
Abstract
Identifying frontal impairment in ALS is an important goal albeit disease-dedicated tools are still scarce. For this reason, we decided to consider primitive reflexes (PRs), variably regarded as correlates of frontal release and/or of upper motor neuron (UMN) impairment, often in the setting of dementias. Specifically, the aims of this work consisted in assessing the exact prevalence of the combination of seven PRs in ALS, trying to clarify their role as putative proxies of cognitive impairment or of UMN dysfunction. In this cross-sectional study, 50 consecutive ALS outpatients were evaluated for the presence of: palmomental (PM), corneomandibular (CM), glabella tap (MY), rooting, sucking, snout, and grasping reflexes. Cognitive screening was performed by the Frontal Assessment Battery (FAB) and the Weigl’s Sorting test (WST); UMN dysfunction was concomitantly evaluated. PM, CM and MY were more frequently detected (62, 52, and 44 % of the ALS sample, respectively), while the other reflexes were under-represented. Patients displaying three or more PRs had significantly lower FAB and WST scores. On the other hand, UMN dysfunction was only moderately associated to PRs. In conclusion, PRs’ assessment is a promising complementary tool for screening cognitive impairment in ALS; however, further work will be necessary to establish its added value with respect to already existing ALS-dedicated screening tools for cognition.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative disorder primarily affecting motoneurons, for which a clear clinico-pathological continuum with frontotemporal degeneration (FTD) has been outlined [1, 2]. This appears to have profound implications in terms of prognosis, since ALS patients displaying dysexecutive deficits have worse outcome [3, 4]. Although several neuropsychological tests are already available for FTD, most do not account for the marked weakness of ALS patients. This issue might be especially relevant when considering the need for retesting patients along the disease course, when functional capacities decline further [5]. There is a strong need for ALS-dedicated cognitive screening tools, and some started to appear [6, 7]. In fact, current ALS management guidelines recommend this screening, but they do not yet specify which tools represent the best choice [8].
Primitive reflexes (PRs) represent a group of motor responses normally seen in early infancy and usually disappearing during adulthood, although rarely they may persist later in life [9]. They can be variously categorized: several are nociceptive (or exteroceptive) reflexes, e.g., glabellar tap (or Myerson’s sign), palmomental, snout, corneomandibular (or Wartenberg’s reflex), etc. Albeit related, others belong to the group of prehensile reflexes, e.g., sucking, palmar grasping. Another grouping considers the “oral primitive reflexes”, i.e., sucking, rooting and snout [9].
The exact significance of PRs is still highly debated since they have been consistently shown in healthy subjects [10], showing little value in neurological localization [11]. Traditionally, PRs have been regarded as correlates of frontal release [12]; other Authors considered them as expression of generalized brain dysfunction, including coma [13], delirium [14], or cognitive impairment [15] and sometimes also as possible proxies of upper motor neuron (UMN) involvement, as in pseudobulbar palsy [16]. Albeit quite controversial [9], this latter issue is also of interest in ALS clinical practice due to the relative lack of UMN signs related to the bulbar region.
Primary aim of this work consisted in assessing the exact prevalence and value of the combination of seven PRs in 50 ALS outpatients undergoing to routine cognitive screening. Furthermore, as secondary aim, the combined prevalence of these PRs was also analyzed with respect to the degree of UMN involvement based on three reflexes expressing UMN impairment in three different regions meaningful for El Escorial diagnostic purposes [17]. Secondary aims included also the attempt of addressing if PRs might be more properly considered as expression of cognitive impairment or UMN dysfunction (or both); this question, indeed, can be ideally addressed in ALS where the two components might be independently present.
Materials and methods
Patients and assessments
Following ethical approval and informed consent, 50 consecutive ALS outpatients were recruited (Table 1). Inclusion criteria were: any outpatient with a diagnosis of possible, probable or definite ALS according to El Escorial criteria [17]. Each patient was screened for dysexecutive dysfunction by the Italian version of the frontal assessment battery (FAB) [18]; considering the bias introduced by pro-rating FAB in those patients presenting marked upper limb weakness (n = 14 [28 %] [5] ), the Weigl’s Sorting Test (WST) [19] was administered. Test results were age- and education- adjusted.
