
Abstract
Multiple sclerosis (MS) is an incurable disease, and despite current pharmacologic treatment being effective in reducing relapse rates and lesion burden, there is little evidence that these treatments work as effectively in preventing disability progression. In such cases, non-pharmacologic techniques such as exercise therapy with rehabilitation purposes may play an important role. This systematic review of randomised controlled trials (RCTs) aims at investigating the effects of exercise therapy in MS patients. The electronic database PubMed was searched for studies indexed between February 2004 and June 2012. Studies eligibility criteria included: clinical diagnosis of MS free of exacerbation; and intervention with exercise therapy, measured as activities of daily living (ADL). Two reviewers independently screened the titles and abstracts of the references retrieved. The methodological quality of the RCTs was assessed using the Physiotherapy Evidence Database scale (PEDro scale). The PubMed search resulted in a total of 72 articles, 11 of which were included in this review. The analysis included 591 participants, of which 358 (60.6 %) were women. Patients had a mean age between 37.1 and 54.6 years. Duration of MS since diagnosis was reported in nine of the 11 studies and varied between 5.2 and 15.9 years. According to PEDro scale, nine of the 11 included studies were considered to be of high methodological quality, with scores ranging from 7 to 10. In eight of the 11 included studies, the effectiveness of exercise therapy was compared to standard care, in two it was compared to those on a waiting list, and in one, to control treatment. The results of this review suggest that exercise therapy may have a beneficial effect in patients with MS, and therefore may be recommended for the rehabilitation of these patients.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Multiple sclerosis (MS) is a chronic inflammatory immune-mediated demyelinating disease of the central nervous system. The worldwide incidence of MS is currently estimated to be 3.6 cases per 100,000 person-years (95 % CI 3.0, 4.2) for women and 2.0 cases per 100,000 person-years (95 % CI 1.5, 2.4) for men. The ratio of female to male incidence of MS has increased over time from an estimated 1.4 in 1955 to 2.3 in 2000 [1].
MS is the most common disabling neurological disease in young adults in Western Europe and in North America [2]. The disease has an unpredictable course, yet the most frequent is the relapsing remitting course, with recurring attacks of acute focal neurological deficits (relapses) alternating with periods of remission, which can be partial or full [3]. The clinical manifestations of MS include motor, sensory, visual, brainstem, cerebellar, cognitive and sphincter signs/symptoms. Ultimately, the natural progression of MS leads to an accumulation of irreversible neurologic deficits [4].
Currently, MS is an incurable disease and its pharmacological treatment relies upon three categories: an increasing armamentarium of disease-modifying drugs (DMD) specifically designed for MS, corticosteroids for acute exacerbations, and various drugs for symptomatic control. DMD reduce the relapse rates and lesion burden, although there is less evidence that they are effective in preventing disability progression [5–7]. Thus, therapeutic strategies for symptom management, including non-pharmacological techniques with rehabilitation purposes, play an important role.
There is systematic review evidence suggesting that exercise therapy is an effective treatment for MS [8]. Nevertheless, due to several limitations of the reviewed studies (e.g. small sample sizes, not controlling for confounders such as patient variability and dose of exercise), the results were not conclusive. Furthermore, although the reviewed studies measured the same domains, different outcomes were used. Consequently, it was not possible to do a meta-analysis and to calculate the effects size of exercise therapy in MS patients.
To investigate the effects of exercise therapy in MS patients, we systematically reviewed randomised controlled trials (RCTs) about this subject. Only RCTs published after those included in the most recent systematic review about this subject [7] (i.e. between February 2004 and June 2012) were reviewed in this study.
Methods
This was a systematic review of RCTs regarding the effects of exercise therapy versus placebo in patients with MS. Exercise therapy was defined as a regimen, or plan of physical activity, designed and prescribed for the therapeutic goal of restoring normal musculoskeletal function of MS patients. The placebo interventions included standard care (i.e. the care the participants would receive normally, had they not been included in the trial), control treatment (i.e. treatment lacking the variable tested in the treatment group), and patients on a waiting list for receiving the intervention.
The RCTs had to include participants with a clinical diagnosis of MS free of exacerbation. The participants could be of either sex and of all ages. The interventions included in this work were those that matched the exercise therapy definition presented above, and that were measured in terms of activities of daily living (ADL). The ADL considered for this review were: fatigue, exercise tolerance, walking, gait and maintaining body position. Interventions such as electric stimulation, transcutaneal electrical nerve stimulation, cryostimulation, and whole body vibration were excluded.
