
Abstract
The aim of this study was to compare the accuracy of the Demirjian method and the Demirjian method as revised by Willems for age estimation based on orthopantomograms from central southern Chinese Han population aged 8–16 years. Discrepancies between chronological and estimated ages were statistically evaluated by analyzing 1249 orthopantomograms from 603 girls and 646 boys. Using the Demirjian method, the mean age estimates underestimated chronological age by 0.03 years (p = 0.48) for girls and overestimated it by 0.03 years (p = 0.59) for boys; these differences with respect to chronological age were not statistically significant. In contrast, the Willems method underestimated chronological age by 0.54 years (p < 0.01) for girls and 0.44 years (p < 0.01) for boys; these differences with respect to chronological age were statistically significant. Compared to the Demirjian method, the overall mean absolute error generated using the Willems method was slightly higher (0.85 and 0.86 years, respectively). Since the Demirjian method was more accurate, we highly recommend that it should be applied when estimating dental age in the Chinese Han population. Further modifications of these two methods for populations from other regions and additional studies of other age groups are warranted.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Age estimation is often an imperative procedure in circumstances where chronological age (CA) is ambiguous, for example, in determining whether a child has reached the age of criminal responsibility during judicial proceedings or whether undocumented individuals have attained the age at which employment, marriage, adoption, or immigration is permitted [1,2,3]. Age estimation of unknown corpses and skeletal remains is also important in anthropological and forensic science [4] and can be helpful for diagnoses and treatment planning in clinical dentistry and orthodontics [5, 6].
CA estimation based on dental panoramic radiography is the most commonly age estimation method [7,8,9,10,11,12,13,14]. Dental calcification development is independent of somatic or sexual maturity, as it is genetically controlled, making it superior to other age estimation methods, such as skeletal indicators [15, 16]. The developmental stages of teeth, compiled by Demirjian in 1973 and revised in 1976 [5, 6], based on French-Canadian individuals is the most widely applied method, on account of its rationality, ease of application, and objectivity. Willems et al. [1] developed a modified version of Demirjian’s scoring system using a Belgian population, by simplifying the conversion steps. Some previous studies have reported that estimated dental age (DA) determined by the method of Willems was more accurate than that generated using the Demirjian method [3, 8, 17,18,19]; however, other studies have reached the opposite conclusion [20, 21].
Ethnic differences significantly influence the development of teeth [18, 20]. Data regarding the accuracy of the Demirjian and Willems methods are lacking for children from Hunan province in central southern China. Accordingly, the objective of this study was to analyze the suitability of the Demirjian and Willems methods for estimation of the CA of Han population children from central southern China.
Subjects and methods
Subjects
Orthopantomograms (n = 1249) for this study were randomly selected from those obtained from patients attending XiangYa Stomatological Hospital of Central South University in Hunan Province. Data were collected from January 2016 to November 2017. The children included were 603 girls and 646 boys (age range, 8–16 years). Samples were divided into nine groups according to CA (one group per year). The sex and age distributions of each group are presented in Table 1.
Selection criteria
The inclusion criteria were as follows: (1) children whose ethnic origin was of the Han population of Hunan province, (2) the orthopantomogram was clear and of high quality, (3) no history of medication or surgery that could affect the eruption and mineralization of the mandibular permanent teeth. The exclusion criteria were as follows: (1) orthopantomogram with missing mandibular permanent teeth on both sides of the mandible, except the third molar; (2) deciduous teeth remaining on the mandible; (3) orthopantomograms from children with systemic disease; (4) gross pathology or tumor in the mandible.
Prior to conducting our research, ethical approval was obtained from the ethics committee of XiangYa Stomatological Hospital and informed consent was provided by all individual participants included in the study, according to the Declaration of Helsinki.
DA estimation
The Demirjian method presents eight development stages of dental maturity, from initial mineralization (stage A) to root completion (stage H), for each of seven left permanent mandibular teeth [5]. Scores were given corresponding to the stage of each tooth and the sum of these scores was converted into DA, with reference to published conversion tables and/or percentile curves [5, 6]. The sum of the corresponding scores for each tooth directly represented the DA of a subject, according to Willems’ table [1]; there are separate tables for boys and girls. CA was obtained by subtracting the date of birth from the date of taking radiographs.
