
Abstract
X-linked adrenoleukodystrophy (XALD), a neurological disorder caused by mutations in the peroxisomal membrane protein gene ABCD1, presents as a rapidly progressing, inflammatory cerebral demyelination (cerebral cases) or a slowly progressing, distal axonopathy (non-cerebral cases). Specific ABCD1 defects do not explain this significant phenotypic variation. Patients have increased plasma and tissue very long chain fatty acid levels and increased cellular oxidative stress and oxidative damage. Superoxide dismutase 2 (SOD2), at candidate modifier locus 6q25.3, detoxifies superoxide radicals protecting against oxidative stress and damage. We tested an SOD2 variant C47T (Ala16Val) associated with reduced enzymatic activity as a potential modifier gene of cerebral demyelinating disease by comparing 117 cerebral XALD cases with 105 non-cerebral XALD cases. The hypoactive valine allele of the variant was associated with cerebral disease under a dominant model in the full data set (p = 0.04; ORT* = 1.90, 95% CI 1.01–3.56) and the non-childhood cerebral disease subset (p = 0.03; ORT* = 2.47, 95% CI 1.08–5.61). Three tag SNPs were genotyped to test for additional SNP or haplotype associations. A common haplotype, GTAC, which included the SOD2 valine allele, was associated with cerebral disease in the full data set (p = 0.03; OR = 1.75, 95% CI 1.11–2.75) and the non-childhood cerebral disease subset (p = 0.008; OR = 2.20, 95% CI 1.27–3.83). There was no association between childhood cerebral XALD and the C47T variant or the GTAC haplotype. Thus, reduced SOD2 activity may contribute to the development of cerebral demyelination in adolescent and adult XALD patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
X-linked adrenoleukodystrophy (XALD) is a neurodegenerative disorder caused by mutations in the peroxisomal membrane protein gene ABCD1 that affects 1:17,000 males [1]. The biochemical hallmark of the disease is an increase in very long chain fatty acid (VLCFA) levels in patient tissues and plasma. All patients carry mutations in the same gene; however, there is wide variability in the clinical presentation of the disease including age of onset, rate of progression, severity of disease, and the initial site of pathology. There are seven main phenotypes (Table 1) [2, 3]. Seventy percent of all patients are adrenal insufficient. The two most common neurological presentations of the disease are an early onset (<10 years), rapidly progressing, inflammatory cerebral demyelination known as childhood cerebral XALD (CCALD) or a later onset (mean age 28 years), slowly progressing, non-inflammatory axonopathy of the spinal cord termed adrenomyeloneuropathy (AMN) [1, 4]. Other less common presentations include adolescent cerebral XALD, adult cerebral XALD, AMN with cerebral involvement, Addison-only phenotype, and asymptomatic. There is no correlation between plasma VLCFA levels and clinical severity of the disease or between the ABCD1 genotype and XALD phenotype [3, 4].
Different phenotypes, including CCALD and AMN, commonly occur within the same family, among individuals with identical ABCD1 genotypes, including patients with the complete absence of ABCD1 protein expression, and among a few monozygous twin pairs [5]. Mice lacking Abcd1 expression exhibit an AMN-like phenotype, axonal degeneration, and mitochondrial deficits, but do not develop cerebral inflammatory disease suggesting that mutations within ABCD1 cause AMN [6]. Therefore, genetic, epigenetic, environmental, and/or stochastic factors may contribute to the phenotypic heterogeneity of XALD [5]. ABCD2, ABCD3, and ABCD4, genes related to ABCD1 by sequence similarity, are not genetic modifiers of XALD [5, 7]. An insertion in the methionine metabolism gene cystathionine-beta-synthase (CBS c.844_845ins68) has been associated with protection against cerebral demyelination [8]. Variants within two other methionine metabolism genes methyltetrahydrofolate-homocysteine-S-methyltransferase (MTR c.2756A>G) and transcobalamin 2 (Tc2 c.776C>G) are associated with cerebral demyelination in AMN patients [9]. Our previous analysis of the CCALD and AMN phenotypes favored a genetic model of a cerebral disease modifier with a dominant allele frequency of 0.44 [4]. Linkage analysis identified the potential modifier loci as 1q31.1–41, 5p15.32, and 6q25.2–25.3.
