
Abstract
Sex estimation is a task of utmost importance in forensic anthropology and bioarcheology. Along with the pelvic bone, the skull is the most important source of sexual dimorphism. On the human skull, the upper third of the face (i.e., the frontal bone) is one of the most significant sexually dimorphic structures useful in anthropological research, especially when studied by methods of virtual anthropology. This study was focused on sex estimation using the form and shape of the external surface of the frontal bone with or without the inclusion of its sinuses. The study sample consisted of 103 cranial CT images from a contemporary Czech population. Three-dimensional virtual models of the frontal bones and sinuses were analyzed using geometric morphometrics and multidimensional statistics: coherent point drift-dense correspondence analysis (CPD-DCA), principal component analysis (PCA), and support vector machine (SVM). The whole external frontal surface was significantly different between males and females both in form and shape. The greatest total success rate of sex estimation based on form was 93.2%, which decreased to 86.41% after crossvalidation, and this model identified females and males with the same accuracy. The best estimation based on shape reached a success rate of 91.26%, with slightly greater accuracy for females. After crossvalidation, however, the success rate decreased to 83.49%. The differences between sexes were significant also in the volume and surface of the frontal sinuses, but the sex estimation had only 64.07% accuracy after crossvalidation. Simultaneous use of the shape of the frontal surface and the frontal sinuses improved the total success rate to 98.05%, which decreased to 84.46% after crossvalidation.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Assessing the biological profiles of individuals is a necessary challenge in forensic anthropology, paleoanthropology, paleodemography, and bioarcheology. Sex estimation is one of the first and important steps in analyses of forensic or archeological contexts [1,2,3]. The most significant intersexual differences on the human skeleton are found on the pelvic bone. They provide reliable sex estimation thanks to the marked manifestation of sexually dimorphic traits and low population specificity [4,5,6]. However, the skull, too, bears sexually dimorphic skeletal elements. Compared with the pelvis, the skull exhibits a lower level of sexual dimorphism whose expressions are population-specific. On the other hand, the skull is more resistant to damage and better maintained by the body [2, 7,8,9]. Some authors regard the skull as the second best bone structure for sex estimation [10,11,12].
The sex of an individual can be estimated using visual and morphometric methods. Visual methods are based on the observation and scoring of sexually dimorphic areas [13, 14] and have been criticized for their high subjectivity [15]. In one of the best known systems for estimating sex, five traits (on the glabella, orbital margins, mastoid process, nuchal crest, and mental eminence) are evaluated in accordance with published standards [14, 16,17,18,19]. Morphometric techniques facilitate the evaluation of differences in the size of structures and provide greater objectivity [5, 20]. An important turn for quantitative methods came with progress in statistical analysis and the development of new methods based on discriminant functions [21,22,23]. In the last few years, the use of geometric morphometrics and three-dimensional quantitative tools has been on the increase. Sexual diagnosis may be performed using measurements [24], a set of landmarks [25, 26], curves [27], the external surface [28], or roundness [29]. The exocranial surface exhibits highly significant intersexual differences and sex estimation based on it has achieved high success rates. In the French population, the application of this method has resulted in 90.3% of correctly estimated individuals after crossvalidation [28]. The results of sex estimation based on the skull were improved further by the inclusion of both the exocranial and the endocranial surface [30].
One of the cranial regions with great potential for the study of sexual dimorphism is the frontal bone [14, 24, 31]. It carries a large number of sexually dimorphic areas. Besides the glabella, which is the most dimorphic and reliable part of the human skull [13, 19], there are also other sexually specific traits that are important for sexual diagnosis. Sex estimation based on certain frontal features can be done by scoring and then sorting these scores into categories previously defined based on shape and size differences [14, 17, 32]. Morphometric studies have especially dealt with the expansion of the supraorbital structure [14, 24, 33, 34]. Three-dimensional quantification of supraorbital structure allowed the successful estimation of 80% of individuals [33] and one shape study of lateral X-ray images was successful in 84% of cases [26]. Relatively few studies have dealt with the overall shape of the frontal bone or the curvature of the forehead [27, 29]. Forehead inclination and superciliary areas have been assessed using curves with greater success in females (88%) than in males (70%) [27]. A landmark-free method comparing the roundness of the frontal bone towards the surface of the sphere correctly estimated 77.5% of individuals [29]. The morphology of the frontal bone varies depending on the origin of the individual [10].
