
Abstract
Demyelination in multiple sclerosis (MS) may cause damage to the vegetative nervous system. Our objective was to examine cerebral autoregulation assessed via blood pressure and cerebral blood flow velocity fluctuations during head-up tilt table testing. We also investigated the effects of high-dose intravenous corticosteroid treatment. Transcranial Doppler registration of middle cerebral artery blood flow velocity and continuous blood pressure and heart rate monitoring were performed at rest and during tilt table testing in 30 MS patients. Ten age-matched healthy subjects were also examined as controls. Correlations between mean arterial blood pressure (MBP) and cerebral blood flow velocity (CBF) fluctuations were averaged, yielding the correlation coefficient index Mx. For a subgroup of 11 patients with acute exacerbations, results were also evaluated before and after methylprednisolone treatment (1 g/day intravenously for 5 days). No significant differences in the autoregulatory indices were seen between patients and controls, or between pre- and post-steroid results. Modeling CBF velocity changes associated with a 1-mmHg increase in MBP, significant differences (p < 0.05) were detected in patients vs. controls, and also after vs. before steroid administration. We conclude that cerebrovascular autoregulation impairments are detectable in early phase MS. Corticosteroid treatment has a significant effect on hemodynamic changes in acute exacerbations.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Multiple sclerosis (MS) is a chronic inflammatory, demyelinating and degenerative disease of the central nervous system, usually characterized clinically by relapses, remissions, and progression of disability over time. Acute attacks of demyelination typically occur at irregular intervals, often resulting in increasing motor disability, visual or sensory loss. There is also evidence of autonomic dysfunction involving the cardiovascular regulation system in MS patients, but this is often subclinical [1–8]. Cerebral vessels are richly innervated by both sympathetic and parasympathetic nerves, and MS may secondarily affect cerebral autoregulation [9]. By definition, cerebrovascular autoregulation is the intrinsic ability of the brain to maintain a constant cerebral blood flow during changes of cerebral perfusion pressure (CPP) [10, 11]. Cerebral autoregulation testing implies a hemodynamic stimulus, such as pharmacon-induced arterial pressure elevation, thigh cuff release, or tilt table declination [10]. Transcranial Doppler (TCD) is a non-invasive method for the assessment of changes in cerebral blood flow (CBF) velocity. Autoregulation monitoring relies on the observation of spontaneous responses of CBF to spontaneous fluctuations in CPP or mean arterial blood pressure (MBP). Thus, continuous blood pressure measurement coupled with TCD-based CBF velocity detection in the middle cerebral arteries (MCAs) allows us to evaluate cerebral autoregulation.
High-dose corticosteroid therapy is the standard regimen for the treatment of acute relapses and optic neuritis; the effect is on inflammation rather than re-myelination and repair of axonal injury [12–15]. A great diversity of mechanisms are potentially involved in the modulation of neuroinflammation by glucocorticoids including: inhibition of pro-inflammatory cytokine production (interferon gamma), upregulation of anti-inflammatory cytokines (interleukin-10), down-regulation of the expression of cell adhesion molecules (very late antigen-4) and chemokine receptors (CXCR3), the induction of T cell apoptosis, inhibition of nitric oxide production and restoring of the blood–brain barrier through down-regulating matrix metalloproteinases, consequently leading to local changes in cerebral blood flow. It is not well understood which mechanisms are essential for therapeutic efficacy [16]. Clinical improvement can be assessed by the expanded disability status scale (EDSS). In addition to their acute effects, steroids are known not to affect patients’ long-term disability outlooks.
This study’s objective was the TCD-based assessment of cerebrovascular autoregulation in the early phase of the disease, whether dysregulation can be detected in patients without significant clinical disability compared to healthy controls. In cases of acute inflammation, i.e., the subgroup of patients with exacerbations, the effect of high-dose anti-inflammatory methylprednisolone (MP) treatment on cerebral hemodynamic changes was also evaluated.
