
Abstract
In this study, we used positron emission tomography (PET) at two different time points to study the temporal evolution of reorganization in patients with good and those without motor recovery from hemiplegia after the occurrence of a stroke. Ten hemiplegic patients with a first subcortical stroke and five healthy control subjects were scanned during passive and active movements at an interval of 8 weeks. PET1 was performed 22.8 ± 7.8 days after the index stroke. At PET2, 8 weeks later, patients were dichotomized to either good recovery or no recovery according to the upper extremity motor component of the Fugl–Meyer score. Increases of regional cerebral blood flow (rCBF) and comparison between groups at PET1 and PET2 were assessed using statistical parametric mapping. At PET 1, activation was found bilaterally in the inferior parietal cortex. Eight weeks later, patients with good recovery showed maximum activation in the contralateral primary somatosensory cortex and overactivation of the contralateral inferior parietal cortex. Patients with poor recovery showed bilateral activation with a maximum in the somatosensory cortex. Studies correlating activation patterns with quality of recovery may identify the neuroanatomical substrates that subserve improved motor function. Such studies may also guide the development of more effective rehabilitative interventions after the occurrence of stroke.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Most patients who survive an acute ischemic stroke experience some functional recovery in the weeks to months following the injury. While ambulatory function recovers in many patients even after dense hemiplegia, restoration of upper extremity motor skills is less complete. Only 20% of patients who remain flaccid 2 weeks after a stroke regain some functional use of their hand [1]. Return of voluntary arm movements is one of the most important goals during stroke rehabilitation to avoid long-term disability in activities of daily living (ADL) function.
Functional imaging and electrophysiologic brain mapping techniques have provided substantial insight into the adaptive changes of cerebral networks associated with recovery from brain damage. Recruitment of areas adjacent to the brain lesion or of ipsilateral motor regions has been described after complete recovery from upper extremity motor impairment [2]. Furthermore, dynamic reorganization of both motor and sensory structures occurs in parallel with improvement of upper extremity motor function [3]. Given the close temporal correlation between these sequential alterations of cerebral activity and return of voluntary motor control, many of the dynamic changes observed in the cerebral cortex may have a restorative function. The evolution of brain activation after a stroke in patients with variable motor recovery has been studied with PET [4] and fMRI [5, 6]. One consistent finding of these prospective studies was a sustained increased activation of bilateral primary and secondary motor areas in patients with poor motor recovery after a stroke. In patients with better motor recovery return of motor function was coupled with decreasing neural activity over time. Patients with good or complete recovery showed activation patterns similar to that of healthy control subjects [4, 7]. More recent data has also emphasized the integrity of the corticospinal tract for successful motor recovery [8, 9]. It is less clear, however, how brain activation of patients with severe hemiparesis or hemiplegia at stroke onset changes over time. This question is important to better understand the relationship between reorganized brain activity and recovery of neurologic function.
The aim of this study was to compare changes of brain activation patterns in patients with good and those with no motor recovery after a subcortical, ischemic stroke causing hemiplegia. We hypothesized that patients with good recovery show more contralateral activation compared to patients with poor recovery. Subcortical lesions were selected for this study because the morphological structure of the cortex is usually preserved in these patients. The severe hemiparesis of our patients precluded any active motor tasks during functional imaging at baseline. Therefore, we used passive forearm movements as an additional, performance-independent activation paradigm. Cortical activation during passive movements is induced by proprioceptive input and shows similar patterns compared to active movements [10]. All patients underwent two PET activation studies each during the first 12 weeks after the occurrence of a stroke.