Statistical analyses
SPSS version 20.0 for Windows (IBM, Armonk, NY, USA) and MS Excel (Microsoft Office) were used for statistical analyses and data management. The Kolmogorov-Smirnov test was used to test the normal distributions of age differences, for each age group and sex. The paired t test was used to analyze the statistical significance of differences between the means of CA and DA by age group and sex. The Wilcoxon signed rank test was also applied to assess the significance of differences between CA and DA in some age groups where these exhibited non-normal distributions. The mean absolute error (MAE) was used to quantify the accuracies of the two methods [22]. A p value less than 0.05 was considered statistically significance.
Intra- and inter-observer reproducibility
All measurements were performed separately by two trained examiners, who were ignorant of sex and CA. To assess the intra- and inter-observer reproducibility of determination of Demirjian stage for each tooth, we calculated Cohen’s Kappa coefficient values. An independent set of 53 randomly selected orthopantomograms were re-examined after an interval of 3 weeks.
Results
Intra- and inter-observer reproducibility was satisfactory, with Kappa coefficients of 0.963 and 0.934, respectively. The mean CA of all the children was 12.04 ± 2.55 years (boys, 12.12 ± 2.59 years; girls, 11.94 ± 2.49 years).
The Demirjian method
For all samples, mean DA estimated using the Demirjian method was slightly higher (0.002 years) than mean CA; the difference was not statistically significant (p = 0.26). In addition, the differences between DA and CA for girls and boys were not statistically significant (p = 0.48 and p = 0.59, respectively). For girls, the mean DA was underestimated, with a mean difference of 0.03 years, while for boys, the mean DA was overestimated by 0.03 years (Table 6).
Comparisons of the accuracies in each age group for girls and boys are presented in Tables 2 and 3 and Fig. 1. For girls, the age difference most frequently observed was between 0 and 0.5 years and the largest under- and overestimation of age was 4.5 years. For boys, the age difference most frequently observed was between − 0.5 and 0.5 years and the largest under- and overestimations of age were 4.0 years. For both sexes, the mean difference between the CA and DA was < 1 year, apart from boys aged 16 years (1.21 ± 0.88 years). For girls, mean differences were only statistically significant in three age groups (8, 12, and 16 years), while for boys, there were statistically significant differences in five age groups (10, 12, 13, 14, and 16 years).

Bar graph of age differences distribution between chronological age and dental age using the Demirjian and Willems methods
The Willems method
For all samples, the mean DA estimated using the Willems method was underestimated with a mean difference of 0.49 years, which was a statistically significant difference (p < 0.001). The differences between DA and CA were also statistically significant for both girls and boys (p < 0.001). The mean DA was underestimated relative to the CA for both girls and boys, with mean differences of 0.54 and 0.44 years, respectively (Table 6).
Comparisons of the accuracy for each age group for both sexes are presented in Tables 4 and 5 and Fig. 1. For girls, the age difference most frequently observed was between 0.5 and 1.0 years and the largest under- and overestimations of age were 5.0 years and 3.5 years, respectively. For boys, the age difference most frequently observed was between 0 and 1.0 years, with the largest under- and overestimations of age 4.5 and 4.0 years, respectively. For girls, the mean differences between CA and DA were < 1.0 year in all age groups; however, they were closest to 1.0 year in the age groups 10, 11, and 16 years. For boys, the age differences were < 1.0 years in all groups except 15 and 16 years. For girls, the mean difference only lacked statistical significance in two age groups (12 and 15 years), while for boys, there was no statistically significant difference in three age groups (8, 12, and 13 years).
Comparison of results obtained using the Demirjian and Willems methods
For girls, the Willems method resulted in clear underestimation of CA compared with the Demirjian method for all age groups, except for girls aged 13 years; in this age group, both methods overestimated the mean CA. In addition, the Demirjian method overestimated the CA in the age groups 11, 12, and 14 years.
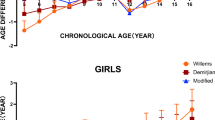
For boys, the Willems method underestimated the mean DA in all age groups except those aged 8 years, while the Demirjian method underestimated the mean DA in four age groups (9, 11, 15, and 16 years). Hence, both the Demirjian method and the Willems method resulted in more accurate estimation in lower, relative to higher, age groups for both sexes (Fig. 2).

Comparison of dental age between the Demirjian method and the Willems method by gender
The small difference in overall MAE between the two methods was not significant (Table 6); however, for girls, the MAE was higher when the Willems method was used (0.84 years vs. 0.72 years for the Demirjian method). The MAE was also higher than the Willems method for boys (0.88 years vs. 0.66 years for the Demirjian method).
