
Abstract
Palatal rugae are known in literature as individualizing anatomical structures with a strong potential for personal identification. However, a 3D assessment of their uniqueness has not yet been performed. The present study aims at verifying the uniqueness of 3D models of the palate. Twenty-six subjects were recruited among the orthodontic patients of a private dental office; from every patient, at least two dental casts were taken in different time periods, for a total of 62 casts. Dental casts were digitized by a 3D laser scanner (iSeries, Dental Wings©, Montreal, Canada). The palatal area was identified, and a series of 250 superimpositions was then performed automatically through VAM©software in order to reach the minimum point-to point distance between two models. In 36 matches the models belonged to the same individual, whereas in 214 mismatches they came from different subjects. The RMS (root mean square) of point-to-point distances was then calculated by 3D software. Possible statistically significant differences were assessed through Mann-Whitney test (p < 0.05). Results showed a statistically significant difference in RMS mean point-to-point distance between matches (mean 0.26 mm; SD 0.12) and mismatches (mean 1.30; SD 0.44) (p < 0.0001).All matches reached an RMS value below 0.50 mm. This study first provided an assessment of uniqueness of palatal rugae, based on their anatomical 3D conformations, with consequent applications to personal identification.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Palatal rugae are anatomical structures in the anterior portion of the palate, deriving from hard connective tissue covered by stratified epithelium. They are formed in utero in the third month and remain stable during the entire life, with the exception of an increase in length according to the normal growth [1].
Thanks to their stability during a lifetime, the analysis of palatal rugae is considered one of the most reliable methods for personal identification in cases of unknown decedents with relatively well preserved soft tissues, and particularly for edentulous individuals where no information from teeth can be recovered [2, 3].
With time, several studies have developed different approaches in order to assess anatomical uniqueness of palatal rugae. Some authors took morphological classifications of rugae into consideration, through the determination of shapes and coding systems [1, 4]. The accuracy of such a procedure reported by different authors is similar and ranges between 72 and 96% according to Adisa et al., [5] and 76.7–96.7% by Bansode and Kulkarni [6]. Experience of the observer proved to be an important factor, as the most experienced operators reached a higher level of correct identification [5].
Other methods took the superimposition of the silhouette of palatal rugae into consideration in order to verify a possible correspondence. Percentage of correct identification seems higher than results provided by the mere comparison and reaches 100% [7].
Possible advantages from automatic methods were explored as well: Hemanth et al. in 2010 tested a software for the automatic comparison of palatal rugae, after manual plotting of reference landmarks. Results showed that three evaluators reached a correct identification in 100% and two observers in 99% of cases [8]. The next step, as suggested by the authors, will be the development of a fully automatic method of comparison, without the residual manual procedure of landmarks plotting [8]. The exploration of automatic methods of comparison was performed also by Limson and Julian in 2004, who developed a software with a mean sensitivity of 0.93 and specificity of 1.00 and a 92–97% success rate [9].
All the previously described methods are based on the detection and comparison of 2D silhouettes of palatal rugae; however, in the last years, the development of modern 3D image acquisition systems allow operators to assess palatal rugae also in three dimensions. This approach has already been known and applied to other anatomical regions in the field of personal identification [10, 11].
The present article aims at testing differences between palatal scans of the same and different individuals in order to verify parameters useful for personal identification and thus test the truly discriminating potential of 3D images of palatal rugae.
Materials and methods
Twenty-six orthodontic patients (7 males and 19 females), aged between 15 and 20 years, without facial deformities, pathologies or signs of previous surgery, were randomly recruited among the patients of a private practice. The work was carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki) and local ethical rules. Informed consent was obtained from all patients or their legal tutors where necessary, and their privacy rights observed. All patients were retrospectively selected from a clinical database, and during the study, their casts were anonymized in order to meet international ethical standards. Their casts were obtained for clinical reasons uncorrelated with this study.
