
Abstract
The ability to estimate stature from various parts of the body is essential in medicolegal investigations, particularly in cases in which human remains have been dismembered or mutilated. Therefore, the aim of this study was to generate linear regression models for predicting stature on the basis of sternum length in contemporary Spaniards. Sternal length, or the combined length of the manubrium and mesosternum, was recorded from digital radiographs of the chest plate for 65 males and 52 females. Correlation coefficients for the regression models were r = 0.391 and r = 0.461 for the male and female formulae, respectively. The standard errors of the estimate were 6.20 cm for the male equation and 5.56 cm for the female equation. Given these relatively large standard error rates, the derived stature estimation models should only be used when other more accurate skeletal elements, such as intact long bones, are unavailable for analysis.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The estimation of stature, or living height, is an important component in the analysis of unidentified human remains. The most accurate method for reconstructing stature involves the measurement of all skeletal elements that contribute to living height, including the cranium, vertebrae, femur, tibia, talus, and calcaneus [1–3]. The sum total of these measurements is then added to an appropriate soft tissue factor to provide an estimate of stature. However, this anatomical method cannot be applied in many cases as human remains recovered from forensic contexts are often incomplete and damaged. As a result, the most commonly employed methods are based on the positive linear relationship between stature and the length of various parts of the body. Individual long bones of the upper (humerus, ulna, and radius) and particularly the lower (femur, tibia, and fibula) extremities are often used in the derivation of regression equations for the estimation of stature [4–9]. Regression formulae have also been devised for fragmentary long limb bones [10–12], as well as other postcranial elements, such as the metacarpals [13, 14], metatarsals [15–17], scapula [18], and segments of the vertebral column [19–21].
Recently, researchers have developed regression equations for stature estimation based on the length of the sternum in several different population groups, including South Indians [22, 23], Northwest Indians [24], and Portuguese [25]. Although these stature formulae are not as accurate (higher standard errors of estimate) as equations derived from measurements of intact long bones of the arm and leg or short bones of the hand and foot, the authors [22–24, but see 25] suggest that they may be of some use in contexts in which human remains are recovered without the extremities. Therefore, the primary objective of the present investigation was to generate linear regression models which can be used to predict stature on the basis of sternum length in contemporary Spaniards, given that equations for stature estimation based on other skeletal elements are generally population-specific and thus cannot be accurately applied to other human groups. An additional, but related, aim was to evaluate the utility of sternal measurements derived from digital radiographs in estimating stature, which provides an alternative method to those based on dry bone specimens or fresh sterna.
Materials and methods
The data used in the present study were obtained from decedents undergoing routine postmortem examination at the Forensic Pathology Service, Institute of Legal Medicine in Seville, Spain, during a 1-year period (August 2012–July 2013). The study sample comprised 117 identified individuals of Spanish Caucasian descent, including 65 males and 52 females, with documented ages at death between 22 and 91 years (Table 1, Fig. 1). The study sample is the same as that employed in a prior investigation which assessed the utility of sternal dimensions for sex estimation [26], but with the addition of a single female specimen.

Age and sex distribution of the study sample
Documented living height (stature) data was not available for the study sample. Therefore, prior to autopsy, cadaver length, measured as the maximum length between the vertex of the head and base of the heel with the body placed in a supine position and in full extension, was recorded to the nearest centimeter using a measuring rod. A number of previous studies, however, have demonstrated that an adjustment factor should be applied to cadaver length given that living height is consistently less than the value recorded postmortem. This discrepancy is primarily due to the compression of intervertebral disks and other joints when a person is standing, the position adopted for the measurement of stature in the living [4, 27–29]. It has also been suggested that the increase in stature postmortem is a result of the lessening of the curvature of the spine in the supine position [29]. It is generally accepted that the extent to which the body lengthens after death is approximately 2.0 cm [6, 13, 30–32], and thus, this correction value was subtracted from cadaver length for each specimen to obtain an estimate of living stature. These corrected stature values were used in the statistical analyses.