Manganese superoxide dismutase (SOD2), a mitochondrial enzyme responsible for detoxifying superoxide radicals, is located within the candidate modifier locus 6q25.3 and is a candidate modifier gene based on function [10]. It is the only inducible superoxide dismutase and the mainline of defense against reactive oxygen species in the mitochondria. Free radical damage is an important contributor to various neurological diseases including XALD [11]. XALD patients exhibit mitochondrial damage, increased oxidative stress and damage, increased lipid peroxidation, and decreased antioxidant activity [6, 12, 13]. The addition of excess hexacosanoic acid (C26:0), a VLCFA, to XALD fibroblasts increased oxidative stress and damage and specifically increased SOD2 protein expression [14]. There was not a concomitant increase in the expression of other antioxidants including catalase, SOD1, or glutathione peroxidase 1. Therefore, in the brain, a tissue with lower antioxidant capacity, SOD2 may also play a key role in handling the increased oxidative stress levels due to ABCD1 defects.
It is clear that mutations in ABCD1 somehow disrupt peroxisomal function. Singh and Pujol propose a three-hit model of pathogenesis leading to cerebral demyelination: the loss of ABCD1 function and excess VLCFAs lead to oxidative stress and damage that along with genetic, epigenetic, stochastic, or environmental modifiers generate inflammatory cerebral disease which causes a further loss of peroxisomal functions [15]. The lack of cerebral oxidative damage and cerebral disease in Abcd1 −/Y mice despite elevated VLCFA levels further supports a role for oxidative stress and damage in the development of cerebral demyelination in XALD patients [6]. Therefore, genetic variants that result in reduced activity of oxidative stress mediators such as SOD2 may explain the development of cerebral disease and the varying severity of human XALD phenotypes.
Studies in mice suggest that reduced SOD2 activity can contribute to demyelination. SOD2 −/− mice exhibit varying phenotypes depending on the genetic background of the mouse. Some SOD2 −/− mice exhibit oxidative damage, neural degeneration, and a pronounced movement disorder as a result of mitochondrial oxidative stress [16–18]. SOD2 −/− mice in a B6D2F1 mouse background have evidence of demyelination and hypomyelination and enlarged and degenerating mitochondria in neurons and axons, characteristics reminiscent of XALD [18]. In addition, ribozyme reduction of SOD2 levels in the mouse eye leads to a loss of axons and myelin [19]. Conversely, increased SOD2 expression suppressed myelin fiber injury in the optic nerves of mice induced with experimental autoimmune encephalomyelitis [20].
SOD2 enzymatic activity varies by 56-fold in healthy individuals [21]. Therefore, differences in SOD2 activity could account for the spectrum of XALD phenotypes. In particular, a common polymorphism C47T (dbSNP: rs4880) within the mitochondrial targeting sequence of SOD2 causes an Ala16Val change (valine allele; frequency 0.53) that disrupts the alpha helical structure of SOD2 causing the protein to be retained in the inner mitochondrial membrane. The valine allele has 30–40% less enzymatic activity and reduces the capacity for cells to handle oxidative stress [22–24]. This variant has been associated with nonfamilial idiopathic cardiomyopathy [25], hereditary hemochromatosis [23], and diabetic neuropathy in type 1 and 2 diabetes patients [26, 27]. The alanine allele has been associated with protection from diabetic retinopathy which involves a loss of myelinated retinal nerve fibers [28]. Following Singh and Pujol’s model of XALD pathogenesis [15], we hypothesized that the reduced activity of the valine allele may contribute to the development of cerebral disease and demyelination in XALD patients by reducing the capacity of the brain to handle oxidative stress thus increasing oxidative damage. The high frequency of this variant could account for the frequent intrafamilial variability in XALD phenotypes.
We performed a case–control study between Caucasian XALD patients exhibiting cerebral demyelinating disease (cases) and those without cerebral disease (controls) and found an association between the C47T variant (Ala16Val) of SOD2 and the development of XALD cerebral disease. Since the C47T variant does not account for all of the variation in SOD2 activity, we hypothesized that other variants might capture additional variation. We genotyped three additional single nucleotide polymorphisms (SNPs) rs2758352, rs2842980, and rs2758329, and tested for allele or haplotype associations with cerebral disease.
Materials and methods
Study population
Genomic DNA from lymphoblasts was obtained from 222 unrelated Caucasian male XALD patients recruited by the Kennedy Krieger Institute, Baltimore, MD. All participants and/or their guardians provided written informed consent. The study was approved by the appropriate ethics committee.