For each subject, at least two casts of the upper dental arch were available, including the palatal area. In detail, 19 patients had two dental casts, four patients had three dental casts and three subjects underwent four dental casts. In total, 62 dental casts were obtained. The time period elapsed between the two casts was between 6 and 48 months. Maxillary expansion treatment and other palatal modifications were excluded from the study.
A 3D model of each cast was obtained by a laser scanner (iSeries, Dental Wings, Montreal, Canada; precision 15 μm), and the palatal surface was identified and manually selected through a 3D image elaboration software (VAM®, Canfield Scientific Inc., Fig. 1). The obtained 3D models were then superimposed one on each other in order to obtain 250 superimpositions through the same VAM® software. Each model was superimposed on the model of the first cast belonging to the same individual, for a total of 36 matches (in cases of patients with two casts there was one match, in cases of patients with three and four casts respectively two and three matches).In addition, each cast was superimposed on the model of the first cast belonging to other individuals. Among all the possible 900 incorrect (between subjects) combinations, 214 mismatches were randomly selected in order to compare the results with the matches (within subject) group (Tables 1).

Example of a 3D-scanned digital model of the palatal area
The superimposition procedure was divided into two phases. In a first step, the palatal area including the rugae was manually selected. This was followed by an automatical procedure performed through VAM® software. In this second step, the superimposition was automatically performed in order to reach the best match between the entire surfaces of both the models. The procedure mathematically superimposes the 3D surfaces according to the least point-to-point distance between the two chosen 3D models.
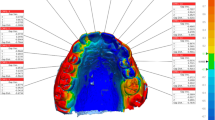
After the two models were registered, the software was requested to provide the point-to-point distance between the two surfaces, expressed as root mean square (RMS): this procedure provided also a chromatic map designed on the model of the second cast representing the areas of changes between the two scans, coloured in blue, green and red (Fig. 2). The entire procedure from 3D acquisition of dental casts to the RMS calculation was automatically performed but for the manual selection of palatal area including the rugae.

Chromatic representation of differences between two superimposed models: on the left, example of match (casts belonging to the same individual): one can observe the prevalence of green colour (unchanged areas); on the right, example of mismatch (casts belonging to different individuals): blue and red coloration describe areas of discordances between the two models
In addition, for ten comparisons the entire procedure from 3D acquisition of casts to the superimposition of the palatal surfaces and the assessment of RMS distance was repeated 2 weeks after the first evaluation by the same and another operator. Differences between the two observations performed by the same observer and by different observers were statistically analysed by paired Wilcoxon test (p < 0.05).
Mann-Whitney test was used for assessing possible statistically significant differences in RMS value between matches and mismatches. Significance level was set at 0.05.
Results
Inter- and intra-observer method errors for RMS values were not statistically significant (Wilcoxon test, p > 0.05).
The mean RMS values of point-to-point distances between the superimposed models was 0.26 mm (SD 0.12) when they belonged to the same individual, and 1.30 mm (SD 0.44) when superimpositions were made from different subjects. Differences were statistically significant (mean ranks of matches 18.5, mean ranks of mismatches 143.5, z 9.59, p < 0.0001). In the former case, the same parameter ranged between 0.04 and 0.49 mm, whereas in the latter case, it was included between 0.50 and 2.68 mm. In no case the values of matches and mismatches superimposed (Fig. 3): 0.50 mm was seen to be the threshold to distinguish matches from mismatches in this dataset (Table 2).

Dispersion of RMS values shown by the 250 comparisons: matches are indicated by the circle
Discussion
Palatal rugae are anatomical structures characterized by uniqueness and a high individuality. Most of the methods currently used in forensic practice for personal identification perform a 2D-2D superimposition through the comparison of the bidimensional projection of palatal rugae [12]. In the last years, the introduction of 3D image acquisition techniques has found novel applications in several fields of forensic odontology [13,14,15], including personal identification [16]. Therefore, it may represent an advantage for the development of novel methods of identification based on the anatomical uniqueness of palatal rugae.
