
Abstract
The aim of this study was to assess the accuracy of Cameriere’s methods on dental age estimation in the northern Chinese population. A sample of orthopantomographs of 785 healthy children (397 girls and 388 boys) aged between 5 and 15 years was collected. The seven left permanent mandibular teeth were evaluated with Cameriere’s method. The sample was split into a training set to develop a Chinese-specific prediction formula and a test set to validate this novel developed formula. Following the training dataset study, the variables gender (g), x 3 (canine teeth), x 4 (first premolar), x 7 (second molar), N 0, and the first-order interaction between s and N 0 contributed significantly to the fit, yielding the following linear regression formula: Age = 10.202 + 0.826 g − 4.068x 3 − 1.536x 4 − 1.959x 7 + 0.536 N 0 − 0.219 s ⋅ N 0, where g is a variable, 1 for boys and 0 for girls. The equation explained 91.2 % (R 2 = 0.912) of the total deviance. By analyzing the test dataset, the accuracy of the European formula and Chinese formula was determined by the difference between the estimated dental age (DA) and chronological age (CA). The European formula verified on the collected Chinese children underestimated chronological age with a mean difference of around −0.23 year, while the Chinese formula underestimated the chronological age with a mean difference of −0.04 year. Significant differences in mean differences in years (DA − CA) and absolute difference (AD) between the Chinese-specific prediction formula and Cameriere’s European formula were observed. In conclusion, a Chinese-specific prediction formula based on a large Chinese reference sample could ameliorate the age prediction accuracy in the age group of children.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Age estimation in children and adolescents plays an important role in forensic medicine, which provides evidence for the judgment of criminal and civil responsibility. According to Chinese criminal law, children under 14 have no criminal responsibility, subjects from 14 to 16 have limited criminal responsibility, and those over 16 have full criminal responsibility [14]. China’s civil law considers children under 10 as having no civil responsibility, teenagers from 10 to 18 as having partial civil responsibility, while those over 18 as having full civil responsibility [16]. In addition, age estimation also plays a key role in the adoption of children if the date of birth is uncertain.
Many methods have been developed for dental age assessment based on the permanent dentition observed in radiographs. Evaluation of the clinical emergence in the mouth and the radiographic evaluation of teeth mineralization are the two main methods [7, 11, 22, 29]. As the clinical eruption of permanent teeth is easily affected by exogenous factors, such as feeding habits, local trauma, the pathology of deciduous teeth, and so on, recent studies favor using tooth mineralization rather than eruption in chronological age assessment [4, 10, 21]. In order to quantify a continuous process from the first traces of cusp mineralization until root apex closure, many researchers suggested a different number of radiographic stages, ranging from three stages to possibly 40 stages [7, 13, 18, 20].
In 2006, Cameriere et al. developed a linear regression formula for chronological age estimation in children according to the relation between age and measurement of open apices in seven left permanent mandibular teeth roots in 455 Italian Caucasian children [1]. In 2007, they published another paper with additional samples of children from various European states, providing a common formula useful for all these countries [2]. It has been reported recently by several other groups that Cameriere’s method is accurate and very useful for estimating the chronological age of children in Brazilian, Bosnian-Herzegovian, and Mexican children groups [6, 8, 9].
However, no studies have been conducted on Chinese children and adolescents to assess the applicability of Cameriere’s formula and to find out whether this formula turns out to be suitable for the Chinese population too. The aims of present study are twofold: firstly, to verify Cameriere’s age estimation model on a sample of Chinese children, and, secondly, to develop a Chinese-specific formula based on Cameriere’s method.
Materials and methods
Study population
A sample of 785 orthopantomographs of healthy northern Chinese children, aged between 5 and 15 years and taken during a course of diagnosis and treatment, was selected (Table 1). The orthopantomograms were taken at the Department of Oral Radiology in the Affiliated Stomatological Hospital of Xi’an Jiaotong University Health Science Center, China, from February 2012 to May 2013. The selection criteria were good image quality and free of any medical or pathology affecting tooth development visible on the panoramic radiographs. The chronological age of each subject was calculated by subtracting the date of birth from the date of the radiograph. The age proof is in the form of birth certificate, school/college register, or identity card. Radiographs were in digital form and images were recorded on computer files, which were processed using a computer-aided drafting program (Adobe Photoshop 7). To avoid bias, prior to data scoring, all images were relabeled randomly in numeric order and all related information was made anonymous.