SNP selection and genotyping
Using the Hapmap Data Release 24/phase II November 2008 and the Tag SNP Picker option (CEU population, r 2 ≤ 0.8 and minor allele frequency ≥0.2) three tag SNPs in addition to rs4880 were chosen across the SOD2 gene region (chromosome 6:160,018,100–160,043,551 bp). Genotyping was performed by amplification of 5 ng of genomic DNA. All four SNPs were genotyped with Taqman technology (Applied Biosystems, Foster City, CA). PCRs were performed on a Bio-Rad iCycler thermal cycler, endpoint fluorescence reads were performed using an ABI PRISM 7900HT (Applied Biosystems), and genotype calling was performed using SDS 2.1 allelic discrimination software (Applied Biosystems). Total genotyping rate 0.985. Haploview 4.2 was used to calculate r 2 values [29].
Statistical analyses
All analyses were conducted using PLINK [30]. All SNPs were in Hardy–Weinberg equilibrium. Single-locus association was tested under four genetic models: allelic (allele 1 vs. allele 2), genotypic (genotype 11 vs. 12 vs. 22), dominant (genotypes 11 and 12 vs. 22), and recessive (genotype 22 vs. 11 and 12) tests. Haplotype-based association tests were performed for haplotypes with a frequency greater than 0.03; and p values were corrected for testing multiple haplotypes using the Bonferroni method. Differences in haplotype frequencies between cases and controls were tested using a likelihood ratio test. Any result with p ≤ 0.05 was considered significant. The genotype and haplotype associations are expressed as an odds ratio (OR) with a 95% confidence interval. All analyses were conducted with the full data set and a subset of cases excluding CCALD patients.
Results
The phenotype distribution of Caucasian male XALD patients included in this study is given in Table 1. A total of 117 patients with CCALD, adolescent cerebral XALD, adult cerebral XALD, or AMN cerebral disease were classified as cases. One hundred five controls consisted of patients diagnosed as AMN without cerebral involvement, Addison-only phenotype, or asymptomatic. XALD is a progressive disease so there may be some phenotypic ambiguity among non-cerebral patients. Association analyses were performed with the total population (n = 222) and with a subset that excluded CCALD patients from the analysis (n = 168). We have speculated that CCALD may be a brain-specific immune response to the elevated VLCFA levels and possibly distinct from the other forms of cerebral XALD [4, 6]. Therefore, analyses were also performed without this group.
We initially tested for association between the functional C47T variant (Ala16Val; rs4880) and the presence of cerebral disease in XALD patients. The frequency of the T allele, encoding the less enzymatically active valine variant, is 0.53. This is frequent enough to account for the common occurrence of multiple phenotypes in a pedigree and similar to the 0.44 allele frequency predicted by the analysis that suggested a dominant model for a modifier effect [4]. Single-locus association analyses were performed using four genetic models in PLINK [30]. The allele and genotype frequencies are listed in Table 2. The T allele was associated with cerebral disease under the dominant model test in the dataset including all cerebral cases (p = 0.04; ORT* = 1.90, 95% CI 1.01–3.56) and in the dataset including only non-childhood cerebral cases (p = 0.03; ORT* = 2.47, 95% CI 1.08–5.61). We did not correct for multiple testing because testing this variant was our single main hypothesis. Additionally, the reported p values are for two-tailed tests, and therefore conservative.
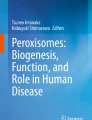
Since the valine allele of the C47T variant was associated (p ≤ 0.05) with cerebral disease in CCALD, adolescent cerebral XALD, adult cerebral XALD, and AMN cerebral patients, we genotyped three tag SNPs (rs2758352, rs2843980, and rs2758329) to perform an exploratory haplotype analysis and determine if we could capture additional genotype effects. The genomic location of the SNPs and the pairwise linkage correlation coefficient values (based on our dataset) are shown in Fig. 1. Since the tag SNPs were chosen with an r 2 cut-off value of 0.80, the correlation coefficient between rs2758352 and rs2842980 is higher than expected (observed r 2 = 0.94). HaploView 4.2 reports an r 2 value of 0.86 using the CEU HapMap data (60 singletons). Linkage disequilibrium is high across the region with all four SNPs falling into one haplotype block. Single-locus association analyses of these three SNPs indicated that none were significantly associated with cerebral disease under any of the four genetic models (Table 3). However, rs2758329 was marginally associated with cerebral disease when the CCALD cases were excluded from the analysis (p = 0.02, p corrected = 0.10; ORC* = 2.60, 95% CI 1.10–6.13). The marginal association of the C allele of rs2758329 likely reflects the high linkage disequilibrium and correlation between this marker and the functional C47T variant (D′ = 0.98; r 2 = 0.90).