Inside the frontal bone, there is a pneumatized cavity. It is part of the paranasal sinuses of the head. The paranasal sinuses are air-filled spaces within the bones of the skull. They are formed by the lateral nasal wall and lined with a ciliated pseudostratified columnar respiratory epithelium that is the same as in the lower airways. The paranasal sinuses consist of the maxillary, frontal, sphenoid, and ethmoid sinuses. They have various functions such as lightening the weight of the head, heating and humidifying inhaled air, and increasing the resonance of speech [35,36,37]. The frontal sinuses are paired and irregularly shaped. They extend from the pars nasalis upward and laterally into the squama frontalis [38, 39]. The right and left part develop independently of each other [40]. Human frontal sinuses are characterized by great variability and asymmetry and are unique to every individual. Their shape, size, and location are influenced, among other factors, by population specificity. A study of the Turkish population found hyperplastic sinuses to be the most common type [41]. Nevertheless, another study identified intermediate or hypoplastic sinuses as the most common. The different variants in the appearance of the sinuses are related also to the closure of the sutura metopica or its persistence. Individuals with sutura metopica were found to have significantly more sinuses with aplasia or hypoplasia [42]. High variability is evident between monozygotic twins [43]. In forensic anthropology, frontal sinuses, because of their specificity, are primarily used for personal identification [44,45,46]. With regard to the influence of sex on the appearance of the structure, some studies have also focused on the study of sexual dimorphism and sex estimation using the frontal sinuses [47,48,49,50]. One advantage of this structure for the identification of individuals and the estimation of their sex lies in its very strong resistance to trauma and high probability of staying intact during mass catastrophes and accidents [51]. Previous works have found significant intersexual differences in the volume or dimensions of the frontal sinuses. However, the accuracy of these methods is relatively low. It ranges from about 63 to 77% [49, 50, 52,53,54,55]. Some studies have revealed that age has a relevant influence on sex estimation [52, 53]. Nevertheless, age has not been found to influence sex estimation using the volume of the frontal sinuses [54].
Our study uses the external surface of the skull, which has proved itself as a highly successful sexual classifier of the whole human skull [28]. The aims of this study were (1) to determine the sexual dimorphism of the external and internal surfaces of the frontal bone and (2) to utilize these results in the assessment of their separate and combined accuracy when incorporated into a sex estimation method.
Materials and methods
Materials
The study was based on cranial computed tomography (CT) images of 103 adult individuals. The sample consisted of a contemporary Czech population of 45 females and 58 males. Characteristics of the Czech sample by age and sex are presented in Table 1. The CT scans of patients aged 21 to 84 years were captured at the Department of Radiology at the Na Homolce Hospital in Prague for medical reasons that had not influenced the morphology of the skull and the frontal bones included in the study had no skeletal pathology. The imaging was performed using a CT Somatom Definition Flash 2x128 machine (Siemens, Erlangen Germany) with the following parameters: cut distance 0.6 mm; 0.4 mm kernel bone tissue H60 (reconstructive computational algorithm for bone tissue). The data used were collected and anonymized by an experienced radiologist with the approval of the ethics committee of the Na Homolce Hospital. Every technical question and problem was consulted with him. All individuals gave their informed consent with the CT imaging and the use of their data for research purposes.
Methods
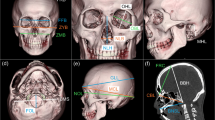
The first step was the preparation of the material (Fig. 1). The whole set of skull CT images was checked with the assistance of an experienced radiologist. All the frontal bones were without deformities and pathologies, so all were included in the study. The CT scans were converted to surface data using the tools of Morphome3cs (www.morphome3cs.com) [56, 57]. The obtained digital skull models were exported into the MeshLab software (Visual Computing Lab, Italian National Research Council) for simplification and the removal of parts of the skull which were not used in the analysis. The external surface of the frontal bone was cut along the commissures: sutura frontonasalis, sutura frontomaxilaris, sutura frontozygomatica, sutura sphenofrontalis, and sutura coronalis. In each specimen, two surfaces were prepared for further analysis: (a) the exterior surface of the frontal bone and (b) the frontal sinuses.

Process of the segmentation of the frontal bone and the frontal sinus from a CT scan
The frontal bone surface was manually trimmed by a trained anthropologist. The interior surface, sinuses, and any segmentation artifacts were removed. The remaining exterior surface was simplified to approx. 10,000 vertices. A set of six landmarks was placed on the frontal bone: bregma, nasion, frontotemporale dx et sin, frontomalare dx et sin.
The sinuses were extracted by manually removing the inner and outer surface of the frontal bone. Segmentation artifacts caused by noise were removed using automatic tools. Hole filling was utilized to produce closed surfaces, which are necessary for calculating volume.
Surface processing was performed in MeshLab and RapidForm XOS 2006 (INUS Technology Inc.). Landmarks were placed by a trained anthropologist in Morphome3cs.