UMN involvement was assessed by testing three classical UMN reflexes: bulbar impairment was assessed by the jaw jerk (UMN-1); Hoffmann’s sign (UMN-2) and the plantar reflex (UMN-3, scored as positive if either showing an extensor response or full Babinski sign) were also recorded bilaterally in all patients for cervical/thoracic and lumbosacral involvement, respectively. UMN-2 and UMN-3 were scored as positive even if the reflex was demonstrated just unilaterally. The sum of the three UMN (UMN total score, t-UMN) was considered as well and patients were dichotomized as either positive (t-UMN score 2–3), or negative (t-UMN score 0–1).
Primitive reflexes
A battery of seven primitive reflexes was administered bilaterally, including: (1) palmomental (PM), (2) corneomandibular (CM), (3) glabella tap (MY), (4) rooting (RO), (5) sucking (SU), (6) snout (SN), and (7) grasping (GR) reflexes. Patients were sitting and a single trial was given for each manoeuvre; for bilateral reflexes, PR was considered present (“positive”) even when the stimulation of just one side evoked a pathological response. Each positive PR was scored as 1 (versus 0 if absent) and the sum of PRs was computed for each patient. For inter-rater reliability, this PR battery was assessed in two different examination rooms during the same session by two raters (an experienced neurologist and a senior resident); for all other analyses only the former set of results was considered.
PM was performed applying a dull point stimulus using a Taylor reflex hammer from the thenar eminence at the wrist up to the base of thumb; a positive result was scored when the contraction of the orbicularis oris and mentalis muscles was observed [20, 21]. CM (or Wartenberg’s reflex) was performed by asking the patients to open mildly the mouth allowing the mandible to hang loosely while the examiner elevated the patient’s eyelid and mildly touched with cotton the center of either cornea; a positive result was scored when a movement of the mandible to the opposite side was observed [22]. MY was performed applying mild finger tapping over the glabella (ten times at about 1 Hz), usually producing a blinking reflex in both eyes; positive sign (or Myerson’s sign) was considered the failure in extinguishing such response that was present ≥4 times [23, 24]. RO was elicited by gently finger stroking each cheek; a positive result was scored when the mouth of the patient turned toward the stimulus [9]. SU was elicited by gently inserting the finger point into the mouth; a positive result was scored when sucking response was felt by the examiner [9]. SN was elicited by applying gentle pressure with the reflex hammer over the nasal philtrum; a positive result was scored when lips puckered [9]. None of the recruited ALS patients was on neuroleptic drugs that are known to induce oral dyskinesias. GR was elicited by asking to the patient to hold the hands with palms facing up while the examiner stimulated each palmar surface with the handle of a Taylor reflex hammer, by initially briefly placing it (~2 s) and then gently moving away from the patient until complete retraction; a positive result was scored only if a “catching” movement was followed by a “holding” one [9].
Statistical analysis
Data are presented as mean ± standard deviation (SD), except where specifically noted. Statistical analysis was performed by Prism 4.00 (GraphPad Software, Inc.). Two-tailed Student’s t test, ANOVA followed by Newman–Keuls multiple comparison and Pearson’s correlation tests were used as appropriate. Concordance between tests was calculated with the Cohen’s kappa score.
Results
Descriptive statistics and PRs inter-rater reliability
Table 1 reports the clinical and demographic characteristics of the sample; ALS progression rate was calculated as previously described [25], i.e., [(48––current ALSFRS-R score)/disease months]; the FAB was completed by 36 patients (72 %), pro-rate was performed for the remaining 14 subjects (28 %) that did not complete the Luria/grasping items; the WST was completed by all the recruited patients; a correlation with FAB score was present (r = 0.649 p < 0.0001) and the Cohen’s kappa score between these two tests was 0.46, as previously shown [5]. The same patients were not scored for GR. All the other PRs were performed without problems.