Methods
Subjects
Ten stroke patients and five control subjects were enrolled in this study. Patients with (a) first subcortical ischemic stroke causing severe contralateral hemiparesis defined as NIH stroke scale [11] question 5 score ≥3, (b) pure motor deficit without sensory impairment, (c) no prior stroke with sensory or motor deficits, and (d) no signs or history of other neurological or psychiatric diseases were included in the study. Lesion volumes in all patients did not exceed 1 × 1 × 1 cm in all subjects. Exclusion criteria were defined by the following NIH stroke scale questions: decreased level of consciousness (questions 1a, 1b, 1c; each >0), aphasia (question 9; score >2), or neglect (question 11; score >2). No patient had evidence of spasticity or joint stiffness. Sensory modalities such as pin prick, light touch and proprioceptive function were intact in all patients. CT or MR images of the brain were performed in all patients to document type and location of stroke. Five age-matched control subjects (63.0 ± 3.0, three females) were recruited through local advertisement. All control subjects were healthy volunteers with no history of neurological or psychiatric disease. The purpose of examining healthy individuals was to demonstrate that the pattern of brain activation over time is stable. Prior to each PET, a full neurological exam including the Fugl-Meyer scale (motor component for upper extremity) was obtained for each subject (range 0–66, normal score: 66 points) [12]. The Fugl-Meyer scale has shown high reliability and validity for the assessment of motor function in hemiparetic stroke patients [13]. Handedness was evaluated according to the Edinburgh Handedness Inventory [14]. All stroke and control subjects were right-handed. Informed consent was obtained from all patients and volunteers. This study was approved by the Ethics Committee of the University of Essen. Permission was granted from the German Commission of radiation protection.
Design and procedures
Ten hemiplegic patients with a first subcortical stroke and five healthy control subjects were scanned twice using the [15O]H2O bolus injection technique. The first PET scan (PET1) was performed within 4 weeks (22.8 ± 7.8 days) after the index stroke. The second PET scan (PET2) was performed exactly 8 weeks later in every subject. At PET2, patients were dichotomized to either good recovery or no recovery according to the upper extremity motor component of the Fugl-Meyer score. Patients with clinically significant improvement of at least 20 points on the Fugl-Meyer motor scale were classified as well recovered. Regional cerebral blood flow (rCBF) was measured during rest and during passive elbow movements of the plegic arm at PET1, and, in addition, during active movements at PET2. Significant differences of rCBF between each condition and comparison between groups at PET1 and PET2 were assessed using statistical parametric mapping (SPM).
PET Data acquisition and reconstruction
The data were acquired in two-dimensional mode on an ECAT EXACT HR+ PET scanner (CTI, Inc., Knoxville, TN). Head movements were minimized with foam rubber pads on each side of the head. For each subject, six consecutive scans of the rCBF during rest (condition A) and during passive elbow movements (condition B) were obtained in alternating order (ABABAB) at baseline. Eight weeks later, patients received a second PET with nine consecutive scans, including active movements (condition C). At PET 2, all patients were able to perform some active flexion and extension of elbows, with reduced range of motion in patients with poor recovery. Five healthy subjects were scanned twice at a 3-week interval. No rehabilitative manipulation was performed in healthy individuals. Healthy subjects were scanned to examine the stability of brain activation patterns in a longitudinal PET study. Subjects kept eyes closed at all times during measurements. The plegic arm was abducted at the shoulder level to 70° and placed in a forearm brace that was connected to a torque motor. Passive forearm movements of the plegic arm (right arm in healthy subjects) with an amplitude of 0–90° flexion/extension of the elbow and a frequency of 0.5 Hz were generated using a torque motor. During active movements, the same range and velocity of forearm movements were generated by subjects. Timing was controlled by verbal cues.
Prior to the start of the first activation scan, a 10-min transmission scan was acquired to provide measured attenuation correction. The regional cerebral blood flow was measured using the [15O]H2O bolus injection technique. Specifically, for each scan, 700 MBq were injected using an automatic injector system. The interval between injections was 10–11 min. During this interval, the [15O]H2O activity in the brain decayed to a background level that was at most 10% of the peak counts of the next scan. A bolus of about 10–20 ml of 0.9% sodium chloride solution over a period of 50 s was administered. After administration of [15O]H2O, the measurements lasted 90 s and started only shortly before the rise of the head curve. The uncertainty of the injected activity is approximately ±10%.
The images were reconstructed with filtered backprojection without smoothing (see section “Data analyses”) and with a cut-off at the Nyquist frequency. The reconstruction zoom was 2.0 and the image matrix 128 × 128. The images were corrected for attenuation using the measured transmission scan. Standard corrections for scatter and dead time were applied.