Among the personal data for patients, the identification number, date of birth, date of radiograph, and gender were collected; the parents of the patients signed an agreement with the stomatological hospital that dental records and radiographs would be used only for research and educational purposes, without personal identification. Ethical approval for this study was obtained from the Ethics Committee of the Affiliated Stomatological Hospital of Xi’an Jiaotong University Health Science Center, China.
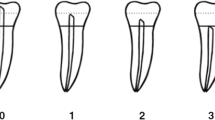
The method is explained in detail by Cameriere et al. [1]. Briefly, radiographs of seven left permanent mandibular teeth, with the apical ends of the roots completely closed (N 0), were examined. Teeth with incomplete root development, i.e., with open apices, were also examined. For teeth with one root, the distance Ai, i = 1,…, 5, between the inner sides of the open apex was measured. For teeth with two roots, Ai, i = 6, 7, the sum of the distances between the inner sides of the two open apices was evaluated. In order to take into account the effect of possible differences among X-rays in magnification and angulations, measurements were normalized by dividing by tooth length (Li, i = 1,…, 7). Dental maturity was evaluated according to the normalized measurements of the seven left mandibular permanent teeth (xi = Ai/Li, i = 1,…, 7), the sum of normalized open apices (s), and the number (N 0) of teeth with root development complete. Lastly, age was calculated with the European formula:
where g is a variable, 1 for boys and 0 for girls.
Statistical analysis and data management
All measurements were carried out by the same observer. To test intra-observer reproducibility, an independent 40 randomly selected radiographs were re-examined after an interval of 1 month and the kappa test was performed. The Cameriere et al. formula, developed on a reference sample of Italian white children [1], was verified on the collected northern Chinese children sample.
The children sample was randomly divided into a training dataset and a test dataset but stratified on age (categories) and gender (Table 2). A Chinese-specific prediction formula, utilizing the Cameriere et al. method [1], was fitted on the subjects in the training dataset. A multiple linear regression model with first-order interactions was developed by selecting variables which contributed significantly to age estimations according to the stepwise selection method. The test dataset was used to verify the constructed Chinese-specific prediction formula and the original Cameriere et al. formula. To compare the age prediction performances, the error of the age prediction was defined as the difference between the dental age and the chronological age (DA − CA). For calibration purposes, the mean differences of DA and CA were expressed to quantify the direction of the error (overestimation or underestimation) and the absolute differences of DA and CA, to quantify the magnitude of the error. Paired samples t test was applied to assess the significances of the difference between DA and CA for the two formulas. Non-parametric Wilcoxon signed-rank test was also applied to assess the significances of the difference between DA and CA because the sample was having non-normal distribution in some age groups. An independent sample t test was used to compare absolute accuracy between genders for each formula.
All statistical analyses were performed using SPSS 13.0. When the p value was less than 0.05, the results were considered statistically significant.
Results
Statistical analysis revealed no statistically significant intra-observer differences between the paired sets of measurements carried out on the re-examined orthopantomograms. The result of the weighted Cohen kappa score for repeatability of the number of closed apices was 1.00. The concordance correlation coefficient for the paired sets of measurements of the sum of normalized open apices (s) was 0.982.
Following the results reported in [1], subjects’ age was modeled as a function of the morphological variables and the results showed that not all the variables used for the European model were significant predictors of age in the northern Chinese sample. In particular, no second premolar and s variables were significant, while statistical analysis showed that in the northern Chinese sample, the morphological variables x 3 (canine teeth), x 4 (first premolar), and x 7 (second molar) were significant predictors of age, which were not significant in the European model (Table 3).
The results showed that these variables contributed significantly to the fit, partly unlike the variables used for the European formula, yielding the following linear regression formula for the northern Chinese population:
where g is a variable, 0 for girls and 1 for boys.
In Eq. 2, only the intercept varies with gender, and therefore, sexual dimorphism does not change with age. But, the equation points out earlier the dental maturity of girls at all ages. Equation 2, with the considered variables, explained 91.2 % (R 2 = 0.912) of the total deviance.