Patients and methods
Thirty patients were enrolled from our neuroimmunology clinic (23 women, seven men; mean age [SD]: 35.1 [9.6] years; duration of the disease: 5.9 [6.8] years). Patients were diagnosed as having relapsing-remitting (RR) (n = 20), primary-progressive (PP) (n = 3) MS according to revised McDonald criteria [17], or clinically isolated syndrome (CIS) (n = 7). Subjects with severe disability (unable to stand and walk without help) were not included. All patients underwent detailed neurological examination performed by the same neurologist. None of the subjects had any other diseases that could have affected cerebrovascular autoregulation (e.g., diabetes mellitus, stroke, thyroid dysfunction). Examinations were also done in ten age- and gender-matched healthy persons as a control group (eight women, two men; mean age [SD]: 34.2 [6.8]). Eleven patients (nine RR-MS, two CIS) had acute exacerbations and received 1,000 mg of methylprednisolone intravenously (iv.) for five consecutive days. These subjects were examined before and after the high-dose methylprednisolone treatment (mean time interval: 6 [1.3] days). Exacerbation was defined as a rapid, progressive worsening of symptoms or development of a new neurological deficit lasting more than 24 h. All subjects signed a written informed consent prior to the investigation. The trial protocol was approved by the local Ethical Committee of University of Debrecen Medical and Health Science Center.
Tilt table tests
Each subject was examined in the morning after overnight fasting. Caffeine-containing products, alcohol, or medications were avoided. Real-time registration of blood flow velocity in both middle cerebral arteries by transcranial Doppler (Multidop ×4, DWL Compumedics Germany GmbH), and non-invasive beat-to-beat blood pressure and heart rate monitoring (CNSystems Task Force monitor 3040i) were continued for 10 min in the supine position for 30 min in a tilted-up position at a 70° angle on the tilt table, and for a final 5 min after tilting back to the supine position. MCA blood flow velocities were recorded at a depth of 50–60 mm through the temporal bone window using 2-MHz TCD probes.
Statistical analysis
The method used for assessment of dynamic cerebral autoregulation has been described previously [10, 11]. Mean values of arterial blood pressure (MBP) and cerebral blood flow velocity were averaged over 3-s intervals. From a consecutive 20 such values, Pearson correlation coefficients between MBP and CBF velocity were calculated for each subject and each minute of a 10-min period. The resulting sets of 1-min correlation coefficients were then averaged for each subject, yielding the autoregulatory index Mx, reflecting the correlation between MBP and mean CBF velocity. Slopes of the rise in heart rate after tilting up were also examined. Changes in CBF velocity associated with a 1-mmHg increase in MBP after the provocation were estimated using multilevel mixed effects linear regression. The analysis encompassed both immediate and delayed changes in CBF, ranging from 0 to 12 s of lag after the provocation. Lag-by-lag and rolling-summed lag effects were evaluated (lag-by-lag effects refer to the additive change in blood flow velocity in reference to the previous second, specifically for each lag-second; rolling-summed lag effects refer to cumulative changes from the moment of MBP increase up to the given lag-second). For unadjusted between-group comparisons, Student’s two-sample t test, Wilcoxon rank-sum test, and the Kruskal–Wallis test were used, subject to number of groups compared and distributional assumptions. Unadjusted within-group before–after comparisons were made using Student’s paired t test or Wilcoxon matched-pairs signed-ranks test, subject to distributional assumptions. Values of p < 0.05 were considered to indicate statistical significance.
