
Abstract
The familial periodic paralyses (PP) were commonly considered to be benign diseases since frequency and severity of the paralytic attacks decrease in adulthood. However, with increasing age, a third of the patients develop permanent weakness and muscle degeneration with fatty replacement. Another complication, cardiac arrhythmia, can result from the dyskalemia during paralytic attacks. The familial PP are typical dominant ion channelopathies: the function of the mutant muscular channel is compensated in the interictal state but defective under certain conditions which then cause flaccid weakness. A triggering factor is the level of serum potassium, the extracellular ion decisive for membrane excitability. In hyper- and hypokalemic periodic paralysis, the mutations are specifically located in the voltage-gated sodium and calcium channels which are essential for action potential generation or excitation-contraction coupling. The common mechanism for the membrane inexcitability during paralytic attacks is a transient membrane depolarization that inactivates the sodium channels which are then no longer available for action potential generation. For the third PP type, the Andersen syndrome, the responsible gene is also expressed in cardiac muscle, and, independently of paralytic attacks, the hazard of ventricular arrhythmias is inherent. The gene product, an inwardly rectifying potassium channel, is responsible for maintaining the resting membrane potential, and all known mutations cause dominant–negative effects on the tetrameric channel complexes. In this article the clinical consequences of the mutations and the therapeutic strategies for all three types of PP are reported.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The familial periodic paralyses (PP) have common clinical features, recurrent patterns of mutations, predictable mechanisms of pathogenesis, and logical therapies (13). Symptoms occur episodically with varying intervals of normal muscle function. Apparently, the underlying ion channel defects are usually well-compensated and an additional trigger is often required for channel, cell and tissue malfunction. Two dominant episodic types of weakness with or without myotonia are distinguished by the serum K+ level during the attacks of tetraplegia: hyper- and hypokalemic PP. Intake of K+ and glucose have opposite effects in the two disorders: while K+ triggers attacks and glucose is a remedy in hyperkalemic PP, glucose-induced hypokalemia provokes attacks in hypokalemic PP which are ameliorated by K+ intake. Because additional release of K+ from muscle in hyperkalemic PP and uptake of K+ by muscle in hypokalemic PP, the resulting dyskalemia can be so severe that cardiac complications arise. During an attack, death can also occur due to respiratory insufficiency. Independently of the severity and frequency of the paralytic episodes, many patients develop a chronic progressive myopathy in the forties, an age at which the attacks of weakness decrease. This myopathy is characterized histologically by central vacuoles in the myofibers and ultrastructurally by a dilation and proliferation of the T-tubular system. This progressive myopathy mainly affects pelvic girdle and proximal and distal lower limb muscles detectable by fatty replacement in the 1H-MRI scan (Fig. 1).

Muscle degeneration in a patient with familial periodic paralysis The T1-weighted 1H images of the upper legs of a 56-year old patient with hypokalemic PP type 1 (R1239H mutation) are shown. Note the fatty degeneration of the gluteal, ischiocrural and vastus lateralis muscles. The vastus medialis, obturatorii interni and piriformis muscles are relatively well maintained
Additional forms of familial PP are the rare normokalemic periodic paralysis and the Andersen syndrome. The latter primarily affects not only the skeletal but also the cardiac muscle and may show hyper-, normo- or hypokalemia during paralytic attacks. Another type of dyskalemic periodic paralysis has been published but questioned since the prevalence of the underlying genetic variant is the same in patients and controls, and no paralytic attacks could be provoked in the carriers. These results will also be discussed.
Hyperkalemic periodic paralysis – a Na+ channelopathy usually associated with myotonia
Hyperkalemic PP is characterized by attacks of flaccid weakness associated with increase in serum potassium (Table 1). Potassium-rich food or rest after exercise may precipitate an attack. A cold environment, emotional stress, fasting, and pregnancy provoke or worsen the attacks. A spontaneous attack commonly starts in the morning before breakfast, lasts for 15 minutes to an hour, and then disappears together with the hyperkalemia. Between attacks, the disease is often associated with myotonia, which is mild and does not impede voluntary movements but may exacerbate at the beginning of an attack.
