
Abstract
Introduction
Post-mortem imaging is increasingly used in forensic field in cases of natural deaths related to cardiovascular diseases, which represent the most common causes of death in developed countries. While radiological examination is generally considered to be a good complement for conventional autopsy, it was thought to have limited application in cardiovascular pathology. The aim of this study was to investigate the role of post-mortem multidetector coronary artery computed tomography in cases of sudden death in adults.
Materials and methods
We have enrolled 11 cases, all of whom were negative for macroscopic extra-cardiac lethal findings after standard autopsy procedure. Later, from the same individuals, isolated single-organ post-mortem computed tomography coronarography (PMCTA), using an iodinated non-ionic contrast medium, was achieved. After computed tomography examination, all the isolated hearths were carried to the forensic pathologist, and a conventional histology assessment was performed on them.
Results
In 7 out of 11 of cadavers, a final diagnosis of myocardial infarction was made after a complete autopsy and histology procedures. Isolated hearts underwent PMCTA scanning and was confirmed in 6/11 cases, with the autopsy findings showing the presence and the localization of occlusions or severe stenoses and the extension of the myocardial hypoxic area by the extravasation of contrast medium as well.
Conclusion
Isolated single-organ PMCTA could be considered a valid and useful tool in addition to traditional autopsy investigation (macroscopic sections and histology) in identifying the cause of death by recognizing the presence and degree of coronary artery disease and myocardial infarction area visualization.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Sudden cardiac death (SCD) is defined as an unexpected death from a cardiac cause occurring within a short time, generally within 1 h of symptom onset, in a person with or without preexisting heart disease [1–3].
Although there is a tendency to ascribe all sudden non-traumatic deaths in middle-aged and elderly subjects to cardiac disease, autopsy studies in unselected subjects suggest that about 2/3 of such deaths are cardiac in origin, with coronary artery disease and its complications accounting for the overwhelming majority of deaths [4, 5]. The single most important cause of death in the adult population of the industrialized world is SCD due to coronary disease. In about 5 % to 10 % of cases, SCD occurs in the absence of coronary artery disease or congestive heart failure [6]. SCD may be the first clinical manifestation of coronary artery disease (CAD), with as many as one in five patients with coronary heart disease, and about 20 % of CAD patients have cardiac arrest as the first clinical manifestation [7].
In clinical practice, the development of ECG-gated multidetector computed tomography angiography led to a great improvement in the diagnosis of coronary artery disease in a selected population [8, 9]. Cardiac MRI is a reference standard for the assessment of ventricular function and may help identify and classify scars for risk stratification [10]. In forensic pathology, classical investigation of SCD includes the evaluation of clinical history, autopsy, and histology examination and, sometimes, the analysis of cardiac biomarkers and/or genetic analysis for channelopathies [2, 11–13].
Currently, there is no gold standard of reference for the post-mortem radiological evaluation of cardiovascular pathologies, but post-mortem imaging is increasingly used in forensic practice in cases of natural deaths related to cardiovascular diseases [14, 15].
At present, multidetector computed tomography (MDCT), CT angiography, and cardiac magnetic resonance imaging (MRI) are being used in post-mortem radiological investigation of cardiovascular pathologies [14]. Radiological coronary artery assessment, using post-mortem computed tomography (PMCT), has, until recently, been impaired due to the lack of an active circulation to deliver suitable contrast agents via an intravenous route. PMCT angiography (PMCTA) has been reported previously, in both animals and humans, using single-organ imaging, with the organ removed from the body, or whole body angiography with a modified heart–lung bypass machine [16–21].
Several studies [9, 14, 15, 22] have addressed the issue of post-mortem imaging in cardiac death. The radiological evaluation of ischemic heart disease includes the examination of the coronary arteries and myocardium. Some authors propose the combination of post-mortem CT angiography and image-guided biopsy of the myocardium to determine the cause of death after chest pain [23]. The aim of this study was to investigate the role of single-organ post-mortem multidetector coronary artery computed tomography angiography applied in cases of sudden cardiac death in adults, and to compare this method with conventional autopsy and histological examination as the reference standard.