PM, MY and CM were consistently reported (62, 52, and 44 %, respectively), while SN was moderately present (14 %), and GR, SU, and RO were definitely under-represented in our sample (5.5, 2 %, and 0, respectively). Kappa score was always high (>0.70) for all PRs.
Average PR sum was 1.78 ± 1.25 (range 0–5). Median PR value was two and most patients [n = 37 (74 %)] displayed from 0 to 2 PRs, while the remaining 13 patients (26 %) presented from 3 to 5 PRs.
PRs as markers of dysexecutive dysfunction in ALS patients
Among the three more represented PRs, CM was associated to significantly lower FAB (13.2 ± 4.07 vs. 16.4 ± 2.17, CM+ vs.CM− , respectively, p = 0.0008 two-tailed Student’s t test) and WST scores (10.0 ± 4.2 vs. 12.3 ± 2.93, p = 0.027), as was MY (FAB: 13.7 ± 4.07 vs. 16.4 ± 2.00, MY+ vs. MY− , respectively, p = 0.0043; WST: 9.6 ± 3.77 vs. 13.1 ± 2.67, p = 0.0004), while PM was not.
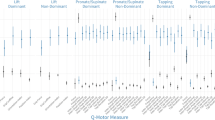
The FAB score was consistently above the cut-off score in the <3 PRs group and, in particular, below in the ≥3 PRs group (p < 0.0001; Fig. 1b). Similarly, dichotomizing patients according to a FAB pathological result, an about twofold increase of average PRs emerged in FAB positive patients with respect to negative ones (Fig. 1a). The FAB score was also overall negatively correlated with the number of positive PRs (r = −0.625 p < 0.0001) and the kappa score was 0.67.

PRs mark dysexecutive dysfunction in ALS patients. a number of positive PRs in FAB positive ALS patients with respect to negative ones (n = 12 vs. 38, respectively; FAB cut-off score ≤ 13.4); b ALS patients with less than 3 PRs displayed on average normal FAB scores, while the opposite was found for those patients presenting with ≥3 PRs (n = 38 vs. 12); c number of positive PRs in WST positive ALS patients with respect to negative ones (n = 9 vs. 41, respectively; WST cut-off score ≤ 8); d ALS patients with less than 3 PRs displayed on average normal WST scores, while borderline average scores were found for those patients presenting with ≥ 3 PRs (n = 38 vs. 12). *p ≤ 0.0007 two-tailed Student’s t test; data are shown as mean ± standard error
WST score was below the cut-off (≤8) in 9 (18 %) patients that again presented an about two-fold increase of PRs (p = 0.0007; Fig. 1c); again, those patients presenting with 0–2 PRs had normal WST scores, while patients with 3–5 PRs displayed average scores just above the test cut-off (p = 0.0005; Fig. 1d). The WST score was also overall negatively correlated with the number of positive PRs (−0.532 p < 0.0001) and the kappa score was 0.46.
PRs and UMN involvement
Among the three more represented PRs, CM positivity was associated to higher t-UMN scores (1.90 ± 0.75 vs. 1.11 ± 0.83, CM+ vs. CM−, respectively, p = 0.0009), while dichotomizing according to MY and PM positivity was not significant. Globally, PRs displayed a tendency to correlation with UMN-1 (r = 0.272 p = 0.055) that was not present when considering both UMN-2 and UMN-3 (p = 0.277 and p = 0.252, respectively). Analogously, dichotomizing patients for UMN-1 presence a tendency toward PR increase was shown (1.56 ± 1.23 vs. 2.21 ± 1.18, UMN-1− vs. UMN-1+, p = 0.055). On the other hand, no relationship was detected between each UMN reflex or t-UMN score and either FAB or WST scores. Conversely, a correlation between PRs and t-UMN scores was present (r = 0.314 p = 0.0261). Similarly, dichotomizing patients for global UMN involvement (see “Methods”) an increase of PRs was shown (1.38 ± 1.13 vs. 2.21 ± 1.25, t-UMN− vs. t-UMN+ , n = 26 vs. 24, p = 0.018).