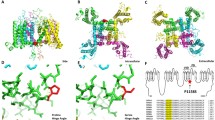
Hyperkalemic PP is caused by mutations in the voltage-gated sodium channel Nav1.4 which is essential for the generation of the muscle fiber action potential [4, 17]. Most Nav1.4 mutations are situated at inner parts of the transmembrane segments or in intracellular protein loops and affect structures that form the three-dimensional docking site for the fast inactivation particle (Fig. 2), and any malformation may reduce the affinity between the “latch bar and the catch”. The mutant channels avoid the inactivated state and, in contrast to normal Na+ channels, reopen or flicker between the inactivated and the open state (Fig. 3), corresponding to a gain-of-function defect [6, 27]. As a result, sodium influx is increased as shown in vitro [12] and in vivo [28] (Figures 4 and 5). This inward current is associated with a sustained membrane depolarization that increases the electrical driving force for potassium, and potassium released from muscle elevates the serum potassium level. Sodium influx into muscle is accompanied by entrance of water into the fibers, causing hemoconcentration and further increase in serum potassium. This is a vicious cycle which spreads out and affects the surrounding muscle fibers [13].

Membrane topology model of the sodium channel of skeletal muscle, Nav1.4 The skeletal muscle α subunit functions as ion-conducting channel and consists of four highly homologous domains (repeats I-IV) containing six transmembrane segments each (S1-S6). The S6 transmembrane segments and the S5-S6 loops form the ion selective pore, and the S4 segments contain positively charged residues conferring voltage dependence to the protein. The repeats are connected by intracellular loops; one of them, the III-IV linker, contains the supposed inactivation particle of the channel. When inserted in the membrane, the four repeats of the protein fold to generate a central pore as schematically indicated on the right-hand bottom of the figure. The different symbols used for the known mutations leading to the three types of periodic paralysis are explained on the left-hand bottom

Hyperkalemic periodic paralysis: Sodium current through mutant channels (A) Current traces of single channel recordings for normal (wild type, WT) and mutant (M1360V) sodium channels. Channel openings were elicited by step depolarizations from a holding potential of −100 to −30 mV. Reopenings were more frequent for mutant channels, thereby leading to a permanent current. (B) Time course of inactivation of heterologously expressed sodium currents recorded in the whole-cell mode of the patch clamp technique. (C) Recovery from inactivation: sodium current amplitudes were measured at −100 mV following a variable latency after a 12 ms depolarization to 0 mV. Modified after (27)

Hyperkalemic periodic paralysis: Sodium influx in a muscle fiber as measured in vitro. The intracellular sodium activity, aNai (upper panel) and the resting membrane potential (lower panel) from an excised muscle fiber from a hyperkalemic PP patient are shown. [K+]o is 3.5 mmol/L unless indicated otherwise. In the presence of 10 mmol/L [K+]o, the fiber shows an abnormally large depolarization (arrow) and, associated with it, an increase in aNai. Blockade of the sodium channels by TTX speeds the reversal of aNai and Em. From (12)

Cold-induced increase in muscular 23Na content in a hyperkalemic PP patient Shown are cross sections of the lower legs of a 17-year-old man with HyperPP before (upper panel) and after cooling (lower panel) of the left lower leg. The 0.3% NaCl solution reference phantom is positioned between both lower legs (arrow, upper panel). The 23Na MR images after provocation reveal an increase in signal intensity by 12% (arrow). The HyperPP patient developed a paresis for foot plantar- and dorsiflexion directly after cooling that was 4 according to MRC score and remained unchanged at follow-up 30 minutes later. Modified after [28]. L, left lower leg
The degree of depolarization determines the clinical symptoms: i.e. at the beginning of an attack, a slight membrane depolarization opens the non-inactivating mutant channels which generate repetitive muscle action potentials. The membrane depolarization (that results from the higher probability of the sodium channels being open) progresses. At stronger depolarization, the population of genetically normal sodium channels becomes inactivated and the muscle paralyzed. Although myotonia and paralysis are clinically the opposite, the pathomechanism is qualitatively the same. The dominance of the mutation results from the fact that the mutation is decisive for the cell excitability. The starting point is the elevation of extracellular potassium due to ingestion or exercise.
Hypokalemic periodic paralysis, a Na+ or Ca2+ channelopathy without myotonia
Hypokalemic PP differs from hyperkalemic PP in the sense that a spontaneous attack is associated with hypokalemia, potassium is a remedy, and carbohydrate- and sodium-rich food triggers an attack, and the EMG does not show myotonia. In general, the attacks last longer and are more severe. Usually, the patients are weakest during the second half of the night and in the morning, and become stronger as the day goes by.