Data analyses
PET data were analyzed using statistical parametric mapping (SPM, Wellcome Department of Cognitive Neurology, London, UK). Images were realigned to the first volume, normalized to the standard anatomical space corresponding to the atlas of Talairach and Tournoux [15] using a least-square fitting program, and then smoothed (low-pass 3-D Gaussian filter; 15 × 15 × 9 mm3 at FWHM) [16]. This smoothing parameter reveals the same final image resolution for all subjects. Statistical parametric maps were then generated for each subject. Global flow differences were normalized voxel by voxel to a mean of 50 ml dl−1 min−1 by proportional scaling. Because the majority of patients had a right-sided infarct, all lesions were assigned to the right side of the brain. Three patients with a left-sided lesion were inverted about the midsagittal plane. Thus, for analytical purposes, the hemiplegic arm was always on the left.
Statistics
Assessment of significant rCBF changes were performed using SPM’99. Statistical inferences were based on group effects using a fixed-effects model. Voxel-by-voxel comparison using the general linear model and t statistics calculated differences of rCBF between passive or active movements and rest (within-group analysis). The t statistics for every voxel was transformed into a unit normal distribution such that ϕ(Z) = ψ(t), where ϕ(Z) is the standard normal cumulative density function and ψ(t) is the Student t distribution with the appropriate degrees of freedom given by the experimental design. The resulting statistical parametric map SPM(Z) was subsequently used to assign p values (to voxels and also to clusters), that are corrected for multiple, non-independent comparisons [16]. Significant differences of activation were accepted at p < 0.01. Small patches of activation, expected to appear by random fluctuations, were excluded by setting a spatial cluster extent level at 10 voxels.
In order to test of relative increases of rCBF in patients with good versus bad recovery, the same model was used (between-group analyses). Differences of activation were considered significant at p < 0.01 and if their spatial extend was >10 voxels. All results of statistical analyses showing areas of significant rCBF increases are displayed by superimposing statistical parametric maps onto three-dimensional Talairach-Tournoux normalized, high-resolution T1-weighted MRI brain scan. Differences between the mean NIHSS and Fugl-Meyer scores in both groups were calculated with a Student’s t test.
Results
Clinical and demographic data of patients are summarized in Table 1. At baseline PET, all patients were unable to move the forearm or distal parts of the upper extremity. Two patients had recovered voluntary control of shoulder elevation and abduction. The first PET scan was performed within 4 weeks after a stroke in all ten patients. At baseline, the mean (±SD) Fugl-Meyer score of all patients was 7.6 ± 3.4 points and NIHSS score was 8.9 ± 2.4 indicating severe hemiparesis. At PET 2 8 weeks later, patients with good motor recovery of the affected upper extremity had a Fugl-Meyer-score of 43.4 ± 9.4 points and NIHSS score 1.4 ± 0.8 points. In patients without motor recovery, the Fugl-Meyer-score remained unchanged in three patients and showed a small increase of three points without functional gains in two other patients. The NIHSS was unchanged in three patients and decreased by 1 point (improvement) in two other patients. All control subjects had normal motor and sensory function with a NIHSS score of 0 and a Fugl-Meyer score of 66 at time of both PET studies.
Normal subjects (passive movements vs. rest)
At PET 1, most significant increases of rCBF were found in the contralateral sensorimotor cortex at 64 mm above the ACPC line. The maximum activation was centered on the posterior bank of the central sulcus (Brodmann areas 1, 2, 3), but activation also covered the precentral gyrus (Brodmann area 4) and supplementary motor area (Brodmann area 6) and cingulate gyrus (Brodmann area 24). Strong bilateral increases of rCBF were also observed in the inferior parietal cortices (Brodmann area 40). At PET 2, 3 weeks later, there was almost identical activation in the contralateral sensorimotor cortex, supplementary motor area, and bilateral inferior parietal cortex compared to PET 1. In a direct comparison of rCBF increases during PET 1 and PET 2 (between-group analysis) no areas of activation were found. There was thus no statistical significant difference in the location or amount of activated areas between PET 1 and PET 2 in normal subjects.
Stroke patients at baseline
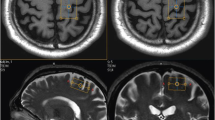
At baseline, significant increases of rCBF were observed bilaterally in the inferior parietal cortex (Brodmann area 40), stronger in the contralateral hemisphere with a maximum at 42 mm above the ACPC line. This cluster also extended into the superior parietal lobe (Brodmann area 7). Activation of the ipsilateral inferior parietal cortex was located between 34 and 48 mm above the ACPC line (Table 2, Fig. 1).