Exploring PRs overall correlates
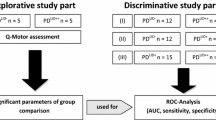
Patients were divided in four groups according to both the FAB scores and the degree of their UMN involvement; average PRs sum score was increased in FAB positive patients more than in t-UMN positive patients (p < 0.0001; Fig. 2) and a significant trend was shown from FAB positive/t-UMN positive patients to FAB+/t-UMN−, to FAB−/t-UMN+, to FAB−/t-UMN− (post-test for linear trend r 2 = 0.346 p < 0.0001) (see Fig. 2).

Analysis of PR correlates. PRs score with respect to FAB status (F+ vs. F−) and UMN involvement (U+ vs. U−, t-UMN score 0–1 vs. 2–3, respectively). p < 0.0001 at ANOVA, followed by Newman–Keuls multiple comparison post-hoc test, *p < 0.001 vs. F+ U+ and F+ U−, p < 0.01 vs. F–U+; °p < 0.05 vs. F+ U+ and F+ U−; F+ U+ vs. F+ U− not significant
Finally, the number of positive PRs correlated to disease progression rate (r = 0.352 p = 0.012) but failed to show any other meaningful relationship with the other continuous or dichotomous clinical and demographic variables, including the site of onset (bulbar versus spinal onset, p = 0.144), correlation with disease duration (p = 0.56), and with the ALSFRS-R score (p = 0.18). On the other hand, bulbar patients displayed a tendency to lower FAB scores with respect to spinal ones (13.1 ± 5.3 vs. 15.4 ± 2.8, respectively, p = 0.066) that reached significance for the WST (8.3 ± 3.8 vs. 11.9 ± 3.4, p = 0.007).
Discussion
We investigated the prevalence and correlates of seven different PRs in a representative sample of ALS outpatients. Our results indicate that albeit each single PR might display limited value, perhaps with the partial exception of CM, the entire battery possesses a synergistic value in screening those patients with cognitive dysfunction or expressing larger UMN involvement. In particular, ALS patients displaying three or more PRs scored, on average, below or just minimally above the cut-off in two tests exploring frontal lobe functions. Certainly, these two tests do not explore the complete cognitive status of our patients and cannot substitute an entire test battery. On the other hand, ALS-dedicated tools are scanty and patients with impaired functional capabilities might not be able to fully complete specific cognitive tests (as in the case of the FAB Luria item) or a full battery (due to fatigue or hypoxia). We expressly chose the WST for overcoming the bias introduced by pro-rating FAB in ALS patients exhibiting profound upper limb weakness [5]. In addition, WST, exploring a single dysexecutive domain (sorting), as opposed to the FAB mini-battery not including this function, allowed to confirm the idea that PRs are correlated to a broadly defined frontal lobe dysfunction. Admittedly, we did not consider the behavioral correlates of the dysexecutive syndrome which might be analogously related to frontal lobe involvement. Further work exploring cognitive and behavioral (e.g., with the Frontal Systems Behavior Scale) correlates of PRs in ALS might be useful to understand the exact meaning of the differences found when considering each single PR performance.
Besides cognition, PRs were also weakly correlated with the estimated degree of UMN involvement. Here, UMN involvement was defined including, where possible, primitive multi-synaptic reflexes (e.g., plantar response and Hoffmann’s sign). Furthermore, we tried to cover all the regions meaningful for ALS diagnosis (bulbar, cervical/thoracic, lumbosacral). Deep tendon reflexes were eventually excluded due to the potential bias deriving from interpreting the finding of normal reflexes in amyotrophic regions as expression of UMN involvement. On the other hand, the three included UMN reflexes usually show responses easily scored either as present or absent. Possibly other UMN tools might be considered for future works, such as finger or foot tapping. Pseudobulbar affect and, possibly, spastic dysarthria might be included as well, albeit clear-cut operational criteria will be required for their assessment [26]. The relatively selective UMN scoring strategy we adopted might have less sensitivity, possibly resulting in a limitation of its discriminative power in defining the exact meaning of PRs.
