
Abstract
Cyanide (CN) blood concentration is hardly considered during routine when evaluating smoke gas intoxications and fire victims, although some inflammable materials release a considerable amount of hydrogen cyanide. CN can be significant for the capacity to act and can in the end even be the cause of death. Systematic data concerning the influence of different fire conditions, especially those of various inflammable materials, on the CN-blood concentration of deceased persons do not exist. This study measured the CN level in 92 blood samples of corpses. All persons concerned were found dead in connection with fires and/or smoke gases. At the same time, the carboxyhemoglobin (COHb) level was determined, and the corpses were examined to detect pharmaceutical substances, alcohol and drugs. Furthermore, we analysed autopsy findings and the investigation files to determine the inflammable materials and other circumstances of the fires. Due to the inflammable materials, the highest concentration of CN in the victims was found after enclosed-space fires (n = 45) and after motor-vehicle fires (n = 8). The CN levels in these two groups (n = 53) were in 47 % of the cases toxic and in 13 % of the cases lethal. In victims of charcoal grills (n = 17) and exhaust gases (n = 6), no or only traces of CN were found. Only one case of the self-immolations (n = 12) displayed a toxic CN level. The results show that CN can have considerable significance when evaluating action ability and cause of death with enclosed-space fires and with motor-vehicle fires.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Smoke inhalation has been well established as a cause of death in fire victims [1–3]. Smoke gas is usually formed by more than 400 toxic constituents [4], but only carbon monoxide (CO) and hydrogen cyanide (HCN) are the two main toxicants [5]. Both develop in particular in incomplete combustion, with HCN forming mainly at high temperatures [6–8], and when nitrogenous materials such as polyurethane, polyamide and polyacrylonitrile, wool or silk are burning [9–11].
According to clinical medicine, deaths in fires are often caused by pure CN intoxication or a mixed CN-CO intoxication [12]. It is nevertheless true that in forensic medicine CO is more regularly assessed than CN when the cause of death is being clarified [13, 14]. It is the aim of the present research to be able to assess more exactly the significance of CN especially for the cause of death. We therefore have to consider different inflammable materials and smoke gases of varying genesis. We also have to bear in mind that the data concerning toxic and lethal human CN concentration in the blood vary. In most cases a CN concentration in the blood of more than 0.5 mg/l is considered to be toxic, while one of more than 3.0 mg/l is considered to be lethal. [15–18]. It is assumed that the potential lethal COHb level is 50 % [19–21].
Materials and methods
Blood samples of corpses - autopsy findings
From 2011 to 2013, the Institute of Legal Medicine at Munich University carried out 92 autopsies connected with fires and/or smoke gas impact. In all the cases, samples of blood from the heart were retained. The autopsy findings were registered with particular regard to potentially competing causes of death. The presence of soot particles in the respiratory tract, in the esophagus and in the stomach was documented.
Investigation files - case groups
The files showed causes, materials and further particulars of the fires. In all the cases, death occurred immediately during or after traumatization. It is to be noted that in six of the cases, resuscitation was attempted, but the persons concerned died at the place where they were found. Based on the investigation reports and considering the autopsy findings, the following case groups were formed:
-
enclosed-space fires
-
motor-vehicle fires
-
self-immolations
-
charcoal grills
-
exhaust gases (motor vehicles, ovens, CO plant chemistry lab)
-
others (explosions, plane crashes)
Chemico-toxicological analyses
Concentrations of CN and CO were measured in blood from the heart. The samples for CN-quantitation were stored at −20 °C (−4 °F). The CN concentrations were analysed by means of a modified microdiffusion in a sodium hydroxide solution. After the reaction with pyridine/barbituric acid reagent [22, 23], the CN level was determined photometrically (Genesys 10 uv, Thermo Electron Corporation). This quantitation was carried out by a six-point calibration. The detection limit was 0.25 mg/l.
The COHb level was determined by spectral photometry immediately after the extraction (ABL 800 Flex, Radiometer).