SOD2 schematic and linkage disequilibrium pattern between SNPs genotyped in the SOD2 gene. The position of each SNP relative to the 14.2 kb gene is indicated. The forward arrow indicates the start of the gene. r 2 values are given in the intersecting boxes (generated in Haploview 4.2). Darker colors indicate stronger linkage disequilibrium (note, the gene is transcribed from the reverse strand)
The frequencies of the 4-SNP haplotypes are listed in Table 4. Three major haplotypes were identified with frequencies >3%. These included 95% or more of the patient population. The global Chi square test for association of haplotypes showed that there was a significant difference in the haplotype distribution between all cases and controls (p = 0.04) and between all non-childhood cases and controls (p = 0.01). The GTAC haplotype, containing the T allele of the C47T variant, was significantly associated with cerebral disease in the analysis with the total population (p corrected = 0.03; OR = 1.75, 95% CI 1.11–2.75) and significantly associated with cerebral disease in the analysis including only non-childhood cerebral cases (p corrected = 0.008; OR = 2.20, 95% CI 1.27–3.83).
Since the single-locus rs4880 and haplotype associations were strengthened when we omitted the CCALD patients, we hypothesize that variants in SOD2 may only contribute to the development of cerebral disease in adolescent and adult XALD patients. To test this, we performed the single-locus rs4880 and haplotype association analyses with only the CCALD cases (46% of total cerebral population) and the non-cerebral controls. The T allele of the C47T variant was not associated with childhood cerebral disease under any genetic model (dominant model p = 0.33; ORT* = 1.47, 95% CI 0.68–3.16). The global Chi-square test for association of haplotypes showed that there was no difference in the haplotype distribution between childhood cerebral cases and non-cerebral controls (p = 0.49); and the GTAC haplotype was also not associated with childhood cerebral cases (p corrected = 0.72; OR = 1.41, 95% CI 0.80–2.48).
Lastly, we tested for association between the valine allele and cerebral disease development in AMN patients by comparing only AMN cerebral cases to all non-cerebral controls. Omitting the adolescent cerebral and adult cerebral patients whose clinical course is most similar to the CCALD patients reduced the number of cerebral cases to 39 patients (33% of the total cerebral patient population). Although this reduces the power to detect an association, the valine allele of the C47T variant was significantly associated with AMN cerebral cases under the dominant model (p = 0.02; ORT* = 3.56, 95% CI 1.16–10.88) and marginally associated under the genotypic (p = 0.06) and allelic (p = 0.11) tests. The GTAC haplotype was associated with AMN cerebral cases (p = 0.03; p corrected = 0.10; OR = 2.07, 95% CI 1.07–4.03).
Discussion
In this study, the T allele encoding the lower functioning valine residue at amino acid position 16 and the GTAC haplotype in the SOD2 gene are significantly associated with cerebral demyelination in XALD patients. We conclude that SOD2 genetic variants play a role in modifying the development of cerebral demyelinating disease in adolescent and adult XALD patients because the associations of the T allele and the GTAC haplotype were slightly strengthened when the CCALD patients were removed from the analyses and because there was no association of the T allele or the GTAC haplotype with CCALD cases. Association of the C47T variant was strongest under the dominant model, supporting our previous segregation analysis. The odds ratio indicates that adolescent and adult cerebral XALD patients and AMN cerebral patients carrying at least one valine allele (CT or TT genotypes) are 2.47 times more likely to develop cerebral disease than those homozygous for the alanine allele (CC genotype).