Discussion
Age estimation of children has a significant role in forensic personal identification, clinical dentistry, and particularly in the determination of legal responsibility. In China, different age groups have different levels of criminal liability, for example, children < 14 years old do not have any criminal liability, those aged from 14 to 16 years should have some criminal liability, and on reaching the age of 16, individuals assume full criminal liability [23].
Dental maturity is a widely used indicator to evaluate dental development and it can also be used to estimate human age. The Demirjian method has been established for more than four decades (since 1973), and it has become the most popular method for estimation of DA [5]. Although the Demirjian method is precise when used for the reference population of French-Canadian individuals, the authors note that their system may not be accurate for other populations [5], and its inaccuracies have been reported in a number of publications [23,24,25,26,27,28,29,30]. A meta-analysis recently showed that the Demirjian method overestimated CA, with a weighted mean difference of 0.62 for males and 0.72 for females [19]. The Willems method, which is a modification of the Demirjian approach, has been the subject of a great deal of research interest, and a recent meta-analysis reported that the majority of studies using the Willems method did not report significant overestimation of age for either sex (0.26 and 0.29 for male and females, respectively) [19]. Nevertheless, some previous studies reported that the Willems method is inaccurate when used in various populations [31,32,33,34]. Hence, population-specific standards should be employed to achieve the most accurate age assessment, rather than a universal standard developed for use in other populations [19].
A total of 1249 panoramic radiographs, from children aged 8–16 years old, were finally chosen for use in estimation of the applicability of the two methods of DA estimation. Panoramic radiographs are rarely taken as routine dental radiographs for children below 8 years old in the clinic; therefore, no panoramic radiographs from children < 8 years old were included in the present study. Furthermore, the applicability of the Demirjian method is limited for estimation of ages > 16 years; hence, no panoramic radiographs from children > 16 years old were included.
In our study, the Demirjian method underestimated the age of girls and overestimated that of boys by 0.03 years in both cases. In contrast, the Willems method underestimated the ages of both girls and boys by 0.54 and 0.44 years, respectively. These data indicate that the Demirjian method is more accurate than the Willems method, contrary to the results of previous studies from other countries [8, 35,36,37,38,39]. For example, Maber et al. showed that the method of Willems was more accurate than the Demirjian method for estimation of the ages of children from London, United Kingdom, with the mean underestimations of 0.05 years for boys and 0.20 years for girls [8]. Grover et al. found that the Demirjian method overestimated DA by a greater degree (0.66 years for boys and 0.56 for girls) than the Willems method in North India [35]. Medina and Blanco reported the mean differences between DA and CA of 0.62 and 0.15 years for the Demirjian and Willems methods, respectively; their data showed that the Willems method for age estimation was more accurate than the Demirjian method in Venezuelan children [39]. However, another study reported that the Demirjian method was more accurate than the Willems approach, consistent with our findings, with an overestimation of 0.1 years for both sexes [20]. The divergence between our results and those reported for other populations is likely due to biological variation among children with different ethnic origins. In addition, sample size, age range, and the age distribution of the samples, and the statistical approach used, may also contribute to the observed differences.
There are 56 ethnic groups in China, which covers a large geographical territory comprising more than 20 provinces, and there may be differences in the growth and the development of children in different provinces of China. This explains why our results are inconsistent with those of previous studies comparing these two DA methods in other Chinese provinces [21, 22]. For example, Xiuxia Ye et al. tested the Demirjian and Willems methods in 941 children from southeastern China (Shanghai municipality) and reported that the Demirjian method clearly overestimated DA by 1.68 years for boys and 1.28 years for girls compared with the Willems method; they concluded that the Demirjian method was not accurate for use in southeastern Chinese children [22]. Although Yue Zhai et al. found that the Demirjian method was more accurate than the Willems method, consistent with our findings, the Demirjian method underestimated age, similar to the Willems method, by 0.47 and 0.63 years for boys and girls, respectively, in northern Chinese children [21]. Similarly, Tunc et al., Altunsoy et al., and Celikoglu et al. reported differences between geographical areas or cities within the same country (North, West, and East Turkey) [29, 40, 41].