Globally, however, our results indicate that PRs were more consistently correlated with cognitive dysfunction with respect to UMN impairment. To our knowledge, this is the first time that a condition, such as ALS, where these two components may independently coexist, is explored. Our conclusion is that PRs might be more properly considered when implementing batteries for cognitive screening in ALS, especially in an outpatient setting. The lower association to UMN, albeit significant, will deserve further consideration in larger series, also given the implicit source of bias caused by the eventual coexistence of LMN dysfunction which might mask UMN signs. Last but not least, few patients with 3 or more PRs without cognitive impairment were recorded. The possibility exists that PRs might precede cognitive dysfunction, and, possibly, even UMN reflex appearance. Follow-up of the patients is required for answering to this question.
The present PR battery undoubtedly needs some refinement, and in future works some reflexes might be eliminated, either for their low prevalence in ALS (e.g., SU and RO), or for the difficulty at assessing the reflex in all patients (e.g., GR). Furthermore, some PR manoeuvres may lead to false positive results, especially for the unexperienced clinician, for example when prominent spasticity is present; this might be the case for GR (spastic catch) or SN (gentle hitting instead of touching might be evoking a myotatic response and not a primitive one, [9]). Indeed, the two raters briefly trained in PR execution before engaging in the study and PR kappa score was always quite good; possibly, we also have to consider that in real world these values might be lower or displaying much more consistent variability. As a matter of fact, our prevalence rates are different with respect to a previous work where CM was found in 71 % of ALS patients, while the same subjects had extensor plantar response in only 36 % of the cases [22]. This might not be surprising considering that consistent variability has been previously shown for the well-known extensor plantar response [27]. On the other hand, false negative results should also be expected considering that extensive LMN dysfunction, besides affecting the clinician’s ability to elicit UMN involvement, might also contribute to lower PR prevalence in these patients. Further work on larger patient cohorts might be useful to detect more precisely the exact prevalence of these responses in ALS (external validity).
When analyzed separately, both CM and MY resulted in good performances (~50 %). CM was robustly associated to both FAB and UMN positive status, while MY was associated to cognitive impairment alone, thus discriminating between the two dysfunctions. However, the synergistic value of the entire battery emerged particularly with respect to cognition, since patients displaying three or more PRs had on average lower test scores in a clinically significant way. For this reason, PM, too, should be probably included in future studies, in spite of its apparent lack of discriminative power. At this point, we may hypothesize that in a screening PR mini-battery dedicated to ALS, CM, MY and PM should be included, and patients scoring positive at all three manoeuvres might deserve further cognitive characterization. Furthermore, PR manoeuvres are fast, simple and reliable, making them suitable for testing ALS patients at any stage of the disease without the bias introduced by advanced disability [5]. On the other hand, one may argue that grouping PRs without knowing the exact neural correlate for each of them might be questionable. Indeed, the choice for our PR battery included a combination of exteroceptive reflexes (CM, PM, MY), oral primitive ones (SN, SU, RO), reflexes implying complex behavioral responses (GR, but also SU, RO), or sensory gating deficit/perseveration (MY). However, the most relevant issue related to PR clinical translation in literature is centered on their absolute value: each single PR does not display sufficient specificity, and sometimes sensitivity, to stand as a useful tool for clinicians. This stringent argument against PR clinical use has been strongly reinforced by their presence, usually with low prevalence, also in healthy controls [20, 28]. Hence, in an attempt at overcoming these limits, some Authors already tried to combine different PRs to test the resulting synergistic value, under the assumption that they might be exploring the same broadly defined dysfunction [14, 29]. The combination of more than two positive PRs resulted in increased specificity for particular subtypes of dementing disorders, such as Lewy body [30] or vascular dementia [15]. Intriguingly enough, the exact prevalence of PRs in FTD is still unclear and reports are not in agreement [31, 32]. Some work has also been produced on single PRs in ALS; perhaps, the most critically appraised PR in ALS has been CM, reported in 30 out of 42 patients. Notably, CM was able to distinguish between ALS and cerebrovascular disease, regardless of pseudobulbar presentation, and the Authors concluded that it might reliably mark UMN involvement [22]. These conclusions should be now reviewed because cognitive screening was not yet part of routine ALS clinical assessment.
