
Abstract
There is a need for dental age estimation methods after completion of the third molar mineralization. Degenerative dental characteristics appear to be suitable for forensic age diagnostics beyond the 18th year of life. In 2012, Olze et al. investigated the criteria studied by Gustafson using orthopantomograms. The objective of this study was to prove the applicability and reliability of this method with a large cohort and a wide age range, including older individuals. For this purpose, 2346 orthopantomograms of 1167 female and 1179 male Germans aged 15 to 70 years were reviewed. The characteristics of secondary dentin formation, cementum apposition, periodontal recession and attrition were evaluated in all the mandibular premolars. The correlation of the individual characteristics with the chronological age was examined by means of a stepwise multiple regression analysis, in which the chronological age formed the dependent variable. Following those results, R 2 values amounted to 0.73 to 0.8; the standard error of estimate was 6.8 to 8.2 years. Fundamentally, the recommendation for conducting age estimations in the living by these methods can be shared. The values for the quality of the regression are, however, not precise enough for a reliable age estimation around regular retirement date ages. More precise regression formulae for the age group of 15 to 40 years of life are separately presented in this study. Further research should investigate the influence of ethnicity, dietary habits and modern health care on the degenerative characteristics in question.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Age estimation in the living has been in the focus of forensic research for several years [6, 16, 27, 45–56]. In particular, it includes legal issues, refugee issues, and the field of competitive sports [7, 8, 29, 32, 33, 43, 44]. The validation of the completion of the 18th and 21st year of life is of special importance in all of these. Providing a proof for the completion of the 18th year of life by means of the established dental methods is however not possible with the forensically required certainty, even if all the third molars of a person are completely mineralized, as their mineralization can be completed before the 18th birthday [52, 53]. Therefore, other methods for age estimation after the completion of third molar mineralization are needed.
For age estimation in living individuals undergoing retirement proceedings, the Study Group on Forensic Age Diagnostics recommends the implementation of the well-known morphological methods of dental age estimation based on existing radiographs from childhood or adolescence. If no previous radiographs should exist, aspartic acid racemization is the recommended method [41]. Further methods with good reliability suitable for older age groups are the analysis of tooth-cementum annulations (TCA) and the Lamendin method with its revisions [1, 4, 5, 19, 34, 58, 59]. Only these methods appear to be sufficiently reliable after the completion of tooth development [4, 5, 10, 20, 24, 26, 30, 36, 37, 39–41, 58, 59]. Since these methods are applicable only to extracted teeth, their use is severely restricted in living individuals for ethical reasons [38, 41]. Furthermore, it has to be mentioned that a comparatively high interobserver-error in TCA-analysis is a cause of concern [35, 42].
Another method for age estimation after the completion of tooth development is the method according to Kvaal et al. [18] using the size of the pulp in full mouth radiographs. However, weaknesses of this method have been described [9, 32]. Therefore, the method according to Kvaal et al. [18] can currently not be seen as a valid alternative for age estimation after third molar mineralization.
Degenerative dental characteristics appear to be suitable for forensic age diagnostics. The first attempts of scientific dental age estimation date back to Gustafson in 1947 [12]. Gustafson presented the characteristics of secondary dentin formation, periodontal recession, attrition, apical translucency, cementum apposition, and external root resorption as phenomena correlating with chronological age [12–14]. In 1981, Matsikidis proved that the characteristics presented by Gustafson for extracted and ground teeth can also be applied to dental films [22]. As not all the characteristics evaluable in an extracted tooth are equally evaluable in radiographies and also since method-related loss in resolution and artificial distortion are to be expected, the accuracy of estimate of the Matsikidis-method was lower than the accuracy of estimate of methods presented for extracted teeth [15, 21, 52].
In 2012, Olze et al. were able to show that the characteristics presented by Gustafson can be determined using orthopantomograms as well. They presented regression formulae for age estimation in the age group of 15 to 40 years, by using these characteristics [29].
The aim of the present study was to validate the method proposed by Olze et al. [29] within a large study population in the age group of 15 to 70. In order to compare our results with the findings presented by Olze et al. [29], separate calculations for the age group 15 to 40 years were performed.
Materials and methods
Subject to the study were 2346 orthopantomograms of 1167 female and 1179 male Germans between 15 and 70 years of age, collected from two dental practices and a maxillofacial surgery practice in the Paderborn area in Germany. The orthopantomograms were made in the period between 1985 and 2011. The first examiner was a dentist with profound professional experience including the examination of orthopantomograms. Prior to the study he had intensively become acquainted to the issue and also discussed it with a forensic dentist experienced in dental age assessment by means of Gustafson’s criteria. After intensive training, the first examiner was very qualified in this method.