Based on our findings, the smallest age differences for both of these two methods were observed in younger age groups, consistent with some previous studies [29, 41,42,43]. Hagg and Matsson reported that, among the various stages of development involved in DA estimation, those occurring in younger children were of shorter duration than those in older individuals; thus, the higher accuracy for young children may be attributable to the evaluation of a large number of stages with shorter durations [42]. The maximum age difference was observed in the oldest age group (16 years), particularly among boys. This may be due to the fact that, when the apical ends of the root canals of the seven left mandibular teeth close, the maximum maturity score in the table for conversion of the maturity score to DA was 98.4 for boys, rather than 100, and there is no means of more accurate dental scoring [8, 44]. Therefore, the age of any individual older than 16 years will be underestimated using this method; however, the generally reported observation that DA assessment for girls is more accurate than that for boys using these two methods was not confirmed by the present study [19, 20, 28, 44].
As this was a retrospective study of radiographs sampled from the patient records from the central southern Chinese Xiangya Stomatological Hospital in Hunan province of Central southern China, our results can only be considered representative of Chinese children in this region; therefore, the accuracy of the method requires verification in other districts of China. Moreover, the applicability of the method to other age groups, or its use with the inclusion of third molar data, warrants further study in the future.
Conclusions
According to our results, the standards developed by Demirjian are more appropriate for estimation of the DA of central southern Chinese children, compared with the Willems method; however, the method should be applied with caution for other age groups and we recommend further research to obtain more accurate results for examining groups of different ethnic and geographical origin.
References
Willems G, Van Olmen A, Spiessens B, Carels C (2001) Dental age estimation in Belgian children: Demirjian’s technique revisited. J Forensic Sci 46(4):893–895. https://doi.org/10.1520/JFS15064J
Patnana AK, Vabbalareddy RS, V Vanga NR (2014) Evaluating the reliability of three different dental age estimation methods in Visakhapatnam children. Int J Clin Pediatr Dent 7(3):186–191. https://doi.org/10.5005/jp-journals-10005-1262
Mani SA, Naing L, John J, Samsudin AR (2008) Comparison of two methods of dental age estimation in 7–15-year-old Malays. Int J Paediatr Dent 18(5):380–388. https://doi.org/10.1111/j.1365-263X.2007.00890.x
Tardivo D, Sastre J, Catherine J-H, Leonetti G, Adalian P, Foti B (2014) Age determination of adult individuals by three-dimensional modelling of canines. Int J Legal Med 128(1):161–169. https://doi.org/10.1007/s00414-013-0863-2
Demirjian A, Goldstein H, Tanner JM (1973) A new system of dental age assessment. Hum Biol 45(2):211–227
Demirjian A, Goldstein H (1976) New systems for dental maturity based on seven and four teeth. Ann Hum Biol 3(5):411–421. https://doi.org/10.1080/03014467600001671
Karkhanis S, Mack P, Franklin D (2014) Age estimation standards for a Western Australian population using the dental age estimation technique developed by Kvaal et al. Forensic Sci Int 235(104):e1–e6. https://doi.org/10.1016/j.forsciint.2013.12.008
Maber M, Liversidge HM, Hector MP (2006) Accuracy of age estimation of radiographic methods using developing teeth. Forensic Sci Int 159(Suppl 1):S68–S73. https://doi.org/10.1016/j.forsciint.2006.02.019
Rozyło-Kalinowska I, Kiworkowa-Raczkowska E, Kalinowski P (2008) Dental age in Central Poland. Forensic Sci Int 174(2–3):207–216. https://doi.org/10.1016/j.forsciint.2007.04.219
Chaillet N, Nyström M, Demirjian A (2005) Comparison of dental maturity in children of different ethnic origins: international maturity curves for clinicians. J Forensic Sci 50(5):1164–1174. https://doi.org/10.1520/JFS2005020