The external surface of the frontal bone was analyzed in Morphome3cs using methods of geometrics morphometrics, which allow to describe surfaces using triangular meshes. Before statistical processing, vertex homology had to be ensured. CPD-DCA [58] was used to produce homologous representations of the surfaces under study. This method uses an automatic non-rigid registration algorithm to fit each shape on to a template which is arbitrarily chosen from the sample. Next, closest point search is used to transfer the topology of the registered template to all other surfaces. After this treatment, the surfaces can be processed using well-established methods of geometric morphometrics. Generalized Procrustes analysis (GPA) was used to normalize the shapes in terms of their location, orientation, and size. Forms were created the same way as shapes, except that size was not normalized. Mean shapes (forms) of male and female frontal bones were calculated by computing mean landmark (surface vertex) configurations of respective surfaces after GPA. Color maps visualizing differences in mean configurations were constructed by color-coding the distances of the vertices from the mean male and female surfaces. Significance maps were constructed by running unpaired two-sample Hotelling’s T2 tests on the coordinates of corresponding vertices, treating males and females as separate samples. The p values from these per-vertex Hotelling tests were color-mapped on to the mean surface. These visualizations were produced using the tools of Morphome3cs.
In surfaces capturing the frontal sinuses, volume and surface were calculated in MeshLab. These quantities were compared for both samples (males and females) using the two-sample t test or Mann-Whitney’s U test, depending on whether violation of normality was detected. Normality was checked using the Shapiro–Wilk test. These statistics were calculated in PAST. Significance was decided at the level of α = 0.05.
Finally, sex estimation based on the shape or form of the exterior frontal bone surfaces and the surface area and volume of the frontal sinuses was performed. Because the number of vertices of the frontal surfaces was very high, dimension reduction was performed using principal component analysis (PCA). Sex estimation was performed by fitting support vector machines (SVM) on to the combinations of the following variables:
- (a)
Principal component scores of frontal bone external surfaces (shape)
- (b)
Principal component scores of frontal bone external surfaces (form)
- (c)
Surface area and volume of the frontal sinuses
In the cases of (a) and (b), an optimal count of PC score variables was chosen in order to maximize the crossvalidation success rate and leave-one-out crossvalidation was performed to detect overfitting. This step was performed in Morphome3cs.
Results
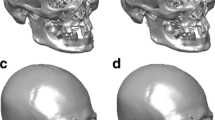
Differences between the sexes in the form and shape of the external surface of the frontal bone were visualized using color maps (Fig. 2a, c) and maps of significance (Fig. 2b, d). In the form analysis (Fig. 2a), red represents areas which were larger and more prominent in males whereas larger and more prominent morphological features in females are depicted in blue. In maps of significance (Fig. 2b), shades of blue represent statistically significant local sexual dimorphic areas. Sexual dimorphism indicating males was found in the lower region of the frontal bone—the glabella and superciliary arches. Upwards towards the squama frontalis, male eminence decreased slightly in comparison with the female bone. In the middle of the squama around the tubera frontalia, there was an opposite prominence pattern in females. The parts located above this middle section turned again to positive values, which are marked in the maps in tones of yellow, orange, to dark red, indicating the gradually increasing eminence of the frontal bone in males, with a peak along the sutura coronalis, which exhibits distinct prominence in contrast to females. The form of the surface of the frontal bone, except for its middle part, differed significantly between the sexes. This area was highly significant, with a significance level of less than 0.001 (Fig. 2b).

Visualized sexual differences between males and females in form and shape. Form: a the scale describes size differences in millimeters, red represents the most prominent areas that are larger in males in comparison to females; b the scale evaluates p values, darker colors indicate lower p values and higher significance. Shape: c the scale describes relative differences, red represents the most prominent areas in males in comparison to females; d the scale evaluates p values, darker colors indicate the lower p values and higher significance
Sexual dimorphism was visualized also for shape alone after size normalization. Dark red indicates extreme male shape variants and dark blue indicates female ones. However, these exceeding manifestations were not found in the shape analysis, but their milder expressions were still present (Fig. 2c). The lower part of the forehead, glabella and superciliary arches was more prominent in males also in shape. In the area around the tubera frontalia, there was a relatively large part of the squama which was more pronounced in females. The lateral sides posteriorly behind the linea temporalis were moderately concave in females. Contrariwise, increasing sharpness of the end part of the squama frontalis at the bregma was typical for males. The glabella, superciliary arches, the tubera frontalia region, and a narrow strip along the sutura coronalis were highly significant. The remaining parts of the frontal bone did not differ significantly in shape between the two sexes (Fig. 2d).
Sex estimation was carried out using the form and shape of the external surface of the frontal bone with or without the inclusion of its sinuses. Estimation using the external surface of the frontal bone was carried out with the help of scores of principal components. The optimum number of components used was selected on the basis of the crossvalidation success rate. The resulting accuracies, both posterior and crossvalidation, are presented in Figs. 3 and 4. The best estimation by form was achieved using the first 20 principal components. The greatest total success rate of sex estimation was 93.2% and 86.41% before and after crossvalidation, respectively (Fig. 3). This model was applicable to females and males with the same rate of success because individuals of both sexes were estimated with almost the same accuracy (Table 3).

