
Abstract
Introduction
To investigate the association of individual and contextual exposures with lung function by gender in rural-dwelling Canadians.
Methods
A cross-sectional mail survey obtained completed questionnaires on exposures from 8263 individuals; a sub-sample of 1609 individuals (762 men, 847 women) additionally participated in clinical lung function testing. The three dependent variables were forced expired volume in one second (FEV1), forced vital capacity (FVC), and FEV1/FVC ratio. Independent variables included smoking, waist circumference, body mass index, indoor household exposures (secondhand smoke, dampness, mold, musty odor), occupational exposures (grain dust, pesticides, livestock, farm residence), and socioeconomic status. The primary analysis was multiple linear regression, conducted separately for each outcome. The potential modifying influence of gender was tested in multivariable models using product terms between gender and each independent variable.
Results
High-risk waist circumference was related to reduced FVC and FEV1 for both genders, but the effect was more pronounced in men. Greater pack-years smoking was associated with lower lung function values. Exposure to household smoke was related to reduced FEV1, and exposure to livestock, with increased FEV1. Lower income adequacy was associated with reduced FVC and FEV1.
Conclusion
High-risk waist circumference was more strongly associated with reduced lung function in men than women. Longitudinal research combined with rigorous exposure assessment is needed to clarify how sex and gender interact to impact lung function in rural populations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Lung function is an established predictor of respiratory and non-respiratory morbidity and mortality [1, 2]. Lung function in adulthood may be compromised by numerous individual and contextual factors across the life span, including low birth weight [3], smoking [4], secondhand smoke exposure [5], central adiposity [6], and lower socioeconomic status (SES) [7]. Occupational exposures to grain dust [8, 9] and cotton dust [10], most often occurring in rural environments, are also associated with reduced lung function.
Lung function is also influenced by sex (biological attributes) and gender (social and economic attributes) [11, 12]. Regarding gender, societal sanctions concerning appropriate behavior for women and men determine, in part, how and where one’s time is spent. For example, segregation in the labor force results in the differential exposure of women and men to occupational risk factors [13]. In Canada in 2011, 72.5 % of registered farm operators were men [14]; farmers are exposed routinely to a variety of dusts, chemicals, gases, and fumes which increase their risk for acquiring respiratory health problems [15]. Conversely, although male-dominated, women’s involvement in farm work, and thus exposure, has been marginalized in research with farming populations [16, 17]. Regarding the influence of sex, given the same exposure, women and men may be differentially vulnerable as a result of sex-linked biological differences. For example, some research suggests women’s lung function may be more adversely affected by smoking than men’s [18], which may be due, in part, to sex differences in airway size [11].
Much of the research on determinants of lung function in rural settings has focused on men employed in male-dominated industries; few studies have examined lung function in general populations of rural-dwellers and in relation to gender.Footnote 1 To address these gaps, the present study uses baseline data from a recent cohort study examining the determinants of respiratory health of farming and non-farming communities in Saskatchewan Canada [20]. One research question guided this investigation: do associations between individual/contextual exposures and lung function vary by gender among rural-dwelling Canadians?
Methods
Participants
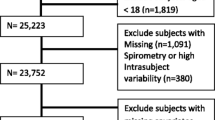
The data source for this study was the Saskatchewan Rural Health Study (SRHS), a prospective cohort study being conducted in two phases, baseline and follow-up. The detailed methodology for the study has been published previously [20]. In brief, purposeful samples of 48 of the 297 rural municipalities and 16 of the 145 towns in southern Saskatchewan were selected to participate in the baseline study. A sample of 9 RMs was randomly generated from four geographical areas: southeast, southwest, northeast, northwest. The local councils for 32 of the 36 RMs and 15 of the 16 towns agreed to participate on behalf of their residents and supplied mailing addresses. Dillman’s method was used to recruit study participants aged 18 and older [21]. In total, 8261 individuals from 4624 households in the selected RMs and towns participated in the baseline survey. Information on primary respiratory health outcomes and contextual and individual factors was collected through self-administered mailed questionnaires. The final question on the questionnaire was: “Would you be willing to be contacted about having breathing and/or allergy tests at a nearby location?” Those who responded “Yes” to this question were invited to participate in the clinical assessment component that is reported here. Of the 3209 respondents who expressed a willingness to participate in the clinical assessment, pulmonary function testing was conducted on 762 men and 847 women.