Vidisdottir SR, Richter S (2015) Age estimation by dental developmental stages in children and adolescents in Iceland. Forensic Sci Int 257(518):e519–e525. https://doi.org/10.1016/j.forsciint.2015.09.007
Leurs IH, Wattel E, Aartman IH, Etty E, Prahl-Andersen B (2005) Dental age in Dutch children. Eur J Orthod 27(3):309–314. https://doi.org/10.1093/ejo/cji010
Tóth ZO, Udvar O, Angyal J (2014) Chronological age estimation based on dental panoramic radiography. Fogorv Sz 107(3):93–98
Liversidge HM (2008) Dental age revisited. In: Irish JD, Nelson GC (eds) Technique and application in dental anthropology. Cambridge University Press, Cambridge, pp 234–252
Demirjian A (1985) Interrelationships among measures of somatic, skeletal, dental, and sexual maturity. Am J Orthod 88(5):433–438. https://doi.org/10.1016/0002-9416(85)90070-3
Al-Emran S (2008) Dental age assessment of 8.5 to 17 year-old Saudi children using Demirjian’s method. J Contemp Dent Pract 9(3):64–71
Ambarkova V, Galic I, Vodanovic M, Biocina-Lukenda D, Brkic H (2014) Dental age estimation using Demirjian and Willems methods: cross sectional study on children from the Former Yugoslav Republic of Macedonia. Forensic Sci Int 234:e181–e187. https://doi.org/10.1016/j.forsciint.2013.10.024
Djukic K, Zelic K, Milenkovic P, Nedeljkovic N, Djuric M (2013) Dental age assessment validity of radiographic methods on Serbian children population. Forensic Sci Int 231(1–3):e391–e398. https://doi.org/10.1016/j.forsciint.2013.05.036
Esan TA, Yengopal V, Schepartz LA (2017) The Demirjian versus the Willems method for dental age estimation in different populations: a meta-analysis of published studies. PLoS One 12(11):e0186682. https://doi.org/10.1371/journal.pone.0186682
Mohanmmed RB, Sanghvi P, Perumalla KK, Srinivasaraju D, Srinivas J, Kalyan US, Rasool SM (2015) Accuracy of four dental age estimation methods in southern Indian children. J Clin Diagn Res 9(1):HC01–HC018. https://doi.org/10.7860/JCDR/2015/10141.5495
Zhai Y, Park H, Han J, Wang H, Ji F, Tao J (2016) Dental age assessment in a northern Chinese population. J Forensic Legal Med 38:43–49. https://doi.org/10.1016/j.jflm.2015.11.011
Ye X, Jiang F, Sheng X, Huang H, Shen X (2014) Dental age assessment in 7-14-year-old Chinese children: comparison of Demirjian and Willems methods. Forensic Sci Int 244:36–41. https://doi.org/10.1016/j.forsciint.2014.07.027
Chen JW, Guo J, Zhou J, Liu RK, Chen TT, Zou SJ (2010) Assessment of dental maturity of western Chinese children using Demirjian’s method. Forensic Sci Int 197(1–3):119.e1–119.e14. https://doi.org/10.1016/j.forsciint.2009.12.009
Abu Asab S, Noor SN, Khamis MF (2011) The accuracy of Demirjian method in dental age estimation of Malay children. Singap Dent J 32(1):19–27. https://doi.org/10.1016/S0377-5291(12)70012-3
Lee SS, Kim D, Lee S, Lee UY, Seo JS, Ahn YW, Han SH (2011) Validity of Demirjian’s and modified Demirjian’s methods in age estimation for Korean juveniles and adolescents. Forensic Sci Int 211(1–3):41–46. https://doi.org/10.1016/j.forsciint.2011.04.011
Carneiro JL, Caldas IM, Afonso A, Cardoso HF (2015) Is Demirjian’s original method really useful for age estimation in a forensic context? Forensic Sci Med Pathol 11(2):216–221. https://doi.org/10.1007/s12024-015-9656-x
Hegde RJ, Khare SS, Saraf TA, Trivedi S, Naidu S (2015) Evaluation of the accuracy of Demirjian method for estimation of dental age among 6-12 years of children in Navi Mumbai: a radiographic study. J Indian Soc Pedod Prev Dent 33(4):319–323. https://doi.org/10.4103/0970-4388.165693
Mohammed RB, Srinivas B, Sanghvi P, Satyanarayana G, Gopalakrishnan M, Pavani BV (2015) Accuracy of Demirjian’s 8 teeth method for age prediction in South Indian children: a comparative study. Contemp Clin Dent 6(1):5–11. https://doi.org/10.4103/0976-237X.149283
Altunsoy M, Nur BG, Akkemik O, Ok E, Evcil MS (2015) Applicability of the Demirjian method for dental age estimation in western Turkish children. Acta Odontol Scand 73(2):121–125. https://doi.org/10.3109/00016357.2014.956333
