
Abstract
This study assessed the correlation between stature and scapular measurements in a Japanese population, using three-dimensional (3D) computed tomographic (CT) images, and derived regression equations for predicting stature. A total of 194 cadavers (100 males 94 females) underwent postmortem CT (PMCT) and subsequent forensic autopsy in our department between May 2011 and April 2014. Left and right longitudinal scapular lengths (LLSL and RLSL, respectively) and left and right transverse scapular lengths (LTSL and RTSL, respectively) were measured on 3D CT reconstructed images that extracted only scapular data. The correlation between stature and each of the scapular measurements were analyzed using Pearson product–moment correlation coefficients. The four variables correlated significantly with stature, regardless of sex. The LLSL measurement had the lowest standard error of estimation value among all subjects (4.22 cm) and among all females (4.37 cm), whereas the RLSL measurement had the lowest standard error of estimation value among all males (3.75 cm). The results of this study indicate that scapular measurements may be useful for the forensic estimation of the stature of Japanese individuals, particularly in cases where better predictors, such as long bone lengths, are unavailable.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Along with sex, age, and ancestry, stature is a biological characteristic that can be determined from a skeleton, even many years after death [1, 2]. Therefore, skeletal stature estimation plays a crucial role in the medicolegal investigation of unidentified human remains. To estimate stature, mathematical methods that require bone measurements from skeletal remains are commonly used. These methods are based on sex- and population-specific regression formulae developed from correlations between stature and skeletal element measurements. In the forensic literature, many papers have been published concerning stature estimation equations, based on long bone measurements, because these measurements allow accurate estimates to be made [3, 4]. However, long bone measurements are sometimes unavailable in cases of mass disasters, burns, or skeletal cases [5]. In preparation for situations in which measurable long bones are unavailable, the correlation between stature and other bones must be investigated [6].
Some researchers have previously assessed the correlation between stature and various skeletal elements such as the sternum [7, 8], vertebrae [9–11], sacrum [12, 13], and pelvis [5, 14]. However, few studies have examined the feasibility of estimating stature using scapular measurements. Although Campobasso et al. [6] and Giurazza et al. [15] analyzed the relationship between scapular measurements and stature in an Italian population, our search of the literature revealed that these correlations using three-dimensional (3D) multidetector computed tomographic (MDCT) images have not been investigated in a Japanese population. The great variability in body proportions among different populations is well known, and a method determined for one population is applicable only to subjects belonging to the same ethnic group [16]. Therefore, different formulae are required for different populations.
To date, few authors have applied computed tomographic (CT) scanning techniques to anthropometric studies [12, 14, 15, 17, 18]. Recently, postmortem computed tomography (PMCT) using MDCT has started to be routinely performed in some forensic departments [14]. The 3D images of bones can be immediately generated from MDCT data using CT values, and forensic investigators can examine bones on CT images without the removal of surrounding tissues or the cleansing of the bones even when the subject is not a skeletonized sample. Therefore, if the evaluation of the scapula using 3D CT images is useful for stature estimation, the time and cost of forensic investigations could be reduced.
The aims of this retrospective study were to assess the correlation between stature and scapular measurements in a Japanese population using 3D CT images and to establish new regression equations for stature prediction.
Materials and methods
This study protocol was approved by the Ethics Committee of Chiba University, and the need for approval from the subjects’ relatives was waived.
Data were reviewed for 194 subjects of known age and sex who underwent PMCT and subsequent forensic autopsy at the Department of Legal Medicine at Chiba University between May 2011 and April 2014. The subjects included 100 male cadavers (range 21–86 years; mean age 54.2 ± 16.0 years) and 94 female cadavers (range 32–92 years; mean age 62.8 ± 15.9 years). The estimated postmortem interval of the subjects was <14 days for all subjects. The exclusion criteria of the subjects were scapular fractures, burn injuries, back injuries, and acquired or congenital abnormalities.