We carried out examinations for ethanol, pharmaceutical substances and drugs by means of gas chromatography as well as by tandem mass spectrometry on the venous blood of the femur.
Statistics
All data was managed with Microsoft Excel 2013 (Microsoft Corporation; USA). Analyses were performed with SPSS software (IBM SPSS; USA) and Microsoft Excel 2013. Pearson’s correlation coefficient was used.
Results
Case groups
Most of the people (n = 45) died in enclosed-space fires. In 30 cases, it was mainly mattresses and upholstery that burned, while in 15 cases it was mainly other material, such as wooden furniture. Eight persons were the victims of motor-vehicle fires, 17 died through charcoal grills, 12 due to self-immolation and six through exhaust gases (three car exhaust fumes, two dismantled flues, one CO plant of a chemistry lab). Four cases were defined as others (two plane crashes, two explosions). Figure 1 shows an overview of the case groups.

Case groups and number of people concerned (n = 92) according to sex
Age and sex
The persons concerned were between 10 and 90 years old (x̄ = 53.3). Two were younger than 16 years old and 23 were older than 70. The proportion of people over 70 years of age in enclosed-space fires was 42 % (n = 19). All in all, we dealt with 58 men and 34 women (Fig. 1).
Concentration of CN and COHb in samples of blood from the heart
Figure 2 shows an overview of the CN readings in the case groups. The group of enclosed-space fires displayed by far the highest concentrations of CN (median 1.0 mg/l, x̄ = 1.5 mg/l); the maximum was 8.0 mg/l. Almost half of these cases (n = 23) showed toxic levels. A lethal concentration was determined in six cases.

Case groups and concentration of CN in samples of blood from the heart
The median in victims who died in connection with motor-vehicle fires was 0.3 mg/l (x̄ = 1.0 mg/l). Twice we detected toxic concentrations (0.5 und 1.8 mg/l) and once a lethal level (5.3 mg/l). In sum, 47 % of the cases had toxic CN levels and 13 % had lethal CN levels.
All the other groups had extremely low readings, mostly < 0.25 mg/l. Only one case of self-immolation displayed a toxic concentration of CN of 1.8 mg/l, and one other had an at best slightly higher CN level of 0.4 mg/l.
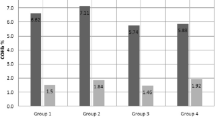
Figure 3 shows the COHb levels of the case groups; they were between 0.0 and 90.2 % COHb. The highest median was found in the group of charcoal grills (74.0 %, x̄ = 67.1 %), the lowest in the group of others (1.0 %, x̄ = 1.8 %).

Case groups and concentration of COHb in samples of blood from the heart
In the group of enclosed-space fires the median was 41.6 % COHb (x̄ = 43.6 %). In 47 % of these cases (n = 21) the levels were > 10 % COHb; in 42 % (n = 19) lethal concentrations were determined. Motor-vehicle fires had a median of 5.9 % (x̄ = 14.3 %). Those who died through exhaust gases had a median of 70.5 % COHb (x̄ = 68.8 %); self-immolations had a median of 3.5 % (x̄ = 5.7 %).
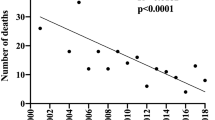
At r = 0.29 there was a slightly positive correlation between the CN and the COHb levels in the group of enclosed-space fires (Fig. 4). The readings in the remaining case groups were not correlated as these groups comprised too little data.

Correlation of COHb and CN concentrations in samples of blood from the heart in the case group of enclosed-space fires
Inflammable materials and causes of enclosed-space fires
When mainly mattresses and upholstery burned, we determined on average higher concentrations than when other inflammable materials burned (Table 1).
The majority of fires were caused by smoking, e.g. because of smoking materials on upholstery. Numerous other fires were often caused by broken electrical appliances or hotplates that were switched on.
