
Abstract
Introduction
Diaphragm excursion and contraction velocity measured using ultrasonography have been used to assess diaphragm function. We aimed to evaluate the performance of diaphragm ultrasonography during weaning from mechanical ventilation (MV).
Methods
Diaphragm ultrasonography was performed on 73 mechanically ventilated patients who were being considered for extubation on three separate occasions: (1) on assist control mode (A/C) during consistent patient triggered ventilation, (2) following 30 min during a spontaneous breathing trial (SBT), (3) 4–24 h following extubation. Right hemidiaphragm excursion and contraction velocity were measured on A/C, during SBT, and following extubation. These measurements were correlated with the outcome of extubation.
Results
Twenty patients failed extubation: 6 of whom required re-intubation and 14 of whom required non-invasive ventilatory support. During SBT, the mean diaphragm excursions were 1.7 ± 0.82 cm in the group who failed extubation compared to 2.1 ± 0.9 cm in the group who were successfully extubated (p = 0.06). To predict successful extubation, a decrease in diaphragm excursion of < 16.4% between A/C and SBT had a sensitivity of 84.9% and a specificity of 65%. The area under curve (AUC) for receiver operative characteristics for above cut-off was 0.75. Diaphragm contraction velocity performed poorly in predicting weaning outcome.
Conclusions
Diaphragm excursion measured during SBT is an imperfect predictor of the outcome of extubation. Maintenance of diaphragm excursion between A/C and SBT has good performance characteristics by AUC analysis. Diaphragm contraction velocity has poor ability to predict outcome of extubation.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Difficulty in weaning from mechanical ventilation (MV) is encountered in approximately 20–25% of patients [1]. Diaphragm dysfunction is well described in critically ill patients [2, 3].
Ultrasonography has been used to determine diaphragm thickening, excursion, and contraction velocity as a measure of its function [4]. Measurements of diaphragm thickening fraction using M-mode ultrasonography predict extubation outcome during spontaneous breathing trial (SBT) on T piece or pressure support ventilation (PSV) mode of MV [5, 6]. Diaphragm dysfunction as assessed by M-mode ultrasonography has been associated with longer total ventilation time, weaning time, and higher rates of weaning failures [7].
Serial assessment of diaphragm function during weaning from MV may be of value to predict successful extubation [8]. The aim of our study was to serially track diaphragm excursion and contraction velocity using ultrasonography, in order to correlate the change in ultrasonography measurements during the weaning process with the outcome of extubation.
Methods
This was a prospective observational study performed between June 2015 and February 2017 in the medical intensive care units (ICU) of North Shore University Hospital, Manhasset, New York and Long Island Jewish Medical Center, New Hyde Park, New York, both belonging to Northwell Health. The institutional review board of the Northwell Health approved the study (IRB protocol #15-049). Study subjects or their appropriate surrogates gave informed consent for participation in the study.
Inclusion Criteria
The ICU team decided about the readiness of a patient to be weaned from MV, the timing of the initiation of the SBT, and extubation based on their clinical assessment. If the ICU team decided to extubate a patient, the primary investigator (AP) was informed.
Exclusion Criteria
Exclusion criteria were age < 18 years, pregnancy, lack of informed consent, MV for < 24 h, unilateral or bilateral diaphragm paralysis, use of a paralytic agent during ICU stay, and do not re-intubate status post extubation.
Study Design
The investigator (AP) performed diaphragm ultrasonography at three separate times:
-
1.
During assist control (A/C) mode of MV while patients were consistently triggering the ventilator as they were being weaned off sedation prior to initiation of the SBT.
-
2.
After completing 30 min of the SBT on PSV with inspiratory pressure of 5 cm of water and positive end expiratory pressure of 5 cm of water. There were at least 30 min between the two measurements during A/C and PSV. At this time, the rapid shallow breathing index (RSBI) was calculated from the tidal volume delivered by the ventilator on PSV mode and respiratory rate as follows: [RSBI = respiratory rate/tidal volume (in liters)].