At the beginning of each autopsy, the cadaver stature was measured using the same method as in our previous study [14]. The adjusted stature (AS, cm) was calculated by subtracting 2.0 cm from the measured stature, to compensate for postmortem changes including reduced spinal curvature.
PMCT was performed using a 16-row detector CT system (Eclos, Hitachi Medical, Tokyo, Japan). The scanning protocol was as follows: collimation, 1.25 mm; reconstruction interval, 1.25 mm; tube voltage, 120 kVp; tube current, 200 mAs; and rotation time, 1/s. A hard filter was used. Image data were processed on a workstation (Synapse Vincent, Fujifilm Medical, Tokyo, Japan) to obtain orthogonal multiplanar reconstruction images and volume-rendered images.
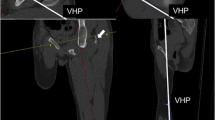
For assessment, a 3D CT reconstructed image which extracted only scapulae using CT value data was used. Left and right longitudinal scapular lengths (LLSL and RLSL, respectively), i.e., the linear distances from the ends of the left and right scapular angles to the superior margins of the left and right coracoid processes, were measured (Fig. 1a and b). Left and right transverse scapular lengths (LTSL and RTSL, respectively), i.e., the linear distances from the left and right medial scapular margins to the inferior margins of the left and right glenoid cavities, were also measured (Fig. 1a and c). These scapular measurements were performed using electronic cursors to the nearest 0.1 mm.

A reconstructed three-dimensional computed tomographic image showing a the linear distance from the end of the scapular angle to the superior margin of the coracoid process (the longitudinal scapular length (LSL)) and the linear distance from the medial scapular margin to the inferior margin of the glenoid cavity (the transverse scapular length (TSL)) in the coronal plane viewed from the anterior side of the body; b the LSL in the sagittal plane viewed from the lateral side of the body; and c the TSL in the axial plane viewed from the inferior side of the body
In order to evaluate intraobserver and interobserver errors, repeated measurements for 20 images selected randomly from the subjects were performed by both the original researcher and another one.
All statistical analyses were performed on a personal computer using SPSS version 21.0 computer software (IBM, Armonk, NY, USA) and Excel software (Microsoft Office 2007, Microsoft, Redmond, WA, USA). The means and standard deviations of AS and the four scapular measurements (LLSL, LTSL, RLSL, and RTSL) were calculated for all subjects as well as separately for the males and females. The technical error of measurement (TEM), the relative technical error of measurement (rTEM, %), and the coefficient of reliability (R) were calculated to evaluate intraobserver and interobserver errors. The allowance of rTEM for intraobserver and interobserver error using beginner anthropometrist levels was up to 1.5 and 2.0 %, respectively [19]; an R value >0.95 was considered sufficiently precise [20]. The correlations between AS and each of the scapular measurements were examined by simple regression analysis using Pearson product–moment correlation coefficient (r); a p value <0.05 was considered statistically significant.
Multiple stepwise regression analyses were also performed using the multiple scapular measurements. The Shapiro-Wilk test was used to determine whether the response variables were normally distributed; a p value >0.05 showed normal distribution of the data.
The adjusted coefficient of determination (r 2), standard error of estimation (SEE, cm), and 95 % confidence interval (95 % CI) were calculated to evaluate the significance of the regression. In order to compare the results of this study with those of Giurazza et al. [15], the mean of the error of absolute value (E, %) was calculated using the following formula to assess the difference between stature estimated using each of the simple regression equations (ES) and AS; n represents the numbers of total, male, and female subjects.
Results
The descriptive statistics of age, AS, and the four scapular measurements are shown in Table 1. The mean stature of the male subjects was 16 cm taller than that of the female subjects. The intraobserver error rTEMs were <1.5 % (0.287–0.587 %), and the interobserver error rTEMs were <2.0 % (0.364–0.603 %); the R values were >0.950 (0.958–0.988) (Table 2).