In contrast to the gain-of-function changes in hyperkalemic PP, hypokalemic PP is associated with a loss-of-function defect of one of two different ion channel types: Cav1.1 (hypokalemic PP type 1) and Nav1.4 (hypokalemic PP type 2) [5, 7, 9, 26]. Cav1.1 is the main subunit of the voltage-gated pentameric L-type Ca2+ channel complex (also called the dihydropyridine receptor) located in the transverse (t) tubular system. Via Cav1.1, a t-tubular action potential activates the Ca2+ release channel (also called the ryanodine receptor) and the Ca2+ released from the sarcoplasmic reticulum activates the contractile machinery. Hypokalemic PP types 1 and 2 are clinically similar and in both responsible channels, the mutations are located exclusively in the voltage-sensing S4 segments: those of Nav1.4 are situated in domain 2 and those of Cav1.1 in domains 2 or 4 (Figs. 2 and 6). Functionally, the inactivated state is stabilized in the Na+ channel mutants [9, 11, 22], while the channel availability is reduced for the Ca2+ channel mutants [8, 15]. It is still unclear how the loss-of-function mutations of these two cation channels can produce the long-lasting and pronounced membrane depolarization that inactivates the sodium channels and thereby leads to the fiber inexcitability [18, 19].

Membrane topology of the L-type calcium channel of skeletal muscle, Cav1.1. The α1 subunit of the skeletal muscle L-type calcium channel (= dihydropyridine receptor, DHPR) resembles α subunit of the sodium channel however the function of the various parts, e.g. the III-IV linker, may not be the same. Mutations described for HypoPP-1 are shown in the 1-letter abbreviation for amino acids
Normokalemic periodic paralysis – a separate entity?
The term normokalemic periodic paralysis was originally given to a variant described in the 1960ies. The disorder resembled HyperPP in many aspects; the only real differences were the lack of increase in the concentration of serum potassium even during serious attacks, and the lack of a beneficial effect of glucose administration. The existence of normokalemic periodic paralysis as a nosological entity was questioned because of the potassium sensitivity of the patients and the identification of the most frequent hyperkalemic PP mutations T704M or M1592V in such families including the original family. However, recently, a potassium-sensitive type of periodic paralysis with normokalemia and episodes of weakness reminiscent of those in both hyperkalemic and hypokalemic PP was reported. This phenotype, also named normokalemic periodic paralysis, is caused by SCN4A mutations at codon 675 [26]. Codon 675 encodes an arginine in the voltage sensor of domain 2 of the sodium channel next to substitutions of R672 and R699 which cause HypoPP2. Future studies will show whether normokalemic PP is a separate clinical entity and whether the ictal normokalemia and the combination of features typical for hyper- and hypokalemic PP can be used to determine the most probable localization of the causative mutation in SCN4A.
K+ channel periodic paralysis with cardiac arrhythmia
Patients with Andersen syndrome may experience a life-threatening ventricular arrhythmia independent of their PP, and long QT syndrome is the primary cardiac manifestation [2, 24]. The syndrome is characterized by the highly variable clinical triad of dyskalemic PP, ventricular ectopy, and potential dysmorphic features [20, 23] (Fig. 7). The paralytic attack may be hyper-, normo- or hypokalemic and accordingly, the response to oral K+ is unpredictable. Mutations of the Kir2.1 K+ channel, an inward rectifier expressed in skeletal and cardiac muscle, are causative of the disorder [16] (Fig. 8). Kir2.1 channels are essential for maintaining the highly negative resting membrane potential of muscle fibers and accelerating the repolarization phase of the cardiac action potential. The mutations mediate loss of channel function by haploinsufficiency or by dominant-negative effects on the wildtype allele [3] and may lead to long-lasting depolarization and membrane inexcitability.

Clinical features of Andersen syndrome. Note the hypertelorism and the broad nose of the two patients

Membrane topology of the Kir2.1 potassium channel. The model shows a monomer of the voltage-independent inward rectifying Kir2.1 potassium channel α subunit encoded by KCNJ2. The gene is expressed in skeletal and cardiac muscle. Loss-of-function mutations cause the Andersen syndrome
Dyskalemic periodic paralysis caused by KCNE3/MiRP2 alteration?