Materials and methods
Subjects
We prospectively evaluate all autopsy cases from 2011 to 2013 performed at the Institute of Legal Medicine of the Catholic University of the Sacred Heart in Rome. According also to previous studies [15, 24, 25], the inclusion criteria were the following: suspected sudden cardiac death, post-mortem interval (time from death to scanning) ranged from several hours to 28 h, with a mean interval of 21 h (range, 15–28 h), absence of macroscopic extra-cardiac lethal findings. A total of 11 cases (male cadavers), with mean age at the time of death of 51 years (range, 33–75 years), met the above reported criteria and were enrolled in the present research.
Autopsy
The autopsies were conducted by board-certified forensic pathologists according to internationally recognized recommendations at European level [26]. All the cases underwent a complete traditional autopsy, including brain examination. The heart was removed and immediately stored at +4 °C, then transferred into a cooled plastic container to the Department of Radiology, “Campus Bio-Medico” University in Rome. The mean interval between imaging and autopsy of heart was 2 h (range, 1–3 h). The cause of death was preliminarily established as sudden cardiac death and subsequently clarified on the basis of autopsy findings, and radiological and histological results.
Preparation of the heart and imaging
An isolated single-organ computed tomography (CT) coronarography, using an iodinated non-ionic contrast medium, was performed on isolated heart, after the autopsy. The aorta was cut 1 cm above the orifice of the coronary arteries, and then the heart was located in a plastic container to maintain the heart’s natural shape and size and previously scanned without the administration of contrast medium, in order to determine the presence and the distribution of calcified coronary artery wall plaques. After the initial scanning, the coronary ostia were selectively catheterized manually with a “head-hunter” 5-French catheter by the forensic pathologist and radiologist (M.P.). The 3 ml iodinated contrast media (Xenetix 350-Lobitridolo-Guerbet-France) was injected in each coronary ostium with automated injector at a rate of 0.3 ml/s in order to avoid artifacts during the procedure. Images were acquired on a 64-slice computed tomography scanner (Somatom Sensation Cardiac, Siemens Medical Solutions, Erlangen, Germany) using the thinnest collimation available (detector configuration 32 × 0.6 mm; 120 kV, and 250 mAs). Images were reconstructed by using a soft-tissue reconstruction kernel (B20) and a CT-angio optimized window with section thicknesses of 0.75 mm, using an increment interval of 0.5 mm. Datasets were transferred to a dedicated workstation (Leonardo 2.2, Siemens Medical Solutions, Erlangen, Germany) for the post-processing reconstructions. Multiplanar reconstruction (MPR), maximum intensity projection (MIP), curved planar reconstruction (CPR), and volume rendering (VR) were obtained.
Radiological interpretation
Images were reviewed by two experienced radiologists blinded to autopsy data (P.S. with 5 years of CT angiography imaging experience and B.B.Z. with 30 years of CT imaging and 9 years of forensic imaging experience). Criteria for cardiac evaluation included left ventricular myocardial thickness, arterial enhancement of the left ventricular myocardium, and grade of stenosis on the basis of visual inspection on curved planar reconstructions (CPRs) and maximum intensity projections (MIPs). The degree of stenosis was calculated as previously reported [27]. CAD was graded as follows: no significant or minimal disease (<50 % stenosis), intermediate or significant disease (50–75 % stenosis), or severe disease (>75 % stenosis). The absence of contrast media filling the arterial lumen was considered as occlusion.