Some attempts at applying 3D image analysis to palatal rugae can be found in literature: Taneva et al. in 2015 performed for forensic purposes a metrical assessment of variations in 13 points of palatal rugae observed in different 3D scans, and between pre-treatment and post-treatment casts. Results did not verify statistically significant differences among scans obtained through different tools and between pre- and post-treatment models; in addition, the authors were able to identify landmarks showing minor differences between pre- and post-treatment scans, which therefore may be more useful for personal identification [17]. This experiment, the first one based on 3D models of palatal rugae [17], shows the great advantages which may come from the application of modern 3D image acquisition systems to the morphological and metrical assessment of these particular structures; however, no one has applied this approach so far to the evaluation of anatomical uniqueness of palatal rugae.
The present study confirmed the uniqueness of palatal rugae by applying a metrical assessment of point-to-point differences between two 3D models. In fact, results show that there is a statistically significant difference between cases of matches and mismatches. In addition, the chosen protocol limits to a minimum the manual procedures which consist only in the selection of the palatal arc for the 3D scan. From this point of view, the novel method provides a further step towards automatization of procedures of comparison, reducing the possible introduction of bias [8]. In addition, the present study first provides the application of modern 3D image acquisition and elaboration systems to the complex issue of anatomical uniqueness of palatal rugae.
Possible modifications which may be suffered by palatal rugae as a consequence of orthodontic therapy are worth being discussed in depth, as they are not univocally treated by literature. Several authors report that extraction treatment may modify the length of palatal rugae, although there is no consensus about which rugae are more or less affected by these modifications [18,19,20]. The third ruga seems to be the most stable one as reported by several authors [21, 22]. Although a contrast exists in literature, most of authors seem to confirm that orthodontic procedures do modify palatal rugae; regardless, although these modifications may have occurred, in the current study, the 3D-3D superimposition protocol was able to correctly distinguish without errors the group of matches from the mismatches. From this point of view, the present results seem to highlight that the current method is not influenced by these unpredictable variables. In other words, individual modifications of rugae seem not to affect identification potential, as also proved by morphological studies [18].
In conclusion, the present study provides a contribution to the issue of uniqueness of palatal rugae through a 3D metrical approach: the method may also find a practical application in the field of personal identification based on the comparison of the morphology of palatal rugae.
References
Santos C, Caldas IM (2012) Palatal rugae pattern in a Portuguese population: a preliminary analysis. J Forensic Sci 57(3):786–788. https://doi.org/10.1111/j.1556-4029.2011.02016.x
Poojya R, Shruthi CS, Rajashekar VM, Kaimal A (2015) Palatal rugae patterns in edentulous cases, are they a reliable forensic marker? Int J Biomed Sci 11(3):109–112
Muthusubramanian M, Limson KS, Julian R (2005) Analysis of rugae in burn victims and cadavers to simulate rugae identification in cases of incineration and decomposition. J Forensic Odontostomatol 23(1):26–29
Dawasaz A, Dinkar AD (2013) Rugoscopy: predominant pattern, uniqueness, and stability assessment in the Indian Goan population. J Forensic Sci 58(6):1621–1627. https://doi.org/10.1111/1556-4029.12190
Adisa A, Kolude B, Ogunrinde TJ (2014) Palatal rugae as a tool for human identification. Niger J Clin Pract 17(5):641–643. https://doi.org/10.4103/1119-3077.141434