Blood alcohol, pharmaceutical substances and drugs
On behalf of the public prosecutors’ examinations were carried out on centrally acting substances. In 38 cases a blood alcohol concentration between 0.01 ‰ and 3.29 ‰ (median 0.94 ‰, x̄ = 1.2 ‰) was measured, with 24 samples displaying levels of > 0.5 ‰. Sixteen other persons concerned were not under the influence of alcohol.
Twenty-two of 43 of the blood samples that were examined for pharmaceutical substances and drugs as ordered were positive in eight cases with concentrations that may indicate centrally acting impediments. Antidepressants, benzodiazepines, opioid, and non-opioid analgesics were those most frequently detected. In one case, cocaine was found, in another heroin.
Morphological findings
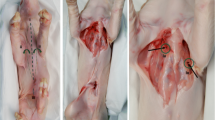
Soot particles were found relatively often in victims of enclosed-space fires, especially in the respiratory tract (87 %), but less frequently in the esophagus (51 %) and in the stomach (31 %). Such particles were detected less frequently in victims of self-immolation and motor-vehicle fires. In the group others soot was found only in the respiratory tract. As expected, no soot particles were found in any of the victims of charcoal grills and exhaust gases. Figure 5 shows further details.

Relative frequency of detection of soot particles in the respiratory tract, the esophagus and the stomach in four of the case groups - the group others showed soot only in the respiratory tract
In 25 % of the autopsies, typical signs of a CO intoxication, such as light red livores mortis and salmon-coloured skeletal muscles, were recorded.
All victims of the group others had third- or fourth-degree burns on the body’s surface; the same applies to 92 % of the victims of self-immolation, 88 % of those of motor-vehicle fires and 47 % of the victims of enclosed-space fires. The victims of charcoal grills and exhaust gases showed no burns.
Five victims of motor-vehicle fires and all victims in the group others suffered a severe polytrauma that was incompatible with life. As expected, the persons over 70 years of age had pre-existing cardiac conditions, such as higher-degree stenoses of the coronary arteries, in some cases with hypertrophy and/or callosities of the myocardium.
Discussion
The highest concentrations of CN were found in the blood of victims of enclosed-space fires. It is probable that the high temperatures that often occur there and hypoxia fostered the formation of CN [6–8]. Particularly high CN levels were found if the inflammable material consisted mainly of mattresses and upholstery. This confirms that the CN level in smoke gases is dependent on the type of inflammable material [24].
It is especially important for the forensic-medical assessment that three of the victims had a lethal concentration of CN, but COHb levels of under 50 %. CN was thus of decisive significance for the death in these cases. In twelve other samples we measured concentrations of CN between 0.5 and 2.0 mg/l, the levels of COHb being between 15 and 40 % (see Fig. 4). We have to assume that in these cases an ultimately lethal mixed intoxication caused the deaths, as the CN and COHb levels alone cannot explain them. It is remarkable that in only three of the 45 cases no CN could be detected. All in all only a weak accordance with other data [25–27] was determined between the CN and COHb levels (r = 0.29) in the group of enclosed-space fires.
The fires were mainly caused by smoking materials [28, 29]. In some cases, the victims were under the significant influence of alcohol, pharmaceutical substances or drugs, all of which can present a risk factor for fire injuries [30].
Almost half of the persons concerned were over 70 years of age. This result is due to the fact that the risk of becoming a victim of an enclosed-space fire increases with age [31]. It was striking that both the CN concentration with a median of 0.8 mg/l (x̄ = 1.2 mg/l) and the COHb levels with a median of 32.4 % (x̄ = 37.0 %) were lower in the elderly than in those less than 70 years old (CN: median 1.2 mg/l, x̄ = 1.8 mg/l, COHb: median 54.8 %, x̄ = 48.4 %). A reason for this discrepancy is the high proportion of existing heart conditions in the group of the elderly [32].