Heart dissection and histology
After CT examination, all the isolated hearths were carried to the autopsy pathologist (VA), and conventional macroscopic section and histology assessment were performed on them. The pathologist was blinded to radiological results and collected five myocardial tissue samples from each heart (anterior, lateral and posterior left ventricular wall, septum, right ventricle). The samples were fixed in 10 % neutral-buffered formalin and embedded in paraffin, according to standard procedures. Tissue sections were then stained with hematoxylin–eosin. The myocardial ischemic damage was staged according to the Lodge-Patch classification [28] (Table 1)
Further post-mortem investigations
Histological examination of the remaining organs and toxicological investigation of the body fluids collected at autopsy (blood, urine, vitreous humor) were also performed.
Data analysis
The results of autopsy and histologic examination were compared with the post-mortem coronary computed tomography angiography findings. The causes of death, determined at conventional autopsy followed by histologic examination, were compared with those deduced by using the postmortem CT coronarography. The inter-reader agreement was determined using the Cohen K test, which is a statistical measure [29] of inter-reader agreement or inter-annotator agreement for qualitative (categorical) items. It is generally thought to be a more robust measure than simple percent agreement calculation, since K takes into account the agreement occurring by chance.
Results
In 6 out of 11 cases (Table 2: case numbers 1, 4, 6, 7, 8, and 9), autopsy investigation together with histology stains validated the cause of death (myocardial infarction) enhanced previously by PMCTA scanning. Moreover, in these cases, contrast medium extravasation was noticed at the PMCTA analysis in the left ventricular myocardium, corresponding to the area of distribution of the coronary disease (severe stenosis or anomaly). Therefore, PMCTA confirmed the overlap between the myocardial contrast medium extravasation area with the ischemic/infarcted area observed at the autopsy investigation.
In 1 out of 11 cases (Table 2: case number 2), myocardial infarction had been missed at the PMCTA.
In 2 out of 11 cases (Table 2: case numbers 3 and 5), the death was attributed to the calcific aortic valve stenosis. Of notice in case number 3, PMCTA demonstrated the extravasation of the anterolateral and apical of the left ventricular myocardium, although no sign of myocardial infarction was observed at the autopsy.
In the remaining two cases (Table 2, case numbers 10 and 11), where both PMCTA and autopsy showed no obvious pathological findings, toxicological investigations were positive for lethal intoxication of drugs. In all cases, according to previous studies, PMCTA was a valuable tool for the investigation of the main coronary artery lumens and side branches. The two readers considered evaluable all the isolated hearths. Inter-reader agreement was excellent (Cohen K > 0.75).
Regarding the degree of atherosclerosis, PMCTA showed normal coronary vessels (no atheroma or minimal [<50 %] stenosis) in three cases (Table 2, case numbers 3, 10, and 11), intermediate, or significant (50–75 % stenosis) obstructive atheroma in one case (Table 2, case number 5), and severe (>75 % stenosis) obstructive coronary artery disease in six cases (Table 2, numbers 1, 2, 4, 7, 8, and 9). Of note, surprisingly, case number 2 was the one where PMCTA missed the main diagnosis (myocardial infarction). Myocardial bridging was noted at the level of medial circumflex artery in one case (Table 2, case number 6).
Discussion
In the last decade, CT and MRI have been increasingly used in routine forensic practice and research, and, recently, also in cases of natural deaths. Sudden cardiac deaths (SCD) represent an important part of forensic practice. In fact, the cause of death is most frequently cardiovascular in origin with ischemic heart disease being most common in the general population in industrialized countries [3]. In 2008, Grabherr at al. introduced the use of a modified heart–lung machine to establish post-mortem circulation, in turn, allowing the injection of a contrast agent and constant perfusion of a body [17].
At present, multidetector CT, CT angiography (CTA), and cardiac MRI are used in post-mortem radiological investigation of cardiovascular pathologies [14].
PMCTA is also very useful for the detection of stenoses and occlusions of coronary arteries, but less so for the identification of ischemic myocardium [15, 30–32]. MRI is the method of choice for the radiological investigation of the myocardium in clinical practice, but its accessibility and application are still limited in postmortem practice.