Table 3 shows the results of the simple linear regression analysis using AS and each of the scapular measurements among the total, male, and female subjects. There were significant positive correlations (p < 0.001) between AS and each of the scapular measurements (Fig. 2). Although the r values for male subjects (0.590–0.755) were similar to those for female subjects (0.552–0.816), the SEE values for male subjects (3.75–4.62 cm) were lower than those for female subjects (4.37–6.31 cm). The SEE values for all subjects ranged from 4.22 to 6.14 cm. The r values between the AS values and the longitudinal scapular lengths (LSLs, comparatively large values) were greater than those between the AS values and the transverse scapular lengths (TSLs, small values). The strongest correlations and the lowest SEE values were found for the LLSLs among all subjects and among the female subjects, and for the RLSLs among the males. The E values for males (1.79–2.16 %) were lower than those for females (2.20–3.34 %). The E values for the LSLs were also lower than those for the TSLs in both sexes.

Scatter plots comparing a the left longitudinal scapular length (LLSL) and the adjusted stature (AS), b the left transverse scapular length (LTSL) and AS, c the right longitudinal scapular length (RLSL) and AS, and d the right transverse scapular length (RTSL) and AS (closed circles represent male subjects; open circles represent female subjects)
The results of the multiple stepwise regression analysis are shown in Table 4. The response variables were normally distributed. The r 2 values of the multiple regression equations were almost equivalent to those for the simple regression equations derived from the LSLs. The SEE values of the multiple regression equations using left variables for all subjects and for females were very slightly lower than those for the simple regression equations; however, the SEE values for the multiple regression equations using the other variables were very slightly higher than those for the simple regression equations.
Discussion
Cadaver stature differs from the stature of a living individual because of physiologic changes, such as the lessening of the curvature of the spine, occurring after death [17, 21]. Therefore, the possibility cannot be ruled out that the formulae derived using statures measured at the beginning of an autopsy may not accurately estimate living stature. Previous researchers have reported that the body length increases by approximately 2.0 cm after death [22, 23]. For this reason, the AS was calculated by subtracting 2.0 cm from the measured stature before evaluating the correlations between stature and the scapular measurements.
In addition, Falsetti [24] reported that forensic stature, which is the stature recorded on driver’s licenses, medical records, and other documents, is often greater than the stature directly measured from a cadaver. On the other hand, measured stature is sometimes greater than the stature described on driver’s licenses because the individuals failed to update their driver’s license information after growth [24, 25]. Thus, if the stature information used in the identification process is derived from personal documents, it tends to confound stature estimations; therefore, AS values were used in the statistical analyses conducted as part of the present study.
The main findings of this study were the significant positive correlations between AS and the several scapular measurements. In particular, the SEE values calculated using longitudinal scapular length (LSL) were less than 5 cm regardless of sex, indicating the feasibility of stature estimations from scapular measurements. However, the 95 % CI values calculated using LSL were approximately 8 cm, suggesting that the estimation method in this study may be of limited value when used in forensic case work. The pooled sex correlation values, namely the r values for all subjects, were probably higher than the within-sex correlation values because of sex differences. Previous studies revealed that male subjects are taller than female subjects in all populations because of the later onset of puberty and the later fusion of the epiphyses in males [26, 27]. However, the sex of severely decomposed or skeletonized human remains is usually unknown. Therefore, regression equations for the pooled sex subjects are vital in addition to the separate equations for male and female subjects.
Hasegawa et al. [28] obtained very low SEE values (male subjects 2.63–2.85 cm; female subjects 2.87–3.03 cm) for stature estimation from measurements of the femur and tibia using dual-energy X-ray absorptiometry in a contemporary Japanese population. The results of our previous study [18] showed slightly lower SEE values (all 4.18–4.72 cm; male subjects 4.09–4.58 cm; female subjects 4.21–4.58 cm) based on the lengths of the radius and ulna than those obtained in this study. In addition, the scapula is fragile and in most cases at least partly damaged. Therefore, using long bones is always the better choice for precise stature estimation whenever one long bone is available. However, the results of this study indicate that scapular measurements may be useful for the forensic estimation of the stature of Japanese individuals, particularly in cases where long bones are no more available, but the scapula is still available.