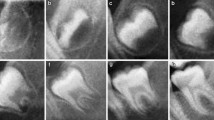
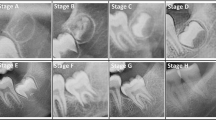
Table 1 shows the number of cases in the sample per age cohort divided by sex. The characteristics of secondary dentin formation, cementum apposition, periodontal recession and attrition were determined in all mandibular premolars using the stage classifications according to Olze et al. [29] (Figs. 1, 2, 3, and 4). The determination of external root resorption was waived, as Olze et al. [29] had found that it cannot be evaluated in orthopantomograms. The exclusion criteria in each case were drawn from the recommendations presented by Matsikidis (Table 2) [18]. Teeth were excluded due to one of Matsikidis’ recommended reasons or due to poor quality of the orthopantomogram. Missing teeth could be missing because of agenesis of the tooth, extraction, or trauma.

Stage classification to determine degree of secondary dentin. Stage 0 Pulp horn (top of the pulp chamber) reaches to above crown equator (largest mesio-distal width). Stage I Pulp horn reaches at maximum to crown equator. Stage II Pulp horn exceeds enamel-cementum junction and falls short of crown equator. Stage III Pulp horn reaches at maximum to enamel-cementum junction

Stage classification to determine degree of periodontal recession. Stage 0 No periodontal recession. Stage I Periodontal recession into cervical root third. Stage II Periodontal recession into middle root third. Stage III Periodontal recession into apical root third

Stage classification to determine degree of attrition. Stage 0 No attrition, cusp tips present. Stage I Beginning attrition with loss of cusp tips. Stage II Attrition reaching into dentin. Stage III Attrition reaching into dentin with opening of pulp cavity

Stage classification to determine degree of cementum apposition. Stage 0 No visible cementum apposition. Stage I Beginning apical cementum apposition. Stage II Clearly visible cementum apposition, reaching beyond the apex
The evaluation of the orthopantomograms was performed randomized and blinded, i.e., without knowledge of the dates of birth or the date of the radiographical examination. Each orthopantomogram was assigned an identification number. Identification number, date of birth, the subject’s sex, date of radiographical examination, and the stages of the teeth included in the study were recorded. In case of non-evaluable teeth, it was distinguished between non-presence and lack of assessability.
The correlation between chronological age and the individual degenerative characteristics was examined by means of a multiple regression analysis, with the chronological age being the dependent variable and the examined degenerative characteristics being the independent variables. The modeling of the linear regression model was developed in single steps with the prognosis-relevant influencing variables of the degenerative characteristics. At each stage of this process, the significant influencing variable was selected from the remaining influencing variables. Only influencing variables with a significance value of <0.05 were included in the regression. Finally, regression formulae to fill in the stages of the degenerative characteristic for reliable age estimations were developed. To every single regression formula, the coefficient of determination and the standard error of estimate were calculated as well. The multiple regression analysis was carried out for the whole age range of 15 to 70 years and also separately for the age group of 15 to 40 years. Furthermore, a study on multicollinearities between the influencing variables was performed, for which the variance inflation factor (VIF) value was noted. A VIF value of >4 was considered to be a critical multicollinearity.
For intra-rater agreement, 100 randomized orthopantomograms were reevaluated by the first examiner. For inter-rater agreement evaluation, the same 100 orthopantomograms were also evaluated by a second examiner. The second examiner was a dentist without experiences in dental age assessment. Cohen’s kappa coefficients were calculated for intra- and inter-rater agreement.
Results
Table 3 shows the number and percentage of teeth which could not be used for statistical evaluation due to predefined exclusion criteria or because of poor quality of the orthopantomogram. The number of missing teeth is provided as well. Depending on the examined tooth, 15–59% of cases were evaluable. Concerning the second premolars, a lower percentage of cases was evaluable. Tables 4 and 5 show the frequencies of the various stages of the examined features. All the examined characteristics were statistically linked to chronological age. The intra-rater agreement was substantial to almost perfect (Kappa 0.78–0.92). The inter-rater agreement was worse than the intra-rater agreement in every case (Kappa 0.38–0.75). Multicollinearities could not be detected. All VIF values were smaller than the critical limit of 4. Tables 6 and 7 show the results of the multiple regression analysis for the age range of 15 to 70 years. Tables 8 and 9 show the results for the multiple regression analysis for the age range of 15 to 40 years. From these tables can be drawn that the values for the standard error of estimate were slightly lower concerning the second premolars when compared to the values for the standard error of estimate concerning the first premolars. Furthermore, the values for the standard error of estimate were lower for the age group of 15 to 40 years compared to the age group 15 to 70 years. Tables 10 and 11 show the values for the quality of the multiple regression for the age group of 15 to 40 years in direct comparison to the results of Olze et al. [29]. These tables show that the quality of the regression could be improved for this age group.