Activation during passive movements at baseline. Increases of regional cerebral blood flow (rCBF) during passive movements of the plegic (left) arm in stroke patients (passive movements vs. rest, within-group analysis, p < 0.01). Surface view of statistical parametric maps. All lesions were assigned to the right side of the brain. Three patients with a left-sided lesion were inverted about the midsagittal plane. Thus, for analytical purposes, the hemiplegic arm was always on the left. Areas of activation are superimposed onto a T1-weighted MRI brain scan
Stroke patients with good motor recovery at follow-up
Eight weeks later, patients showed predominant activation of the contralateral primary somatosensory cortex (Brodmann areas 1) during passive movements. No ipsilateral activations were found during passive movements (Table 3a, Fig. 2). During active movements, the most significant activation was located in the contralateral primary somatosensory cortex. Small increases of cerebral blood flow were also found bilaterally in the dorsolateral prefrontal cortex (Table 3b, Fig. 2).

Sites of activation in stroke patients with good recovery. Increases of regional cerebral blood flow (rCBF) during passive movements (upper panel) and active movements (lower panel) of the plegic (left) arm in stroke patients with good recovery (within-group analysis, p < 0.01)
Stroke patients with poor motor recovery at follow-up
During passive movements, patients with poor or no motor recovery showed predominant bilateral activation. Strongest increases of cerebral blood flow were found in the contralateral postcentral gyrus (Brodmann areas 1–3). There was also bilateral activation of the superior temporal gyrus and the cerebellum. Ipsilateral activations were found in the inferior parietal cortex (Table 4a, Fig. 3).

Sites of activation in stroke patients with poor recovery. Increases of regional cerebral blood flow (rCBF) during passive movements (upper panel) and active movements (lower panel) of the plegic (left) arm in stroke patients with poor recovery (within-group analysis, p < 0.01)
During active movements, there was again bilateral activation with most significant increases of cerebral blood flow in the contralateral primary somatosensory cortex. Similar to activation areas during passive movements, we observed contralateral activation of the medial temporal gyrus and ipsilateral activation of the superior temporal gyurs and cerebellum. Ipsilateral activations were again found in the inferior parietal cortex (Table 4b, Fig. 3).
Relative overactivation in patients with good recovery (between-group comparisons)
To identify areas that were relatively more activated in patients with good motor recovery versus those with poor recovery, we directly compared increases of rCBF obtained from PET 2 in both groups (between-group comparison). This was achieved by subtracting increases of rCBF during active movements of the poor recovery group from those with good recovery. Relative overactivation during active movements in patients with good motor recovery was found in contralateral Brodmann Area 40 of the inferior parietal cortex (x = 60, y = −46, z = 20, Z-score 3.5) and in Brodmann area 19 (x = 30, y = −82, z = −8, Z-score 3.5; Fig. 4).

Sites of relative overactivation in patients with good recovery. Increases of regional cerebral blood flow (rCBF) during active movements of the plegic (left) arm in stroke patients with good recovery compared to patients with bad recovery (between-group analysis, p < 0.01)
Conversely, areas with relatively more activation in patients with poor recovery compared to those with good recovery were identified by subtracting increases of rCBF of the poor recovery group from those of the good recovery group. In this analysis, no foci of activation were found above threshold.
Discussion
In this study, serial PET imaging was used to evaluate differences in brain activation between patients with different degrees of recovery from hemiplegic stroke. We did not find any statistical significant differences between PET 1 and PET 2 in healthy individuals suggesting that the pattern of brain activation during passive movements is very stable across time in serial PET of normal subjects. The observed stability of brain activation in our and other serial PET experiments of healthy subjects is an important property of this methodology and helps in the interpretation of sequential functional imaging results in patients [17].
All patients included in this study had a dense flaccid hemiplegia and were unable to perform active forearm movement at time of inclusion into the study. We therefore selected passive forearm movements as an activation paradigm that is independent of the patients’ motor skills. At baseline, the most significant increases of rCBF were found in the bilateral inferior parietal cortex. This pattern of brain activation in hemiplegic stroke patients prior to clinical recovery corroborates results from previous study of severely affected stroke patients [3].