For girls, the mean (standard deviation) CA was 10.21 years (0.30 year). According to the European formula (Eq. 1), the mean DA was 10.17 years (0.24 year). The mean DA was 10.19 years (0.28 year) according to the Chinese formula (Eq. 2). For boys, the mean CA was 10.07 years (0.29 year). The mean DA was 9.64 years (0.20 year) according to the European formula and 10.00 years (0.25 year) according to the Chinese formula. Results comparing accuracy by the two formulas for girls and boys are shown in Table 4, and the distribution of the results into the age cohorts for girls and boys separately are given in Table 5 and Figs. 1, 2.

Girls’ boxplot of the differences between the dental age and the chronological age (DA − CA) for the 5–15-year age groups according to the European formula and Chinese formula. The boxplot shows the median and interquartile range; whiskers indicate the range. DE shows the results of the European formula; DC shows the results of the Chinese formula

Boys’ boxplot of the differences between the dental age and the chronological age (DA − CA) for the 5–15-year age groups according to the European formula and Chinese formula. The boxplot shows the median and interquartile range; whiskers indicate the range. DE shows the results of the European formula; DC shows the results of the Chinese formula
According to the European formula, the DA was found to be underestimated but not statistically significant (p = 0.640), with a mean difference of 0.03 year for girls. It was underestimated with a mean difference of 0.43 year for boys, while the difference between the DA and the CA for boys was significant from zero (p = 0.001). The DA was found to be underestimated according to the Chinese formula, with a mean difference of 0.01 year for girls and 0.06 year for boys. The difference between the DA and the CA for both genders was not found statistically significant (p > 0.05).
The mean values of absolute differences for the two formulas are presented in Table 4 and distribution of the results into the age cohorts for girls and boys separately are given in Table 6 and Figs. 3, 4. For the European formula, the absolute differences were 0.86 year for girls and 1.12 years for boys. The difference between the two mean absolute differences for both genders was statistically significant (p = 0.002). For the Chinese formula, the mean absolute differences were 0.60 year for girls and 0.67 year for boys. Although absolute accuracy was better for girls than for boys, statistical significance was not found between genders (p = 0.272).

Girls’ boxplot of the absolute differences between the dental age and the chronological age (DA − CA) for 5–15-year age groups according to the European formula and Chinese formula. The boxplot shows the median and interquartile range; whiskers indicate the range. DEabsolute shows the results of the European formula; DCabsolute shows the results of the Chinese formula

Boys’ boxplot of the absolute differences between the dental age and the chronological age (DA − CA) for 5–15-year age groups according to the European formula and Chinese formula. The boxplot shows the median and interquartile range; whiskers indicate the range. DEabsolute shows the results of the European formula; DCabsolute shows the results of the Chinese formula
Mean differences in years with 95 % confidence intervals between the DA and the CA for age cohorts of both genders are shown in Table 5. In the Chinese formula, the mean differences between the estimated DA and the CA for girls and boys were less than a year per age cohort except for the age group of 15 years, while in the European formula, the mean differences in years (DA − CA) of three age cohorts were more than 1 year for the girls and those of seven age cohorts were more than 1 year for the boys.
Discussion
Age estimation is of great importance in forensic medicine both for living persons and human postmortem remains. According to the Study Group on Forensic Age Diagnostic (AGFAD), three independent parts contribute to the estimation of chronological age, including physical examination, X-ray examination of the left hand, and dental examination with the determination of the dental status and X-ray examination of the dentition. If the skeletal development of the hand is complete, an additional plain radiography, computed tomography (CT), or magnetic resonance imaging (MRI) of the sterna extremity of the clavicle is recommended [12, 26, 28]. Recently, radiological examination of the ossification of the distal radius and iliac crest apophysis and the distal tibial and calcaneum epiphysis has been studied in estimating the age of living individuals [25, 27, 30]. Among them, it is known that teeth can be preserved longer than bone and dental development is less affected by environmental quality and genetic factor than skeletal development [23]. It is generally accepted that the development of the crown and roots of growing teeth is commonly used in estimating the dental age of children [5].