-
3.
Following discontinuation of MV. The ultrasonography was repeated between 4 and 24 h after extubation.
-
4.
The ICU team was blinded to the ultrasonography measurements. The decision to re-intubate or to use non-invasive ventilation (NIV) after extubation was left up to the discretion of ICU team.
Definition of Weaning Failure
Weaning failure was defined as the inability to maintain spontaneous breathing for at least 48 h, without any form of ventilatory support [9]. Patients who required re-intubation or NIV within 48 h of extubation were included in the ‘failure’ group.
Diaphragm Ultrasonography Measurements
Patients were studied in a semi-recumbent position between 20° and 40°. The right hemidiaphragm was examined using 2-dimensional and M-mode ultrasonography to record diaphragm excursion and contraction velocity during tidal breathing.
Measurement of Diaphragm Excursion
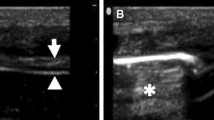
Diaphragm excursion was measured using a 3.5 MHz convex phase array probe (M turbo P21 probe, SonoSite, Bothell, WA) as previously described (Fig. 1) [10]. With liver serving as an acoustic window, the probe was placed immediately below the right costal margin in the mid-clavicular line in longitudinal scanning plane with the tomographic plane angled in the cephalad direction such that the ultrasound beam was perpendicular to the posterior third of the right hemidiaphragm (Fig. 2) [10]. When the diaphragm was identified with 2-dimensional imaging, the M-mode interrogation line was adjusted to be perpendicular to the movement of the posterior one-third of the right hemidiaphragm. The diaphragm excursion was measured on the vertical axis of the M-mode tracing (cm) from the beginning to end of tidal inspiration from the leading edge of the right hemidiaphragm.

Diaphragm excursion and inspiratory time represented by yellow and red double arrows, respectively

Measurement of diaphragm excursion and inspiratory time using ultrasonography. The ultrasound probe is angulated cephalad to be perpendicular to the posterior third of right hemidiaphragm. The dotted line represents M-mode interrogation line
Measurement of Diaphragm Contraction Velocity
From the M-mode tracing, diaphragm contraction velocity was calculated from the excursion and inspiratory time (Fig. 1) as follows:
The investigator performed diaphragm ultrasonography measurements when there was a pattern of consistent tidal breathing pattern in order to exclude variability related to tidal volume. Three measurements each of diaphragm excursion and contraction velocity were performed during tidal breathing and their mean was calculated. The duration of ultrasonography examination was < 5 min.
Statistical Analysis
Mann–Whitney U Test was used to compare continuous variables while Chi-square tests or Fisher’s exact tests were used to compare categorical variables. Percent change of diaphragm excursion and contraction velocity between A/C, SBT, and extubation were calculated separately as
A separate logistic regression model predicting “success” of extubation was performed for each of the above measures. A receiver operating characteristic (ROC) area under curve (AUC) was constructed to look at the model’s ability to predict “success.” The level of significance was fixed at p < 0.05. All analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC).
Results
During the study period, we included 73 patients; 53 patients were successfully extubated (i.e., no re-intubation or NIV for 48 h after extubation). The rate of failure of extubation was 27%. Six of 20 patients in the group that failed extubation were re-intubated without use of NIV within 48 h of extubation. The remaining 14 patients in the ‘failure’ group were initiated on NIV within 48 h of extubation either pre-emptively or as rescue therapy. Seven of these 14 patients were placed on NIV support immediately following extubation; the remaining 7 patients were initiated on NIV after the development of respiratory distress following extubation. Three of 14 patients that required NIV were re-intubated within 48 h following extubation. The remaining 11 patients were weaned from NIV without the need for re-intubation. Patient demographics and disease characteristics are summarized in Table 1. When compared to the group that was successfully extubated, the RSBI was significantly higher in the group that failed extubation.