Finally, in our series PRs were not associated to bulbar presentation, although our conclusions cannot be firmly drawn because only a minority of patients presented with this site of onset. WST scores were significantly lower in bulbar patients but FAB failed to confirm the association with cognitive impairment, suggesting that our study cannot answer to this question. Finally, PRs were correlated to disease progression rate, indirectly suggesting that cognitive dysfunction might identify more rapidly evolving patients, as already pointed out [3, 4]. Further research directions might include to study PR neural correlates by advanced neuroimaging techniques.
In conclusion, our study suggests that PRs deserve further examination as a promising proxy for cognitive screening of ALS outpatients or, at least, as complementary items in dedicated psychometric mini batteries. This issue is of great relevance considering the actual need for specific tools able to reliably bypass the motor handicaps of these patients.
References
Robberecht W, Philips T (2013) The changing scene of amyotrophic lateral sclerosis. Nat Rev Neurosci 14:248–264
Ling SC, Polymenidou M, Cleveland DW (2013) Converging mechanisms in ALS and FTD: disrupted RNA and protein homeostasis. Neuron 79:416–438
Chiò A, Ilardi A, Cammarosano S, Moglia C, Montuschi A, Calvo A (2012) Neurobehavioral dysfunction in ALS has a negative effect on outcome and use of PEG and NIV. Neurology 78:1085–1089
Elamin M, Bede P, Byrne S, Jordan N, Gallagher L, Wynne B, O’Brien C, Phukan J, Lynch C, Pender N, Hardiman O (2013) Cognitive changes predict functional decline in ALS: a population-based longitudinal study. Neurology 80:1590–1597
Tremolizzo L, Ferrarese C, Appollonio I (2013) Exploring limits of neuropsychological screening in ALS: the FAB problem. Amyotroph Lateral Scler Frontotemporal Degener 14:157–158
Woolley SC, York MK, Moore DH, Strutt AM, Murphy J, Schulz PE, Katz JS (2010) Detecting frontotemporal dysfunction in ALS: utility of the ALS cognitive behavioral screen (ALS-CBS). Amyotroph Lateral Scler 11:303–311
Abrahams S, Newton J, Niven E, Foley J, Bak TH (2014) Screening for cognition and behaviour changes in ALS. Amyotroph Lateral Scler Frontotemporal Degener 15:9–14
Miller RG, Jackson CE, Kasarskis EJ, England JD, Forshew D, Johnston W, Kalra S, Katz JS, Mitsumoto H, Rosenfeld J, Shoesmith C, Strong MJ, Woolley SC, Quality Standards Subcommittee of the American Academy of Neurology (2009) Practice parameter update: the care of the patient with amyotrophic lateral sclerosis: multidisciplinary care, symptom management, and cognitive/behavioral impairment (an evidence-based review): report of the quality standards subcommittee of the American academy of neurology. Neurology 73:1227–1233
Schott JM, Rossor MN (2003) The grasp and other primitive reflexes. J Neurol Neurosurg Psychiatry 74:558–560
Strong MJ (2012) Amyotrophic lateral sclerosis and the frontotemporal dementias. Oxford University Press, Oxford
Brazis PW, Masdeu JC, Biller J (eds) (2012) Localization in clinical neurology. Lippincott Williams & Wilkins, London
Girling DM, Berrios GE (1990) Extrapyramidal signs, primitive reflexes and frontal lobe function in senile dementia of the Alzheimer type. Br J Psychiatry 157:888–893
Heliopoulos I, Vadikolias K, Tsivgoulis G, Mikroulis D, Tsakaldimi S, Piperidou C (2013) Corneomandibular reflex (Wartenberg reflex) in coma: a rarely elicited sign. JAMA Neurol 70:794–795