Postmortem MR (PMMR) examination of ischemic myocardium was first performed on eight autopsy cases in 2006 by Jackowski et al. These authors demonstrated that PMMR enables the detection of myocardial infarction in situ and the estimation of infarct age based on signal behavior [33]. In post-mortem imaging, cardiovascular pathologies have been analyzed by only a few groups [15, 19, 31, 32, 34]. While PMCTA allows morphological evaluation of coronary arteries and the detection of suspected stenoses and occlusions, PMMR provides superior soft tissue visualization [15, 19, 31, 32, 34, 35].
In the field of the cardiovascular pathology, the post-mortem radiological examination is often not sufficient to establish the exact cause of death, and autopsy remains the gold standard. At present, there are no non-invasive techniques that can replace histological examination [14]. In our study, a technique already used in the past [36] was chosen to analyze the single organs after the removal, due to difficulties related to the management of the corpse in the absence of a radiological dedicated equipment or a specialized machinery as the modified heart–lung bypass machine to establish post-mortem circulation [16, 17].
Moreover, single-organ postmortem computed tomography angiography is simpler to implement to standard autopsy. Our study demonstrated good visualization of the coronary arteries lumen, enabling the detection of stenoses and occlusions, as well demonstrated in other reports [15, 30–32].
The same studies suggested that it is not possible to diagnose an acute myocardial infarction, primary myocyte disease, or myocarditis, with PMCT and PMCTA, as these techniques have yet to be sufficiently validated [14, 22]. Previous studies focused on the agreement between autopsy, histology, and PMCTA regarding the presence of critical coronary stenosis [37]. In our study, we specifically evaluated through PMTCA analysis transmural contrast media extravasation in the wall of the left ventricular myocardium, and we were able to detect this pathological phenomenon in 7 out of 11 cases. Specifically, in six out of seven, the area of extravasation corresponded to the distribution area of the coronary artery affected by disease demonstrating the main cause of death (myocardial infarction) confirmed by autopsy and histological examination. In the remaining case (one out of seven), extravasation area did not correlated with signs of myocardial infarction observed at the autopsy. In this case, the main cause of death was calcification of aortic valve leaflets and was therefore labeled as false-positive (Figs. 1 and 2.

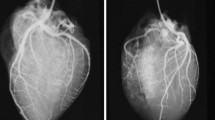
Case 1. a 3D volume-rendering reconstruction demonstrates left anterior descending and circumflex coronary arteries lumen and the left ventricular myocardial extravasation area (arrow); b curved planar reconstruction with thin-slab maximum intensity projection shows a severe stenosis at the level of proximal left anterior descending artery (arrow); c myocardial transversal section showing the infarcted area (lateral wall); d sclerosis and atherosclerotic lesion of the left anterior descending coronary artery (arrow); e–f histological sample stained with hematoxylin and eosin showing ischemic damage (stage I of Lodge-Patch)

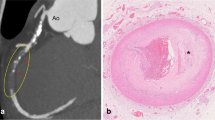
Case 4. a 3D volume-rendering reconstruction of the precontrast CT scan demonstrates extensive calcifications of the left coronary system arteries interesting left main and both left anterior descending and circumflex coronary arteries (small arrows). Note the calcification of the aortic root walls (curved arrow). b 3D volume-rendering reconstruction after injection of contrast medium in the coronary arteries lumen. Note the filling defect at the level of left main consistent with severe stenosis (arrow). c maximum-intensity projection reconstruction confirms the lack of opacification of the left mail lumen (curved white arrow) and the left ventricular myocardial extravasation area (black arrows); note the presence of an early opacified venous vessel crossing behind the left descending coronary artery (b–c). d Heart transversal section with ischemic damage matching the PTMCA images; e anterior descending coronary artery (cross-section) showing critical stenosis. f Histological sample stained with hematoxylin and eosin showing ischemic damage (stage V with foci of stage I of Lodge-Patch)
In the remaining 4 cases out of 11, those samples where myocardial contrast medium extravasation was not observed at PMTCA analysis, one had severe CAD, visible also in PMTCA, and the autopsy and histological examination showed the presence of myocardial infarction. This case was labeled as false-negative. In the other three cases, the main cause of death was respectively identified in one case as severe calcific aortic valve stenosis and in the last two cases as acute drug intoxication including heroine and cocaine (Table 1).