Diaphragm excursion and contraction velocity on A/C mode, during SBT, and following extubation are compared between the two patient groups in Table 2. Diaphragm contraction velocity did not differ significantly between the two patient groups during A/C, SBT, and following extubation. Diaphragm excursion did not differ between the two patient groups on A/C. Patients in the group that failed extubation had significantly lower diaphragm excursion following extubation compared to the group that was successfully extubated (p = 0.02). The difference in diaphragm excursion between the two groups approached statistical significance during SBT (p = 0.06). During SBT, 6 of 20 patients who failed extubation and 4 of 53 patients in the group that were successfully extubated had a diaphragm excursion of < 1 cm. Diaphragm excursion of < 1 cm during SBT had a sensitivity of 30% and specificity of 92.5% for predicting extubation failure (AUC 0.64).
The mean percent change in diaphragm excursion between A/C to SBT in the group who failed extubation was − 12.6% while that in the group successfully extubated was 18.9%. When measured between A/C and SBT, a decrease in diaphragm excursion of < 16.4% had a sensitivity of 84.9% and a specificity of 65% for predicting successful extubation. (AUC = 0.75) (Fig. 1). When measured between A/C and following extubation between the two patient groups, a decrease in diaphragm excursion of < 5.9% predicted successful extubation with a sensitivity of 76.9% and a specificity of 71.4% (AUC = 0.74) (Fig. 2). The changes in diaphragm contraction velocity for the remaining time-points showed poor sensitivity and specificity for predicting successful extubation (Table 3).
Discussion
The results of this study demonstrate that during weaning from MV support, diaphragm excursion is a better predictor of extubation outcome than diaphragm contraction velocity. Both during SBT and following extubation, patients who failed extubation had lower diaphragm excursion when compared to the patients who were successfully extubated. Diaphragm excursion < 1 cm during SBT is highly specific to predict failure, but not sensitive. A decrease in diaphragm excursion between A/C and SBT < 16.4% is sensitive but not highly specific to predict success weaning. Changes in diaphragm excursion measured serially between A/C and SBT performed better than an arbitrary cut-off for diaphragm excursion alone during SBT to predict the outcome of extubation.
Several factors may contribute to extubation failure including alteration in airway resistance, respiratory system compliance, load-related cardiac dysfunction, respiratory muscle weakness, or failure of airway clearance. The RSBI may have limited ability to predict extubation outcome [11,12,13]. In our study, RSBI was significantly higher in the patient group that failed extubation compared to the group who was successfully extubated. However, in both groups the mean values for RSBI were < 105, emphasizing the limitation of this parameter.
Diaphragm dysfunction is associated with difficult weaning from MV [14]. Jiang et al. used the mean value of inspiratory excursions of the spleen and liver during SBT as a surrogate measurement of diaphragm excursion identifying a cut-off value of 1.1 cm having a sensitivity and specificity of 84 and 83%, respectively, to predict the success of extubation [15]. Kim et al. reported that diaphragm excursion of < 10 mm during SBT identified a higher rate of extubation failure than excursion greater than or equal to 10 mm [7]. Osman and Hashim found a cut-off value for diaphragm excursion of < 10 mm during SBT-predicted extubation failure with a 83.3% sensitivity, 100% specificity, 94.3% negative predictive value, 100% positive predictive value, and AUC of 0.83 [16]. Saeed et al. studied 30 patients with chronic obstructive pulmonary disease on MV and reported that cut-off value for diaphragm excursion of 1.1 cm during SBT had a sensitivity of 86.4%, specificity of 87.5%, and accuracy of 89.5% to predict extubation outcome [17]. Farghaly and Hasan found the cut-off value of ≥ 10.5 mm for diaphragm excursion during quiet tidal breathing at the time of SBT for successful extubation with a sensitivity of 87.5% and a specificity of 71.5% [18].