The chest plate, consisting of the complete sternum, costal cartilages, and medial ends of the first through seventh ribs, was subsequently excised from cadavers during routine postmortem examination. After removal, calibrated digital radiographs were obtained for all specimens using the Carestream DirectView Vita CR (Carestream Health; Rochester, NY, USA) image acquisition and processing system. Each chest plate was placed directly on top of the photostimuable phosphor (PSP) detector plate with the posterior surface facing the X-ray source, which was directed perpendicular to the surface of the detector plate and at a focus distance of 100 cm. A posterior-anterior orientation was utilized in an effort to obtain proximity of the sternum to the PSP detector plate and align the long axis of the sternum parallel to the detector plate, thus minimizing image magnification and distortion [33, 34]. The exposure parameters were set at 60 kVp and 6.3 mAs for all radiographs. The chest plate was subsequently returned to the body upon completion of the postmortem examination.
Sternal dimensions were recorded from the digital images using the measurement tools included within the image analysis software program associated with the Carestream DirectView radiographic system. Sternum length was calculated as the combined length of the manubrium and mesosternum (Fig. 2). Length of the manubrium was measured, to the nearest tenth of a millimeter, as the midsagittal distance from the suprasternal notch to the manubriosternal junction. Mesosternum, or sternal body, length was measured, to the nearest tenth of a millimeter, as the midsagittal distance from the manubriosternal junction to the mesoxiphoidal junction. In sterna with complete fusion (no fusion scar present) of the manubrium and mesosternum, the midpoint of the left and right articular facets for the second costal cartilage along the lateral borders of the sternum formed the landmark to differentiate the two elements and thus identify the manubriosternal junction [33]. Likewise, in sterna with complete fusion of the mesosternum and xiphoid process, the inferior margin of the left and right articular demifacets for the seventh costal cartilage along the lateral borders of the sternal body formed the landmark to differentiate the mesosternum from the xiphoid process and thus identify the mesoxiphoidal junction [22]. It is important to note that these sternal length measurements are not equivalent to those obtained directly from dry bone specimens. Although digital radiography minimizes magnification error compared to conventional radiography, thus producing more accurate measurements, bone lengths obtained from digital radiographic images may still be slightly larger than those recorded from dry bones using calipers [35]. In addition, dry bones are generally shorter than fresh bones, such as those observed for cadavers during postmortem examination, due to the possible desiccation and shrinkage of skeletonized remains [36–39].

Linear measurements (white lines) used to calculate sternum length: manubrium length (M) and mesosternum, or sternal body, length (B)
Digital radiography was used to record sternal length in order to test the usefulness of this method as an alternative to measurements derived from dry bone specimens or fresh sterna, as proposed in earlier studies [22–25]. An advantage of this radiographic technique is that it can be used with fleshed remains as well as decomposed bodies, particularly in contexts in which maceration, a labor-intensive and time-consuming process, is not feasible or warranted. In addition, digital radiographs and sternal measurements are easily obtained as the chest plate is routinely excised from decedents during postmortem examination to gain access to the thoracic cavity. Furthermore, sternal length was not recorded from fresh specimens during autopsy given that xiphoid process length and shape are highly variable [22, 40], and this element may be absent or remain unfused with the mesosternum even in older individuals [41–43]. Likewise, the manubrium and mesosternum often do not fuse even in later life [41], and as a result, equivalent sternal length measurements may not be accurately recorded for all specimens.
Bodies that were decomposed, burned, mutilated, or displayed physical deformities affecting the measurement of cadaver length were excluded from the study. Likewise, sterna that exhibited trauma or pathology, as assessed from radiographic images, were not included in the sample.
A test of the repeatability of the utilized measurements was performed prior to the statistical analyses. Lengths of the manubrium and mesosternum were recorded a second time by the first author with a minimum of 2 weeks between measurement sessions. Mean intra-observer error, calculated following the equation presented by Albanese et al. [44, 45], was less than 1 % for both dimensions and thus within the acceptable limit (below 2.0–2.5 %).