Regarding the advantages in using this technique, we do believe that it is a diagnostic tool available in every radiology department. Although several weaknesses have been already described [19] with the use of this kind of contrast medium, we obtained a good contrast enhancement of the vascular tree (U.H. > 300), coronary arteries showed physiologic dimension, and the penetration of the surrounding myocardial tissue was not considered a major limitation for the histological analysis. Also, post-mortem clots were not a major limitation in our series. For these reasons, single-organ PMCTA could be considered an effective technique for the detection of coronary artery disease. In fact, it could represent a useful support to the conventional autoptical and histological approach, allowing a more accurate coronary artery evaluation and the myocardial sampling, in order to reduce the inaccuracy in post-mortem diagnosis and to improve pre-mortem clinical diagnosis. To achieve extensively this purpose, more studies and a larger population are necessary to validate this method for the identification of myocardial infarcted area. We believe that, although macroscopic examination of different organs at autopsy and subsequent histological evaluation represent the gold standard, the use of PMCTA can be considered as an effective preliminary examination before proceeding to the anatomical dissection in cases of suspected sudden cardiac death.
In conclusion, PMTCA techniques using injected contrast agents are very useful for the detection of coronary stenoses and occlusions, but, till now, the suspected diagnosis must be confirmed visually at autopsy and/or histologically. Certainly, the combination of post-mortem PMTCA techniques with conventional autopsy appears to increase the results of post-mortem investigations in cases of natural death.
Limitation of the study
The main limitation of this study is that the injection of an iodinated contrast agent in the coronary vessels has been made before performing the histology evaluation. This action could be considered invasive and may be able to produce some modifications in the myocardial tissue. In fact, the contrast agent injections leading to extravasations can heavily affect histology. The answer to this criticism is that, in our series, we have used iodinated contrast media injected in each coronary ostium with automated injector at a rate of 0.3 ml/s in order to maintain the pressure stable during the injection with the specific purpose to avoid artifacts. However, further research is needed to establish definitively the significance of the extravasation sign. Furthermore, we need to take into account additional limitations concerning the limited number of cases enrolled in our research and the absence of the control group. The cohort of controls could be very important to make appropriate correlation and discrimination between pathological phenomenon and/or artifacts. Moreover, the results of our preliminary research need to be considered cautiously as soon as further observations will assess definitively the correlation, which is missing in our study, between the dimensions of the infarction areas assessed at PMCTA combined with histology.