The electronic database PubMed was searched for studies indexed between February 2004 and June 2012. Only English language studies were considered for this review. The used search strategy was as follows: (((((“Multiple Sclerosis/rehabilitation”[Mesh] OR “Multiple Sclerosis/therapy”[Mesh])) NOT “Multiple Sclerosis/drug therapy” [Mesh])) AND (“Controlled Clinical Trial”[Publication Type] OR “Randomized Controlled Trials as Topic”[Mesh] OR “Randomized Controlled Trial”[Publication Type])) AND ((“Exercise Therapy”[Mesh] OR “Physical Therapy Modalities”[Mesh] OR “Physical Therapy Department, Hospital”[Mesh]) OR “Exercise”[Mesh])”.
Two reviewers independently screened the titles and abstracts of the references retrieved using the above search strategy. Full text articles were obtained for all the references considered eligible for inclusion by both reviewers. Disagreements between the reviewers were resolved by consensus.
Data from the RCTs were extracted using a data extraction sheet developed for this purpose. Data extraction was performed by one reviewer, and then this was cross-checked by a second reviewer. The collected data were: (a) name of the authors; (b) characteristics of the participants (number, sex, age, type of MS, disease duration, Expanded Disability Status Scale [EDSS] score); (c) description of the intervention and follow-up; (d) dose of the intervention (duration, frequency and intensity); (e) results. No authors were contacted for further information.
The quality of the RCTs was assessed using the Physiotherapy Evidence Database scale (PEDro scale) [9]. This scale is used for rating the methodological quality of RCTs according to a list of 11 criteria. The first criterion rates whether the eligibility criteria for the RCT were specified, and it is used to assess the external validity of the study (i.e. generalizability of the results). The other ten criteria rate clear reporting of: random allocation of participants, concealed allocation of participants, similarity at baseline for most important prognostic indicators, blinding of participants, blinding of therapists, blinding of assessors, follow up of more than 85 % of the randomised participants, intention to treat analysis, between-group statistical comparisons and variability measures for at least one outcome. These criteria are used to assess the internal validity of the study (i.e. extent to which causality has been established), and the last two criteria are also used to establish whether the study provided sufficient statistical information to make the results interpretable. A point is awarded for each clearly satisfied criterion; otherwise, no point is awarded. In this way, RCTs are rated between 1 and 11, with higher scores indicating higher methodological quality. For the purpose of this review, RCTs scored 6 or higher were considered to be of “high quality,” and those with scores lower than 6 were considered to be of “low quality”. The methodological quality of the RCTs was assessed independently by two reviewers and score disagreements were resolved by consensus.
Results
Study selection
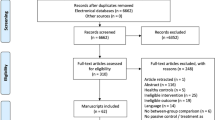
The Pubmed search resulted in a total of 72 articles. As presented in Fig. 1, after the screening of titles and abstracts, 17 articles were considered to be eligible to be included, and after reading the full text, 11 articles were included in this review.

Flowchart for the selection of the included articles
Participants
A total of 591 participants were included in the analysis, 358 (60.6 %) of which were women, and the mean age of all participants varied between 37.1 and 54.6 years old. The duration of MS diagnosis was only reported in nine studies [10–18], and this value varied, on average, between 5.2 and 15.9 years. Mean EDSS scores were reported in six studies [10, 11, 13, 16, 17, 19] and median EDSS scores were reported in two studies [14, 15] (see Table 1). All participants were diagnosed with MS, in five studies [11, 12, 14–16] according to Poser criteria [21], in two studies [17, 19] according to McDonald criteria [22], and in four studies [10, 13, 18, 20] no diagnosis criteria were presented. Detailed information about patient characteristics is presented in Table 1.
Methodological quality
The PEDro scores for the methodological quality of the RCTs varied between 4 and 10 (see Table 2). However, in any of the studies, the participants were blinded, as this does not apply to physical therapy interventions. The three most common methodological quality criteria that were not identified in the studies were: “There was blinding of all therapists who administered the therapy”; “There was blinding of all assessors who measured at least one key outcome”; “All subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analysed by intention to treat”. Nine out of the 11 studies [10, 12–17, 19, 20] were considered to be of high methodological quality, with PEDro scores ranging from 7 to 10.