After verifying the normality of the sternal length data for both sex samples (D’Agostino-Pearson omnibus test: K 2 ≤ 0.260, p ≥ 0.878) and the calculation of descriptive statistics, separate linear regression equations for estimating stature on the basis of sternum length were then devised for males and females, given that previous studies have demonstrated that stature formulae are not only population-specific but also sex-specific [24, 46, 47]. The study sample was randomly divided into two subsamples. A calibration sample, which consisted of 50 males and 42 females, was used to develop the sex-specific linear regression equations. A validation sample comprising the remaining 15 male and 10 female individuals was then used to test the predictive accuracy of the two models. Specifically, model accuracy was assessed by observing the number of individuals in the validation sample whose corrected stature fell within the 95 % confidence interval of the predicted value, following the equation presented by Giles and Klepinger [48]. As discussed by these authors [48, 49], this formula provides a more accurate calculation of the confidence interval of a linear regression equation than simply doubling the standard error of the estimate, particularly when the value of the bone measurement used for the stature estimate deviates considerably from the sample mean.
Results
Corrected stature for the male calibration sample ranged from 148.0 to 176.0 cm, with a mean and standard deviation of 164.4 ± 6.67 cm, and mean sternum length was 157.3 ± 12.12 mm, ranging from 137.1 to 186.3 mm. For the female calibration sample, corrected stature varied between 138.0 and 164.0 cm, with a mean and standard deviation of 152.1 ± 6.19 cm, and mean sternum length was 133.3 ± 11.41 mm, ranging from 102.1 to 155.7 mm.
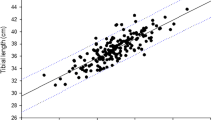
The linear regression analysis for the calibration sample data yielded the following formulae: male stature = 130.515 + 0.215 (sternum length) and female stature = 118.774 + 0.250 (sternum length). Sternal length showed a significant positive correlation with cadaver length in both males and females (p > 0.01). Pearson’s correlation coefficients for the regression models were r = 0.391 and r = 0.461 for the male and female formulae, respectively. The standard errors of the estimate (SEE) were 6.20 cm for the male equation and 5.56 cm for the female equation.
Descriptive statistics for the validation sample, which was not used to develop the regression models, are similar to those for the calibration sample. Mean corrected stature was 168.3 ± 7.42 cm with a range of 155.0 to 184.0 cm for males and 155.1 ± 7.88 cm with a range of 143.0 to 170.0 cm for females. Mean sternal length was 166.7 ± 14.63 mm with a range of 140.2 to 196.0 mm for the male sample and 135.4 ± 10.16 mm with a range of 120.4 to 148.1 mm for the female sample.
When the sternal length data of the validation sample were applied to the above derived linear regression equations, the corrected stature of nearly all 25 individuals fell within the 95 % confidence interval of the predicted value. The confidence interval of the stature estimate did not encompass the corresponding corrected stature for only one female individual (Table 2).
Discussion and conclusions
A number of previous investigations have demonstrated that the bones of the anterior thorax, and in particular the sternum, can be used for the accurate discrimination of sex [26, 50, 51], as well as provide useful information regarding the assessment of age at death [40, 41, 52, 53], of unidentified human remains. In addition, morphological variations or anomalies of the sternum, such as the presence of sternal foramina, may aid in the process of personal identification [40, 43]. Recently, a few studies have also evaluated the potential of the sternum for stature estimation [22–25].
The results obtained in this study demonstrate that sternum length (combined length of the manubrium and mesosternum) has only a weak, albeit statistically significant, association with stature (corrected cadaver length) in the Spanish population. Given the modest relationship between the two variables, the standard errors of the estimate for the regression formulae derived for the Spanish sample were relatively large, ranging between 5.56 cm for females to 6.20 cm for males. In addition, although the 95 % confidence intervals of the predicted values encompassed the correct stature of all but one specimen in the validation sample, these intervals are so wide that they have limited practical application. The purpose of stature estimation in forensic contexts is to narrow the potential list of presumptive identifications, and thus, stature estimates with confidence intervals of approximately 23 cm in females and 25 cm in males, as observed in this study, provide little assistance in discriminating between individuals of similar height [25].
The correlation coefficient and standard error of the estimate values obtained in the current study are generally comparable to those observed in previous investigations which assessed the efficacy of sternal measurements for stature estimation in other population groups. For example, Marinho and colleagues [25] reported a correlation coefficient of 0.329 and a standard error of 6.59 cm for the length, including the xiphoid process, of fresh sterna in a male sample from Portugal. Similarly, Singh et al. [54], in their study of a Northwest Indian population sample, obtained correlation coefficient values of 0.316 for males and 0.328 for females for regression models based on sternal length taken from dry bone specimens which were not degreased or allowed to dry extensively. The corresponding standard errors of the estimate for these regression models were 6.83 and 6.65 cm for males and females, respectively. Menezes et al. [22, 23] obtained higher correlation coefficients and lower standard errors of the estimate for regression models derived from the combined length of the manubrium and mesosternum recorded from dry bone specimens in a South Indian sample. For the male sample, the correlation coefficient was 0.638 and the standard error was 5.64 cm, whereas for the female sample, these two values were 0.639 and 4.11 cm, respectively.