Measures
Dependent Variables
Mobile clinics were set up in participating towns, and research nurses trained in spirometry and allergy assessment telephoned each household of consenting participants to arrange a time and a place (usually no greater than 60 km from their residence) for clinical assessment. The protocol used to obtain pulmonary function measurements is described elsewhere [20]. Lung function measures of interest in this investigation were (1) forced expired volume in one second (FEV1), (2) forced vital capacity (FVC), and (3) FEV1/FVC ratio. Of the 1609 participants that underwent lung function testing, 738 men and 827 women met American Thoracic Society spirometry testing standards [22].
Independent Variables
Individual factors of primary interest were body mass index (BMI), waist circumference, and personal smoking. BMI was calculated by dividing respondents’ measured weight in kg by height in m2 to form three groupings: normal (<25 kg/m2), overweight (25–30 kg/m2), and obese (>30 kg/m2). Measured waist circumference was categorized as low risk or high risk based on sex-specific cut-off points (men ≥102 cm = high risk; women ≥88 cm = high risk) established by Health Canada [23]. Pack-years was calculated to quantify cigarette smoking exposure, based on self-reported duration and amount of cigarette consumption and grouped into the following categories: never smoker <0–10, >10–25, and >25 years.
Contextual factors included those related to the household environment, occupation, and socioeconomic circumstances. Three indoor household exposures were assessed. Dampness was measured with the question: “During the past 12 months, has there been water or dampness in your home from broken pipes, leaks, heavy rain, or floods?” (yes/no). Mold was assessed with the question: “Does your home (including basement) frequently have a mildew odor or musty smell?” (yes/no). Household smoking (yes/no) was measured with the question: “Do any of the people who live in your house use any of the following tobacco products in the home?” with options: “cigarettes,” “cigars,” or “pipes.” Occupational exposures were assessed with the question: “Have you ever been exposed to any of the following in the work place…” (yes/no): grain dust, livestock, insecticides, herbicides, fungicides; responses to the latter three exposures were collapsed to create a pesticide exposure (yes/no) variable. Location of residence (farm/non-farm) was based on answers to the question “Where is your home located?” with the options of “farm,” “in town,” or “acreage”; town and acreage responses were combined to create a non-farm category. Farm/non-farm residence was considered an occupation-related exposure in this study in recognition of the fact that the farming workplace often overlaps with family residence in rural Saskatchewan. SES was measured by household income adequacy (low, middle, high), a derived variable based on total household income and the number of people living in the household [24].
Statistical Analysis
Thirteen households had two participants each; to avoid accounting for within-subject household clustering at the analysis stage, we randomly excluded 13 individuals (five men and eight women) from the analysis. This exclusion, which resulted in a sample size of 819 women and 733 men, allowed for the use of classical linear regression techniques to examine associations between exposure variables and lung function measures. Following descriptive analyses, multiple linear regression analyses were conducted separately for each lung function measure. In the first step, individual exposures were entered as a group, followed by contextual exposures in step 2. In step 3, two-way interactions between gender and exposure variables were assessed. Final multivariable models included statistically significant variables (p ≤ 0.05), adjusted for age and height. For statistically significant interaction terms, predicted probabilities based on the final multiple regression models were depicted graphically. Statistical analysis was completed using IBM SPSS version 20 [IBM Corp., NY, USA].
Results
The frequency distribution of study variables, by gender, is given in Table 1. A higher percentage of men than women were in the older age categories, with no differences observed for marital status. A greater proportion of men than women smoked and were in the overweight/obese BMI categories, although no difference was observed for waist circumference. Regarding contextual factors, no gender differences emerged for indoor household exposures. A higher proportion of men than women reported occupational exposure to grain dust, livestock, pesticides, and living on a farm. Women and men reported similar levels of income adequacy.
The age- and height-adjusted ANOVA results of lung function measures by individual and contextual variables, analyzed separately for women and men, are shown in Table 2. For both women and men, pack-years smoking was inversely related to FEV1 and FEV1/FVC. Greater BMI was associated with lower FVC in both genders and lower FEV1 in men. High-risk waist circumferences was related to lower lung function for all participants with the exception of FEV1/FVC in men. Exposure to household smoke was related to lower FEV1 and FEV1/FVC for both genders. In women only, home dampness was associated with reduced FEV1/FVC. The presence of a mildew/musty odor was related to increased FEV1 in women, reduced FEV1 in men, and reduced FEV1/FVC in women. Exposure to grain dust was associated with reduced FEV1/FVC ratio in men. Farm/non-farm home location was unrelated to lung function. Lower income adequacy was associated with lower FVC and FEV1 in both women and men.
