider cognitive impairment [3, 4] yet its presence or absence could have a profound impact on whether extra-motor abnormalities were found; similarly others [5] did not account for symptom duration which could also influence whether degeneration had spread beyond the motor system. These problems are best exemplified by two previous studies that reported diametrically opposed results. The first, a DTI study, reported prefrontal involvement in ALS-L but not ALS-B [4]. The study did not, however, include cognitive evaluation making it possible that the ALS-L effect was driven by patients with more cognitive impairment. Moreover, the study was not matched for group size (almost twice as many ALS-L cases), suggesting that differential power could have caused greater statistical sensitivity in the ALS-L group. The study also used VBM which, as already mentioned, is not ideal because even subtle degrees of misregistration could cause spurious findings by WM matter tracts not being precisely aligned.
In contrast, an FDG-PET study reported the opposite pattern—more extensive prefrontal hypometabolism in ALS-B compared to ALS-L [31]. In this study, neuropsychology was included and it revealed the ALS-B group to have significantly greater cognitive impairment suggesting in turn that this, rather than ALS-B per se, was the explanation. Taken together with the present results which found no differences in distribution with matched groups, it would appear that extra-motor differences in neurodegeneration distribution reported in past studies have been driven by these confounding factors rather than having any specific relationship to whether the disease starts in limbs or bulbar regions.
To conclude, heterogeneity in ALS is an enormous challenge to imaging research. A range of different clinical phenotypes; the variable contribution of upper and lower motor neuron degeneration to clinical disability; the presence or absence of cognitive involvement; as well as the usual factors such as matching for severity and demographic variables can all conspire to make study interpretation close to impossible. The magnitude of this challenge is highlighted in the present study where 120 ALS cases were required to identify matched groups of 14 with ALS-L and ALS-B. Nevertheless, this approach, in which patients were selected from a very large initial pool to improve matching on as many variables as possible, offers a way forward to improve interpretability and stability across studies. This methodological approach allowed us to establish an unbiased comparison between degenerative changes in ALS-L and ALS-B with respect to controls ultimately suggesting that ALS-B is associating with greater central white matter degeneration than ALS-L.
References
Roche JC, Rojas-Garcia R, Scott KM, Scotton W, Ellis CE, Burman R, Wijesekera L, Turner MR, Leigh PN, Shaw CE, Al-Chalabi A (2012) A proposed staging system for amyotrophic lateral sclerosis. Brain 135(Pt 3):847–852
Ganesalingam J, Stahl D, Wijesekera L, Galtrey C, Shaw CE, Leigh PN, Al-Chalabi A (2009) Latent cluster analysis of ALS phenotypes identifies prognostically differing groups. PLoS ONE 4(9):e7107
van der Graaff MM, Sage CA, Caan MW, Akkerman EM, Lavini C, Majoie CB, Nederveen AJ, Zwinderman AH, Vos F, Brugman F, van den Berg LH, de Rijk MC, van Doorn PA, Van Hecke W, Peeters RR, Robberecht W, Sunaert S, de Visser M (2011) Upper and extra-motoneuron involvement in early motoneuron disease: a diffusion tensor imaging study. Brain 134(Pt 4):1211–1228
Prell T, Peschel T, Hartung V, Kaufmann J, Klauschies R, Bodammer N, Kollewe K, Dengler R, Grosskreutz J (2013) Diffusion tensor imaging patterns differ in bulbar and limb onset amyotrophic lateral sclerosis. Clin Neurol Neurosurg 115(8):1281–1287
Ellis CM, Simmons A, Jones DK, Bland J, Dawson JM, Horsfield MA, Williams SC, Leigh PN (1999) Diffusion tensor MRI assesses corticospinal tract damage in ALS. Neurology 53(5):1051–1058
Sach M, Winkler G, Glauche V, Liepert J, Heimbach B, Koch MA, Buchel C, Weiller C (2004) Diffusion tensor MRI of early upper motor neuron involvement in amyotrophic lateral sclerosis. Brain 127(Pt 2):340–350
Jones DK, Cercignani M (2010) Twenty-five pitfalls in the analysis of diffusion MRI data. NMR Biomed 23(7):803–820
Smith SM, Jenkinson M, Johansen-Berg H, Rueckert D, Nichols TE, Mackay CE, Watkins KE, Ciccarelli O, Cader MZ, Matthews PM, Behrens TE (2006) Tract-based spatial statistics: voxelwise analysis of multi-subject diffusion data. NeuroImage 31(4):1487–1505
Brooks BR, Miller RG, Swash M, Munsat TL, World Federation of Neurology Research Group on Motor Neuron D (2000) El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotrophic Lateral Scler Other Motor Neuron Disord 1(5):293–299