The present study demonstrated sex differences in the SEE and E values. These results may be due to age differences; the mean age of the female subjects studied in this report was approximately 8 years older than that of the male subjects. Nichilson et al. [29] examined 420 scapulae and reported that the incidence of anteroinferior acromial spur increased with specimen age. Thus, the possibility cannot be excluded that age-related spur formations may also be observed in the glenoid cavities and the coracoid processes which comprise part of the shoulder joint along with acromion. Further studies on the structural changes of the glenoid cavity and the coracoid process relative to age are required.
In the present study, the r 2 and SEE values provided by the multiple regression equations were similar to those obtained using the simple regression equations and LSL measurements regardless of sex, indicating that the simple linear regression equations using LSL measurements are as reliable for stature estimation as the multiple stepwise regression equations. Therefore, when the LSL of an unidentified cadaver can be measured, there may be no need to perform multiple scapular measurements to estimate the subject’s stature.
Table 5 shows a summary of the r, SEE, and E values for the simple regression formulae used to estimate stature based on scapular measurements. Campobasso et al. [6] examined the correlation between stature and scapular measurements using dry bones in a Southern Italian population and obtained smaller r values and similar SEE values compared with those in our study, probably due to the substantially fewer subjects examined in their study. Those authors also reported a larger r value for the transverse scapular length (TSL) measurements than for the LSL measurements in the male subjects. However, Giurazza et al. [15] assessed the correlation between stature and the scapular measurements in an Italian population using CT and reported that the LSL had a stronger correlation with stature than the TSL regardless of sex, in accordance with the present study. The E values Giurazza et al. [15] obtained for female subjects were smaller than those in our study, suggesting that the SEE values which were not reported might also have been smaller. There have been a few reports of anthropometric evaluations based on CT imaging. Giurazza et al. [17] compared measurements of the femur and skull with living statures in an Italian population and concluded that CT is one of the most accurate and precise techniques for the study of bone morphometry. We recently assessed the relationship between stature and pelvic bone measurements using MDCT and developed regression equations to estimate stature in a modern Japanese population; we obtained comparatively low SEE values (male 3.72–5.14 cm; female 5.02–5.57 cm) [14]. In addition, other researchers reported that image analysis of bones in a CT sample is useful for age estimation and superimposition [30–32]. Because digital CT images can be permanently stored in little or no physical space, repeated measurements can be performed even after autopsy, resulting in an effective increase in intraobserver and interobserver reproducibility [33]. Although all CT examinations deliver high radiation doses that should not be applied to living individuals for stature estimation [15], radiation exposure is inconsequential during routine cadaveric examinations. However, special CT-skills may be necessary to achieve reliable results, when working with 3D CT imaging.
Sakuma et al. [34] measured skull lengths with calipers and subsequently re-measured the skulls using reconstructed 3D CT images in our department. They reported no significant difference between the actual measurements and the measurements based on 3D CT images. Therefore, the scapular CT measurements are considered to be similar to actual physical measurements performed on dry bones using calipers. In other words, stature estimation based on physical scapular measurements may be possible in forensic departments and institutes that are not equipped with CT scanners.
To the best of our knowledge, this is the first study to derive regression equations for stature estimation using scapular measurements in a Japanese population. Our study concludes that scapular measurements may be useful for stature estimation in the Japanese population, particularly in circumstances in which more accurate skeletal elements, such as intact long bones, are not available for analysis. Similar studies on the correlations between stature and the scapular measurements in different ethnic groups are warranted in order to compile a list of helpful regression equations for forensic investigations.