Adverse events
Only three of the RCTs [13, 19, 20] investigated whether the interventions in place were associated with adverse events (AE). No AEs were reported at all in two RCTs [13, 19], and one non-serious AE (muscle soreness that was resolved within a few days) was reported in one RCT [20].
Effectiveness of exercise therapy versus standard care
Exercise therapy was compared to standard care in eight studies [11–15, 17, 18, 20]. Six out of these were considered to be of high methodological quality (see Table 2) [12–15, 17, 20].
Cattaneo et al. [12] did a 3-week pilot study about the effects of balance exercises on motor and sensory strategies of MS patients. Group 1 (G1) received balance rehabilitation to improve motor strategies (e.g. patients were retrained with standing and dynamic tasks) and sensory strategies (e.g. sensory compensation and habituation), group 2 (G2) received task-oriented balance rehabilitation to improve motor strategy, and not specifically to improve sensory strategy, and group 3 (G3) received standard care. Fifty patients were randomized to each of the three groups, but six patients were lost to follow-up. Despite this, all patients were considered for statistical analysis. The follow-up was carried out at week 3 after study start. The Berg Balance scale and Dynamic Gait index scores significantly improved in G1 when compared to G3. The Berg Balance scale score significantly improved in G2 when compared to G3, but only when excluding the losses to follow-up. No significant differences between groups were identified for activities specific to balance confidence and for the modified dizziness handicap inventory.
Dalgas et al. [17], 2007, investigated the effects of a progressive resistance training (PRT) programme on MS patients. This programme lasted for 12 weeks. It included exercises for the lower extremities (leg press, knee extension, hip flexion, hamstring curl and hip extension), and the intensity of the exercises increased over time according to a progression model. Thirty-eight patients were randomised to an exercise group or to a standard care group. Out of these patients, seven were lost-to-follow-up and, therefore, only 31 patients were considered for statistical analysis. The follow up was carried out 12 weeks after study start. The one-dimensional Fatigue Severity scale and general fatigue of the Multidimensional Fatigue Inventory scores significantly improved in the exercise group when compared to standard care. The SF-36 physical component also improved significantly in the exercise group when compared to the control group. No significant differences between groups were identified for physical fatigue, reduced motivation, reduced activity and mental fatigue of the multidimensional fatigue inventory, and no significant differences were found between groups for the SF-36 mental component.
Dodd et al. [20] investigated the effects of a 10-week PRT programme on MS patients, at a community gymnasium. The included exercises were leg press, knee extension, calf raise, leg curl, reverse leg press. The intensity of the exercises increased over time according to a progression model based on the American College of Sports Medicine [23]. Seventy-six patients were randomised either to a treatment group or to standard care, but five patients were lost-to-follow up. Despite this, all patients were considered for statistical analysis. Follow-ups were carried out 10 and 22 weeks after study start. The walking distance over 2 min (primary variable) did not significantly improve in the exercise group, when compared to standard care, both after 10 and 22 weeks of PRT.
McCullagh et al. [18] investigated the effects of a 12-week physiotherapy programme in MS patients. This programme was carried out at a gym, and it included exercises such as treadmill walking/running, cycling, stair-master training, arm-strengthening exercises, volleyball and outdoor walking. Seventy-six patients were randomised to an exercise group or to standard care. There were no losses to follow-up, and therefore, all patients were considered for the statistical analysis. Follow-ups were carried out 3 and 6 months after study start. The Modified Fatigue Impact Scale score in the exercise group significantly improved, when compared to control, both after 3 and 6 months of training.
Miller et al. [13] investigated the effects of an 8-week home-based physiotherapy programme in MS patients. This programme included upper and lower limb strengthening using Theraband, mobile pedals, and weights. Thirty patients were randomised either to exercise group or to standard care. There were no losses to follow-up, and therefore, all patients were considered for the statistical analysis. The follow-ups were carried out at 8 and 16 weeks after study start. Right knee extension, right knee flexion and left knee flexion significantly improved for the exercise group when compared to control, after the 16 weeks of training. No significant differences between groups were identified for left knee extension.