Jayarman J, King NM, Roberts GJ, Wong HM (2011) Dental age assessment: are Demirjian’s standards appropriate for Southern Chinese children? J Forensic Odontostomatol 29(2):22–28
Galic I, Vodanovic M, Cameriere R, Nakas E, Galic E, Selimovic E, Brkic H (2011) Accuracy of Cameriere, Haavikko, and Willems radiographic methods on age estimation on Bosnian-Herzegovian children age groups 6-13. Int J Legal Med 125(2):315–321. https://doi.org/10.1007/s00414-010-0515-8
de Souza RB, da Silva Assuncao LR, Franco A, Zaroni FM, Holderbaum RM, Fernandes A (2015) Dental age estimation in Brazilian HIV children using Willems’ method. Forensic Sci Int 257(510):e511–e514. https://doi.org/10.1016/j.forsciint.2015.07.044
Onat Altan H, Altan A, Bilgic F, Akinci Sozer O, Damlar I (2016) The applicability of Willems’ method for age estimation in southern Turkish children: a preliminary study. J Forensic Legal Med 38:24–27. https://doi.org/10.1016/j.jflm.2015.11.015
Franco A, Thevissen P, Fieuws S, Souza PH, Willems G (2013) Applicability of Willems model for dental age estimations in Brazilian children. Forensic Sci Int 231(1–3):e401–e404. https://doi.org/10.1016/j.forsciint.2013.05.030
Grover S, Marya CM, Avinash J, Pruthi N (2012) Estimation of dental age and its comparison with chronological age: accuracy of two radiographic methods. Med Sci Law 52(1):32–35. https://doi.org/10.1258/msl.2011.011021
Urzel V, Bruzek J (2013) Dental age assessment in children: a comparison of four methods in a recent French population. J Forensic Sci 58(5):1341–1347. https://doi.org/10.1111/1556-4029.12221
Liversidge HM, Smith BH, Maber M (2010) Bias and accuracy of age estimation using developing teeth in 946 children. Am J Phys Anthropol 143(4):545–554. https://doi.org/10.1002/ajpa.21349
Jayaraman J, Wong HM, King NM, Roberts GJ (2013) The French-Canadian data set of Demirjian for dental age estimation: a systematic review and meta-analysis. J Forensic Legal Med 20(5):373–381. https://doi.org/10.1016/j.jflm.2013.03.015
Medina AC, Blanco L (2014) Accuracy of dental age estimation in Venezuelan children: comparison of Demirjian and Willems methods. Acta Odontol Latinoam 27(1):34–41
Tunc ES, Koyuturk AE (2008) Dental age assessment using Demirjia’s method on Northern Turkish children. Forensic Sci Int 175(1):23–26. https://doi.org/10.1016/j.forsciint.2007.04.228
Celikoglu M, Cantekin K, Ceylan I (2011) Dental age assessment: the applicability of Demirjian method in eastern Turkish children. J Forensic Sci 56(Suppl 1):S220–S222. https://doi.org/10.1111/j.1556-4029.2010.01598.x
Hagg U, Matsson L (1985) Dental maturity as an indicator of chronological age: the accuracy and precision of three methods. Eur J Orthod 7(1):25–32. https://doi.org/10.1093/ejo/7.1.25
Davis PJ, Hägg U (1994) The accuracy and precision of the “Demirjian system” when used for age determination in Chinese children. Swed Dent J 18(3):113–116
Tian X, Tan Y, Han B, Wang X, Feng H, Wang H, Wang J, Zhang J (2010) Gender difference of calcification in mandibular permanent teeth of the Chinese Han nationality groups aged 6 to 18 years old. Chin J Forensic Med 25(4):223–231
Funding
This research was supported by Natural Science Foundation of Hunan Province (2017JJ3422) and Shanghai Key Laboratory of Forensic Medicine Open Project (KF1815).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Ethical approval was granted by the ethics committee of XiangYa Stomatological Hospital.
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required.
Informed consent
Informed consent was provided by all individual participants included in the study, according to the Declaration of Helsinki.
Additional information
Ying Liu and Lagabaiyila Zha contributed equally to this article; they are joint corresponding author.
Rights and permissions
About this article

Cite this article
Yang, Z., Geng, K., Liu, Y. et al. Accuracy of the Demirjian and Willems methods of dental age estimation for children from central southern China. Int J Legal Med 133, 593–601 (2019). https://doi.org/10.1007/s00414-018-1924-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-018-1924-3