In our study, although the mean diaphragm excursion was greater in the patient group who were successfully extubated than those who failed extubation, there was an overlap in diaphragm excursion between the two groups during SBT. Fourteen of 20 patients in the group who failed extubation had diaphragm excursion of 1 cm or greater; this emphasizes the limitation of using an arbitrary cut-off value of diaphragm excursion to predict outcome of extubation.
Our results indicate that maintenance of diaphragm excursion during serial measurement between A/C and SBT may have utility in predicting the outcome of extubation when compared to the measurement of diaphragm excursion alone during SBT. We speculate on this unanticipated finding. When the patient is transitioned between A/C and SBT, the mechanical load on the diaphragm increases. If the ventilatory function of the patient is able to overcome the increased mechanical load during SBT with preserved contraction and excursion of the diaphragm, the patient is more likely to achieve successful extubation. Conversely, a significant reduction of diaphragm excursion following the withdrawal of positive pressure support may suggest an inadequate response of the ventilatory apparatus to augmented mechanical load and may portend a failed weaning attempt. As compared to measurements made on A/C, when the magnitude of diaphragm excursion continues to decline following extubation, it is likely that the patient would require re-intubation or NIV support. Conceptually, the maintenance of diaphragm excursion following withdrawal of ventilatory support indicates that the contractile function of the diaphragm is able to replace the mechanical work of the ventilator.
The utility of diaphragm contraction velocity using ultrasonography for predicting extubation outcomes has not been studied. In our study, we did not find significant difference in the diaphragm contraction velocity during SBT or following extubation between the two patients groups with respect to the outcome of extubation.
There are limitations to our study. One investigator performed all the ultrasonography measurements. There was no measurement of inter- or intra-observer variability. Boussuges et al. reported that the measurement of diaphragm excursion using M-mode ultrasonography is easy to perform and has high correlation coefficients between and within observers [10]. Measurements were made on the right hemidiaphragm alone. Left hemidiaphragm is often poorly visualized. Other investigators [6, 19] suggest measurement of left hemidiaphragm excursion may not be necessary, unless there is unilateral phrenic nerve injury. The overall extubation failure rate in our study was relatively high (27%), as patients who needed rescue NIV were included in the ‘failure’ group. The ICU team decided about initiation of NIV after extubation based on their clinical assessment. In the group that failed extubation, seven patients were initiated on NIV after development of respiratory distress and seven patients were pre-emptively initiated on NIV immediately following extubation, The overall rate of re-intubation within 48 h following extubation (12.5%) was comparable to what has been previously reported [1].
Conclusions
Diaphragm excursion measured during SBT has some utility to predict the outcome of extubation. Maintenance of diaphragm excursion between A/C and SBT is a better predictor of extubation outcome than is excursion measured alone during SBT, although both are imperfect predictors of extubation outcome. Diaphragm contraction velocity does not have prognostic value for extubation outcome. The finding that diaphragm excursion is an imperfect predictor reflects the complexity of factors that determine outcome of extubation. It is not likely that a single parameter will be sufficient for this purpose.