Results
Clinical characteristics of the patient and control groups are summarized in Table 1. Patients’ mean age was 35 years, with <6 years of disease history on average. None of the patients had significant clinical disability. The mean score was 2.6 [1.24] on the Expanded Disability Status Scale (EDSS) and 0.054 [0.5] on the Multiple Sclerosis Functional Composite (MSFC) instrument. Fourteen patients were on immunomodulatory treatment (interferon-beta or glatiramer-acetate) and one patient received plasmapheresis after the examination because of a severe relapse. None of the subjects had any other concomitant disease that could have affected cerebrovascular autoregulation (e.g., diabetes mellitus, stroke, thyroid dysfunction). The conventional MRI examination showed more than nine supratentorial lesions in 25 patients, at least one brainstem lesion in 21 cases, and spinal cord lesions in 13 cases on T2-weighted images. Table 2 presents p values for differences comparing patients and controls in terms of Mx index before, during, and after provocation by tilting. The Mx index for the correlation between MBP and CBF velocity changes was calculated for the left and right sides separately, and also bilaterally. All results were compared to their counterparts obtained from the control group. Calculations were also carried out stratified for disease subtype. No significant differences were seen in unilateral or bilateral Mx indices between patients and controls before or after provocation by tilting (Table 2). Similar non-significant Mx index differences were found when comparing patients of various MS subtypes to healthy subjects. No correlation was found between Mx values and EDSS or MSFC results.
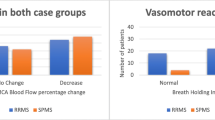
Eleven patients suffering from acute exacerbation (nine RR-MS, two CIS) were examined before and after intravenous corticosteroid treatment. Clinical improvement was assessed via EDSS and MSFC. The mean [SD] EDSS was 3.59 [0.8] before the treatment and decreased to 3.32 [0.93] (p = 0.084), while MSFC changed from −0.22 [0.46] to –0.02 [0.57] (p = 0.024) during the treatment period. The administration of high-dose methylprednisolone did not cause significant changes in the Mx indices (Table 2).
Though these analyses did not detect any significant differences between MS patients and controls, Fig. 1 shows that a more prominent increase in heart rate and a greater decrease in CBF velocity were observed in patients than in controls after head-up tilting (Fig. 1). Curves were similarly different after vs. before steroid administration (Fig. 2), suggesting a tendency of normalization for these parameters. The slope of the upsurge section of the heart rate curve was not significantly steeper in the patient group. However, the slope of tilt-induced heart rate elevation was significantly lower after steroid treatment within the first 8-s time-window after the stimulus (p = 0.010); the difference gradually diminished upon extending the slope calculation time-window to 14 s where it became of borderline significance (p = 0.05).

Trends in heart rate and in cerebral blood flow during the test in the patient and control groups. A prominent increase in heart rate and a greater decrease in CBF velocity were observed in the patient group after tilting up (HR heart rate, CBF cerebral blood flow velocity)

Trends in heart rate and in cerebral blood flow during the test before and after steroid treatment. Increased CBF velocity and reduction in the extent of heart rate elevation were observed after steroid administration (HR heart rate, CBF cerebral blood flow velocity)
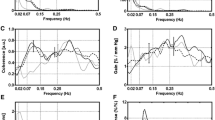
Finally, changes in CBF velocity associated with a 1-mmHg increase in MBP were modeled. Upon an MBP increase of 1 mmHg, CBF velocity also becomes higher by about 0.5 cm/s within the same second (lag = 0), followed by quick counter-regulation that produces an overshoot, but eventually CBF velocity returns to the base level. The flow increase after MBP elevation is lower in patients, but the subsequent compensation is more prominent; these differences are statistically significant (p < 0.05) (Fig. 3). The differences were also significant when comparing MBP-related CBF velocity changes after steroid administration with the pre-treatment reference (Fig. 4).