Posterior and crossvalidation accuracies plotted against the number of principal components of form used

Posterior and crossvalidation accuracies plotted against the number of principal components of shape used
As in the case of form, the classifier for sex prediction was used for shape, too. The best results were achieved with 19 principal components. The total success rate was 91.26%, being slightly greater for females (93.33%) than for males (89.65%). After crossvalidation, the highest success rate based on shape decreased to 83.49% (Fig. 4), which was lower than in the case of form.
The frontal sinuses were evaluated using two markers—volume and surface. The testing of differences between the two sexes was performed based on the results of a Shapiro–Wilk normality test, which showed that volume did not have a normal distribution in the population. A Mann-Whitney U test was therefore employed. By contrast, surface had a normal distribution, and for this reason a two-sample t test was carried out. In the cases of both quantities, the frontal sinuses differed significantly between males and females (p = 0.001 for volume, p = 0.001 for surface). Table 2 presents the results of volume and surface measurements of the frontal sinuses according to sex. Minimum and maximum volume and surface values showed greater variability in males (range of volume from 457.84 to 45,134.04 mm3 and surface from 408.08 to 14,212.96 mm2) than in females (range of volume from 742.83 to 22,079.82 mm3 and surface from 1104.81 to 8566.19 mm2).
Sex estimation was carried out also based on the frontal sinuses (Table 3). Using their volume and surface, the highest total success rate reached 65.05%. The sex estimation achieved better results during the diagnosis of females. The less successful estimation of males could be explained by greater variability in the volume and surface of the frontal sinuses, as can be seen in Table 2. After crossvalidation, the accuracy was 64.07%.
The success of sex estimation was tested through the simultaneous use of the external surface of the frontal bone and the volume and surface of the frontal sinuses (Table 3). First, the estimation was carried out using both markers of the frontal sinuses together with the scores of principal components of the form of the external surface of the frontal bone. The total success rate reached 96.12%, which was an almost 3% better result than using only the form of the external surface of the frontal bone. However, after crossvalidation, this success rate decreased to 85.4%, which was not an improvement over the estimation using solely the frontal bone.
The total success rate of sex estimation using the volume and surface of the frontal sinuses together with the principal components of the shape of the frontal bone reached 98.05%, with the incorrect estimation of two males, though crossvalidation reduced its accuracy to 84.46%. Despite this marked decline, this is an almost 1% better result compared with the estimation based on the surface of the frontal bone after crossvalidation.
Discussion
This study was focused on the sex estimation of individuals using the external morphology of the frontal bone and the frontal sinuses by applying advanced methods of geometric morphometrics. Sex estimation using the external surface of the frontal bone methodologically builds on the research of Musilová et al. [28], who used the external surface of the whole human skull. Their results indicated that the frontal bone is one of the most sexually dimorphic cranial regions both in form and shape. According to their results pertaining to cranial form, the most significant is the lower region of the frontal bone—the glabella and superciliary arches. This conclusion is also supported by another study using the entire surface of the skull [30]. In shape, a significant difference was observed in the upper part of the bone, particularly between the frontal tubers [28]. These conclusions were confirmed by our significance testing, which verified the differences between male and female frontal bone surfaces. The form analysis showed that the most significant is the area of the glabella and superciliary arches, but also the lateral sides of the frontal bone and parts located along the sutura coronalis. All these regions, which were evaluated as statistically significant, are more distinctive and prominent in males [24, 33]. As concerns the shape of the frontal bone, our study demonstrates the significance of the middle part of the squama frontalis, including the frontal tubers, which indicate females, and the significance of the superciliary arches, glabella [26, 27, 31], superior margin of orbits [25], and the superior part of the frontal bone, which indicate males. We came to a consensus with the conclusions that skulls of females are full, rounded, and with a more vertical forehead, in contrast to males, whose foreheads are more inclined [10, 32, 59].
In the next part of our study, the sex estimation was tested using the form and shape of the external frontal surface. The greatest success rate of our method was 86.41% in form analysis, after leave-one-out crossvalidation. After crossvalidation, we achieved a success rate of 83.49% in the shape analysis. Our results indicate that the inclusion of size significantly increased the sex estimation accuracy, as confirmed by other studies dealing with form and shape [28, 30]. Compared with other studies evaluating the sexual dimorphism of the frontal bone, our estimation using the entire external surface of the frontal bone achieved slightly better results. The quantification of superciliary arches allowed correct estimation in 80% of cases after crossvalidation [33]. Sex estimation based on curves describing the curvature of the frontal bone, medially through the glabella and laterally through the most prominent point of the superciliary arches, yielded a success rate of 79%, which was considerably more successful at estimating females [27]. Contrariwise, our form-based method was an opportune tool for identifying the two sexes with the same precision, and in shape analysis females were estimated only slightly more successfully than males. Compared with the non-landmark method of evaluating the shape of the frontal bone against the curvature of a sphere [29], our estimation model achieved an almost 6% greater success rate. Our results are consistent with the conclusion of a previous study that assessed by geometric morphometrics the shape of the frontal bone from lateral X-rays of skulls, which reached a success rate of 84% [26].