Discussion
In the past, it was shown that regressive dental changes in correlation to chronological age qualify for age estimations after the completion of the third molar mineralization [18, 28]. These changes begin immediately after eruption and continue throughout the whole life [3, 13, 15, 17, 25, 60]. In 2012, Olze et al. published a study of their results on an investigation of Gustafson’s criteria in orthopantomograms [29]. In their study, they included 1299 radiographs of 650 female and 649 male Germans between 15 and 40 years of life. The characteristics of secondary dentin formation, cementum apposition, periodontal recession, and attrition were evaluated in all of the mandibular premolars. They developed a staging system with less stages compared to the staging system Matsikidis had presented for regressive dental changes. This was done for a better applicability to orthopantomograms [29]. They studied the correlation between individual characteristics and chronological age by means of a stepwise multiple regression analysis in which chronological age formed the dependent variable. Regression formulae to calculate the estimated age of a person were presented. They recommended their method for age estimation with the restriction that the quality of the radiographs often limits the applicability of the method [29].
The aim of the present study was to investigate the validity of the results of Olze et al. [29]. The individuals studied were 15 to 70 years old, meaning the age interval included all ages of forensic importance. As an uneven age distribution within the sample may lead to systematic over- or underestimation of age [11], the attempt was made to fill every age cohort equally. Especially in the older age cohorts, this objective could not always be achieved, as there were not as many radiographs available for the older age cohorts, even though the radiographs had been collected from three different dental and oral maxillofacial surgery practices. In the age cohort of 15 to 40 years the objective of equal distribution could mainly be achieved. The stage classifications presented by Olze et al. [29] were used. The mandibular premolars were examined since Olze et al. [29] described them to be the only suitable teeth for this purpose.
After exclusion of missing teeth, those that could not be assessed due to the quality of the radiographs and those teeth that had been excluded due to the criteria by Matsikidis [22], 15 to 59% of the cases were suitable for evaluation. The bottom limit is much lower here than the values Olze et al. [29] presented in their study. They had been able to evaluate 45–60% of cases [29]. The low value of our study can be explained by the older cohort in this study, in that a higher age means an increase in the likelihood of Matsikidis’ criteria [22] being met or to having lost a certain tooth during lifetime. The common upper value of about 60% appears to be set due to the quality of the radiographs and therefore appears to be the upper limit of the method.
The intra-rater agreement was substantial to almost perfect. The inter-rater agreement was worse than the intra-rater agreement in every case. This must be seen against the background of the second examiner being a dentist completely inexperienced in age estimation methods. Thus, the low inter-rater agreement shows once again that age estimation is a task for experts only [57].
In the present study, stepwise multiple regression analysis was used to develop calculation formulae regarding the lower premolars in relation to regressive tooth changes with a known significant correlation to age, in order to estimate the age of an individual and to determine the corresponding correlation coefficient according to Olze et al. [29]. Regression analyses should only be used for metrically scaled variables, whereas the age estimation characteristics examined in this study are ordinally scaled variables. As an alternate multivariate analysis method for ordinally scaled variables, the Bayes theorem was proposed [2]. However, a study by Thevissen et al. [54] showed that by applying the Bayes theorem, an improvement in the accuracy of estimation could not be achieved in comparison to when applying linear regression analysis. We therefore deemed it appropriate to use regression analyses for the statistical evaluation of our data.
Regression analyses were performed separately for the age cohorts 15 to 70 years and 15 to 40 years and per sex, for the best possible comparability of this study’s results and those presented by Olze et al. [29]. The calculated R 2 values range from 0.69 to 0.77 and thus are similar to or above the values for the age cohort presented by Olze et al. [29]. With the formulae presented in this study, more accurate age estimations are possible in the age group 15 to 40 years. For the age group 15 to 70 years, the values for the standard error of estimate were higher. The range for the R 2 is 0.73 to 0.8 and the range for the standard error of estimate in this age group lies at 6.8 to 8.2 years. The pronounced standard errors of estimate appear too high for reliable age estimations in the elderly. These findings underline the problem of utilizing morphological characteristics for age estimations in the elderly.