The standard errors of the estimate for the stature formulae derived from the sternal data in the current study are larger than those obtained for measurements of other postcranial bones among contemporary Spaniards, which is not surprising considering that the sternum does not contribute directly to the height of an individual. Muñoz et al. [34], in a radiographic study of the extremities, reported standard errors for length measurements of the lower limb bones (femur, tibia, and fibula) ranging from 3.61 to 4.01 cm in males and 3.03 to 3.27 cm in females. The stature formulae for bones of the upper limb (humerus, radius, and ulna) were slightly less accurate with standard errors ranging from 4.34 to 5.18 cm in the male sample and 3.50 to 3.93 cm in the female sample. More recently, in another radiographic study, Rodríguez and colleagues [55] obtained standard errors of 5.10 and 5.98 cm in males and 4.54 and 4.67 cm in females, for regression models based on length of the first and second metatarsal, respectively. The standard errors of the estimate for the regression formulae for females were lower than those of males for all six long bones of the limbs [34], as well as for the two metatarsals [55]. This pattern was also observed in the current study, in which length of the sternum provided a more accurate stature estimate for the female sample. The greater accuracy in females could be due, in part, to the higher variability in males, as demonstrated by the larger standard deviation value for both cadaver and sternal length measurements.
Taken together, the results indicate that sternal length measurements, derived from digital radiographs, do not provide a highly reliable method for estimating stature in the Spanish population. This finding is in agreement with Marinho and colleagues [25] who emphasized, in contrast to prior investigations [22–24], the limitations of using sternal dimensions for stature prediction in forensic contexts. However, in cases in which bones of the extremities are not present, or maceration cannot be conducted, the regression equations derived in this study may be used to provide a stature estimate.
Limitations
Documented living height (stature) data was not available in all individuals and for that reason was not included in the study sample. However, we do not consider this as a serious limitation given that in most stature studies, only cadaver length is employed.
References
Fully G (1956) Une nouvelle méthode de détermination de la taille. Ann Med Leg 40:266–273
Raxtor MH, Auerbach BM, Ruff CB (2006) Revision of the Fully technique for estimating statures. Am J Phys Anthropol 130:374–384
Raxtor MH, Ruff CB, Auerbach BM (2007) Technical note: revised Fully stature estimation technique. Am J Phys Anthropol 133:817–818
Trotter M, Gleser GC (1952) Estimation of stature from long bones of American whites and Negroes. Am J Phys Anthropol 10:463–514
Lundy JK (1983) Regression equations for estimating living stature from long limb bones in the South African Negro. S Afr J Sci 79:337–338
De Mendonca MC (2000) Estimation of height from the length of long bones in a Portuguese adult population. Am J Phys Anthropol 112:39–48
Celbis O, Agritmis H (2006) Estimation of stature and determination of sex from radial and ulnar bone lengths in a Turkish corpse sample. Forensic Sci Int 158:135–139
Dayal MR, Steyn M, Kuykendall KL (2008) Stature estimation from bones of South African whites. S Afr J Sci 104:124–128
Agnihotri AK, Kachhwaha S, Jowaheer V, Singh AP (2009) Estimating stature from percutaneous length of tibia and ulna in Indo-Mauritian population. Forensic Sci Int 187:109.e1–109.e3
Steele DG, McKern TW (1969) A method for assessment of maximum long bone length and living stature from fragmentary long bones. Am J Phys Anthropol 31:215–228
Chibba K, Bidmos MA (2007) Using tibia fragments from South Africans of European descent to estimate maximum tibia length and stature. Forensic Sci Int 169:145–151