Romberg et al. [14] investigated the effects of a 6-month PRT programme combined with aerobic training in MS patients. The programme included exercises for lower and upper extremities, and for the trunk. Therabands were used both for lower and upper extremities. The number of exercise repetitions changed over time, as well as the stiffness of the Therabands, in order to increase the intensity of the exercises. As determined by a sample size calculation, 114 patients were randomised either to an exercise group or to standard care. There were no losses to follow-up, and for this reason, all patients were considered in the statistical analysis. The follow-up was carried out 6 months after study start. The results for the 7.62-m walking test, 500-m walking test, and the first 500 m of the walking tests significantly improved in the exercise group, when compared to control. No significant differences between the groups were identified for the final 50 m of the 500 m walking test, knee extension and knee flexion.
Further results of the above study were published in a later paper by Romberg et al. [15]. In this paper, it was reported that, the 25-foot walking test and of the 9-hole Peg test significantly improved in the exercise group when compared to control.
Surakka et al. [11] investigated the effects of aerobic combined with resistance training in patients with MS. This programme included five supervised sessions over 3 weeks, followed by a home training programme for 23 weeks. The resistance training included circuit of exercises (i.e. scapular adduction, hip extension, arm pull down, seated abdomen, hip abduction, triceps push, seated back, leg curl, biceps brachii curl and knee extension), and the aerobic training included gymnastic exercises in shoulder-deep water. The home training programme included exercises for the same muscle groups that were trained during the first 3 weeks. One hundred and fourteen patients were randomised to exercise group or to standard care, but 19 patients were lost to follow up. Therefore, 95 patients were considered for statistical analysis. The follow-up was carried out 6 months after study start. The fatigue index for leg flexion, significantly improved for the women of the treatment group when compared to women in the control group. No significant improvements were identified for the fatigue index for left leg extension, in either men or women, and for the fatigue index for left leg flexion in men.
Effectiveness of exercise therapy versus waiting list
Exercise therapy was compared to waiting list in two studies [16, 19]. Both studies were considered to be of high methodological quality (see Table 2).
Mutluay et al. [16] investigated the effects of breathing-enhanced upper extremity in MS patients. The exercises included all the relevant procedures involving arm motions recommended by Watchie [24] (e.g. while sitting on a chair, inhale while flexing both arms up over the head and then exhale while returning the arms to the sides). Outpatients from a neurology clinic were recruited for this study. Forty patients were randomised to exercise group or to a waiting list. There were no losses to follow-up, and therefore, all patients were considered for the statistical analysis. The follow-up was carried out 6 weeks after study start. The 6-min walking test significantly improved in the treatment group when compared to the waiting list.
Oken et al. [19] investigated the effects of aerobic training and of yoga in MS patients. The aerobic training consisted of bicycling on recumbent or dual-action stationary bicycles, and the yoga class was an Iyengar yoga class, modified to take into account fatigue as well as spasticity and cerebellar dysfunction. Sixty-nine patients were randomised to exercise group, yoga group or to a waiting list, but two patients were lost to follow-up. Despite this, all patients were considered for statistical analysis. The follow-up was carried out 6 months after study start. The short-form 36 health survey and the multidimensional fatigue inventory physical scale, significantly improved in aerobic training and in yoga groups, when compared to wait list. No significant differences between intervention groups and waiting list were identified for reduced activity, reduced motivation and mental fatigue of the multidimensional fatigue inventory.
Effectiveness of exercise therapy versus control treatment
Exercise therapy was compared to control treatment in one study [10]. This study was considered to be of high methodological quality.
Dettmers et al. [10] investigated the effects of endurance exercises in MS patients. The exercises consisted of warming up, mild strength training, and repetitive endurance exercise, followed by relaxation and feedback. Thirty patients were randomised either to an exercise group or to control treatment (warming up, sensory training, stretching, balance, coordination training and periods of relaxation—training involving the heart and circulation was avoided). There were no losses to follow-up, and all patients were considered for statistical analysis. The walking distance and walking time significantly improved in the control group when compared to control treatment.
Discussion
This study systematically reviewed RCTs regarding the efficacy of exercise therapy in restoring normal musculoskeletal function of MS patients. The interventions included were: aerobic training, breathing-enhanced upper extremity exercises, endurance exercises, exercise classes, PRT, upper and lower limb strengthening, and yoga. High quality studies showed that exercise therapy has a positive impact on Berg Balance scale, Dynamic Gait index scores, multidimensional fatigue inventory physical scale, right knee extension, right knee flexion and left knee flexion, SF-36 health survey, one-dimensional Fatigue Severity Scale, and General Fatigue of the Multidimensional Fatigue Inventory scores and on walking tests [10, 12–17, 19, 20]. Low quality studies showed that exercise therapy has a positive impact on the fatigue index for leg flexion in women and on the Modified Fatigue Impact Scale score [11, 18].