Temporal sequence of the changes in CBF velocity associated with a 1-mmHg increase in MBP in the patient and control groups. The immediate flow elevation upon a unit increase in MBP is significantly lower in patients: the subsequent compensation is more prominent (95 % confidence intervals not including the reference line indicate p < 0.05, multilevel mixed effects linear regression). (MBP mean arterial blood pressure, CBF cerebral blood flow velocity, lag-by-lag effects: additive changes in blood flow velocity in reference to the previous second, rolling-summed lag effects: cumulative changes from the moment of MBP increase up to the given lag-second)

Temporal sequence of the changes in CBF velocity associated with a 1-mmHg increase in MBP before and after high-dose methylprednisolone treatment. The immediate flow increase after MBP elevation is lower after the treatment, followed by significantly more prominent compensation compared to the pre-treatment result (95 % confidence intervals not including the reference line indicate p < 0.05, multilevel mixed-effects linear regression). (MBP mean arterial blood pressure, CBF cerebral blood flow velocity, lag-by-lag effects: additive changes in blood flow velocity in reference to the previous second, rolling-summed lag effects: cumulative changes from the moment of MBP increase up to the given lag-second)
Discussion
Dynamic cerebral autoregulation (dCA), the acute response of cerebral perfusion to changes in MBP, is a sensitive indicator in the detection of cerebral hemodynamic impairment. There are no clear standards for measurement and analysis of dCA [18, 19]. The method used in this study was previously applied in patients with head injury and stroke [10, 11, 20]. The general assumption is that the predominant sources of CBF velocity fluctuations over a short period of time are fluctuations of CPP or MBP. By continuous monitoring of consecutive time-averaged samples, a correlation coefficient between MBP and mean CBF velocity is calculated. Evaluating the autoregulatory Mx index, our study did not show a significant disturbance of dynamic cerebral autoregulation in MS patients, and produced similar correlation estimates between MBP and CBF velocity in healthy persons and MS patients. Beside dCA we also evaluated the dynamic rise in heart rate after provocation, but no significant difference was found in MS patients compared to the control group. It is known from the literature that a sudden drop in MBP evokes a response characterized by decreased cerebral flow for a few seconds, followed by a relatively slow return to the base level [18, 19]. In our investigation into the changes in CBF velocity associated with a 1-mmHg increase in MBP, we observed an immediate elevation in blood flow velocity, but 2 s later, counter-regulation set in, causing an overshoot of the flow velocity to below the base level. Another counter-regulation occurred in the next second, and the flow velocity gradually reached the base level after 5 s. Along the course of the regulation process, significant differences were detected between MS patients and the healthy group.
Impaired cardiovascular regulation can be an important manifestation of autonomic dysfunction in MS patients. Some studies reported decreased heart beat variability, others described orthostatic tachycardia and dysregulation of blood pressure and cerebral blood flow during tilt table testing [2, 8, 21–27]. The pathophysiology behind these symptoms is not fully clarified. Demyelinated plaques may cause disruption to reflex pathways in crucial areas including the brainstem, spinal cord, hypothalamus, limbic system, and frontal cortex [2, 5, 8, 22, 24]. In our study, 25 out of 30 patients had multiple supratentorial lesions by conventional MRI, 70 % had brainstem, and 43 % had spinal cord location without hypothalamic or gray matter involvement. In fact, multiple sclerosis is not only a focal, inflammatory demyelinating disease. It is a diffuse central nervous system disease with an important neurodegenerative component, which occurs very early in the course of disease and the correlation between MRI measures of inflammation and neurodegeneration is weak in all disease phases [28]. It is not surprising that the inclusion of the MRI findings as adjustment factors or stratification variables did not affect the analysis results to any meaningful extent. According to the literature, if orthostatic dysregulation occurs, it never comes as the first manifestation or as an episodic feature of multiple sclerosis: it is characteristic of the late stage of the disease [3]. Longer disease duration leads to progressive impairment of cardiac autonomic balance in MS patients [6, 23, 25]. However, Flachenecker [1] reported the presence of abnormal heart rate response to orthostatic challenge in CIS patients.
Saari et al. [8] examined cardiovascular autonomic control in 51 clinically definite MS patients and found that the results were correlated with the lesion load on MRI scans of the brain. Patients had relapsing-remitting or secondary progressive MS with a mean EDSS of 4.3. The study’s findings included reduced heart rate variation in deep breathing, and decreased heart rate and blood pressure response in tilt table testing. In particular, midbrain lesions on the MRI scans were associated with cardiovascular dysfunction.