In our study, the values for the standard error of estimate were slightly lower concerning the second premolars when compared to the values for the standard error of estimate concerning the first premolars. A possible explanation for this could be that the second premolars take part in the occlusion with five contact points, whereas the first premolars take part in it with only two contact points. Improper burdening of the first premolars could thereby accelerate degenerative changes.
In conclusion, the method presented by Olze et al. [29] could be validated in the present study. The method is applicable and reliable for dental age diagnostics in the age group up to 40 years. For age estimations concerning older age groups, e.g., around retirement date ages, the method appears to be too inaccurate. The values for the standard error of estimate are too high for a precise and reliable age estimation around retirement date ages. Furthermore, the method is limited by the number of radiographs suitable for evaluation. Moreover, the examined phenomena must be questioned for whether or not they depend on ethnicity. This has to be considered, especially concerning the age estimations in refugees [23, 31, 44]. Additionally, the influence of dietary habits and modern health care on the degenerative dental characteristics has not been investigated yet. Therefore, despite a long history of studies on these characteristics, more studies are needed to more precisely draw the boundary line between physiological age-related changes and pathological processes. Also, it should be investigated, whether methods free of ionizing radiation like magnetic resonance imaging can be utilized for Gustafson’s criteria, as MRI appears to be suitable to detect mineralization stages in the third molars [31].
References
Baccino E, Sinfield L, Colomb S, Baum TP, Martrille L (2014) Technical note: The two step procedure (TSP) for the determination of age at death of adult human remains in forensic cases. Forensic Sci Int 244:247–251
Braga J, Heuze Y, Chabadel O, Sonan NK, Gueramy A (2005) Non-adult dental age assessment: correspondence analysis and linear regression versus Bayesian predictions. Int J Legal Med 119:260–274
Burke FM, Samarawickrama DYD (1995) Progressive changes in the pulpo-dentinal complex and their clinical consequences. Gerodontology 12:57–66
Charles KD, Condon K, Cheverud JM, Buikstra JE (1986) Cementum annulation and age determination in Homo sapiens. I. Tooth variability and observer error. Am J Phys Anthropol 71:311–320
Condon K, Charles KD, Cheverud JM, Buikstra JE (1986) Cementum annulation and age determination in Homo sapiens. II. Estimates and accuracy. Am J Phys Anthropol 71:321–330
Demirjian A, Goldstein H, Tanner JM (1973) A new system of dental age assessment. Hum Biol 45:211–27
Dvorak J, George J, Junge A, Hodler J (2007) Application of MRI of the wrist for age determination in international U-17 soccer competitions. Br J Sports Med 41:497–500
Engebretsen L, Steffen K, Bahr R, Broderick C, Dvorak J, Janarv PM, Johnson A, Leglise M, Mamisch TC, McKay D, Micheli L, Schamasch P, Singh GD, Stafford DEJ, Steen H (2010) The International Olympic Committee consensus statement on age determination in high-level young athletes. Br J Sports Med 44:476–484
Erbudak HÖ, Ozbek M, Uysal S, Karabulut E (2012) Application of Kvaal et al’.s age estimation method to panoramic radiographs from Turkish individuals. Forensic Sci Int 219:141–146
Fu SJ, Fan CC, Song HW, Wei FQ (1995) Age estimati on using a modified HPLC determination of ratio of aspartic acid in dentin. Forensic Sci Int 73:35–40
Gelbrich B, Lessig R, Lehmann M, Dannhauer K-H, Gelbrich G (2010) Altersselektion in Referenzstichproben. Auswirkung auf die forensische Altersschätzung. Rechtsmed 20:459–463
Gustafson G (1947) Åldersbestämningar på tänder. Odont Tidskr 55:556–568
Gustafson G (1950) Age determination on teeth. J Am Dent Assoc 41:45–54
Gustafson G (1955) Altersbestimmung an Zähnen. Deutsche Zahnärztl Z 10:1763–1768