In 2001, an R83H substitution in a K+ channel beta subunit, MiRP2, was suggested as the cause of dyskalemic periodic paralysis because it showed a loss of function in vitro and was found in 2 of 100 of such patients but in none of 120 unaffected controls [1]. By later studies, the substitution was identified in 1 of 104 and 1 of 138 patients, but also in 8 of 506 and 3 of 321 controls [10, 21]. Taken together, the substitution is present in 1.17% of patients and in 1.16% of healthy controls, which does not support disease causality and shows that the common lab practice to exclude a novel mutation in approximately 100 healthy controls is insufficient. The number of controls required to prove disease causality of a putative mutation can be calculated a simple algorithm [10]. Even though the difference between defining a putative mutation as being truly disease-causing or as being a functional polymorphism may seem only marginal on a scientific level, this difference in definition has drastic consequences for an affected carrier whose diagnosis is made or confirmed by the finding and who is being medically treated. This problem will increasingly need to be addressed in future studies when the number of known mutations and putatively associated phenotypes continues to increase.
Rationale for the therapy of the periodic paralyses
In hyperkalemic PP, physiological membrane depolarization can be prevented by avoiding potassium-retaining medications, potassium-rich foods, fasting, strenuous work, and exposure to cold. At the beginning of a paralytic attack, the serum potassium level can be reduced by stimulation of the sodium-potassium pump, e.g. by continuous mild exercise or ingestion of carbohydrates or inhalation of salbutamol. It is often advisable to stabilize serum potassium levels at the low normal range by thiazide diuretics. Carbonic anhydrase inhibitors are the second choice and may be effective via myoplasmic acidification [14].
In hypokalemic PP, all substances which decrease serum potassium levels either by shifting potassium into the cells or by excretion by the kidney should be prevented: high carbohydrate meals, high sodium meals, bicarbonate and potassium-lowering diuretics, sedentary lifestyle and strenuous physical exercise. Attacks of generalized paralysis should be treated orally with potassium chloride. Intravenous potassium administration should be restricted to patients with severe tetraplegia treated in an intensive care unit. Carbonic anhydrase inhibitors are the prophylactic medication of choice. Potassium-sparing diuretics, such as triamterene, amiloride, and spironolactone may be administered in addition. Particularly patients with a chronic progressive myopathy should be treated as long as muscle is conserved even though the effect of the drugs on the course of the disease is unknown. Why carbonic anhydrase inhibitors can provoke muscle weakness in some patients has to be elucidated [14].
In Andersen syndrome, the most important task is to find out whether the cardiac arrhythmia is potentially fatal or not. Drugs or provocative tests which induce hypokalemia can provoke ventricular tachycardia and must be avoided. Patients with former syncopes and bursts of ventricular tachycardia in the resting condition or in Holter ECG recordings are at high risk. Such symptoms and signs may demand the implantation of a defibrillator or a pacemaker or both. An important rule for drug administration is to treat the patient and not the ECG. Some ECG changes may vanish under conditions at which action potentials are shortened due to tachycardia, e.g. during exercise or increased body temperature. Stabilization of serum potassium in the middle of the normal range may be an effective prophylactic treatment for preventing both arrhythmia and paralytic attacks [14]. It has to be clarified whether carbonic anhydrase inhibitors help to prevent attacks of weakness.
Conclusions
The periodic paralyses were commonly considered to be benign diseases indicating that regularly occurring specific morphological changes were not to be expected in persons at age under 45 years. One reason may be directly concluded from the fact that symptoms up to this age occur only episodically with varying intervals of normal muscle function and excitation in between. Apparently, the ion channel defects are usually well-compensated and an additional, special endogenous or exogenous trigger is required for malfunction to become apparent. With increasing age, a portion of the patients develops permanent weakness especially of the hands and the lower extremities and vacuolar muscle degeneration with fatty replacement may be found histologically and in the MRI.
Spontaneous attacks of paralysis or permanent weakness drastically reduce the patient’s ability to perform activities of daily living. For many patients disruption of their jobs and social and family relationships is more distressing than physical powerlessness. The inherent hazard of a cardiac arrhythmia aggravates the situation in patients with Andersen syndrome who may experience a life-threatening ventricular arrhythmia independent of paralysis. Only about 60 % of the patients who present with periodic paralysis, arrhythmia, and dysmorphic features carry a mutation in the KCNJ2 gene. The remaining patients are supposed to have an Andersen-like syndrome and to carry a mutation in a so far unidentified gene.
