
Abstract
Third molar development was assessed using a sample of 1,131 orthopantomograms from a Portuguese population. The methodology applied was the eight stages (A–H) method described by Demirjian et al. The final sample was made of 739 orthopantomograms, 387 (52.5%) of which belonging to females; age ranged between 6.1 and 22.5 years old (mean age = 14.49, S.D. = 4.37). For each developmental stage, mean age, standard deviation, and minimal and maximal age was assessed; evaluation of the rate formation of each tooth, according to sex, was calculated and data distribution expressed in percentiles for each stage; the probability of an individual being 16 was also evaluated. The relationship between tooth development and chronological age had a statistical significance for all teeth and both sexes (p < 0.0001). The data described may provide reference for forensic application and agree with the thesis that each population need specific data.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Age estimation is an important area of forensic dentistry which has been gaining increasing importance in the past few years. In accordance with the recommendations for age estimation in criminal proceedings of the study group on forensic age diagnostics, for an age estimation, an physical examination, an X-ray examination of the hand, and a dental examination should be carried out; if the skeletal development of the hand is completed, an additional X-ray examination (or CT scan) of the clavicles (medial extremity) should be performed [1].
Developing teeth are a useful indicator of maturation (and hence of biological age) because they are less affected than other body tissues by diseases and environmental insults [2]. Dental development may be measured either by tooth eruption or tooth formation. While eruption is a discontinuous and variable measurement, affected by several factors like malnutrition, premature loss of primary teeth, crowding and dental decay, tooth formation is seen as a more robust measure with high heritability, low coefficient of variation and resistance to environmental effects [2]. Most authors have chosen the eighth-grade scheme of Demirjian for dental age estimation, for reasons of accuracy and practicability. Third molar development is particularly important due to the fact of it being the only teeth still in development by age 16; however, previous findings showed that the mineralization of the wisdom teeth is a population-specific process and does not occur in every ethnic group at the same age [3–5]. According to Olze et al. [6] there are not enough data to decide how ethnic origin affects teeth mineralization, and the forensic value of age estimation depends on it. Therefore, it is crucial to use population-specific reference data in forensic age estimation of living people. Hence, the aim of this study is to obtain data regarding third molar development in a Portuguese population.
Material and methods
A total sample of 1,131 orthopantomogram collected from a Portuguese population aged between 6 and 22 years old was analyzed. The radiographs used were taken from patient files of the Faculty of Dentistry of Porto University, Portugal.
The exclusion criteria were the following:
-
Other nationalities other than Portuguese;
-
Absence of all third molars;
-
Image deformity affecting third molars;
-
Orthopantomogram exhibiting obvious pathology.
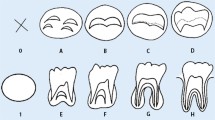
A >cross-sectional study was carried out to assess chronological age based on the stages of third molar development. Dental development was assessed using the method developed by Demirjian et al. [7]. To assess reliability, 80 randomly selected radiographs were examined by the two first authors; 80 randomly selected orthopantomograms were assessed twice by the first author, with a 1 month interval between the two observations. Intra- and interobserver agreement was determined using the Wilcoxon signed ranks. Statistical analysis was performed using the SPSS 16.0 (SPSS Inc., Chicago, IL).
Results
Repeated scoring of 80 radiographs revealed no significant intra- or interobserver differences (p > 0.05). Intraobserver agreement occurred in 95% and interobserver agreement occurred in 93%. The final sample was made of 739 orthopantomograms, 387 (52.5%) of which belonging to females; age ranged between 6.1 and 22.5 years old (mean age = 14.49; S.D. = 4.37). Orthopantomograms distribution, according with age and sex is shown in Table 1. Of the orthopantograms, 17.1% were excluded since they present no third molars; 4.9% presented one third of a molar; 6.1%, two; 6.9% had three third molars; and 65.0% presented all four third molars.