All the studies reviewed herein were published after the only systematic review of the effects of exercise therapy, alone, in MS patients [8]. Several recommendations for future research were issued in that review. Despite this, the shortcomings of the studies reviewed here are similar to those included in the previous review. Firstly, MS patients’ characteristics varied widely among the included studies. For example, the ages varied between 37.1 and 54.6 years, the duration of MS diagnosis varied, on average, between 5.2 and 15.9 years and the mean EDSS scores varied between 2.5 and 7.1. Furthermore, none of the RCTs stratified the patients according to MS characteristics. Therefore, the effects of exercise therapy in MS patients with different characteristics remain unclear. Secondly, the dose of the exercises varied widely among the RCTs (see Table 1). None of the studies investigated the effects of different doses of exercise therapy in MS patients. Therefore, it is still unclear whether different doses of exercise therapy have different effects in MS patients. Thirdly, although the vast majority of the studies scored high in the PEDro scale for assessing the quality of the methods (see Table 2), the authors carried out sample size calculations in only two studies. Therefore, as will be presented in detail below, the results of the RCTs may not be generalizable to all MS patients. Finally, different RCTs used different outcomes to measure the effects of similar interventions, making it not possible to pool the data.
Limitations
The first limitation of this review is that the results may not be generalizable to all MS patients. The majority of the reviewed studies included small sample sizes. Only two studies [14, 20] carried out sample size calculations. Consequently, the results of the studies may suffer from type II statistical errors (i.e. to conclude that an intervention has the same effects as no intervention, when this is in fact not true). For example, in the study by Surakka et al. [11], resistance training combined with aerobic training improved the Fatigue Index for leg flexion in women but not in men. No statistical power calculations were done in this study. Furthermore, the sample of men (n = 34) was much smaller than that of women (n = 61). Therefore, it is not possible to exclude that the first may have not been large enough for the effect to be detected.
The second limitation is that this review may suffer from reporting bias. Only articles indexed to PubMed were included in this review. Therefore, this literature review may have not been comprehensive enough to include all the RCTs on the effects of exercise therapy in MS patients. Despite this, PubMed is a major medical electronic database, indexing a great number of journals. Consequently, a considerable number of such RCTs is expected to have been included in this review.
Implications for practice
Despite all the limitations presented above, the results of this review suggest that exercise therapy may have a beneficial effect on patients with MS. Furthermore, no adverse events of such an intervention have been reported by most studies. Therefore, exercise therapy may be recommended for the rehabilitation of MS patients.
Implications for future research
For the reasons presented above, future RCTs about the effects of exercise therapy on MS patients should take measures to ensure the external validity of the studies. MS patients should be stratified according to disease characteristics, and the size of the study sample should be established using statistical power calculations. Consensus about the best outcomes to assess the effectiveness of exercise therapy is necessary. Studies about the effects of different doses of exercise therapy for MS patients are needed.