In the past, provocative tests have been carried out for diagnostic reasons. As they have harboured the risk of inducing a severe attack they had to be performed by an experienced physician and a stand-by anesthesiologist, and the serum potassium and glucose levels and the ECG had to be closely monitored. Nowadays, provocative tests should be restricted to patients in whom molecular genetics have failed to identify the mutation underlying the disease. Since histological alterations are not specific, a muscle biopsy should only be performed in patients with atypical features or documentation of a vacuolar myopathy.
References
Abbott GW, Butler MH, Bendahhou S, Dalakas MC, Ptacek LJ, Goldstein SA (2001) MiRP2 forms potassium channels in skeletal muscle with Kv3.4 and is associated with periodic paralysis. Cell 104:217–231
Andelfinger G, Tapper AR, Welch RC, Vanoye CG, George AL Jr, Benson DW (2002) KCNJ2 mutation results in Andersens syndrome with sex-specific cardiac and skeletal muscle phenotypes. Am J Hum Genet 71:663–668
Bendahhou S, Donaldson MR, Plaster NM, Tristani-Firouzi M, Fu YH, Ptacek LJ (2003) Defective potassium channel Kir2.1 trafficking underlies Andersen-Tawil syndrome. J Biol Chem 278:51779–51785
Fontaine B, Khurana TS, Hoffman EP, Bruns GAP, Haines JL, Trofatter JA, Hanson MP, Rich J, McFarlane H, McKenna-Yacek D, Gusella JF, Brown RH (1990) Hyperkalemic periodic paralysis and the adult muscle sodium channel alpha-subunit gene. Science 250:1000–1002
Fontaine B, Vale-Santos JE, Jurkat-Rott K, Reboul J, Plassart E, Rime CS, Elbaz A, Heine R, Guimaraes J, Weissenbach J, Baumann N, Fardeau M, Lehmann-Horn F (1994). Mapping of the hypokalaemic periodic paralysis (HypoPP) locus to chromosome 1q31–32 in three European families. Nature Genet 6:267–272
Hayward LJ, Brown RH Jr, Connon SC (1996) Inactivation defects caused by myotonia-associated mutations in the sodium channel III-IV linker. J Gen Physiol 107:559–576
Jurkat-Rott K, Lehmann-Horn F, Elbaz A, Heine R, Gregg RG, Hogan K, Powers P, Lapie P, Vale-Santos JE, Weissenbach J, Fontaine B (1994) A calcium channel mutation causing hypokalemic periodic paralysis. Hum Mol Gen 3:1415–1419
Jurkat-Rott K, Uetz U, Pika-Hartlaub U, Powell J, Fontaine B, Melzer W, Lehmann-Horn F (1998) Calcium currents and transients of native and heterologously expressed mutant skeletal muscle DHP receptor α1 subunits (R528H). FEBS Lett 423:198–204
Jurkat-Rott K, Mitrovic N, Hang C, Kuzmenkin A, Iaizzo P, Herzog J, Lerche H, Nicole N, Vale-Santos J, Chauveau D, Fontaine B, Lehmann-Horn F (2000) Voltage sensor sodium channel mutations cause hypokalemic periodic paralysis type 2 by enhanced inactivation and reduced current. Proc Natl Acad Sci USA 97:9549–9554
Jurkat-Rott K, Lehmann-Horn F (2004) Periodic paralysis mutation MiRP2-R83H in controls: interpretations and general recommendation. Neurology 62:1012–1015
Kuzmenkin A, Muncan V, Jurkat-Rott K, Hang C, Lerche H, Lehmann-Horn F, Mitrovic N (2002) Enhanced inactivation and pH sensitivity of Na+ channel mutations causing hypokalemic periodic paralysis type II. Brain 125:835–843
Lehmann-Horn F, Kuther G, Ricker K, Grafe P, Ballanyi K, Rüdel R (1987) Adynamia episodica hereditaria with myotonia: A non-inactivating sodium current and the effect of extracellular pH. Muscle Nerve 10:363–374
Lehmann-Horn F, Jurkat-Rott K (1999) Voltage-gated ion channels and hereditary disease. Physiol Rev 79:1317–1371