Johanson G (1971) Age determination from human teeth. Thesis Odont Revy 22(suppl 21):1–126
Kellinghaus M, Schulz R, Vieth V, Schmidt S, Schmeling A (2010) Forensic age estimation in living subjects based on the ossification status of the medial clavicular epiphysis as revealed by thin-slice multidetector computed tomography. Int J Legal Med 124:149–154
Ketterl W (1983) Age-induced changes in the teeth and their attachment apparatus. Int Dent J 33:262–271
Kvaal KI, Kollveit KM, Thomsen IO, Solheim T (1995) Age estimation of adults from dental radiographics. Forensic Sci Int 74:175–85
Lamendin H, Baccino E, Humbert JF, Tavernier JC, Nossintchouk RM, Zerilli A (1992) A simple technique for age estimation in adult corpses: the two criteria dental method. J Forensic Sci 37:1373–1379
Lippitsch A, Grupe G (2007) Variability of the apposition of the acellular, extrinsic fibre cementum and its influence on the tooth cementum annulation technique in humans: the influence of physical demands and functional morphology. Doc Archaeobiolo 5:87–112
Maples WR, Rice PM (1979) Some difficulties in the Gustafson dental age estimations. J Forensic Sci 24:168–172
Matsikidis G (1981) Altersbestimmung aus Zahnfilmen. Med Diss. University of Heidelberg, Heidelberg
Müller K, Fuhrmann A, Püschel K (2011) Altersschätzung bei einreisenden jungen Ausländern. Erfahrungen aus dem Institut für Rechtsmedizin Hamburg Rechtsmed 21:33–38
Mörnstad H, Pfeiffer H, Teivens A (1994) Estimation of dental age using HPLC—technique to determine the degree of aspartic acid racemization. J Forensi c Sci 39:1425–1431
Nitzan DW, Michaeli Y, Winreb M, Azaz B (1986) The effect of aging on tooth morphology: a study on ompacted teeth. Oral Surg Oral Med Oral Path 61:54–60
Ogino T, Ogino H, Nagy B (1985) Application of aspartic acid racemization to forensic odontology: post mortem designation of age of death. Forensic Sci Int 29:259–267
Olze A, Bilang D, Schmidt S, Wernecke K-D, Geserick G, Schmeling A (2005) Validation of common classification systems for assessing the mineralization of third molars. Int J Legal Med 119:22–26
Olze A, SolheimT SR, Kupfer M, Pfeiffer H, Schmeling A (2010) Assessment of the radiographic visibility of the periodontal ligament in the lower third molars for the purpose of forensic age estimation in livin individuals. Int J Legal Med 124:445–448
Olze A, Hertel J, Schulz R, Wierer T, Schmeling A (2012) Radiographic evaluation of Gustafson’s criteria for the purpose of forensic age diagnostics. Int J Legal Med 126:615–621
Ohtani S (1995) Estimation of age from the teeth of unidentified corpses using the amino acid racemization method with reference to actual cases. Am J Forensic Med Pathol 16:238–242
Ottow C, Krämer JA, Olze A, Schmidt S, Schulz R, Wittschieber D, Heindel W, Pfeiffer H, Ribbecke S, Vieth V, Schmeling A (2014) Magnetresonanztomographiestudie zur Altersschätzung von unbegleiteten minderjährigen Flüchtlingen. Rechtsmed 25:12–20
Paewinsky E, Pfeiffer H, Brinkmann B (2005) Quantification of secondary dentine formation from orthopantomograms—a contribution to forensic age estimation methods in adults. Int J Med 119:27–30
Parzeller M (2015) Juristische Aspekte der forensischen Altersdiagnostik. Rechtsprechung-Update 2010-2014. Rechtsmed 25:21–29
Prince DA, Ubelaker DH (2002) Application of Lamendin’s adult dental aging technique to a diverse skeletal sample. J Forensic Sci 47:107–116
Renz H, Radlanski RJ (2006) Incremental lines in root cementum of human teeth—a reliable age marker? Homo 57:29–50
Ritz S, Schütz HW, Peper C (1993) Postmortem estimation of age at death based on aspartic acid racemization in dentin: its applicability for root dentin. Int J Legal Med 105:289–293
Ritz S, Stock R, Schütz HW, Kaatsch H-J (1995) Age estimation in biopsy specimens of dentin. Int J Legal Med 108:135–139
Ritz S, Kaatsch HJ (1996) Methoden der Altersbestimmung an lebenden Personen: Möglichkeiten, Grenzen, Zulässigkeit und ethische Vertretbarkeit. Rechtsmed 6:171–176