Although these manifestations of autonomic dysfunction are seldom recognized in patients with MS, they may cause serious complications. Recently, Hengstman and Kusters [29] published a case when a patient with active RR-MS died unexpectedly due to a sudden onset of cardiac arrhythmias and post-mortem examination showed the presence of active demyelinating lesions in the medulla oblongata.
Gonul et al. [9] examined cerebrovascular autoregulation in 20 RR-MS patients by transcranial Doppler during head-up tilt. The mean CBF velocity was found to be significantly reduced in comparison with the baseline values in patients and controls after tilting up. They detected a greater blood flow velocity decrease in patients than in controls. Changes in CBF velocity were more prominent in the subgroup of patients with EDSS ≥ 2. No statistically significant difference was found for change in mean blood pressure and heart rate. Furthermore, there was no evidence for a relationship between the lesion locations on MRI and the changes of CBF velocity values during head-up tilt in patients with MS.
High-dose intravenous methylprednisolone is the most common therapeutic modality to treat acute exacerbations in MS. Glucocorticoids have beneficial effects on neuroinflammation as they induce or repress the expression of secreted molecules and surface receptors on leukocytes, endothelial cells of the blood–brain barrier, and also cause T cell apoptosis [13–15]. Özkan et al. [30] observed a significant decrease in CBF velocity with a non-significant increase in vascular reactivity after 5 days of 1,000 mg iv. methylprednisolone treatment in 48 MS patients. They supposed that inflammation can cause an increase in blood flow velocity due to increased perfusion. Steroid treatment of the acute attack caused clinical improvement assessed by EDSS and decreased perfusion measured by blood flow velocity. Conversely, i.v. MP may cause cardiovascular abnormality as a side effect: Vasheghani-Farahani et al. [31] detected cardiac arrhythmias in MS patients receiving high-dose steroids. This effect could be mediated by direct action on the myocardial cell membrane, or via alterations in cardiovascular sensitivity to catecholamines. Corticosteroids also have a mineralocorticoid function resulting in the retention of sodium and intracellular fluids, causing high blood pressure and congestive heart failure.
In this study, the effect of high-dose i.v. MP on dynamic cerebral autoregulation was also investigated in a subgroup of patients having acute exacerbations, but only a non-significant difference in Mx indices was detected after steroid treatment compared to the pre-steroid results. However, the slope of tilt-induced heart rate elevation was significantly lower after steroid administration within the first 14-s time-window after the stimulus. Looking at a 1-mmHg MBP increase, the effect detected in CBF velocity changes was significantly different after the treatment than before. The difference could be explained by the local changes in blood flow as a major consequence of inflammation. Substances presumably released during brain inflammation in multiple sclerosis, such as nitric oxide and substance P, are classical vasodilators [32]. According to perfusion MRI studies, endothelial cell dysfunction occurs very early during the inflammatory cascade, and acute plaques are associated with an increase in both CBF and cerebral blood volume. This hyperperfusion precedes overt changes in blood–brain barrier permeability [32, 33]. We confirmed that steroid treatment of the acute attack caused clinical improvements assessed by EDSS and MSFC, and reduced inflammation results in significant hemodynamic changes compared to the pre-treatment results. The phenomenon of the change in CBF velocity upon MBP elevation becoming more prominent could be explained, on one hand, by altered neuronal activity and local metabolic changes secondary to diminished inflammation and improvement in endothelial cell function; on the other hand, the explanation may lie in corticosteroids having mineralocorticoid-like effects on vascular reactivity. This way, the rapid action can mediate vasodilatation through an endothelium-dependent mechanism, and/or vasoconstriction via a direct smooth muscle effect. A shift in this balance from endothelial to vascular smooth muscle mediated effects may also be important in vascular dysregulation [34].
We are aware of the fact that this study is not without limitations. The small number of subjects and heterogeneity of MS in the patient group are fundamental limitations. It is important to emphasize that only CBF velocity was measured by TCD, which only reflects changes in CBF if the MCA’s diameter remains constant [35]. As previously mentioned, standards for measurement and analysis of dCA are lacking [18, 19].