Results were studied according to sex and age for every third molar. Table 2 shows the mean age, standard deviation, standard error of the mean, and minimal and maximal age (in years) for third molars, for stages A–G. For stage H, mean values were not calculated, and the probability of excluding age younger than 18 years old was calculated for every third molar, both for males and females (Table 3). Table 4 presents 50% probability values for stage H.
To allow better visualization of the rate formation of each tooth, according to sex, the data distribution is expressed in percentiles for each stage, in Table 5. The frequency distribution by stages and sex for each group age is shown in Table 6. Stage A was not observed beyond the age group 13–13.9 years, and stage B was rare in those age groups. From stage D onward, all group ages older than 9, for females, and 10, for males, were verified.
A correlation analysis with Spearman rank order correlation (rho) was used to assess the strength and direction of the linear relationship between tooth development and chronological age. There was a strong, positive correlation between the two variables for every tooth in both genders (p < 0.005). The Kruskal–Wallis test was used to check for differences in tooth mineralization according to sex. It was found that, overall, there were statistically significant differences for all third molar mineralization rate in males and females (tooth 18, p = 0.002; tooth 28, p < 0.001; tooth 38, p = 0.005; tooth 48, p = 0.002); however, considering each stage separately, it was found that sexual dimorphism was not always the case, and significant differences concerned only stages F, G, and H for all four teeth. Differences in the mineralization rate between the upper and lower, left and right third molars were also evaluated (Table 7), and no significant differences were observed, except for females, between the upper third molars (p = 0.024).
A logistic regression analysis was also performed for age 16 years old, with teeth staging (from D to F) as predictor variables. Analysis was done dividing the sample according to gender. For females, a total of 260 cases were analyzed and for males, 205 cases were analyzed (Table 8). Stage D was found to be a useful marker for diagnosing age equal or superior to 16 years, both in males and females, with 98.4% and 96.3% of correct predictions, respectively.
Criteria validity was also assessed, evaluating this method’s specificity (the percentage of non-occurrences correctly predicted) and sensitivity (the percentage of occurrences correctly predicted) (Table 9). The results pointed out that excluding age 16 or over (true negatives) is a more secure prediction for every stage.
Discussion
Age estimation using dental development has been used for a long time since it is recognized that dental mineralization is an accurate measure of chronological age, not being particularly affected by other factors (as diseases, nutrition, among others); however, contradiction is reported on the usefulness of third molars for dental age estimation [8]. On one hand, there are various studies using distinct methodologies, for instance, Mesotten et al. [8] performed dental age estimation using a modification of the method of Gleiser and Hunt [9], wherein third molar development is assessed taking into consideration ten developmental stages. The same procedure was adopted by Gunst et al. [10] in a continuation and extension of the previous study.
According to De Salvia et al. [11], a method evaluation should be accurate, not invasive, reproducible and, if possible, easy exploitable. In this study, we chose to adopt the eighth-grade scheme of Demirjian et al. [7] because it obeys the characteristics; in addition, it does not require tooth measurements and is an easy, objective, and practical method requiring only experience in orthopantomogram interpretation. Besides, it is the preferred method by several authors [12–19], allowing us to compare our results with those from other studies. Olze et al. [6] also found the Demirjian method as the one more suitable for their investigation, claiming that other methods, such as the one used by Gleiser and Hunt [9] or the one described by Moorrees et al. [20] or yet, that applied by Kullman et al. [21], used many stages, making it harder to compare results and also use estimation values of the root future length, which results in a subjective approach to estimation. In another investigation, Olze et al. [22] referred to this method as the one revealing the highest inter- and intraindividual correspondence between evaluators and as the one with the highest correspondence between estimated age and chronological age as well.
On the other hand, third molars are frequently absent, adopt aberrant positions, and vary in size, structure, formation, and eruption times [23–25]. Nevertheless, after a certain age, (approximately 15 years of age) third molars are the only teeth developing and therefore, the only useful age indicator [26], but because, root mineralization can be completed under age 18, other alternative methods that do not consider tooth mineralization as a factor are being studied. For instances, Olze et al. [27] described the radiographic visibility of the root pulp in third molars as a potential age estimation criterion, concluding that it is possible, “beyond resonable doubt” state that a person is over 18 years old if a certain stage is attained. We chose to study the mineralization stages of third molars because in Portugal, the age with legal relevancy is 16 and not 18 years old.