The comparatively high CN levels in two of the eight victims of motor-vehicle fires can evidently be attributed to the use of nitrogenous plastics in the engine compartment and in the passenger cabin [33]. One case displayed a toxic CN level of 1.8 mg/l, while the corresponding COHb level was 29.1 %. The other case showed a lethal level of 5.3 mg/l and a COHb concentration of 60 %. One further case of an explosion-like fire that originated mainly from the passenger cabin showed a CN level of 0.5 mg/l and a COHb level of 10 %. The other five victims of motor-vehicle fires and those in the group others showed only very low concentrations of CN and COHb, as these persons died very quickly due to injuries caused by accidents. In such cases inhalation of smoke gases can no longer be expected [34].
Only one case in the group of self-immolations displayed a toxic CN level of 1.8 mg/l and a COHb level of 17.5 %. A 61-year-old man had poured a fire accelerant over himself in the open air and set himself on fire. Apparently the material of his clothing was the reason for the CN level. Apart from that, no or only very low concentrations of CN were measured in this group; higher COHb levels were not to be expected either [25].
As expected, no increased concentrations of CN were found in victims of exhaust gases and charcoal grills. However, both groups displayed the highest COHb levels on average.
If soot particles were present in the respiratory tract, in the esophagus or in the stomach, toxic and/or lethal CN and COHb concentrations were almost always present. Three exceptions were found in the group of enclosed-space fires - cases with COHb levels of 45, 65 and 71 %, which, however, did not contain any soot particles. One of the victims of motor-vehicle fires also showed no soot; the CN level was 1.8 mg/l and the COHb level was 29 %. As the soot particles that are formed in a fire rise with the flames and are not to be found close to the fire, it is conceivable that these victims were clear of the upper edge of the flames during the development of the fire [32].
Conclusion
Due to frequently occurring nitrogenous inflammable materials in enclosed-space fires and motor-vehicle fires the release of HCN is to be expected. Some of the victims die from a mixed CN-CO intoxication because the individual concentrations of either gas alone often cannot explain the deaths. In some of the cases CN is the lethal element. In addition to routine measurement of the COHb concentration, the CN level in the corpse’s blood should also be determined to clarify the cause of death.
References
Mierley MC, Baker SP (1983) Fatal house fires in an urban population. JAMA 249:1466–1468
Karter MJ Jr (1986) Fire loss in the United States during 1985. Fire J 80:26–65
Loke J, Matthay RA, Smith GJW (1988) The toxic environment and its medical implications with special emphasis on smoke inhalation. In: Loke J (ed) Pathophysiology and treatment of inhalation injuries. Marcel Dekker, New York, pp 453–504
Barillo DJ (2009) Diagnosis and treatment of cyanide toxicity. J Burn Care Res 30(1):148–152
Hull TR, Stec AA, Lebek K, Price D (2007) Factors affecting the combustion toxicity of polymeric materials. Polym Degrad Stab 92:2239–2246
Alarie Y (2002) Toxicity of fire smoke. Crit Rev Toxicol 32(4):259–289
Blomqvist P, Lönnermark A (2001) Characterization of the combustion products in large-scale fire tests: comparison of three experimental configurations. Fire Mater 25:71–81
Baud FJ (2009) Akute Vergiftungen mit Kohlenmonoxid und Zyaniden. Ther Umsch 66:387–397 (in German)
Terrill JB, Montgomery RR, Reinhardt CF (1978) Toxic gases from fires. Science 200:1343–1347