Bansode SC, Kulkarni MM (2009) Importance of palatal rugae in individual identification. J Forensic Dent Sci 1(2):77–81. https://doi.org/10.4103/0974-2948.60378
Mohammed RB, Patil RG, Pammi VR, Sandya MP, Kalyan SV, Anitha A (2013) Rugoscopy: human identification by computer-assisted photographic superimposition. J Forensic Dent Sci 5(2):90–95. https://doi.org/10.4103/0975-1475.119771
Hemanth M, Vidya M, Shetty N, Karkera BV (2010) Identification of individuals using palatal rugae: computerized method. J Forensic Dent Sci 2(2):86–90. https://doi.org/10.4103/0975-1475.81288
Limson KS, Julian R (2004) Computerized recording of the palatal rugae pattern and an evaluation of its application in forensic identification. J Forensic Odontostomatol 22(1):1–4
De Angelis D, Sala R, Cantatore A, Grandi M, Cattaneo C (2009) A new computer-assisted technique to aid personal identification. Int J Legal Med 123(4):351–356. https://doi.org/10.1007/s00414-008-0311-x
Gibelli D, Obertovà Z, Ritz-Timme S, Gabriel P, Arent T, Ratnayake M, De Angelis D, Cattaneo C (2016) The identification of living persons on images: a literature review. Legal Med 19:52–60. https://doi.org/10.1016/j.legalmed.2016.02.001
De Angelis D, Riboli F, Gibelli D, Cappella A, Cattaneo C (2012) Palatal rugae as an individualising marker: reliability for forensic odontology and personal identification. Sci Justice 52(3):181–184. https://doi.org/10.1016/j.scijus.2011.09.002
Naether S, Buck U, Campana L, Breitbeck R, Thali M (2012) The examination and identification of bite marks in foods using 3D scanning and 3D comparison methods. Int J Legal Med 126(1):89–95. https://doi.org/10.1007/s00414-011-0580-7
Molina A, Martin-de-las-Heras S (2015) Accuracy of 3D scanners in tooth mark analysis. J Forensic Sci 60(Suppl. 1):S222–S226. https://doi.org/10.1111/1556-4029.12598
De Angelis D, Gibelli D, Gaudio D, Cipriani Noce F, Guercini N, Varvara G, Sguazza E, Sforza C, Cattaneo C (2015) Sexualdimorphism of canine volume: a pilotstudy. Legal Med 17(3):163–166. https://doi.org/10.1016/j.legalmed.2014.12.006
Franco A, Willems G, Souza PH, Tanaka OM, Coucke W, Thevissen P (2017) Three-dimensional analysis of the uniqueness of the anterior dentition in orthodontically treated patients and twins. Forensic Sci Int 273:80–87. https://doi.org/10.1016/j.forsciint.2017.02.010
Taneva ED, Johnson A, Viana G, Evans CA (2015) 3D evaluation of palatal rugae for human identification using digital study models. J Forensic Dent Sci 7(3):244–252. https://doi.org/10.4103/0975-1475.172451
Batool A, Shaikh A, Fida M (2016) Stability of palatal rugae as a forensic marker in orthodontically treated cases. J Forensic Sci 61(5):1351–1355
Bailey LT, Esmailnejad A, Almedia MA (1996) Stability of the palatal rugae as landmarks for analysis of dental cases in extraction and non-extraction cases. Angle Orthod 66(1):73–78. https://doi.org/10.1043/0003-3219(1996)066<0073:SOTPRA>2.3.CO;2
Mustafa AC, Allouh MZ, Alshehab RM (2015) Morphological changes in palatal rugae patterns following orthodontic treatment. J Forensic Legal Med 31:19–22. https://doi.org/10.1016/j.jflm.2015.01.002
Shukla D, Clowdhry A, Bablani D, Jain P, Thapar R (2011) Establishing the reliability of palatal rugae pattern in individual identification (following orthodontic treatment). J Forensic Odontostomatol 29(1):20–29
Deepak V, Malgaonkar NI, Shah NK, Nasser AS, Dagrus K, Bassel T (2014) Palatal rugae patterns in orthodontically treated cases, are they a reliable forensic marker? J Int Oral Health 6(8):89–95
Acknowledgements
We thank Ms. Alice Loviglio for her precious help in data collection and analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Gibelli, D., De Angelis, D., Pucciarelli, V. et al. Application of 3D models of palatal rugae to personal identification: hints at identification from 3D-3D superimposition techniques. Int J Legal Med 132, 1241–1245 (2018). https://doi.org/10.1007/s00414-017-1744-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-017-1744-x