Ritz-Timme S (2000): Lebensaltersbestimmung aufgrund des Razemisierungsgrades von Asparaginsäure. Grundlagen, Methodik, Möglichkeiten, Grenzen, Anwendungsbereiche. In: Berg S, Brinkmann B (Hrsg.) Arbeitsmethoden der medizinischen und naturwissenschaftlichen Kriminalistik, Band 24, Lübeck, Schmidt-Römhild
Ritz-Timme S, Cattaneo C, Collins M, Waite ER, Schütz HW, Kaatsch HJ, Borrman HIM (2000) Age estimation: the state of the art in relation to the specific demands of forensic practise. Int J Legal Med 113:129–136
Ritz-Timme S, Kaatsch HJ, Marré B, Reisinger W, Riepert T, Rösing FW, Rötzscher K, Schmeling A, Geserick G (2002) Empfehlungen für die Altersdiagnostik bei Lebenden im Rentenverfahren. Rechtsmed 12:193–194
Rösing FW, Kvaal SI (1998) Dental age in adults. A review of estimation methods. In: Alt KW, Rösing FW, Teschler-Nicola M (eds) Dental Anthropology. Springer, Wien, pp 443–468
Schmeling A, Grundmann C, Fuhrmann A, Kaatsch HJ, Knell B, Ramsthaler F, Reisinger W, Riepert T, Ritz-Timme S, Rösing FW, Rötzscher K, Geserick G (2008) Criteria for age estimation in living individuals. Int J Leg Med 122:457–460
Schmeling A, Geserick G, Tsokos M et al (2014) Aktuelle Diskussionen zur Altersdiagnostik bei unbegleiteten minderjährigen Flüchtlingen. Rechtsmed 24:475–479
Solheim T (1988) Dental color as an indicator of age. Gerodontics 4:114–118
Solheim T (1988) Dental attrition as an indicator of age. Gerodontics 4:299–304
Solheim T (1989) Dental root translucency as an indicator of age. Scand J Dent Res 97:189–197
Solheim T (1990) Dental cementum apposition as an indicator of age. Scand Dent Res 98:510–519
Solheim T (1992) Amount of secondary dentin as an indicator of age. Scand J Dent Res 100:193–199
Solheim T (1992) Recession of periodontal ligament as an indicator of age. J Forensic Odontostomatol 10:32–42
Solheim T (1993) Dental root surface structure as an indicator of age. J Forensic Odontostomatol 11:9–21
Solheim T (1993) A new method for dental age estimation in adults. Forensic Sci Int 59:137–147
Streckbein P, Reichert I, Verhoff MA, Bödeker RH, Kähling C, Willbrand JF, Schaaf H, Howaldt HP, May A (2014) Estimation of legal age using calcification stages of third molars in living individuals. Sci Justice 54:447–450
Thevissen PW, Fieuws S, Willems G (2010) Human dental age estimation using third molar developmental stages: does a Bayesian approach outperform regression models to discriminate between juveniles and adults? Int J Legal Med 124:35–42
Vieth V, Kellinghaus M, Schulz R, Pfeiffer H, Schmeling A (2010) Beurteilung des Ossifikationsstadiums der medialen Klavikulaepiphysenfuge. Vergleich von Projektionsradiographie, Computertomographie und Magnetresonanztomographie. Rechtsmed 20:483–488
Vieth V, Schulz R, Brinkmeier P, Dvorak J, Schmeling A (2014) Age estimation in U-20 football players using 3.0 tesla MRI of the clavicle. Forensic Sci Int 241:118–122
Wittschieber D, Schulz R, Vieth V, Küppers M, Bajanowski T, Ramsthaler F, Püschel K, Pfeiffer H, Schmidt S, Schmeling A (2014) Influence of the examiner’s qualification and sources of error during stage determination of the medial clavicular epiphysis by means of computed tomography. Int J Legal Med 128:183–191
Wittwer-Backofen U, Gampe J, Vaupel JW (2004) Tooth cementum annulation for age estimation: results from a large known-age validation study. Am J Phys Anthropol 123:119–129
Wittwer-Backofen U, Buckberry J, Czarnetzki A, Doppler S, Grupe G, Hotz G, Kemkes A, Larsen CS, Prince D, Wahl J, Fabig A, Weise S (2008) Basics in paleodemography: a comparison of age indicators applied to the early medieval skeletal sample of Lauchheim. Am J Phys Anthropol 137:384–396
Zuhrt R (1991) Biologische Aspekte der Endodontie im höheren Erwachsenenalter. Dtsch Stomatol 41:4–10
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Timme, M., Timme, W.H., Olze, A. et al. Dental age estimation in the living after completion of third molar mineralization: new data for Gustafson’s criteria. Int J Legal Med 131, 569–577 (2017). https://doi.org/10.1007/s00414-016-1492-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-016-1492-3