Bidmos MA (2008) Estimation of stature using fragmentary femora in indigenous South Africans. Int J Legal Med 122:293–299
Meadows L, Jantz RL (1992) Estimation of stature from metacarpal length. J Forensic Sci 37:147–154
Zaher JF, El-Ameen NFM, Seedhom AE (2011) Stature estimation using anthropometric measurements from computed tomography of metacarpal bones among Egyptian population. Egypt J Forensic Sci 1:103–108
Byers S, Akoshima K, Curran B (1989) Determination of adult stature from metatarsal length. Am J Phys Anthropol 79:275–279
Bidmos MA (2008) Metatarsals in the estimation of stature in South Africans. J Forensic Leg Med 15:505–509
Cordeiro C, Muños-Barús JI, Wasterlain S, Cunha E, Vieira DN (2009) Predicting adult stature from metatarsal length in a Portuguese population. Forensic Sci Int 193:e1–e4
Giurazza F, Del Vescovo R, Schena E, Cazzato RL, D’Agostino F, Grasso RF, Silvestri S, Zobel BB (2013) Stature estimation from scapular measurements by CT scan evaluation in an Italian population. Leg Med. doi:10.1016/j.legalmed.2013.01.002
Jason DR, Taylor K (1995) Estimation of stature from the length of the cervical, thoracic and lumbar segments of the spine in American whites and blacks. J Forensic Sci 40:59–62
Pelin I, Duyar EM, Kayahan R, Zaĝyapan AM, Ağukdere A, Erar B (2005) Body height estimation based on dimensions of sacral and coccygeal vertebrae. J Forensic Sci 50:294–297
Nagesh KR, Kumar GP (2006) Estimation of stature from vertebral column length in South Indians. Leg Med 8:269–272
Menezes RG, Kanchan T, Kumar GP, Rao PPJ, Lobo SW, Uysal S, Krishan K, Kalthur SG, Nagesh KR, Shettigar S (2009) Stature estimation from the length of the sternum in South Indian males: a preliminary study. J Forensic Leg Med 16:441–443
Menezes RG, Nagesh KR, Monteiro FNP, Kumar GP, Kanchan T, Uysal S, Rao PPJ, Rastogi P, Lobo SW, Kalthur SG (2011) Estimation of stature from the length of the sternum in South Indian females. J Forensic Leg Med 18:242–245
Singh J, Pathak RK, Chavali KH (2011) Skeletal height estimation from regression analysis of sternal lengths in a Northwest Indian population of Chandigarh region: a postmortem study. Forensic Sci Int 206:211.e1–221.e8
Marinho L, Almeida D, Santos A, Cardoso HFV (2012) Is the length of the sternum reliable for estimating adult stature? A pilot study using fresh sterna and a test of two methods using dry sterna. J Forensic Sci 220:292.e1–292.e4
Macaluso PJ Jr, Lucena J (2013) Estimation of sex from sternal dimensions derived from chest plate radiographs in contemporary Spaniards. Int J Legal Med DOI. doi:10.1007/s00414-013-0910-z
Manouvrier L (1892) Determination de la taille d’après les grands os des members. Rev Ecole Anthropol 2:227–233
Pearson K (1899) Mathematical contribution to the theory of evolution: on the reconstruction of the stature of prehistoric races. Philos Trans R Soc Lond (Biol) 192:169–244
Hauser R, Smoliński J, Gos T (2005) The estimation of stature on the basis of measurements of the femur. Forensic Sci Int 147:185–190
Telkkä A (1950) On the prediction of human stature from the long bones. Acta Anat 9:103–117
Radoinova D, Tenekedjiev K, Yordanov Y (2002) Stature estimation from long bone lengths in Bulgarians. HOMO-J Comp Hum Biol 52:221–232
Mahakkanukrauh P, Khanpetch P, Prasitwattanseree S, Vichairat K, Case DT (2011) Stature estimation from long bone lengths in a Thai population. Forensic Sci Int 210:279.e1–279.e7
McCormick WF, Stewart JH, Langford LA (1985) Sex determination from chest plate roentgenograms. Am J Phys Anthropol 68:173–195
Muñoz JI, Liñares-Iglesias M, Suárez-Peñaranda JM, Mayo M, Miguéns X, Rodríguez-Calvo MS, Concheiro L (2001) Stature estimation from radiographically determined long bone length in a Spanish population sample. J Forensic Sci 46:363–366