References
Sen-Chowdhry S, McKenna WJ (2006) Sudden cardiac death in the young: a strategy for prevention by targeted evaluation. Cardiology 105:196–206
Partemi S, Berne PM, Batlle M, Berruezo A, Mont L, Riuró H, Ortiz JT, Roig E, Pascali VL, Brugada R, Brugada J, Oliva A (2010) Analysis of mRNA from human heart tissue and putative applications in forensic molecular pathology. Forensic Sci Int 203(1–3):99–105
Chugh SS, Reinier K, Teodorescu C, Evanado A, Kehr E, Al Samara M, Mariani R, Gunson K, Jui J (2008) Epidemiology of sudden cardiac death: clinical and research implications. Prog Cardiovasc Dis 51(3):213–228
Thomas AC, Knapman PA, Krikler DM, Davies MJ (1988) Community study of the causes of ‘natural’ sudden death. BMJ 297:1453–1456
Leach IH, Blundell JW, Rowley JM, Turner DR (1995) Acute ischaemic lesions in death due to ischaemic heart disease. An autopsy study of 333 cases of out-of-hospital death. Eur Heart J 16:1181–1185
Priori SG, Aliot E, Blomstrom-Lundqvist C, Bossaert L, Breithardt G, Brugada P, Camm AJ, Cappato R, Cobbe SM, Di Mario C, Maron BJ, McKenna WJ, Pedersen AK, Ravens U, Schwartz PJ, Trusz-Gluza M, Vardas P, Wellens HJJ, Zipes DP (2001) Task force on sudden cardiac death of the European Society of Cardiology. Eur Heart J 22:1374–1450
Priori SG, Aliot E, Blomstrom-Lundqvist C, Bossaert L, Breithardt G, Brugada P et al (2003) Update of the guidelines on sudden cardiac death of the European Society of Cardiology. Eur Heart J 24:13–15
Urbania TH, Hope MD, Huffaker SD, Reddy GP (2009) Role of computed tomography in the evaluation of acute chest pain. J Cardiovasc Comput Tomogr 3(1 Suppl):S13–S22
Mowatt G, Cook JA, Hillis GS et al (2008) 64-Slice computed tomography angiography in the diagnosis and assessment of coronary artery disease: systematic review and meta-analysis. Heart 94(11):1386–1393
Sparrow PJ, Merchant N, Provost YL, Doyle DJ, Nguyen ET (2009) Paul NS CT and MR imaging findings in patients with acquired heart disease at risk for sudden cardiac death. RadioGraphics 29(3):805–823
Campuzano O, Allegue C, Partemi S, Iglesias A, Oliva A, Brugada R (2014) Negative autopsy and sudden cardiac death. Int J Legal Med 128:599–606
Oliva A, Brugada R, D’Aloja E, Boschi I, Partemi S, Brugada J, Pascali VL (2011) State of the art in forensic investigation of sudden cardiac death. Am J Forensic Med Pathol 32(1):1–16
Madea B, Saukko P, Oliva A, Musshoff F (2010) Molecular pathology in forensic medicine—introduction. Forensic Sci Int 203(1–3):3–14
Michaud K, Grabherr S, Jackowski C, Bollmann MD, Doenz F, Mangin P (2014) Postmortem imaging of sudden cardiac death. Int J Legal Med 128(1):127–137
Michaud K, Grabherr S, Doenz F, Mangin P (2012) Evaluation of postmortem MDCT and MDCT-angiography for the investigation of sudden cardiac death related to atherosclerotic coronary artery disease. Int J Cardiovasc Imaging 28(7):1807–1822
Thali MJ, Dirnhofer R, Vock P (2009) The virtopsy approach: 3D optical and radiological scanning and reconstruction in forensic medicine. CRC Press, London
Grabherr S, Gygax E, Sollberger B et al (2008) Two-step post-mortem angiography with a modified heart–lung machine: preliminary results. AJR 190(2):345–351
Ross S, Spendlove D, Bolliger S, Christe A, Oesterhelweg L, Grabherr S et al (2008) Post-mortem whole-body CT angiography: evaluation of two contrast media solutions. Am J Roentgenol 190:1380–1389
Grabherr S, Djonov V, Yen K, Thali MJ, Dirnhofer R (2007) Postmortem angiography: review of former and current methods. Am J Roentgenol 188(3):832–838
Jackowski C, Persson A, Thali MJ (2008) Whole body post-mortem angiography with a high viscosity contrast agent solution using poly ethylene glycol as contrast agent dissolver. J Forensic Sci 53:465–468