Selecting a good method includes low bias and low mean/median absolute difference. Accuracy is the degree of error or average deviation in a measurement as calculated from the true value. An accurate method has no bias; that is, the mean difference between dental age and chronological age is zero or close to zero. Reliability can be tested by conducting inter-observer or intra-observer variation studies to determine error rates. It means the degree to which a method produces the same results when it is used at different times. The standard deviation of the mean difference between dental age and chronological age refers to the precision or reliability of the estimated age [17, 24]. A better method demonstrates the highly consistent over-repeated measurements of the same individual and a smaller difference between dental age and chronological age [3]. Cameriere et al. [1] developed an age estimation method based on the relationship between age and measured open apices of seven left permanent teeth. Comparing the accuracy of this method with the widely used Demirjian et al. method [7] and with the method proposed by Willems et al. [29], the Cameriere method was the most accurate; median underestimations were −0.081 and −0.036 year for girls and boys, respectively, while the Demirjian method overestimated the real age with a median residual error of −0.750 year for girls and −0.611 year for boys, respectively. In the Willems method, the median underestimation was −0.073 year for girls and boys were overestimated at 0.247 year. The mean absolute differences for the Demirjian and Willems methods were 1.13 years and 0.93 year for girls and 1.01 years and 0.93 year for boys, respectively, which were both less accurate compared with the Cameriere method, which were 0.48 year for girls and 0.50 year for boys [3]. Recently, the method has been tested in several parts of the world, including Europe, India, Brazil, Mexico, and Egypt [2, 6, 8, 19, 23]. However, a Chinese sample had never been studied.
In the present study, a northern Chinese-specific prediction formula was fitted on the sample of 556 individuals in the training dataset. The variables “canine,” “first premolar,” and “second molar” contributed significantly to the fit and were therefore included in the regression equation. The canine and first premolar have been used in Kvaal’s method for age estimation and have proved to be reliable in the estimation of age [15]. Moreover, they are single-rooted teeth and the measurement of open apices is easier. The second molar was included in the Chinese formula, and it is possible that the open apices of the second molar are the last to be closed among the teeth, excluding third molars, which are at the ages between 12 and 15 years in healthy children.
A new northern Chinese sample of 229 individuals in the test dataset was examined in order to ascertain whether the European formula can predict age accurately or whether Chinese-specific equations could improve the age assessment. For girls, according to the European formula, the mean DA was underestimated by the range of differences of −0.14 year to −1.31 years for the 8-, 9-, 11-, 12-, 13-, 14-, and 15-year-old groups, whereas it was overestimated by the means of differences of 0.67 year to 1.46 years for the 5-, 6-, 7-, and 10-year-old groups. According to the Chinese formula, the DA was underestimated by the mean differences of −0.03 year to −1.05 years for the 8-, 9-, 11-, 14-, and 15-year-old groups and it was overestimated for the 5-, 6-, 7-, 10-, 12-, and 13-year-old groups by the mean differences of 0.10 year to 1.02 years. The mean differences for the Chinese formula were significantly better than those of the European formula except for the 8- and 10-year-old groups. For boys, the mean DA was overestimated according to the European formula by the range of differences of 0.13 year to 1.79 years for the age groups from 5 to 8 years, whereas it was underestimated by the means of differences of −0.47 year to −1.90 years for the age groups from 9 to 15 years. The DA was underestimated at −0.06 year according to the Chinese formula by the range of differences of −1.06 year to 0.89 year for all age groups. The mean differences for the Chinese formula were significantly more accurate than those for European formula except for the 7- and 8-year-old groups.
When the equation is applied to older children (15–15.99 years) with closed apices, the estimated chronological age will be the same regardless of their age. For girls of the 15-year-old group, the mean DA was underestimated by −1.05 years according to the Chinese formula by the range of differences of −1.05 to −1.05 years. For boys, the mean DA was underestimated for −1.06 years according to the Chinese formula by the mean of differences of −1.75 years to −0.38 year for the 15-year-old group. The significant decrease in accuracy in this age cohort may be attributed to the almost complete maturation of the teeth. This is in accordance with Cameriere et al.[1] who proposed that the predicted age in younger children could be more accurate than that in older ones.