By comparing the results of sex estimation of this study with others that estimated sex using a dataset of Czech individuals, we found our estimation model based on form to be slightly less successful. The most successful model based on upper face form achieved 91.1% of correctly classified individuals from the recent period, which is greater than our accuracy of 86.41%. However, our result is comparable with estimation using upper face form of individuals from the early modern Czech population which achieved a success rate of 87.5%. As concerns shape analysis, there is no marked difference between the estimation using the external surface of the frontal bone (83.49%) and the estimation using the shape of the upper face (83.3%). Nevertheless, the model based on the shape of the upper face of early modern individuals achieved only 70.3% of correctly classified individuals [60]. Sex estimation using the shape of mandibles of the contemporary Czech population achieved a success rate of 77.6% in males and 83.7% in females [61] which is lower than the prediction based on the external surface of the frontal bone.
Our estimation system will likely prove useful to other anthropologists, provided that their data are prepared in the same way. The preparation process, which can take about a day, included CT imaging, segmentation of the frontal bone from CT scans, surface analysis, and sex estimation. For anthropologists having computed tomography at their disposal, the application of this method will not be too complicated. CT images have recently been widely used in virtual anthropology. Surface models generated from volumetric CT data describe details (e.g., holes, cavities, or depressions) much more accurately than surface models acquired using a laser scanner. They correspond better to the real surface of the frontal bone [62].
Of course, the success rate of sex estimation is influenced by variability within the population [60, 61], but also by variability between populations. It is necessary to keep in mind that features on the skull are population-specific. The extent of this population specificity can be ascertained by applying our estimation system to other populations, be it temporally or geographically. The system should preferably be applied to geographically close populations from the same time period. For this reason, we plan to test our estimation model on other populations and to publish a sex classifier that any anthropologist will be able to use for sex estimation using a three-dimensional model of the frontal bone.
The main advantage of this approach is that the described method focuses only on the frontal bone, which is highly sexually dimorphic. Comparison of the discrimination utility of the frontal bone with that of other skull structures shows that the frontal bone is one of the most sexually dimorphic areas of the skull, along with the mandible [63, 64]. Areas of the processus mastoideus, foramen magnum, or condili occipitales provide sexual diagnostic tools with accuracy in the range of 65–76% [8, 21, 65, 66]. Importantly, the method deals with the entire external surface and not only with landmarks or dimensions. These two facts lend it high utility in estimating the sex of bone remains. This virtual technique enables the evaluation of all sexually dimorphic areas of the frontal bone in one step, which should improve the success rate of estimation compared with studying the individual parts separately. Nevertheless, compared with more traditional methods, sex estimation based on visual evaluation of the glabella resulted in an 82.6% success rate [14], which is not much different from our results. On the other hand, software processing and thus greater objectivity contributes to high-quality results. As far as practical matters are concerned, every method is time-consuming and requires sedulity and precision, and this approach is no exception. The question is how will the method be limited by the need for CT imaging and data processing, for example during mass deaths. One obvious disadvantage, which would be significant in cases of mass death, is the higher price of CT images.
Sex estimation in our study was carried out also using the volume and surface of the sinus frontalis. Significant differences between the two sexes were found in the volume and surface of the frontal sinuses, but the success rate of sex prediction using these criteria only reached 64.07% after crossvalidation. Similar decreases of discrimination success rates after crossvalidation are also reported in other works [55]. The low estimation accuracy was a consequence of high variability within the dataset. Our method estimated correctly 66.66% of females and 63.79% of males. The lower accuracy of estimation in males than females can be explained by the greater variability in volume and surface of the frontal sinuses of Czech males. Compared with other methods using the frontal sinuses for sex estimation, our result accomplished a similar level of success. Using the frontal sinus index, it was possible to distinguish the sexes from lateral X-ray scans with 67.5% accuracy [49] and from 3D models based on CT images with success in the range of 63–77% [50]. Sex discriminatory power of models based on volume was also verified in relation to age. This study demonstrated the possibility to discriminate between the sexes with a success rate of 72.5% without the negative impact of aging [54]. Besides volume, we also used the surface of the frontal sinuses to test the effect of adding another parameter. However, despite the use of the two markers, we achieved a lower level of accuracy. This can be explained by both high variability within the population and by population specificity because the original volume study was accomplished using a different population.