Nicolson SE, Chabon B, Larsen KA, Kelly SE, Potter AW, Stern TA (2011) Primitive reflexes associated with delirium: a prospective trial. Psychosomatics 52:507–512
Di Legge S, Di Piero V, Altieri M, Vicenzini E, Tombari D, Di Stani F, Lenzi GL (2001) Usefulness of primitive reflexes in demented and non-demented cerebrovascular patients in daily clinical practice. Eur Neurol 45:104–110
Loeb C, Gandolfo C, Caponnetto C, Del Sette M (1990) Pseudobulbar palsy: a clinical computed tomography study. Eur Neurol 30:42–46
Brooks BR, Miller RG, Swash M, Munsat TL, World Federation of Neurology Research Group on Motor Neuron Diseases (2000) El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disord 1:293–299
Appollonio I, Leone M, Isella V, Piamarta F, Consoli T, Villa ML, Forapani E, Russo A, Nichelli P (2005) The frontal assessment battery (FAB): normative values in an Italian population sample. Neurol Sci 26:108–116
Laiacona M, Inzaghi MG, De Tanti A, Capitani E (2000) Wisconsin card sorting test: a new global score, with Italian norms, and its relationship with the Weigl sorting test. Neurol Sci 21:279–291
Owen G, Mulley GP (2002) The palmomental reflex: a useful clinical sign? J Neurol Neurosurg Psychiatry 73:113–115
Marinesco G, Radovici A (1920) Sur un reflexe cutane nouveau: reflexe palmo-mentonnier. Rev Neurol 27:237–240
Okuda B, Kodama N, Kawabata K, Tachibana H, Sugita M (1999) Corneomandibular reflex in ALS. Neurology 52:1699–1701
Pearce J, Aziz H, Gallagher JC (1968) Primitive reflex activity in primary and symptomatic Parkinsonism. J Neurol Neurosurg Psychiatry 31:501–508
Jenkyn LR, Walsh DB, Culver CM, Reeves AG (1977) Clinical signs in diffuse cerebral dysfunction. J Neurol Neurosurg Psychiatry 40:956–966
Aliberti S, Messinesi G, Gramegna A, Tremolizzo L, Susani E, Pesci A (2013) Diaphragm ultrasonography in the management of patients with amyotrophic lateral sclerosis. Amyotroph Lateral Scler Frontotemporal Degener 14:154–156
Smith RA, Berg JE, Pope LE, Thisted RA (2004) Measuring pseudobulbar affect in ALS. Amyotroph Lateral Scler Other Motor Neuron Disord 5(Suppl 1):99–102
Miller TM, Johnston SC (2005) Should the Babinski sign be part of the routine neurologic examination? Neurology 65:1165–1168
Marti-Vilalta JL, Graus F (1984) The palmomental reflex. Clinical study of 300 cases. Eur Neurol 23:12–16
Isakov E, Sazbon L, Costeff H, Luz Y, Najenson T (1984) The diagnostic value of three common primitive reflexes. Eur Neurol 23:17–21
Borroni B, Broli M, Costanzi C, Gipponi S, Gilberti N, Agosti C, Padovani A (2006) Primitive reflex evaluation in the clinical assessment of extrapyramidal syndromes. Eur J Neurol 13:1026–1028
Links KA, Merims D, Binns MA, Freedman M, Chow TW (2010) Prevalence of primitive reflexes and Parkinsonian signs in dementia. Can J Neurol Sci 37:601–607
Sjögren M, Wallin A, Edman A (1997) Symptomatological characteristics distinguish between frontotemporal dementia and vascular dementia with a dominant frontal lobe syndrome. Int J Geriatr Psychiatry 12:656–661
Acknowledgments
Mrs. Sofia Rosso and the Italian association for ALS (AISLA).
Conflicts of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Tremolizzo, L., Susani, E., Lunetta, C. et al. Primitive reflexes in amyotrophic lateral sclerosis: prevalence and correlates. J Neurol 261, 1196–1202 (2014). https://doi.org/10.1007/s00415-014-7342-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-014-7342-7