Rascovsky K, Hodges JR, Knopman D et al (2011) Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain 134(Pt 9):2456–2477
Cedarbaum JM, Stambler N, Malta E, Fuller C, Hilt D, Thurmond B, Nakanishi A (1999) The ALSFRS-R: a revised ALS functional rating scale that incorporates assessments of respiratory function. BDNF ALS Study Group (Phase III). J Neurol Sci 169(1–2):13–21
Nasreddine ZS, Phillips NA, Bedirian V, Charbonneau S, Whitehead V, Collin I, Cummings JL, Chertkow H (2005) The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 53(4):695–699
Griswold MA, Jakob PM, Heidemann RM, Nittka M, Jellus V, Wang J, Kiefer B, Haase A (2002) Generalized autocalibrating partially parallel acquisitions (GRAPPA). Magn Reson Med 47(6):1202–1210
Smith SM, Jenkinson M, Woolrich MW, Beckmann CF, Behrens TE, Johansen-Berg H, Bannister PR, De Luca M, Drobnjak I, Flitney DE, Niazy RK, Saunders J, Vickers J, Zhang Y, De Stefano N, Brady JM, Matthews PM (2004) Advances in functional and structural MR image analysis and implementation as FSL. NeuroImage 23(Suppl 1):S208–S219
Jenkinson M, Smith S (2001) A global optimisation method for robust affine registration of brain images. Med Image Anal 5(2):143–156
Smith SM (2002) Fast robust automated brain extraction. Hum Brain Mapp 17(3):143–155
Smith SM, Nichols TE (2009) Threshold-free cluster enhancement: addressing problems of smoothing, threshold dependence and localisation in cluster inference. NeuroImage 44(1):83–98
Hw L (1967) On the Kolmogorov–Smirnov test for normality with mean and variance unknown. J Am Stat Assoc 62:399–402
Mann HB, Whitney DR (1947) On a test of whether one of two random variables is stochastically larger than the other. Ann Math Stat 18:50–60
Muller HP, Unrath A, Huppertz HJ, Ludolph AC, Kassubek J (2012) Neuroanatomical patterns of cerebral white matter involvement in different motor neuron diseases as studied by diffusion tensor imaging analysis. Amyotrophic Lateral Scler 13(3):254–264
Iwata NK, Aoki S, Okabe S, Arai N, Terao Y, Kwak S, Abe O, Kanazawa I, Tsuji S, Ugawa Y (2008) Evaluation of corticospinal tracts in ALS with diffusion tensor MRI and brainstem stimulation. Neurology 70(7):528–532
Graham JM, Papadakis N, Evans J, Widjaja E, Romanowski CA, Paley MN, Wallis LI, Wilkinson ID, Shaw PJ, Griffiths PD (2004) Diffusion tensor imaging for the assessment of upper motor neuron integrity in ALS. Neurology 63(11):2111–2119
Filippini N, Douaud G, Mackay CE, Knight S, Talbot K, Turner MR (2010) Corpus callosum involvement is a consistent feature of amyotrophic lateral sclerosis. Neurology 75(18):1645–1652
Agosta F, Pagani E, Petrolini M, Caputo D, Perini M, Prelle A, Salvi F, Filippi M (2010) Assessment of white matter tract damage in patients with amyotrophic lateral sclerosis: a diffusion tensor MR imaging tractography study. Am J Neuroradiol 31(8):1457–1461
Abe O, Yamada H, Masutani Y, Aoki S, Kunimatsu A, Yamasue H, Fukuda R, Kasai K, Hayashi N, Masumoto T, Mori H, Soma T, Ohtomo K (2004) Amyotrophic lateral sclerosis: diffusion tensor tractography and voxel-based analysis. NMR Biomed 17(6):411–416
Smith MC (1960) Nerve fibre degeneration in the brain in amyotrophic lateral sclerosis. J Neurol Neurosurg Psychiatry 23(4):269–282
Acosta-Cabronero J, Alley S, Williams GB, Pengas G, Nestor PJ (2012) Diffusion tensor metrics as biomarkers in Alzheimer’s disease. PLoS ONE 7(11):e49072
Sajjadi SA, Acosta-Cabronero J, Patterson K, Diaz-de-Grenu LZ, Williams GB, Nestor PJ (2013) Diffusion tensor magnetic resonance imaging for single subject diagnosis in neurodegenerative diseases. Brain 136(Pt 7):2253–2261
Acosta-Cabronero J, Williams GB, Pengas G, Nestor PJ (2010) Absolute diffusivities define the landscape of white matter degeneration in Alzheimer’s disease. Brain 133(Pt 2):529–539
Nir TM, Jahanshad N, Villalon-Reina JE, Toga AW, Jack CR, Weiner MW, Thompson PM, Alzheimer’s Disease Neuroimaging I (2013) Effectiveness of regional DTI measures in distinguishing Alzheimer’s disease, MCI, and normal aging. NeuroImage Clin 3:180–195
Cistaro A, Valentini MC, Chio A, Nobili F, Calvo A, Moglia C, Montuschi A, Morbelli S, Salmaso D, Fania P, Carrara G, Pagani M (2012) Brain hypermetabolism in amyotrophic lateral sclerosis: a FDG PET study in ALS of spinal and bulbar onset. Eur J Nucl Med Mol Imaging 39(2):251–259
Conflicts of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical standard
The study was approved by the local ethics committee of Otto-von-Guericke University.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Cardenas-Blanco, A., Machts, J., Acosta-Cabronero, J. et al. Central white matter degeneration in bulbar- and limb-onset amyotrophic lateral sclerosis. J Neurol 261, 1961–1967 (2014). https://doi.org/10.1007/s00415-014-7434-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-014-7434-4