While the valine allele may contribute to the development of cerebral disease, its effect is not large enough to account for all of the phenotypic diversity in XALD. Our analyses of the three additional SNPs and haplotypes also cannot account for this phenotypic diversity. Other variants in SOD2 or an interplay of other genetic variants and environmental or stochastic factors may modify the development of cerebral disease and phenotypic heterogeneity in XALD. In the SOD2 gene region there are over 100 SNPs including at least 18 with possible functional significance and eight coding SNPs that result in nonsynomymous changes (http://ensembl.org) [31]. Some of these polymorphisms may account for the 56-fold variation in SOD2 enzymatic activity observed in healthy individuals and may contribute to the development of cerebral demyelination in XALD patients [21]. We cannot exclude the possibility that other variants within SOD2 that were not captured by our analyses contribute to the development of cerebral demyelination in XALD patients.
In the general population, antioxidant capacity decreases with age [32]. In XALD, decreases in the antioxidant capacity of the brain may lead to cerebral disease and may contribute to the progressive phenotypes of XALD. Approximately 35% of AMN patients develop cerebral demyelination, and therefore in this study some non-cerebral AMN patients that were classified as controls may develop cerebral disease in the future [15, 33]. However, only 3% of Addison-only or asymptomatic patients developed cerebral disease in a study by van Geel et al. [33]; and therefore, we do not regard them as major confounders.
In XALD, the loss of ABCD1 function causes metabolic abnormalities that include an increase in mitochondrial damage, an increase in VLCFA levels possibly due to reduced mitochondrial function, and increased oxidative stress and damage that precedes the development of cerebral disease [12, 15]. In general, the brain is more susceptible to oxidative stress and damage than other tissues because it has relatively low levels of antioxidants and a high content of easily oxidized substrates that make it vulnerable to reactive oxygen species [13, 32]. SOD2 is critical in modulating the response of neurons to various stresses and capable of protecting the brain from oxidative damage [32]. Alterations in SOD2 activity (and/or other enzymes) that decrease the ability of the brain and/or mitochondria to handle increased oxidative stress may contribute to the development of cerebral demyelinating disease in XALD by further increasing the rate or amount of oxidative damage and mitochondrial damage that occurs in the brain. When the antioxidant defenses are overwhelmed, cerebral demyelination may develop. Genetic variants that result in differing capacities of the brain to handle increased oxidative stress in combination with environmental and stochastic factors may explain why it is more common for different XALD phenotypes rather than the same XALD phenotype to occur in XALD kindreds [1].
The methionine metabolism variants that are associated with the development of cerebral disease in XALD patients may also alter oxidative stress levels in the brain. Glutathione, a metabolite of methionine, is an important intracellular antioxidant that protects against free-radical damage. The insertion allele (c.844_845ins68) of the CBS gene that is associated with protection from cerebral demyelination in AMN patients is suggested to be a gain-of-function allele that increases glutathione synthesis [8]. Therefore, increased glutathione levels may protect against the development of cerebral demyelination in XALD by increasing the antioxidant capacity of the brain and reducing levels of oxidative stress and oxidative damage.
In conclusion, the reduced function variant C47T and the GTAC haplotype in the SOD2 gene are significantly associated with cerebral demyelination in adolescent cerebral XALD, adult cerebral XALD, and AMN cerebral patients. If adolescent or adult XALD patients with cerebral demyelination have reduced SOD2 activity, then either SOD2 genotyping or enzymatic assays may be used as a predictive measure of cerebral disease development and be used to determine which patients may benefit from antioxidant therapy.