The results of this investigation point to an almost linear relationship between age and third molar mineralization regardless of the individual sex. It also shows that complete mineralization occurs a little later in females. This is consistent, in general lines, with the relevant literature; however, not all data are consistent, and a clear tendency of earlier mineralization chronology is evident in our sample. Nevertheless, it must be taken into account that the mean age is influenced by the maximum age of the sample.
The present investigation showed no intra- or interobserver significant differences, and this finding is consistent with many other studies in the area [5, 15, 17–19, 28–30]. It was also found that there is a strong correlation between age and third molar development, both for males and females (p < 0.001, for both sexes). The correlation coefficients were 0.772 and 0.705 (tooth 18), 0.853 and 0.728 (tooth 28), 0.848 and 0.771 (tooth 38), and 0.843 and 0.759 (tooth 48), for girls and boys, respectively. Similar results were presented by other investigators [15, 17, 29].
Trends for an earlier third molar formation in males were apparent in all teeth and in all stages. These data agree with some and disagree with others, those from other investigations. For instance, in an Austrian sample of 610 individuals aged between 12 and 24 years old [5], a tendency for earlier third molar mineralization in females was apparent at earlier crown formation stages; the authors claim then an inversion and a faster root formation in male individuals, with boys reaching stage E 2 years earlier than girls. In this Portuguese sample, as stated before (stage E), these were also first reached by boys (1.3 to 1.8 years earlier). On the other hand, Lee et al. [17] stated that, as in this study, third molar formation happens earlier in males. The same resultes were stated by Rai et al. and Olze et al. [28, 31].
In this study, there were statistically significant differences for all third molar mineralization rate in males and females. Considering each stage separately, it was found that sexual dimorphism was not always the case, and significant differences concerned only stages F, G, and H, for all four teeth. These results partially agree with those from other studies; Meinl et al. [5] stated that significant sexual dimorphism was presented in stages E and F, Olze et al. [15] reported no significant differences between males and females, but no individual stage analysis was done. Prieto et al. [16] found that, as in our sample, there were no significant differences between genders, but when considering each stage isolated, significant sexual dimorphism was found in stages E, F, and G with males reaching maturity indicators earlier than females. Lee et al. [17] stated that significant sexual dimorphism as present in stages F and G. In a Chinese population, Bai et al. [18] also reported the presence of significant sexual dimorphism but on earlier and later stages (D, E, and H). These differences could be related with sample differences or with population-specific data.
No differences in the mineralization rate between the upper and lower, left and right third molars were observed, except for females, between the upper third molars. This difference was not observed in any of the investigations consulted [17, 19, 28].
Most authors chose to determine the likelihood that a subject is over 18 [11]; however, in Portugal, the age with legal relevancy is 16, therefore, 16 was the choosen age for this assessment. In our opinion, the diagnosis of being younger than 16 years old can be made with accuracy using stage D of the radiological development of the third molars. In fact, logistic regression pointed out that stage D can be used to predict age equal or superior to 16 with an accuracy of 96.3% for females and 98.4% for males. It should be stated that stage D is not the best stage to diagnose age over 16 since third molar mineralization increases with age. In this manner, stage E, F, G, and H are more suitable indicators. Stage D is, perhaps, the earliest indicator of age over 16 years; however, dental age estimation is one more complementary method of age estimation, and other indicators should be used in order to improve specificity and sensitivity and diminish the occurrence of technically and ethically unacceptable errors. These type of errors were described by Garamendi et al. [32] who refer to the errors derived from a forensic age estimation indicating that a subject who is actually over 18 (in our case, 16) is a minor (technically unacceptable errors) and to the errors indicating that minors are over 18. The first type of error leads to a more benevolent criminal treatment and the second one leads to a violation of minors’ rights. Taking this into account, additional age estimation methods should be used to reduce technically unacceptable to a minimum, and to erase ethically unacceptable.