Jackowski C, Sonnenschein M, Thali MJ, Aghayev E, von Allmen G, Yen K et al (2005) Virtopsy: post-mortem minimally invasive angiography using cross section techniques—implementation and preliminary results. J Forensic Sci 50:1175–1186
Rutty G, Saunders S, Morgan B, Raj V (2012) Targeted cardiac post-mortem computed tomography angiography: a pictorial review. Forensic Sci Med Pathol 8:40–47
Ross SG, Thali MJ, Bolliger S, Germerott T, Ruder TD, Flach PM (2012) Feasibility of virtual autopsy with postmortem CT angiography and biopsy. Radiology 264: (1)
Jackowski C, Schwendener N, Grabherr S, Persson A (2013) Post-mortem cardiac 3-T magnetic resonance imaging: visualization of sudden cardiac death? J Am Coll Cardiol 62(7):617–629
Jackowski C, Christe A, Sonnenschein M, Aghayev E, Thali MJ (2006) Postmortem unenhanced magnetic resonance imaging of myocardial infarction in correlation to histological infarction age characterization. Eur Heart J 27(20):2459–2467
Brinkmann B (1999) Harmonization of medico-legal autopsy rules. Committee of Ministers. Council of Europe. Int J Legal Med 113(1):1
Weissleder R, Wittenberg J, Harisinghani MG, Chen J (2007) Cardiac imaging: acquired heart disease. In: Primer of diagnostic imaging. 4th ed. Philadelphia, Pa: Mosby Elsevier; 149
Lodge-Patch I (1951) The ageing of cardiac infarcts and its influence on cardiac rupture. Br Heart J 13:37–42
Berry CC (1992) The kappa statistic. JAMA 268(18):2513–2514
Grabherr S, Doenz F, Steger B, Dirnhofer R, Dominguez A, Sollberger B, Gygax E, Rizzo E, Chevallier C, Meuli R, Mangin P (2010) Multi-phase post-mortem CT angiography: development of a standardized protocol. Int J Legal Med: 1–12
Roberts ISD, Benamore RE, Peebles C, Roobottom C, Traill ZC (2011) Diagnosis of coronary artery disease using minimally invasive autopsy: evaluation of a novel method of post-mortem coronary CT angiography. Clin Radiol 66(7):645–650
Saunders S, Morgan B, Raj V, Robinson C, Rutty G (2011) Targeted post-mortem computed tomography cardiac angiography: proof of concept. Int J Legal Med: 1–8
Jackowski C, Christe A, Sonnenschein M, Aghayev E, Thali MJ (2006) Postmortem unenhanced magnetic resonance imaging of myocardial infarction in correlation to histological infarction age characterization. Eur Hear J 27(20):2459–2467
Jackowski C, Warntjes M, Berge J, Bär W, Persson A Magnetic resonance imaging goes postmortem: noninvasive detection and assessment of myocardial infarction by postmortem MRI. Eur Radiol 21(1): 70–78.
Roberts ISD, Benamore RE, Benbow EW, Lee SH, Harris JN, Jackson A, Mallett S, Patankar T, Peebles C, Roobottom C, Traill ZC (2011) Post-mortem imaging as an alternative to autopsy in the diagnosis of adult deaths: a validation study. Lancet 379(9811):136–142
Schlesinger MJ (1938) An injection plus dissection study of coronary artery occlusions and anastomosis. Am Heart J 15:528–568
Morgan B, Biggs MJ, Barber J, Raj V, Amoroso J, Hollingbury FE, Robinson C, Rutty GN (2013) Accuracy of targeted post-mortem computed tomography coronary angiography compared to assessment of serial histological sections. Int J Legal Med 127(4):809–817
Author information
Authors and Affiliations
Corresponding author
Additional information
Antonio Oliva and Riccardo Rossi are co-senior authors.
Rights and permissions
About this article

Cite this article
Polacco, M., Sedati, P., Arena, V. et al. Visualization of myocardial infarction by post-mortem single-organ coronary computed tomography: a feasibility study. Int J Legal Med 129, 517–524 (2015). https://doi.org/10.1007/s00414-014-1085-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-014-1085-y