Eight weeks after baseline PET, we found different patterns of brain activation in patients with good recovery compared to those without recovery. The brain activation maps of patients with good recovery showed recruitment of additional areas in the contralateral parietal cortex including the occipitoparietal association cortex compared to those with poor or no recovery. To exclude the possibility that the patterns of brain activation differed at PET 1 we also compared rCBF increases between both groups at PET 1 and did not find any statistical significant differences in the activation of motor or sensory systems. Stroke patients of both groups were closely matched in the initial degree of motor deficit and did not differ in demographic or clinical parameters such as age, sex, or stroke topography. Because contralateral overactivation of the parietal somatosensory cortex was seen only in patients with good recovery, this area may play an important role in recovery of upper extremity motor function. A predominantly contralateral (ipsilesional) activation in patients with good recovery has also been reported in well-recovered patients of a longitudinal PET-study by Carey et al. [4]. In our study, however, recruitment of additional areas was found in the contralateral parietal cortex, a finding that was not reported in previous longitudinal functional imaging studies comparing different degrees of motor recovery [4–8]. The severe hemiparesis at stroke onset of our patients and the use of forearm movements as an activation paradigm may explain the activation of the contralateral parietal cortex observed in our study.
Activation of the parietal cortex has been associated with preparation and redirection of movements and movement intentions [18]. Areas contributing to motor attention such as the posterior parietal cortex may help to recover lost motor function when efferent fibers from primary motor areas are damaged by ischemic lesions. Postcentral cortex activation is similar during passive and active forearm movements in normal subjects suggesting that this activation is largely mediated by processing of proprioceptive information in different population of cells within the same area [10, 19]. Brodmann area 40 has an important function in proprioceptive integration. Neuroanatomical studies have shown that secondary sensory cortical regions, such as BA 40, are interconnected with the postcentral gyrus (SI, area 3b), the posterior parietal cortex and prefrontal cortex, a distributed network involved in processing somatosensory inputs [20]. BA 40 (including SII) is involved in high-level sensory processing and sensorimotor integration [21]. Increased reliance on structures normally involved in processing somatosensory information may be an integral part for reorganization of sensory systems and subserve motor recovery. The importance of the somatosensory cortex for motor recovery has also been confirmed in a recent study that used fMRI in the first days after the occurrence of a stroke: the authors found brain activation of the postcentral gyrus that correlated with subsequent motor recovery [22].
In contrast, patients with poor recovery maintained ipsilateral inferior and superior parietal activation during passive movements. No other additional motor or sensory areas were recruited in the poor recovery group. A strong area of increased cerebral blood flow was also found in the somatosensory cortex, similar to that observed in patients with good recovery. During active movements, patients with poor recovery showed predominant activation of parietal and temporal cortical areas. No activation was found in the somatosensory cortex, as observed in patients with good recovery.
In this group of patients, the ischemic lesion involved the basal ganglia and the pons and was balanced between both groups. More recent studies have linked defined regions such as the area leading from the corona radiate to the corticospinal tract as critical for restoration of upper extremity motor performance after a stroke [23]. Stroke location was not different between patients with good and those with bad or no recovery. We therefore do not believe that differences in the location of the lesion alone explain the observed patterns of brain activation in patients with good and those without or with poor recovery. Our data indicate a relationship between task-related activation of predominantly sensory systems and degree of motor recovery after a stroke.
In conclusion, stroke patients with different degrees of recovery have different patterns of brain activation. Good recovery was associated with relatively more contralateral brain activation of secondary somatosensory areas. The sample size in the dichotomized groups at follow-up is small. Comparisons where therefore based on a fixed-effects model that does not permit any generalization to the stroke population. However, we carefully selected patients with comparable stroke pathology and loss of motor control. It is challenging to find patients with homogenous neurologic functional deficits. Future studies on a larger sample size correlating activation patterns with quality of recovery are needed to identify the neuroanatomical substrates that subserve improved motor function. Such studies may also guide the development of more effective rehabilitative interventions after a stroke.