Because in some few procedures, age 18 may be the age with legal relevancy (in determining illegal imigration, for instances), probability calculation of excluding age younger than 18 if stage H is attained was also calculated. As recommended by Knell et al. [33], mean values of age ate at stage H were not calculated, since they can lead to false conclusions.
Finally, we believe that, based on our results, and the differences between them and those of other populations, we do agree with Olze et al. [6] when they state that population-specific standards enhance the accuracy of forensic age estimation based on third molar mineralization in living subjects. Nevertheless, this remains to be proven, and some investigators do state that there is no indication at all that not using country-specific information influences the percentage of correctly identified subjects [30].
Conclusion
The present investigation provides important data on third molar mineralization in the Portuguese population. It can be concluded that stage D can be used to predict age equal or superior to 16 with an accuracy of 96.3% for females and 98.4% for males. It is also evident that different populations have different data; in this manner, these data may not be valid to other populations. The data described may provide a reference for forensic application; however, additional studies with a larger population sample should be conducted to meet provisions of more accurate data concerning the Portuguese population.
References
Schmeling A, Grundmann C, Fuhrmann A, Kaatsch H-J, Knell B, Ramsthaler F, Reisinger W, Riepert T, Ritz-Timme S, Rösing W, Rötzscher K, Geserick G (2008) Criteria for age estimation in living individuals. Int J Leg Med 122:457–460
Liversidge HM, Chaillet N, Mörnstad H, Nyström M, Rowlings K, Taylor J, Willems G (2006) Timing of Demirjian’s tooth formation stages. Ann Hum Biol 33(4):457–470
Olze A, Taniguchi M, Schmeling A, Zhu BL, Yamada Y, Maeda H, Geserick G (2003) Comparative study on the chronology of third molar mineralization in a Japanese and a German population. Leg Med Tokyo 5(Suppl 1):S256–S260
Olze A, Schmeling A, Taniguchi M, Maeda H, Van Niekerk P, Wernecke KD, Geserick G (2004) Forensic age estimation in living subjects: the ethnic factor in wisdom tooth mineralization. Int J Leg Med 118:170–173
Meinl A, Tangl S, Huber C, Maurer B, Watzek G (2007) The chronological of third molar mineralization in the Austrian population—a contribution to forensic age estimation. Forensic Sci Int 169:161–167
Olze A, Reisinger W, Geserick G, Schmeling A (2006) Age estimation of unaccompanied minors. Part II. Dental aspects. Forensic Sci Int 159:S65–S67
Demirjian A, Goldstein H, Tanner JM (1973) A new system of dental age assessment. Hum Biol 45(2):211–227
Mesotten K, Gunst K, Carbonez A, Willems G (2002) Dental age estimation and third molars: a preliminary study. Forensic Sci Int 129:110–115
Gleiser I, Hunt EE Jr (1955) The permanent first molar: its calcification, eruption and decay. Am J Phys Anthropol 13:253–284
Gunst K, Mesotten K, Carbonez A, Willems G (2003) Third molar root development in relation to chronological age: a large sample sized retrospective study. Forensic Sci Int 136:52–57
De Salvia A, Calzetta C, Orrico M, De Leo D (2004) Third molar radiological development as an indicator of chronological age in European population. Forensic Sci Int 146:S9–S12
Koshy S, Tandon S (1998) Dental age assessment: the applicability of Demirjian’s method in south Indian children. Forensic Sci Int 94(1–2):73–85
Tunc ES, Koyuturk AE (2008) Dental age assessment using Demirjian’s method on northern Turkish children. Forensic Sci Int 175(1):23–26
Maia MC, Martins Mda G, Germano FA, Brandão Neto J, da Silva CA (2010) Demirjian’s system for estimating the dental age of northeastern Brazilian children. Forensic Sci Int 200(1–3):177.e1–4