References
Alonso A, Hernán MA (2008) Temporal trends in the incidence of multiple sclerosis: a systematic review. Neurology 71(2):129–135
Murray TJ Diagnosis and treatment of multiple sclerosis. BMJ (Clin Res ed.) [Internet]. 2006 Mar 4 [cited 2013 Mar 20]; 332(7540):525–7. Available from: http://www.bmj.com/content/332/7540/525
Compston A, Coles A Multiple sclerosis. Lancet [Internet]. 2008 Oct 25 [cited 2012 Oct 26]; 372(9648):1502–17. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18970977
Confavreux C, Vukusic S (2006) Natural history of multiple sclerosis: a unifying concept. Brain: J Neurol 129(Pt 3):606–616
Mendes A, Sá MJ (2011) Classical immunomodulatory therapy in multiple sclerosis: how it acts, how it works. Arq Neuropsiquiatr 69(3):536–543
Sá MJ, Guimaraes J et al (2011) Etiopathogenesis, classical immunotherapy and innovative nanotherapeutics for inflammatory neurological disorders. Curr Nanosci 7(1):2–20
Multiple Sclerosis Therapy Consensus Group (MSTCG), Wiendl H, Toyka KV, Rieckmann P, Gold R, Hartung HP, Hohlfeld R (2008) Basic and escalating immunomodulatory treatments in multiple sclerosis: current therapeutic recommendations. J Neurol 255:1449–1463
Rietberg MB, Brooks D, Uitdehaag BM, Kwakkel G (2005) Exercise therapy for multiple sclerosis. Cochrane Database Syst Rev (1):CD003980
PEDro scale [Internet]. [cited 2013 Mar 20]; Available from: http://www.pedro.org.au/english/downloads/pedro-scale/
Dettmers C, Sulzmann M, Ruchay-Plossl A, Gutler R, Vieten M (2009) Endurance exercise improves walking distance in MS patients with fatigue. Acta Neurol Scand 120(4):251–257
Surakka J, Romberg A, Ruutiainen J, Aunola S, Virtanen A, Karppi SL et al (2004) Effects of aerobic and strength exercise on motor fatigue in men and women with multiple sclerosis: a randomized controlled trial. Clin Rehabil 18(7):737–746
Cattaneo D, Jonsdottir J, Zocchi M, Regola A (2007) Effects of balance exercises on people with multiple sclerosis: a pilot study. Clin Rehabil 21(9):771–781
Miller L, Paul L, Mattison P, McFadyen A (2011) Evaluation of a home-based physiotherapy programme for those with moderate to severe multiple sclerosis: a randomized controlled pilot study. Clin Rehabil 25(8):720–730
Romberg A, Virtanen A, Ruutiainen J (2005) Long-term exercise improves functional impairment but not quality of life in multiple sclerosis. J Neurol 252(7):839–845
Romberg A, Virtanen A, Ruutiainen J, Aunola S, Karppi S-L, Vaara M et al (2004) Effects of a 6-month exercise program on patients with multiple sclerosis: a randomized study. Neurology 63(11):2034–2038
Mutluay FK, Demir R, Ozyilmaz S, Caglar AT, Altintas A, Gurses HN (2007) Breathing-enhanced upper extremity exercises for patients with multiple sclerosis. Clin Rehabil 21(7):595–602
Dalgas U, Stenager E, Jakobsen J, Petersen T, Hansen HJ, Knudsen C et al (2010) Fatigue, mood and quality of life improve in MS patients after progressive resistance training. Mult Scler 16(4):480–490
McCullagh R, Fitzgerald AP, Murphy RP, Cooke G (2008) Long-term benefits of exercising on quality of life and fatigue in multiple sclerosis patients with mild disability: a pilot study. Clin Rehabil 22(3):206–214
Oken BS, Kishiyama S, Zajdel D, Bourdette D, Carlsen J, Haas M et al (2004) Randomized controlled trial of yoga and exercise in multiple sclerosis. Neurol 62(11):2058–2064
Dodd KJ, Taylor NF, Shields N, Prasad D, McDonald E, Gillon A (2011) Progressive resistance training did not improve walking but can improve muscle performance, quality of life and fatigue in adults with multiple sclerosis: a randomized controlled trial. Mult Scler 17(11):1362–1374
Poser CM, Paty DW, Scheinberg L, McDonald WI, Davis FA, Ebers GC et al (1983) New diagnostic criteria for multiple sclerosis: guidelines for research protocols. Annals Neurol 13(3):227–231
McDonald WI, Compston A, Edan G, Goodkin D, Hartung HP, Lublin FD et al (2001) Recommended diagnostic criteria for multiple sclerosis: guidelines from the international panel on the diagnosis of multiple sclerosis. Annals Neurol 50(1):121–127
Kraemer WJ, Adams K, Cafarelli E, Dudley GA, Dooly C, Feigenbaum MS et al (2002) American College of Sports Medicine position stand: progression models in resistance training for healthy adults. Med Sci Sports Exerc 34(2):364–380
JW (1995) Cardiopulmonary physical therapy: a clinical manual
Acknowledgments
The author wants to thank KeyPoint, Scientific Consultancy for the support in writing and submitting the manuscript.
Conflicts of interest
The author declares that she does not have any conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sá, M.J. Exercise therapy and multiple sclerosis: a systematic review. J Neurol 261, 1651–1661 (2014). https://doi.org/10.1007/s00415-013-7183-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-013-7183-9