Finally, the simultaneous use of the external surface of the frontal bone and the volume and surface of the frontal sinuses was tested because the combination of these two parts had never been used for sex estimation. Estimation based on the form of the external frontal surface and the volume and surface of the frontal sinuses reached a total success rate of 96.12%, meaning that the total success rate for the frontal bone surface alone was improved by less than 3%. However, after crossvalidation, it dropped to 85.43% and did not improve the estimation based solely on the frontal bone. Associating the shape of the external surface of the frontal bone and the volume and surface of the frontal sinuses allowed the prediction of sex with 98.05% accuracy. Because of substantial interindividual variability, this high success rate decreased after crossvalidation. It might be interesting to apply this approach to a more extensive sample and to evaluate how sample size affects the accuracy of the estimation. Despite the drop in the success rate to 84.46% after crossvalidation, it is a better result by almost 1% than that achieved by the estimation model based solely on the shape of the frontal bone.
Conclusions
The described approach is an example of the successful use of geometric morphometrics and multidimensional statistics for analyzing sexual dimorphism in external morphology of the frontal bone and frontal sinuses in virtual anthropology and bioarcheology. In the contemporary Czech population, the external surface of the frontal bone offered the greatest success rate of 86.41% in form analysis and 2.92% lower accuracy in shape analysis. Using the shape of the external frontal surface together with the volume and surface of the frontal sinuses increased the success rate by about 0.97% compared with only using the shape of the external surface of the frontal bone. Studying the form of the external frontal surface, including analysis of the frontal sinuses, did not improve the success rate of the estimation.
References
Ferembach D, Schwidetzky I, Stloukal M (1980) Recommendations for age and sex diagnoses of skeletons. J Hum Evol 9:517–549
Spradley MK, Jantz RL (2011) Sex estimation in forensic anthropology: skull versus postcranial elements. J Forensic Sci 56:289–296
Guyomarc’h P, Bruzek J (2011) Accuracy and reliability in sex determination from skulls: a comparison of Fordisc® 3.0 and the discriminant function analysis. Forensic Sci Int 208:180.e1–180.e6
Bruzek J (2002) A method for visual determination of sex, using the human hip bone. Am J Phys Anthropol 117:157–168
Bruzek J, Murail P (2006) Methodology and reliability of sex determination from the skeleton. In: Schmitt A, Cunha E, Pinheiro J (eds) Forensic anthropology and medicine: complementary sciences from recovery to cause of death. Humana Press Inc., New Jersey, pp 225–242
Özer BK, Özer I, Sagir M, Gülec E (2014) Sex determination using the tibia in an ancient Anatolian population. Mediter Archaeol Archaeom 14:329–336
Kemkes-Grottenthaler A (2001) The reliability of forensic osteology – a case in point: case study. Forensic Sci Int 117:65–72
Gapert R, Black S, Last J (2009b) Sex detrmination from the foramen magnum: discriminant function analysis in an eighteenth and nineteenth century British sample. Int J Legal Med 123:25–33
Caple J, Stephan CN (2016) Photo-realistic statistical skull morphotypes: new exemplars for ancestry and sex estimation in forensic anthropology. J Forensic Sci 62:562–572
Krogman WM (1962) The human skeleton in forensic medicine. Charles C Thomas Publisher, Illinois
Pickering RB, Bachman D (2009) The use of forensic anthropology, Second edn. CRC Press, Boca Ranton
Byers SN (2015) Introduction to forensic anthropology, Fourth edn. Routledge, New York
Williams BA, Rogers TL (2006) Evaluating the accuracy and precision of cranial morphological traits for sex determination. J Forensic Sci 51:729–735
Walker PL (2008) Sexing skulls using discriminant function analysis of visually assessed traits. Am J Phys Anthropol 136:39–50
Petaros A, Garvin HM, Sholts SB, Schlager S, Wärmländer SK (2017) Sexual dimorphism and regional variation in human frontal bone inclination measured via digital 3D models. Legal Med 29:53–61
Lewis C, Garvin HM (2016) Reliability of the Walker cranial nonmetric method and implications for sex estimation. J Forensic Sci 61:743–751
Buikstra JE, Ubelaker DH (1994) Standards for data collection from human skeletal remains: proceedings of a seminar at the field museum of natural history, organized by Jonathan Haas. Arkansas Archeological Survey, Fayetteville