Orhan K, Ozer L, Orhan AI, Dogan S, Paksoy CS (2007) Radiographic evaluation of third molar development in relation to chronological age among Turkish children and youth. Forensic Sci Int 165:46–51
Prieto JL, Barbería E, Ortega R, Magaña C (2005) Evaluation of chronological age based on third molar development in the Spanish population. Int J Leg Med 119:349–354
Lee SH, Lee JY, Park HK, Kim YK (2009) Development of third molars in Korean juveniles and adolescents. Forensic Sci Int 188:107–111
Bai Y, Mao J, Zhu S, Wei W (2008) Third molar development in relation to chronologic age in young adults of central China. J Huazhong Univ Sci Technolog Med Sci 28(4):487–490
Zeng DL, Wu ZL, Cui MY (2010) Chronological age estimation of third molar mineralization of Han in southern China. Int J Leg Med 124:119–123
Moorrees CF, Fanning EA, Hunt EE Jr (1963) Age variation of formation stages for ten permanent teeth. J Dent Res 42:1490–1502
Kullman L, Johanson G, Akesson L (1992) Root development of the lower third molar and its relation to chronological age. Swed Dent 16:161–167
Olze A, Bilang D, Scmidt S, Wemecke KD, Geserick G, Schmeling A (2005) Validation of common classifications systems for assessing the mineralization of third molar. Int J Leg Med 19:22–26
Celikoglu M, Miloglu O, Kazanci F (2010) Frequency of agenesis, impaction, angulation, and related pathologic changes of third molar teeth in orthodontic patients. J Oral Maxillofac Surg 68(5):990–995
Levesque GY, Demirijian A, Tanguay R (1981) Sexual dimorphism in the development, emergence, and agenesis of the mandibular third molar. J Dent Res 60(10):1735–1741
Sánchez MJ, Vicente A, Bravo LA (2009) Third molar agenesis and craniofacial morphology. Angle Orthod 79(3):473–478
Woelfel JB (1997) Dental anatomy. Its relevance to dentistry. Williams and Wilkins, Baltimore
Olze A, Solheim T, Schulz R, Kupfer M, Schmeling A (2009) Evaluation of the radiographic visibility of the root pulp in the lower third molars for purpose of forensic age estimation in living individuals. Int J Leg Med 124:183–186
Rai B, Kaur J, Jafarzadeh H (2010) Dental age estimation from the developmental stage of the third molars in Iranian population. J Forensic Leg Med 17(6):309–311
Cruz-Landeira A, Linares-Argote J, Martínez-Rodríguez M, Rodríguez-Calvo MS, Otero XL, Concheiro L (2010) Dental age estimation in Spanish and Venezuelan children. Comparison of Demirjian and Chaillet’s scores. Int J Leg Med 124(2):105–112
Thevissen PW, Alqerban A, Asaumi J, Kahveci F, Kaur J, Kim YK, Pittayapat P, Van Vlierberghe M, Zhang Y, Fieuws S, Willems G (2010) Human dental age estimation using third molar developmental stages: accuracy of age predictions not using country-specific information. Forensic Sci Int 201(1–3):106–111
Olze A, Pynn BR, Kraul V, Schulz R, Heinecke A, Pfeiffer H, Schmeling A (2010) Studies on the chronology of third molar mineralization in First Nations people of in First Nations people of Canada. Int J Legal Med 124(5):433–437
Landa GPM, MI BJ, Solano MA (2005) Reliability of the methods applied to assess age minority in living subjects around 18 years old. A survey on a Moroccan origin population. Forensic Sci Int 154:3–12
Knell B, Ruhstaller P, Prieels F, Schmeling A (2009) Dental age diagnostics by means of radiographical evaluation of the growth stages of lower wisdom teeth. Int J Leg Med 123(6):465–469
Acknowledgments
The authors would like to thank to Dr. B. Knell for all the support given.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Caldas, I.M., Júlio, P., Simões, R.J. et al. Chronological age estimation based on third molar development in a Portuguese population. Int J Legal Med 125, 235–243 (2011). https://doi.org/10.1007/s00414-010-0531-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-010-0531-8