Kieffer CL (2010) Tibia and fibula stature formulae for modern female populations based on digital radiographic measurements. J Forensic Sci 55:695–700
Rollet É (1888) De la mensuration des os longs des membres dans ses rapports avec l’anthropologie, la clinique et la médecine judiciaire [in French]. Lyon
Ingalls NW (1927) Studies on the femur. III. The effects of maceration and drying in the white and negro. Am J Phys Anthropol 10:297–321
Todd TW, Pyle SI (1928) Effects of maceration and drying upon the vertebral column. Am J Phys Anthropol 12:303–319
Athawale MC (1963) Estimation of height from lengths of forearm bones: a study of one hundred Maharashtrian male adults of ages between twenty-five and thirty years. Am J Phys Anthropol 21:105–112
Singh J, Pathak RK (2013) Sex and age related non-metric variation of the human sternum in a Northwest Indian postmortem sample: a pilot study. Forensic Sci. doi:10.1016/j.forsciint.2013.02.002
Chandrakanth HV, Kanchan T, Krishan K, Arun M, Kumar GNP (2012) Estimation of age from human sternum: an autopsy study on a sample from South India. Int J Legal Med 126:863–868
Yekeler E, Tunaci M, Tunaci A, Dursun M, Acunas G (2006) Frequency of sternal variations and anomalies evaluated by MDCT. Am J Roentgenol 186:956–960
Verna E, Piercecchi-Marti M, Chaumoitre K, Bartoli C, Leonetti G, Adalian P (2013) Discrete traits of the sternum and ribs: a useful contribution to identification in forensic anthropology and medicine. J Forensic Sci Doi:. doi:10.1111/1556-4029.12111
Albanese J (2003) A metric method for sex determination using the hipbone and the femur. J Forensic Sci 48:263–273
Albanese J, Eklics G, Tuck A (2008) A metric method for sex determination using the proximal femur and fragmentary hipbone. J Forensic Sci 53:1283–1288
Bidmos MA, Asala SA (2005) Calcaneal measurement in estimation of stature of South African blacks. Am J Phys Anthropol 126:335–342
Sahni D, Sanjeev, Sharma P, Harjeet, Kaur G, Aggarwal A (2010) Estimation of stature from facial measurements in northwest Indians. Leg Med 12:23–27
Giles E, Klepinger LL (1988) Confidence intervals for estimates based on linear regression in forensic anthropology. J Forensic Sci 33:1218–1222
Klepinger LL (2006) Fundamentals of forensic anthropology. Wiley, Hoboken
Bongiovanni R, Spradley MK (2012) Estimating sex of the human skeleton based on metrics of the sternum. Forensic Sci Int 219:290.e1–290.e7
Franklin D, Flavel A, Kuliukas A, Cardini A, Marks MA, Oxnard C, O’Higgins P (2012) Estimation of sex from sternal measurements in a Western Australian population. Forensic Sci Int 217:230.e1–230.e5
Sun YX, Zhao GC, Yan W (1995) Age estimation on the female sternum by quantification theory I and stepwise regression analysis. Forensic Sci Int 74:57–62
Kaneriya D, Umarvanshi B, Patil D, Mehta C, Chauhan K, Vora R (2013) Age determination from fusion of the sternal elements. Int J Appl Basic Med Res 3:22–29
Singh J, Pathak RK, Singh D (2012) Morphometric sex determination from various sternal widths of Northwest Indian sternums collected from autopsy cadavers: a comparison of sexing methods. Egypt J Forensic Sci. doi:10.1016/j.ejfs.2011.12.002
Rodríguez S, Miguéns X, Rodríguez-Calvo MS, Febrero-Bande M, Muñoz-Barús JI (2013) Estimating adult stature from radiographically determined metatarsal length in a Spanish population. Forensic Sci. doi:10.1016/j.forsciint.2012.12.006
Acknowledgements
The authors thank their colleagues and the technicians at the Forensic Pathology Service, Institute of Legal Medicine, Seville, Spain, for their help and support in conducting this research. The authors also thank the reviewers for their insightful and helpful comments.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Macaluso, P.J., Lucena, J. Stature estimation from radiographic sternum length in a contemporary Spanish population. Int J Legal Med 128, 845–851 (2014). https://doi.org/10.1007/s00414-014-0975-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-014-0975-3