In conclusion, beside these limitations, we successfully demonstrated that hemodynamic changes are present in early MS compared to healthy controls after a hemodynamic stimulus such as tilt table declination. Significant effects of high-dose corticosteroid treatment were detected; however, further studies are needed to clarify the relationship between hemodynamic changes and clinical symptoms.
References
Flachenecker P (2007) Autonomic dysfunction in Guillain-Barré syndrome and multiple sclerosis. J Neurol 254(Suppl 2):1196–11101
Haensch CA, Jörg J (2006) Autonomic dysfunction in multiple sclerosis. J Neurol 253(Suppl 1):13–19
Lensch E, Jost WH (2011) Autonomic disorders in multiple sclerosis. Autoimmune Dis 803841 Epub. 2011 Apr 17
Linden D, Diehl RR, Berlit P (1995) Subclinical autonomic disturbances in multiple sclerosis. J Neurol 242:374–378
Lorberboym M, Lamlp Y, Nikolov G, Sadeh M, Gilad R (2008) I-123 MIBG cardiac scintigraphy and autonomic test evaluation in multiple sclerosis patients. J Neurol 255:211–216
Kodounis A, Stamboulis E, Constantinidis TS, Liolios A (2005) Measurement of autonomic dysregulation in multiple sclerosis. Acta Neurol Scand 112:403–408
Merkelbach S, Haensch CA, Hemmer B, Koehler J, König NH, Ziemssen T (2006) Multiple sclerosis and the autonomic nervous system. J Neurol 253(Suppl 1):121–125
Saari A, Tolonen U, Paakkö E, Suominen K, Pyhtinen J, Sotaniemi K et al (2004) Cardiovascular autonomic dysfunction correlates with brain MRI lesion load in MS. Clin Neurophysiol 115:1473–1478
Gonul M, Asil T, Balci K, Celik Y, Turgut N, Uzunca I (2008) Changing cerebral blood flow velocity detected by transcranial Doppler ultrasound during head up tilt in patients with multiple sclerosis. Eur J Neurol 15:725–729
Czosnyka M, Brady K, Reinhard M, Smielewski P, Steiner LA (2009) Monitoring of cerebrovascular autoregulation: facts, myths, and missing links. Neurocrit Care 10:373–386
Reinhard M, Roth M, Guschlbauer B, Harloff A, Timmer J, Czosnyka M et al (2005) Dynamic cerebral autoregulation in acute ischemic stroke assessed from spontaneous blood pressure fluctuations. Stroke 36:1684–1689
Noseworthy JH, Lucchinetti C, Rodriguez M, Weinshenker BG (2000) Multiple sclerosis. N Eng J Med 343:938–952
Pozzilli C, Marinelli F, Romano S, Bagnato F (2004) Corticosteroids treatment. J Neurol Sci 223:47–51
Sloka JS, Stefanelli M (2005) The mechanism of action of methylprednisolone in the treatment of multiple sclerosis. Mult Scler 11:425–432
Tischner D, Reichardt HM (2007) Glucocorticoids in the control of neuroinflammation. Mol Cell Endocrinol 275:62–70
Schweingruber N, Reichardt SD, Lühder F, Reichardt HM (2012) Mechanisms of glucocorticoids in the control of neuroinflammation. J Neuroendocrinol 24:174–182
Polman CH, Reingold SC, Edan G, Filippi M, Hartung HP, Kappos L et al (2005) Diagnostic criteria for multiple sclerosis: 2005 revisions to the “McDonald Criteria”. Ann Neurol 58:840–846
Gommer ED, Shijaku E, Mess WH, Reulen JPH (2010) Dynamic cerebral autoregulation: different signal processing methods without influence on results and reproducibility. Med Biol Eng Comput 48:1243–1250
Secher NH, van Lieshout JJ (2010) Dynamic cerebral autoregulation and monitoring cerebral perfusion. Hypertension 56:189–190
Schramm P, Klein KU, Pape M, Berres M, Werner C, Kochs E et al (2011) Serial measurement of static and dynamic cerebrovascular autoregulation after brain injury. J Neurosurg Anesthesiol 23:41–44