References
Gocha TP, Vercellotti G, McCormick LE, Van Deest TL (2013) Formulae for estimating skeletal height in modern South-East Asians. J Forensic Sci 58:1279–1283
Ahmed AA (2013) Estimation of stature from the upper limb measurements of Sudanese adults. Forensic Sci Int 228:178.e1–178.e7
Krishan K, Kanchan T, Asha N (2012) Estimation of stature from index and ring finger length in a North Indian adolescent population. J Forensic Leg Med 19:285–290
Bidmos MA (2008) Stature reconstruction using fragmentary femora in South Africans of European descent. J Forensic Sci 53:1044–1048
Giroux CL, Wescott DJ (2008) Stature estimation based on dimensions of the bony pelvis and proximal femur. J Forensic Sci 53:65–68
Campobasso CP, Di Vella G, Introna F Jr (1998) Using scapular measurements in regression formulae for the estimation of stature. Boll Soc Ital Biol Sper 74:75–82
Marinho L, Almeida D, Santos A, Cardoso HF (2012) Is the length of the sternum reliable for estimating adult stature? A pilot study using fresh sterna and a test of two methods using dry sterna. Forensic Sci Int 220:292.e1–292.e4
Macaluso PJ Jr, Lucena J (2014) Stature estimation from radiographic sternum length in a contemporary Spanish population. Int J Legal Med [Epub ahead of print]
Terazawa K, Takatori T, Mizukami K, Tomii S (1985) Estimation of stature from somatometry of vertebral column in Japanese. Nihon Hoigaku Zasshi 30:35–40
Terazawa K, Akabane H, Gotouda H, Mizukami K, Nagao M, Takatori T (1990) Estimating stature from the length of the lumbar part of the spine in Japanese. Med Sci Law 30:354–357
Jason DR, Taylor K (1995) Estimation of stature from the length of cervical, thoracic and lumbar segments of spine in American whites and blacks. J Forensic Sci 40:59–62
Torimitsu S, Makino Y, Saitoh H, Ishii N, Hayakawa M, Yajima D, Inokuchi G, Motomura A, Chiba F, Iwase H (2014) Stature estimation in Japanese cadavers using the sacral and coccygeal length measured with multidetector computed tomography. Leg Med (Tokyo) 16:14–19
Pelin C, Duyar I, Kayahan EM, Zağyapan R, Ağildere AM, Erar A (2005) Body height estimation based on dimensions of sacral and coccygeal vertebrae. J Forensic Sci 50:294–297
Torimitsu S, Makino Y, Saitoh H, Sakuma A, Ishii N, Hayakawa M, Yajima D, Inokuchi G, Motomura A, Chiba F, Iwase H (2014) Stature estimation in Japanese cadavers based on pelvic measurements in three-dimensional multidetector computed tomographic images. Int J Legal Med [Epub ahead of print]
Giurazza F, Del Vescovo R, Schena E, Cazzato RL, D’Agostino F, Grasso RF, Silvestri S, Zobel BB (2013) Stature estimation from scapular measurements by CT scan evaluation in an Italian population. Leg Med (Tokyo) 15:202–208
Krishan K, Kanchan T, Sharma A (2012) Multiplication factor versus regression analysis in stature estimation from hand and foot dimensions. J Forensic Leg Med 19:211–214
Giurazza F, Del Vescovo R, Schena E, Battisti S, Cazzato RL, Grasso FR, Silvestri S, Denaro V, Zobel BB (2012) Determination of stature from skeletal and skull measurements by CT scan evaluation. Forensic Sci Int 222:398.e1–398.e9
Torimitsu S, Makino Y, Saitoh H, Sakuma A, Ishii N, Hayakawa M, Yajima D, Inokuchi G, Motomura A, Chiba F, Iwase H (2014) Stature estimation based on radial and ulnar lengths using three-dimensional images from multidetector computed tomography in a Japanese population. Leg Med (Tokyo) 16:181–186