References
Feys H, de Weerdt W, Nuyens G, van de Winckel A, Selz B, Kiekens C (2000) Predicting motor recovery of the upper limb after stroke rehabilitation: value of a clinical examination. Physiother Res Int 5:1–18
Calautti C, Naccarato M, Jones PS et al (2007) The relationship between motor deficit and hemisphere activation balance after stroke. A 3T fMRI study. Neuroimage 34:322–331
Nelles G, Spiekermann G, Jueptner M, Leonhardt G, Muller S, Gerhard H, Diener HC (1999) Evolution of functional reorganization in hemiplegic stroke: a serial positron emission tomographic activation study. Ann Neurol 46:901–909
Carey LM, Abbott DF, Egan GF, O’Keefe GJ, Jackson GD, Bernhardt J, Donnan GA (2006) Evolution of brain activation with good and poor motor recovery after stroke. Neurorehabil Neural Repair 20:24–41
Ward NS, Brown MM, Thompson AJ, Frackowiak RS (2003) Neural correlates of motor recovery after stroke: a longitudinal fMRI study. Brain 126:2476–2496
Tombari D, Loubinoux I, Pariente J, Gerdelat A, Albucher JF, Tardy J, Cassol E, Chollet F (2004) A longitudinal fMRI study: in recovering and then in clinically stable sub-cortical stroke patients. Neuroimage 23:827–839
Calautti C, Leroy F, Guincestre JY (2001) Baron JC. Dynamics of motor network overactivation after striatocapsular stroke: a longitudinal PET study using a fixed-performance paradigm Stroke. 32:2534–2542
Ward NS, Newton JM, Swaynde OB, Lee L, Thompson AJ, Greewood RJ, Rothwell JC, Frackowiak RSJ (2006) Motor system activation after subcortical stroke depends on corticospinal system integrity. Brain 129:809–819
Lindenberg R, Renga V, Zhu LL, Betzler F, Alsop D, Schlaug G (2010) Structural integrity of corticospinal motor fibers predicts motor impairment in chronic stroke. Neurology 74:280–287
Weiller C, Juptner M, Fellows S et al (1996) Brain representation of active and passive movements. Neuroimage 4:105–110
Brott T, Adams HP, Olinger CP et al (1989) Measurements of acute cerebral infarction: a clinical examination scale. Stroke 20:864–870
Fugl-Meyer AR, Jaasko L, Leyman I, Olsson S, Steglind S (1975) The post-stroke hemiplegic patient. 1. A method for evaluation of physical performance. Scand J Rehabil Med 7:13–31
Duncan PW, Propst M, Nelson SG (1983) Reliability of the Fugl-Meyer assessment of sensorimotor recovery following cerebrovascular accident. Phys Ther 63:1606–1610
Oldfield RC (1971) The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia 9:97–113
Talairach J, Tournoux J (1988) Coplanar stereotaxic atlas of the human brain. Thieme Verlag, New York
Frackowiak RSJ, Friston KJ, Frith C, Dolan R, Mazziotta J (1997) Human brain function. Academic Press, San Diego
Carey LM, Abbott DF, Egan GF, Tochon-Danguy HJ, Donnan GA (2000) The functional neuroanatomy and long-term reproducibility of brain activation associated with a simple finger tapping task in older healthy volunteers: a serial PET study. Neuroimage 11:124–144
Rushworth MF, Johansen-Berg H, Göbel SM, Devlin JT (2003) The left parietal and premotor cortices: motor attention and selection. Neuroimage S89–S100
Rausch M, Spengler F, Eysel UT (1998) Proprioception acts as the main source of input in human S-I activation experiments: a functional MRI study. Neuroreport 9:2865–2868
Baleydier C, Mauguiere F (1987) Network organization of the connectivity between parietal area 7, posterior cingulate cortex and medial pulvinar nucleus: a double fluorescent tracer study in monkey. Exp Brain Res 66:385–393
Freund HJ (2001) The parietal lobe as a sensorimotor interface: a perspective from clinical and neuroimaging data. Neuroimage 14:S142–S146
Marshall RS, Zarahn E, Alon L, Minzer B, Lazar RM, Krakauer JW (2009) Early imaging correlates of subsequent motor recovery after stroke. Ann Neurol 65:596–602
Lo R, Gitelmann DD, Levy R, Hulvershorn J, Parrish T (2010) Identification of critical areas for motor function recovery in chronic stroke subjects using voxel-based lesion symptom mapping. Neuroimage 49:9–18
Acknowledgments
We thank N. Boden for expert technical assistance. We would also like to thank all individuals who participated in this study.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nelles, G., Jentzen, W., Bockisch, A. et al. Neural substrates of good and poor recovery after hemiplegic stroke: a serial pet study. J Neurol 258, 2168–2175 (2011). https://doi.org/10.1007/s00415-011-6085-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-011-6085-y