Lehmann-Horn F, Rüdel R, Jurkat-Rott K (2004) Chapter 46: Nondystrophic myotonias and periodic paralyses. In: Engel AG, Franzini-Armstrong C (ed) Myology. McGraw-Hill, New York, 3rd edition, pp 1257–1300
Morrill JA, Cannon SC (1999) Effects of mutations causing hypokalaemic periodic paralysis on the skeletal muscle L-Type Ca2+ channel expressed in Xenopus laevis oocytes. J Physiol (London) 520:321–336
Plaster NM, Tawil R, Tristani-Firouzi M, Canun S, Bendahhou S, Tsunoda A, Donaldson MR, Iannaccone ST, Brunt E, Barohn R, Clark J, Deymeer F, George AL Jr, Fish FA, Hahn A, Nitu A, Özdemir C, Serdaroglu P, Subramony SH, Wolfe G, Fu YH, Ptáček LJ (2001) Mutations in Kir2.1 cause the developmental and episodic electrical phenotypes of Andersen’s syndrome. Cell 105:511–519
Rojas CV, Wang J, Schwartz L, Hoffman EP, Powell BR, Brown RH Jr (1991) A Met-to-Val mutation in the skeletal muscle sodium channel -subunit in hyperkalemic periodic paralysis. Nature 354:387–389
Rüdel R, Lehmann-Horn F, Ricker K, Küther G (1984) Hypokalemic periodic paralysis: in vitro investigation of muscle fiber membrane parameters. Muscle Nerve 7:110–120
Ruff RL (1999) Insulin acts in hypokalemic periodic paralysis by reducing inward rectifier K+ current. Neurology 53:1556–1563
Sansone V, Griggs RC, Meola G, Ptáček LJ, Barohn R, Iannaccone S, Bryan W, Baker N, Janas SJ, Scott W, Ririe D, Tawil R (1997) Andersens syndrome: a distinct periodic paralysis. Ann Neurol 42:305–312
Sternberg D, Tabti N, Fournier E, Hainque B, Fontaine B (2003) Lack of association of the potassium channel-associated peptide MiRP2-R83H variant with periodic paralysis. Neurology 61:857–859
Struyk AF, Scoggan KA, Bulman DE, Cannon SC (2000) The human skeletal muscle Na channel mutation R669H associated with hypokalemic periodic paralysis enhances slow inactivation. J Neurosci 20:8610–8617
Tawil R, Ptáček LJ, Pavlakis SG, DeVivo DC, Penn AS, Özdemir C, Griggs RC (1994) Andersens’s syndrome: potassium-sensitive periodic paralysis, ventricular ectopy, and dysmorphic features. Ann Neurol 35:326–330
Tristani-Firouzi M, Jensen JL, Donaldson MR, Sansone V, Meola G, Hahn A, Bendahhou S, Kwiecinski H, Fidzianska A, Plaster N, Fu YH, Ptáček LJ, Tawil R (2002) Functional and clinical characterization of KCNJ2 mutations associated with LQT7 (Andersens syndrome). J Clin Invest 110:381–388
Venance SL, Cannon SC, Fialho D, Fontaine B, Hanna MG, Ptacek LJ, Tristani-Firouzi M, Tawil R, Griggs RC, CINCH investigators (2006) The primary periodic paralyses: diagnosis, pathogenesis and treatment. Brain 129:8–17
Vicart S, Sternberg D, Fournier E, Ochsner F, Laforet P, Kuntzer T, Eymard B, Hainque B, Fontaine B (2004) New mutations of SCN4A cause a potassium-sensitive normokalemic periodic paralysis. Neurology 63:2120–2127
Wagner S, Lerche H, Mitrovic N, Heine R, George AL, Lehmann-Horn F (1997) A novel sodium channel mutation causing a hyperkalemic paralytic and paramyotonic syndrome with variable clinical expressivity. Neurology 49:1018–1025
Weber M-A, Nielles-Vallespin S, Essig M, Jurkat-Rott K, Kauczor H-U, Lehmann-Horn F (2006) Muscle Na+ channelopathies: MR1 detects intracellular 23Na accumulation during episodic weakness. Neurology 67:1151–1158
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jurkat-Rott, K., Lehmann-Horn, F. Paroxysmal muscle weakness - the familial periodic paralyses. J Neurol 253, 1391–1398 (2006). https://doi.org/10.1007/s00415-006-0339-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-006-0339-0