Jamaiyah H, Geeta A, Safiza MN, Khor GL, Wong NF, Kee CC, Rahmah R, Ahmad AZ, Suzana S, Chen WS, Rajaah M, Adam B (2010) Reliability, technical error of measurements and validity of length and weight measurements for children under two years old in Malaysia. Med J Malaysia 65:131–137
Arroyo M, Freire M, Ansotegui L, Rocandio AM (2010) Intraobserver error associated with anthropometric measurements made by dietitians. Nutr Hosp 25:1053–1056
Hauser R, Smoliński J, Gos T (2005) The estimation of stature on the basis of measurements of the femur. Forensic Sci Int 147:185–190
De Mendonca MC (2000) Estimation of height from the length of long bones in a Portuguese adult population. Am J Phys Anthropol 112:39–48
Mahakkanukrauh P, Khanpetch P, Prasitwattanseree S, Vichairat K, Troy Case D (2011) Stature estimation from long bone lengths in a Thai population. Forensic Sci Int 210:279.e1–279.e7
Willey P, Falsetti T (1991) Inaccuracy of height information on driver’s licenses. J Forensic Sci 36:813–819
Ousley SD (1995) Should we estimate biological or forensic stature? J Forensic Sci 40:768–773
Rastogi P, Nagesh KR, Yoganarasimha K (2008) Estimation of stature from hand dimensions of north and south Indians. Leg Med (Tokyo) 10:185–189
Abdel-Malek AK, Ahmed AM, El-Sharkawi SA, El-Hamid NA (1990) Prediction of stature from hand measurements. Forensic Sci Int 46:181–187
Hasegawa I, Uenishi K, Fukunaga T, Kimura R, Osawa M (2009) Stature estimation formulae from radiographically determined limb bone length in a modern Japanese population. Leg Med (Tokyo) 11:260–266
Nicholson GP, Goodman DA, Flatow EL, Bigliani LU (1996) The acromion: morphologic condition and age-related changes. A study of 420 scapulas. J Shoulder Elbow Surg 5:1–11
Lopez-Alcaraz M, Gonzalez PM, Aguilera IA, Lopez MB (2014) Image analysis of pubic bone for age estimation in a computed tomography sample. Int J Legal Med [Epub ahead of print]
Chiba F, Makino Y, Motomura A, Inokuchi G, Torimitsu S, Ishii N, Sakuma A, Nagasawa S, Saitoh H, Yajima D, Hayakawa M, Odo Y, Suzuki Y, Iwase H (2013) Age estimation by multidetector CT images of the sagittal suture. Int J Legal Med 127:1005–1011
Lorkiewicz-Muszyńska D, Kociemba W, Żaba C, Łabęcka M, Koralewska-Kordel M, Abreu-Głowacka M, Przystańska A (2013) The conclusive role of postmortem computed tomography (CT) of the skull and computer-assisted superimposition in identification of an unknown body. Int J Legal Med 127:653–660
Karakas HM, Celbis O, Harma A, Alicioglu B (2011) Total body height estimation using sacrum height in Anatolian Caucasians: multidetector computed tomography-based virtual anthropometry. Skeletal Radiol 40:623–630
Sakuma A, Ishii M, Yamamoto S, Shimofusa R, Kobayashi K, Motani H, Hayakawa M, Yajima D, Takeichi H, Iwase H (2010) Application of postmortem 3D-CT facial reconstruction for personal identification. J Forensic Sci 55:1624–1629
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical standards
This study complies with the current laws of the country in which it was performed.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Torimitsu, S., Makino, Y., Saitoh, H. et al. Stature estimation in Japanese cadavers based on scapular measurements using multidetector computed tomography. Int J Legal Med 129, 211–218 (2015). https://doi.org/10.1007/s00414-014-1054-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-014-1054-5