Langley NR, Dudzik B, Cloutier A (2018) A decision tree for nonmetric sex assessment from the skull. J Forensic Sci 63:31–37
Garvin HM, Sholts SB, Mosca LA (2014) Sexual dimorphism in human cranial trait scores: effects of population, age, and body size. Am J Phys Anthropol 154:259–269
Ousley S, Jantz R (2013) Fordisc 3: third generation of computer-aided forensic anthropology. Rechtsmedizin 23:97–99
Gapert R, Black S, Last J (2009a) Sex determination from the occipital condyle: discriminant function analysis in an eighteenth and nineteenth century British sample. Am J Phys Anthropol 138:384–394
Ogawa Y, Imaizumi K, Miyasaka S, Yoshino M (2013) Discriminant functions for sex estimation of modern Japanese skulls. J Forensic Legal Med 20:234–238
Lee UY, Kim IB, Kwak DS (2015) Sex determination using discriminant analysis of upper and lower extremity bones: new approach using the volume and surface area of digital model. Forensic Sci Int 253:135.e1–135.e4
Shearer BM, Sholts SB, Garvin HM, Wärmländer SKTS (2012) Sexual dimorphism in human browridge volume measured from 3D models of dry crania: a new digital morphometrics approach. Forensic Sci Int 222:400.e1–400.e5
Bigoni L, Velemínská J, Brůžek J (2010) Three-dimensional geometric morphometric analysis of cranio-facial sexual dimorphism in a Central European sample of known sex. HOMO 61:16–32
Perlaza NA (2014) Sex determination from the frontal bone: a geometric morphometric study. J Forensic Sci 59:1330–1332
Hochstein LAE (2014) The frontal bone as a proxy for sex estimation in humans: a geometric morphometric analysis. Master Thesis, Louisiana State University and Agricultural and Mechanical College
Musilová B, Dupej J, Velemínská J, Chaumoitre K, Bružek J (2016) Exocranial surfaces for sex assessment of the human cranium. Forensic Sci Int 269:70–77
Bulut O, Petaros A, Hizliol I, Wärmländer SKTS, Hekimoglu B (2016) Sexual dimorphism in frontal bone roundness quantified by a novel 3D-based and landmark-free method. Forensic Sci Int 261:162.e1–162.e5
Fatah A, Shirley N, Jantz R, Mahfouz M (2014) Improving sex estimation from crania using a novel three-dimensional quantitative method. J Forensic Sci 59:590–600
Dempf R, Eckert AW (2010) Contouring the forehead and rhinoplasty in the feminization of the face in male-to-female transsexuals. J Craniomaxillofac Surg 38:416–422
Keen JA (1950) A study of differences between male and female skulls. Am J Phys Anthropol 8:65–80
Garvin HM, Ruff CB (2012) Sexual dimorphism in skeletal browridge and chin morphologies determined using a new quantitative method. Am J Phys Anthropol 147:661–670
Rosas A, Bastir M (2002) Thin-plate spline analysis of allometry and sexual dimorphism in the human craniofacial complex. Am J Phys Anthropol 117:236–245
Dalgorf DM, Harvey RJ (2013) Sinonasal anatomy and function. Am J Rhinol Allergy 27:S3–S6
Negus V (1957) The function of the paranasal sinuses. JAMA Otolaryngol Head Neck 66:430–442
Reddy UDMA, Dev B (2012) Pictorial essay: anatomical variations of paranasal sinuses on multidetector computed tomography–how does it help FESS surgeons? Indian J Radiol Imaging 22:317–324
White TD, Folkens PA (2005) The human bone manual. Elsevier Academic Press, San Diego
Čihák R (2011) Anatomie 1, Third edn. Grada, Prague
Duque C, Casiano R (2005) Surgical anatomy and embryology of the frontal sinus. In: Kountakis SE, Senior BA, Draf W (eds) The frontal sinus. Springer, Berlin
Aslier NGY, Karabay N, Zeybek G, Keskinoglu P, Kirai A, Sütay S, Ecevit MC (2016) The classification of frontal sinus pneumatization patterns by CT-based volumetry. Surg Radiol Anat 38:923–930
Guerram A, Minor JML, Renger S, Guillaume B (2014) Brief communication : the size of the human frontal sinuses in adults presenting complete persistence of the metopic suture. Am J Phys Anthropol 154:621–627
Kjær I, Pallisgaard C, Brock-Jacobsen MT (2012) Frontal sinus dimensions can differ significantly between individuals within a monozygotic twin pair, indicating environmental influence on sinus sizes. Acta Otolaryngol 132:988–994
Quatrehomme G, Fronty P, Sapanet M, Grévin G, Bailet P, Ollier A (1996) Identification by frontal sinus pattern in forensic anthropology. Forensic Sci Int 83:147–153
Kim DI, Lee UY, Park SO, Kwak DS, Han SH (2013) Identification using frontal sinus by three-dimensional reconstruction from computed tomography. J Forensic Sci 58:5–12