References
Moser HW, Mahmood A, Raymond GV (2007) X-linked adrenoleukodystrophy. Nat Clin Pract Neurol 3(3):140–151
Eichler F, Mahmood A, Loes D, Bezman L, Lin D, Moser HW, Raymond GV (2007) Magnetic resonance imaging detection of lesion progression in adult patients with X-linked adrenoleukodystrophy. Arch Neurol 64(5):659–664
Smith KD, Kemp S, Braiterman LT, Lu JF, Wei HM, Geraghty M, Stetten G, Bergin JS, Pevsner J, Watkins PA (1999) X-linked adrenoleukodystrophy: genes, mutations, and phenotypes. Neurochem Res 24(4):521–535
Heinzer AK, McGuinness MC, Lu JF, Stine OC, Wei H, Van der Vlies M, Dong GX, Powers J, Watkins PA, Smith KD (2003) Mouse models and genetic modifiers in X-linked adrenoleukodystrophy. Adv Exp Med Biol 544:75–93
Maier EM, Mayerhofer PU, Asheuer M, Kohler W, Rothe M, Muntau AC, Roscher AA, Holzinger A, Aubourg P, Berger J (2008) X-linked adrenoleukodystrophy phenotype is independent of ABCD2 genotype. Biochem Biophys Res Commun 377(1):176–180
Powers JM, Pei Z, Heinzer AK, Deering R, Moser AB, Moser HW, Watkins PA, Smith KD (2005) Adreno-leukodystrophy: oxidative stress of mice and men. J Neuropathol Exp Neurol 64(12):1067–1079
Matsukawa T, Asheuer M, Takahashi Y, Goto J, Suzuki Y, Shimozawa N, Takano H, Onodera O, Nishizawa M, Aubourg P, Tsuji S (2011) Identification of novel SNPs of ABCD1, ABCD2, ABCD3, and ABCD4 genes in patients with X-linked adrenoleukodystrophy (ALD) based on comprehensive resequencing and association studies with ALD phenotypes. Neurogenetics 12(1):41–50
Linnebank M, Semmler A, Kleijer WJ, van der Sterre ML, Gartner J, Fliessbach K, Sokolowski P, Kohler W, Schlegel U, Klockgether T, Wanders RJ, Schmidt S, Wullner U, Kemp S (2006) The cystathionine beta-synthase variant c.844_845ins68 protects against CNS demyelination in X-linked adrenoleukodystrophy. Hum Mutat 27(10):1063–1064
Linnebank M, Kemp S, Wanders RJ, Kleijer WJ, van der Sterre ML, Gartner J, Fliessbach K, Semmler A, Sokolowski P, Kohler W, Schlegel U, Schmidt S, Klockgether T, Wullner U (2006) Methionine metabolism and phenotypic variability in X-linked adrenoleukodystrophy. Neurology 66(3):442–443
Pinteaux E, Copin JC, Ledig M, Tholey G (1996) Modulation of oxygen-radical-scavenging enzymes by oxidative stress in primary cultures of rat astroglial cells. Dev Neurosci 18(5–6):397–404
Patten DA, Germain M, Kelly MA, Slack RS (2010) Reactive oxygen species: stuck in the middle of neurodegeneration. J Alzheimers Dis 20(2):S357–S367
McGuinness MC, Lu JF, Zhang HP, Dong GX, Heinzer AK, Watkins PA, Powers J, Smith KD (2003) Role of ALDP (ABCD1) and mitochondria in X-linked adrenoleukodystrophy. Mol Cell Biol 23(2):744–753
Vargas CR, Wajner M, Sirtori LR, Goulart L, Chiochetta M, Coelho D, Latini A, Llesuy S, Bello-Klein A, Giugliani R, Deon M, Mello CF (2004) Evidence that oxidative stress is increased in patients with X-linked adrenoleukodystrophy. Biochim Biophys Acta 1688(1):26–32
Fourcade S, Lopez-Erauskin J, Galino J, Duval C, Naudi A, Jove M, Kemp S, Villarroya F, Ferrer I, Pamplona R, Portero-Otin M, Pujol A (2008) Early oxidative damage underlying neurodegeneration in X-adrenoleukodystrophy. Hum Mol Genet 17(12):1762–1773
Singh I, Pujol A (2010) Pathomechanisms underlying X-adrenoleukodystrophy: a three-hit hypothesis. Brain Pathol 20(4):838–844
Melov S, Schneider JA, Day BJ, Hinerfeld D, Coskun P, Mirra SS, Crapo JD, Wallace DC (1998) A novel neurological phenotype in mice lacking mitochondrial manganese superoxide dismutase. Nat Genet 18(2):159–163
Hinerfeld D, Traini MD, Weinberger RP, Cochran B, Doctrow SR, Harry J, Melov S (2004) Endogenous mitochondrial oxidative stress: neurodegeneration, proteomic analysis, specific respiratory chain defects, and efficacious antioxidant therapy in superoxide dismutase 2 null mice. J Neurochem 88(3):657–667