Koschel MJ (2002) Where there’s smoke, there may be cyanide. AJN 102(8):39–42
Geldner G, Koch EM, Gottwald-Hostalek U, Baud F, Burillo G, Fauville JP et al (2013) Report on a study of fires with smoke gas development. Anaesthesist 62:609–616
Anseeuw K, Delvau N, Burillo-Putze G, De Iaco F, Geldner G, Holmström P et al (2013) Cyanide poisoning by fire smoke inhalation: a European expert consensus. Eur J Emerg Med 20(1):2–9
Noguchi TT, Eng JJ, Klatt EC (1988) Significance of cyanide in medicolegal investigations involving fires. Am J Forensic Med Path 9(4):304–309
Grabowska T, Skowronek R, Nowicka J, Sybirska H (2012) Prevalence of hydrogen cyanide and carboxyhaemoglobin in victims of smoke inhalation during enclosed-space fires: a combined toxicological risk. Clin Toxicol 50:759–763
Borron SW (2006) Recognition and treatment of acute cyanide poisoning. J Emerg Nurs 32(4 suppl):S11–S18
Deslauriers CA, Burda AM, Whal M (2006) Hydroxycobalamin as a cyanide antidote. Am J Ther 13(2):161–165
Stewart R (1974) Cyanide poisoning. Clin Toxicol 7(5):561–564
Baud FJ (2007) Cyanide: critical issues in diagnosis and treatment. Hum Exp Toxicol 26:191–201
Barillo DJ, Goode R, Esch V (1994) Cyanide poisoning in victims of fire: analysis of 364 cases and review of the literature. J Burn Care Rehabil 15:46–57
Levine B, D’Nicuola J, Kunsman G, Smith M, Stahl C (1996) Methodologic considerations in the interpretation of postmortem carboxyhemoglobin concentrations. Toxicology 115:129–134
Gerling I, Meissner C, Reiter A, Oehmichen M (2001) Death from thermal effects and burns. Forensic Sci Int 115:33–41
Asmus E, Garschagen H (1953) Über die Verwendung der Barbitursäure für die photometrische Bestimmung von Cyanid und Rhodanid. Z Anal Chem 138:414–422 (in German)
Feldstein L, Klendshoj NC (1954) The determination of cyanide in biological fluids by microdiffusion analysis. J Lab Clin Med 44:166–170
Stoll S, Krüger S, Roider G, Kraus S, Keil W (2016) Hydrogen cyanide in fire tests - forensic aspects. Rechtsmedizin. DOI 10.1007/s00194-016-0090-5
Yeoh MJ, Braitberg G (2004) Carbon monoxide and cyanide poisoning in fire related deaths in Victoria, Australia. J Toxicol Clin Toxicol 42(6):855–863
Yoshida M, Adachi J, Watabiki T, Tatsuno Y, Ishida N (1991) A study on house fire victims: age, carboxyhemoglobin, hydrogen cyanide and hemolysis. Forensic Sci Int 52:13–20
Baud FJ, Barriot P, Toffis V, Riou B, Vicaut E, Lecarpentier Y et al (1991) Elevated blood cyanide concentrations in victims of smoke inhalation. N Eng J Med 325:1761–1766
Runyan CW, Bangdiwala SI, Linzer MA, Sacks JJ, Butts J (1992) Risk factors for fatal residential fires. N Eng J Med 327(12):859–863
Barillo DJ, Goode R (1996) Fire fatality study: demographics of fire victims. Burns 22:85–88
Barillo DJ, Goode R (1996) Substance abuse in victims of fire. J Burn Care Rehabil 17:71–76
Gulaid JA, Sacks JJ, Sattin RW (1989) Deaths from residential fires among older people, United States, 1984. J Am Geriatr Soc 37(4):331–334
Bohnert M, Werner CR, Pollak S (2003) Problems associated with the diagnosis of vitality in burned bodies. Forensic Sci Int 135:197–205
Pohl KD (1989) Der Kraftfahrzeugbrand. DAT, Stuttgart (in German)
Bohnert M (2007) Kraftfahrzeugbrand. Rechtsmedizin 17:175–186, (in German)
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Stoll, S., Roider, G. & Keil, W. Concentrations of cyanide in blood samples of corpses after smoke inhalation of varying origin. Int J Legal Med 131, 123–129 (2017). https://doi.org/10.1007/s00414-016-1426-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-016-1426-0