Beaini TL, Duailibi-Neto EF, Chilvarquer I, Melani RFH (2015) Human identification through frontal sinus 3D superimposition: pilot study with cone beam computer tomography. J Forensic Legal Med 36:63–69
Lee MK, Sakai O, Spiegel JH (2010) CT measurement of the frontal sinus – gender differences and implications for frontal cranioplasty. J Craniomaxillofac Surg 38:494–500
Goyal M, Acharya AB, Sattur AP, Naikmasur VG (2013) Are frontal sinuses useful indicators of sex? J Forensic Legal Med 20:91–94
Sai Kiran C, Ramaswamy P, Khaitan T (2014) Frontal sinus index – a new tool for sex determination. J Forensic Radiol Imaging 2:77–79
Benghiac A, Thiel BA, Haba D (2015) Reliability of the frontal sinus index for sex determination using CBCT. Rom J Leg Med 23:275–278
da Silva RF, Prado FB, Caputo IGC, Devito KL, Botelho T d L, Júnior ED (2009) The forensic importance of frontal sinus radiographs. J Forensic and Legal Med 16:18–23
Belaldavar C, Kotrashetti VS, Hallikerimath SR, Kale AD (2014) Assessment of frontal sinus dimensions to determine sexual dimorphism among Indian adults. J Forensic Dent Sci 6:25–30
Akhlaghi M, Bakhtavar K, Moarefdoost J, Kamali A, Rafeifar S (2016) Frontal sinus parameters in computed tomography and sex determination. Legal Med 19:22–27
Michel J, Paganelli A, Varoquaux A, Piercecchi-Marti MD, Adalian P, Leonetti G, Dessi P (2015) Determination of sex: interest of frontal sinus 3D reconstructions. J Forensic Sci 60:269–273
Luo H, Wang J, Zhang S, Mi C (2018) The application of frontal sinus index and frontal sinus area in sex estimation based on lateral cephalograms among Han nationality adults in Xinjiang (accepted manuscript). J Forensic and Legal Med
Kotěrová A, Velemínská J, Dupej J, Brzobohatá H, Pilný A, Brůžek J (2016) Disregarding population specificity: its influence on the sex assessment methods from the tibia. Int J Legal Med 131:251–261
Dupej J, de Lázaro GR, Pereira-Pedro AS, Píšová H, Pelikán J, Bruner E (2018) Comparing endocranial surfaces: mesh superimposition and coherent point drift registration. In: Bruner E., Ogihara N., Tanabe H. (eds) Digital Endocasts. Replacement of Neanderthals by Modern Humans Series. Springer, Tokyo
Dupej J, Krajíček V, Velemínská J, Pelikán J, Statistical mesh shape analysis with nonlandmark nonrigid registration. Poster presented at 12th Symposium on Geometry Processing; 9–11 Jul 2014, Cardiff, UK
Russell MD, Brown T, Garn SM, Giris F, Turkel S, İşcan MY, Oyen OJ, Jacobshagen B, Pietrusewsky M, Rightmire GP, Smith FH, Turner CH II, Živanović S (1985) The supraorbital torus: a most remarkable peculiarity. Curr Anthropol 26:337–360
Bejdová Š, Dupej J, Krajíček V, Velemínská J, Velemínský P (2017) Stability of upper face sexual dimorphism in central European populations (Czech Republic) during the modern age. Int J Legal Med 132:321–330
Bejdová Š, Krajíček V, Velemínská J, Horák M, Velemínský P (2013) Changes in the sexual dimorphism of the human mandible during the last 1200 years in Central Europe. HOMO 64:437–453
Brzobohatá H, Prokop J, Horák M, Jančárek A, Velemínský J (2012) Accuracy and benefits of 3D bone surface modelling: a comparison of two methods of surface data acquisition reconstructed by laser scanning and computed tomography outputs. Coll Anthropol 36:801–806
Giles E (1964) Sex determination by discriminant function analysis of the mandible. Am J Phys Anthropol 22:129–136
Gamba TDO, Alves MC, Haiter-Neto F (2016) Mandibular sexual dimorphism analysis in CBCT scans. J Forensic Legal Med 38:106–110
Kemkes A, Göbel T (2006) Metric assessment of the “mastoid triangle” for sex determination: a validation study. J Forensic Sci 51:985–989
Madadin M, Menezes RG, Al Dhafeeri O, Kharoshah MA, Al Ibrahim R, Nagesh KR, Ramadan SU (2015) Evaluation of the mastoid triangle for determining sexual dimorphism: a Saudi population based study. Forensic Sci Int 254:244.e1–244.e4
Funding
This research was supported by the Grant Agency of Charles University (project no. 1590218).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent was obtained from all individual participants from the contemporary Czech population included in the study.
This article does not contain any studies with animals performed by any of the authors.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Čechová, M., Dupej, J., Brůžek, J. et al. Sex estimation using external morphology of the frontal bone and frontal sinuses in a contemporary Czech population. Int J Legal Med 133, 1285–1294 (2019). https://doi.org/10.1007/s00414-019-02063-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-019-02063-8