References
Esteban A, Alia I, Ibanez J, Benito S, Tobin MJ, Spanish Lung Failure Collaborative Group (1994) Modes of mechanical ventilation and weaning: a national survey of Spanish hospitals. Chest 106(4):1188–1193
Grosu HB, Im Lee Y, Lee J, Eden E, Eikermann M, Rose KM (2012) Diaphragm muscle thinning in patients who are mechanically ventilated. Chest 142(6):1455–1460
Jaber S, Petrof BJ, Jung B et al (2011) Rapidly progressive diaphragmatic weakness and injury during mechanical ventilation in humans. Am J Respir Crit Care Med 183:364–371
Matamis D, Soilemezi E, Tsagourias M et al (2013) Sonographic evaluation of the diaphragm in critically ill patients. Technique and clinical applications. Intensive Care Med 39(5):801–810
Ferrari G, De Filippi G, Elia F, Panero F, Volpicelli G, Aprà F (2014) Diaphragm ultrasound as a new index of discontinuation from mechanical ventilation. Crit ultrasound J 6(1):8
DiNino E, Gartman EJ, Sethi JM, McCool FD (2013) Diaphragm ultrasound as a predictor of successful extubation from mechanical ventilation. Thorax thoraxjnl-2013
Kim WY, Suh HJ, Hong SB, Koh Y, Lim CM (2011) Diaphragm dysfunction assessed by ultrasonography: influence on weaning from mechanical ventilation. Crit Care Med 39(12):2627–2630
Palkar A, Darabaner R, Singh K et al (2016) Serial lung and diaphragm ultrasonography to predict successful discontinuation of mechanical ventilation [abstract]. Chest 150(4_S):465A
Boles JM, Bion J, Connors A et al (2007) Weaning from mechanical ventilation. Eur Respir J 29(5):1033–1056
Boussuges A, Gole Y, Blanc P (2009) Diaphragmatic motion studied by m-mode ultrasonography: methods, reproducibility, and normal values. Chest 135(2):391–400
Epstein SK (1995) Etiology of extubation failure and the predictive value of the rapid shallow breathing index. Am J Respir Crit Care Med 152(2):545–549
Lee KH, Hui KP, Chan TB, Tan WC, Lim TK (1994) Rapid shallow breathing (frequency-tidal volume ratio) did not predict extubation outcome. Chest 105(2):540–543
Krieger BP, Isber J, Breitenbucher A, Throop G, Ershowsky P (1997) Serial measurements of the rapid-shallow-breathing index as a predictor of weaning outcome in elderly medical patients. Chest 112(4):1029–1034
Ambrosino N, Makhabah DN (2013) Comprehensive physiotherapy management in ARDS. Minerva Anestesiol 79(5):554–563
Jiang JR, Tsai TH, Jerng JS, Yu CJ, Wu HD, Yang PC (2004) Ultrasonographic evaluation of liver/spleen movements and extubation outcome. Chest 126(1):179–185
Osman AM, Hashim RM (2017) Diaphragmatic and lung ultrasound application as new predictive indices for the weaning process in ICU patients. Egypt J Radiol Nucl Med 48(1):61–66
Saeed AM, El Assal GI, Ali TM, Hendawy MM (2016) Role of ultrasound in assessment of diaphragmatic function in chronic obstructive pulmonary disease patients during weaning from mechanical ventilation. Egypt J Bronchol 10(2):167
Farghaly S, Hasan AA (2017) Diaphragm ultrasound as a new method to predict extubation outcome in mechanically ventilated patients. Aust Crit Care 30(1):37–43
Goligher EC, Laghi F, Detsky ME et al (2015) Measuring diaphragm thickness with ultrasound in mechanically ventilated patients: feasibility, reproducibility and validity. Intensive Care Med 41(4):642–649
Author information
Authors and Affiliations
Contributions
AP had full access to study data and takes full responsibility for the integrity of the work as a whole, from inception to published article. AP and KS contributed to study design, institutional review board application, data collection, analysis, study design, institutional review board application, data analysis, manuscript composition, and editing. PM, SK, EG, MN, KS, and AS contributed to manuscript composition and editing. MA and RD contributed to data analysis.
Corresponding author
Ethics declarations
Conflict of interest
The authors have reported that no potential conflicts of interest exist with any companies/organizations whose products or services may be discussed in this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The institutional review board of the Northwell Health approved the study (IRB protocol #15-049).
Informed Consent
Informed consent was obtained from all individual participants or their appropriate surrogates for their inclusion in the study.
Rights and permissions
About this article

Cite this article
Palkar, A., Mayo, P., Singh, K. et al. Serial Diaphragm Ultrasonography to Predict Successful Discontinuation of Mechanical Ventilation. Lung 196, 363–368 (2018). https://doi.org/10.1007/s00408-018-0106-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00408-018-0106-x