Flachenecker P, Wolf A, Krauser M, Hartung HP, Reiners K (1999) Cardiovascular autonomic dysfunction in multiple sclerosis: correlation with orthostatic intolerance. J Neurol 246:578–586
Kanjwal K, Karabin B, Kanjwal Y, Grubb BP (2010) Autonomic dysfunction presenting as postural orthostatic tachycardia syndrome in patients with multiple sclerosis. Int J Med Sci 7:62–67
Mahovic D, Lakusic N (2007) Progressive impairment of autonomic control of heart rate in patients with multiple sclerosis. Arch Med Res 38:322–325
McDougall AJ, McLoad JG (2003) Autonomic nervous system function in multiple sclerosis. J Neurol Sci 215:79–85
Nasseri K, TenVoorde BJ, Ader HJ, Uitdehaag BMJ, Polman CH (1998) Longitudinal follow-up of cardiovascular reflex tests in multiple sclerosis. J Neurol Sci 155:50–54
Sanya EO, Tutaj M, Brown CM, Goel N, Neundörfer B, Hilz MJ (2005) Abnormal heart rate and blood pressure responses to baroreflex stimulation in multiple sclerosis patients. Clin Auton Res 15:213–218
de Seze J, Stojkovic T, Gauvrit JY, Devos D, Ayachi M, Cassim F et al (2001) Autonomic dysfunction in multiple sclerosis: cervical spinal cord atrophy correlates. J Neurol 248:297–303
Filippi M, Rocca MA (2005) MRI evidence for multiple sclerosis as a diffuse disease of the central nervous system. J Neurol 252(Suppl 5):v16–v24
Hengstman GJ, Kusters B (2011) Sudden cardiac death in multiple sclerosis caused by active demyelination of the medulla oblongata. Mult Scler 17:1146–1148
Özkan S, Uzuner N, Kutlu C, Özbabalik D, Özdemir G (2006) The effect of methylprednisolone treatment on cerebral reactivity in patients with multiple sclerosis. J Clin Neurosci 13:214–217
Vasheghani-Farahani A, Sahraian MA, Darabi L, Aghsaie A, Minagar A (2011) Incidence of various cardiac arrhythmias and conduction disturbances due to high dose intravenous methylprednisolone in patients with multiple sclerosis. J Neurol Sci 309:75–78
Wuerfel J, Bellman-Strobl J, Brunecker P, Aktas O, McFarland H, Villringer A et al (2004) Changes in cerebral perfusion precede plaque formation in multiple sclerosis: a longitudinal perfusion MRI study. Brain 127:111–119
Wuerfel J, Paul F, Zipp F (2007) Cerebral blood perfusion changes in multiple sclerosis. J Neurol Sci 259:16–20
Feldman RD, Gros R (2010) Rapid vascular effects of steroids—a question of balance? Can J Cardiol 26(Suppl A):22A–26A
Zhang R, Zuckerman JH, Iwasaki K, Wilson TE, Crandall CG, Levine BD (2002) Autonomic neural control of dynamic cerebral autoregulation in humans. Circulation 106:1814–1820
Conflicts of interest
The authors declare that they have no conflict of interest.
Ethical standard
The study received approval from the local Ethical Committee of the University of Debrecen Medical and Health Science Center and adhered to the ethical guidelines of the most recent Helsinki Declaration (Edinburgh, 2000). After receiving information about the purpose of the study, all patient signed a consent form before the ultrasound examination.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mezei, Z., Olah, L., Kardos, L. et al. Cerebrovascular hemodynamic changes in multiple sclerosis patients during head-up tilt table test: effect of high-dose intravenous steroid treatment. J Neurol 260, 2335–2342 (2013). https://doi.org/10.1007/s00415-013-6977-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-013-6977-0