Lynn S, Huang EJ, Elchuri S, Naeemuddin M, Nishinaka Y, Yodoi J, Ferriero DM, Epstein CJ, Huang TT (2005) Selective neuronal vulnerability and inadequate stress response in superoxide dismutase mutant mice. Free Radic Biol Med 38(6):817–828
Qi X, Lewin AS, Hauswirth WW, Guy J (2003) Optic neuropathy induced by reductions in mitochondrial superoxide dismutase. Invest Ophthalmol Vis Sci 44(3):1088–1096
Guy J (2008) Optic nerve degeneration in experimental autoimmune encephalomyelitis. Ophthalmic Res 40(3–4):212–216
Bastaki M, Huen K, Manzanillo P, Chande N, Chen C, Balmes JR, Tager IB, Holland N (2006) Genotype-activity relationship for Mn-superoxide dismutase, glutathione peroxidase 1 and catalase in humans. Pharmacogenet Genomics 16(4):279–286
Rosenblum JS, Gilula NB, Lerner RA (1996) On signal sequence polymorphisms and diseases of distribution. Proc Natl Acad Sci USA 93(9):4471–4473
Valenti L, Conte D, Piperno A, Dongiovanni P, Fracanzani AL, Fraquelli M, Vergani A, Gianni C, Carmagnola L, Fargion S (2004) The mitochondrial superoxide dismutase A16V polymorphism in the cardiomyopathy associated with hereditary haemochromatosis. J Med Genet 41(12):946–950
Sutton A, Khoury H, Prip-Buus C, Cepanec C, Pessayre D, Degoul F (2003) The Ala16Val genetic dimorphism modulates the import of human manganese superoxide dismutase into rat liver mitochondria. Pharmacogenetics 13(3):145–157
Hiroi S, Harada H, Nishi H, Satoh M, Nagai R, Kimura A (1999) Polymorphisms in the SOD2 and HLA-DRB1 genes are associated with nonfamilial idiopathic dilated cardiomyopathy in Japanese. Biochem Biophys Res Commun 261(2):332–339
Nomiyama T, Tanaka Y, Piao L, Nagasaka K, Sakai K, Ogihara T, Nakajima K, Watada H, Kawamori R (2003) The polymorphism of manganese superoxide dismutase is associated with diabetic nephropathy in Japanese type 2 diabetic patients. J Hum Genet 48(3):138–141
Mollsten A, Marklund SL, Wessman M, Svensson M, Forsblom C, Parkkonen M, Brismar K, Groop PH, Dahlquist G (2007) A functional polymorphism in the manganese superoxide dismutase gene and diabetic nephropathy. Diabetes 56(1):265–269
Tian C, Fang S, Du X, Jia C (2011) Association of the C47T polymorphism in SOD2 with diabetes mellitus and diabetic microvascular complications: a meta-analysis. Diabetologia 54(4):803–811
Barrett JC, Fry B, Maller J, Daly MJ (2005) Haploview: analysis and visualization of LD and haplotype maps. Bioinformatics 21(2):263–265
Purcell S, Neale B, Todd-Brown K, Thomas L, Ferreira MA, Bender D, Maller J, Sklar P, de Bakker PI, Daly MJ, Sham PC (2007) PLINK: a tool set for whole-genome association and population-based linkage analyses. Am J Hum Genet 81(3):559–575
Wiener HW, Perry RT, Chen Z, Harrell LE, Go RC (2007) A polymorphism in SOD2 is associated with development of Alzheimer’s disease. Genes Brain Behav 6(8):770–775
Colombrita C, Calabrese V, Stella AM, Mattei F, Alkon DL, Scapagnini G (2003) Regional rat brain distribution of heme oxygenase-1 and manganese superoxide dismutase mRNA: relevance of redox homeostasis in the aging processes. Exp Biol Med (Maywood) 228(5):517–524
van Geel BM, Bezman L, Loes DJ, Moser HW, Raymond GV (2001) Evolution of phenotypes in adult male patients with X-linked adrenoleukodystrophy. Ann Neurol 49(2):186–194
Acknowledgments
We thank Ann Moser, Kim Hollandsworth, and Lena Bezman at the Kennedy Krieger Institute for the verification of patient diagnoses and Hugo and Ann Moser for the patient samples. This work was supported by the Johns Hopkins McKusick-Nathans Institute of Genetic Medicine and Public Health Service grants GM077456, HD10981, and HD20961 from the National Institutes of Health.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Brose, R.D., Avramopoulos, D. & Smith, K.D. SOD2 as a potential modifier of X-linked adrenoleukodystrophy clinical phenotypes. J Neurol 259, 1440–1447 (2012). https://doi.org/10.1007/s00415-011-6371-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-011-6371-8