The mean absolute difference quantifies the distance from the true age and does not consider whether dental age is overestimated or underestimated. Mean absolute differences for the European formula were 0.86 year and 1.12 years for girls and boys, respectively, whereas the absolute accuracy for the Chinese formula for both genders was significantly more accurate (p < 0.001) which were 0.60 and 0.67 year for girls and boys, respectively. The medians of the absolute differences for the European formula were 0.75 and 0.94 year for girls and boys, while according to the Chinese formula, the medians of absolute differences were 0.51 and 0.48 year for girls and boys, respectively.
According to literature, there are no other published articles about age estimation in Chinese children by measurements of the open apices of the seven left permanent mandibular teeth. This study is the first to develop a Chinese-specific prediction formula based on Cameriere’s method and to compare the accuracy on age estimation with the previous European formula in a test sample. In a country as large as China, the factors, such as ethical, social, and nutritional, probably influence children’s growth differently. Future studies should focus on the effects of the regional background, gender, nutrition factor, and chronological age distribution of the sample on the accuracy and reliability of dental age assessment in Chinese children.
Conclusion
Cameriere’s European formula verified on northern Chinese children underestimates chronological age in both genders, and the significant differences were only found in the boys’ group. A Chinese-specific prediction formula based on a large Chinese reference sample could ameliorate the age prediction accuracy in the age group of children.
References
Cameriere R, Ferrante L, Cingolani M (2006) Age estimation in children by measurement of open apices in teeth. Int J Legal Med 120:49–52
Cameriere R, De Angelis D, Ferrante L, Scarpino F, Cingolani M (2007) Age estimation in children by measurement of open apices in teeth: a European formula. Int J Legal Med 121:449–453
Cameriere R, Ferrante L, Liversidge HM, Prieto JL, Brkic H (2008) Accuracy of age estimation in children using radiograph of developing teeth. Forensic Sci Int 176:173–177
Chen JW, Guo J, Zhou J, Liu RK, Chen TT, Zou SJ (2010) Assessment of dental maturity of western Chinese children using Demirjian's method. Forensic Sci Int 197(119):e111–e114
Cunha E, Baccino E, Martrille L, Ramsthaler F, Prieto J, Schuliar Y, Lynnerup N, Cattaneo C (2009) The problem of aging human remains and living individuals: a review. Forensic Sci Int 193:1–13
De Luca S, De Giorgio S, Butti AC, Biagi R, Cingolani M, Cameriere R (2012) Age estimation in children by measurement of open apices in tooth roots: study of a Mexican sample. Forensic Sci Int 221(155):e151–e157
Demirjian A, Goldstein H, Tanner JM (1973) A new system of dental age assessment. Hum Biol 45:211–227
Fernandes MM, Tinoco RL, de Braganca DP, de Lima SH, Francesquini Junior L, Daruge Junior E (2011) Age estimation by measurements of developing teeth: accuracy of Cameriere's method on a Brazilian sample. J Forensic Sci 56:1616–1619
Galic I, Vodanovic M, Cameriere R, Nakas E, Galic E, Selimovic E, Brkic H (2011) Accuracy of Cameriere, Haavikko, and Willems radiographic methods on age estimation on Bosnian-Herzegovian children age groups 6-13. Int J Legal Med 125:315–321
Guo YC, Yan CX, Lin XW, Zhang WT, Zhou H, Pan F, Wei L, Tang Z, Liang F, Chen T (2014) The influence of impaction to the third molar mineralization in northwestern Chinese population. Int J Legal Med 128:659–665
Guo YC, Yan CX, Lin XW, Zhou H, Pan F, Wei L, Tang Z, Liang F, Chen T (2014) Studies of the chronological course of third molars eruption in a northern Chinese population. Arch Oral Biol 59:906–911
Hillewig E, Degroote J, Van der Paelt T, Visscher A, Vandemaele P, Lutin B, D'Hooghe L, Vandriessche V, Piette M, Verstraete K (2013) Magnetic resonance imaging of the sternal extremity of the clavicle in forensic age estimation: towards more sound age estimates. Int J Legal Med 127:677–689
Hunt EE Jr, Gleiser I (1955) The estimation of age and sex of preadolescent children from bones and teeth. Am J Phys Anthropol 13:479–487
Jun L (2005) Investigation on disputed issues about criminal responsibility of criminal minor in China. J Liaoning Univ (Phil Soc Sci) 33:34–39
Kvaal SI, Kolltveit KM, Thomsen IO, Solheim T (1995) Age estimation of adults from dental radiographs. Forensic Sci Int 74:175–185
Lengfu Z (2006) On minors’ civil liability ability. J Shangluo Teach Coll 20:59–63
Liversidge HM, Smith BH, Maber M (2010) Bias and accuracy of age estimation using developing teeth in 946 children. Am J Phys Anthropol 143:545–554
Moorrees CF, Fanning EA, Hunt EE Jr (1963) Age variation of formation stages for ten permanent teeth. J Dent Res 42:1490–1502
Nik-Hussein NN, Kee KM, Gan P (2011) Validity of Demirjian and Willems methods for dental age estimation for Malaysian children aged 5-15 years old. Forensic Sci Int 204(208):e201–e206
Nolla C (1960) The development of the permanent teeth. J Dent Child 27:254–266
Olze A, Bilang D, Schmidt S, Wernecke KD, Geserick G, Schmeling A (2005) Validation of common classification systems for assessing the mineralization of third molars. Int J Legal Med 119:22–26
Olze A, van Niekerk P, Ishikawa T, Zhu BL, Schulz R, Maeda H, Schmeling A (2007) Comparative study on the effect of ethnicity on wisdom tooth eruption. Int J Legal Med 121:445–448
Rai B, Kaur J, Cingolani M, Ferrante L, Cameriere R (2010) Age estimation in children by measurement of open apices in teeth: an Indian formula. Int J Legal Med 124:237–241
Ritz-Timme S, Cattaneo C, Collins MJ, Waite ER, Schutz HW, Kaatsch HJ, Borrman HI (2000) Age estimation: the state of the art in relation to the specific demands of forensic practise. Int J Legal Med 113:129–136
Saint-Martin P, Rerolle C, Dedouit F, Bouilleau L, Rousseau H, Rouge D, Telmon N (2013) Age estimation by magnetic resonance imaging of the distal tibial epiphysis and the calcaneum. Int J Legal Med 127:1023–1030
Schmeling A, Grundmann C, Fuhrmann A, Kaatsch HJ, Knell B, Ramsthaler F, Reisinger W, Riepert T, Ritz-Timme S, Rosing FW, Rotzscher K, Geserick G (2008) Criteria for age estimation in living individuals. Int J Legal Med 122:457–460
Schmidt S, Schiborr M, Pfeiffer H, Schmeling A, Schulz R (2013) Age dependence of epiphyseal ossification of the distal radius in ultrasound diagnostics. Int J Legal Med 127:831–838
Schulz R, Muhler M, Reisinger W, Schmidt S, Schmeling A (2008) Radiographic staging of ossification of the medial clavicular epiphysis. Int J Legal Med 122:55–58
Willems G, Van Olmen A, Spiessens B, Carels C (2001) Dental age estimation in Belgian children: Demirjian's technique revisited. J Forensic Sci 46:893–895
Wittschieber D, Vieth V, Wierer T, Pfeiffer H, Schmeling A (2013) Cameriere's approach modified for pelvic radiographs: a novel method to assess apophyseal iliac crest ossification for the purpose of forensic age diagnostics. Int J Legal Med 127:825–829
Acknowledgments
The authors would like to thank Dr. Juan Yin, Pei-feng Liang, and Ya-ling Zhao for their help with data analysis. This work was supported by the Scientific Research Foundation of the Education Ministry and HR Ministry of China for the Returned Overseas Scholars (SLZ2008010), the Science and Technology Research Program, and the International Co-operation Project of Shaanxi (2006k8-G6) for C.-X. Yan.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article

Cite this article
Guo, Yc., Yan, Cx., Lin, Xw. et al. Age estimation in northern Chinese children by measurement of open apices in tooth roots. Int J Legal Med 129, 179–186 (2015). https://doi.org/10.1007/s00414-014-1035-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-014-1035-8