Results of the final multivariable models by lung function measure are presented in Table 3. Greater pack-years smoking was associated with reduced lung function. The relationship between waist circumference and FVC and FEV1 was modified by gender; although high-risk waist circumference was related to reduced lung function for both genders, the effect was more pronounced in men than women (Figs. 1, 2). Exposure to household smoke was associated with reduced FEV1, and exposure to livestock, with increased FEV1. Lower income adequacy was related to reduced FVC and FEV1.

Mean predicted values of FVC stratified by waist circumference and gender

Mean predicted values of FEV1 stratified by waist circumference and gender
Discussion
This study examined the association of individual and contextual factors with lung function by gender in a general population of rural-dwelling Canadians. Our results showed a stronger detrimental effect of high-risk waist circumference on lung function in men than women. Greater pack-years smoking, exposure to household smoke, lower income adequacy, and grain dust exposure were associated with reduced lung function. Exposure to livestock was associated with increased lung function.
In this study, high-risk waist circumference was related to reduced lung function, whereas BMI showed no significant association. Research has shown that obesity, particularly abdominal adiposity, may result in restricted breathing, potentially causing reductions in FEV1 and FVC [6, 25]. Waist circumference, compared to overall weight or BMI, may be a more reliable indicator of abdominal obesity [26]. The results of several studies also suggest that the relationship between central adiposity and lung function may be more pronounced in men [25, 27, 28], possibly due to sex-linked differences in the distribution of body fat [11]. Consistent with these findings, although greater waist circumference was associated with reduced FEV1 and FVC for both women and men in our study, the effects were stronger in men.
Smoking is a well-established risk factor for impaired lung function [4, 29]. Some [18, 30] but not all [31, 32] studies suggest that smoking may be more detrimental to lung function in women than men. Women’s smaller airway size has been postulated as one potential explanation, though sex differences in hormones, immunology, and genetics have also been hypothesized [11]. The results of this study however, indicated a similar, negative association of smoking with lung function in both women and men.
We found that exposure to household smoke was also associated with reduced lung function. Secondhand smoke comprises many of the same hazardous agents that are inhaled by smokers themselves. Although household secondhand smoke has been associated with reduced FEV1 in several studies, findings have not always been consistent and when present, effect sizes have been small [5, 33]. Although some very limited evidence suggests that passive smoke exposure may be more strongly related to impaired lung function in women [34], we found no evidence of a gender effect.
No association between indicators of mold/musty odor and lung function emerged in our multivariable analysis. A systematic review of respiratory health effects of dampness concluded that although such exposures appear to be associated with an increased risk of respiratory symptoms and asthma, the evidence regarding reduced lung function was inconclusive [35]. Only a limited amount of research has examined gender differences in the health effects of mold/dampness; that being said, however, the results of several studies have shown, in contrast to our results, stronger associations between indicators of damp housing and reduced lung function [36, 37] and respiratory symptoms [38] in women than men. Longitudinal designs combined with enhanced exposure measurement are needed to clarify such relationships in future research.
Occupational exposure to grain dust was associated with reduced FEV1 and FEV1/FVC ratio in this study. Consistent with our findings, a number of cross-sectional and longitudinal studies have shown associations between exposure to grain dust and reduced lung function [8, 9, 39, 40]. The vast majority of these studies were restricted to male samples; the many challenges to studying the effects of sex and gender in occupational health research have been well articulated in the literature, particularly in highly sex-segregated occupations [41–43]. However, the findings of several recent meta-analyses suggest that the effect of organic dust (including grain dust) on impaired lung function [44] and development of chronic respiratory symptoms [45] may be more pronounced in men than women. Recent longitudinal research with cotton workers in China have reported greater FEV1 impairment in male than female exposed workers [46] and among those retired from the cotton industry, more limited lung function recovery [47]. Although sex-linked differences in response to endotoxin exposure have been proposed as one possibility to explain these findings, uncontrolled differences in exposure between women and men occupying the same job cannot be ruled out as an alternative explanation, nor can the possibility of residual confounding due to smoking [48]. In our study, although the gender/grain dust interaction was not statistically significant, the higher prevalence of grain dust exposure in men than women may indicate exposed men as the main driver of the observed associations.
An unexpected result in this study, and in contrast to previous research [49–51], was the positive association between exposure to livestock and lung function. Some research suggests that exposure to farm animals early in life may be associated with reduced asthma risk [52, 53] and increased lung function in adulthood [54]. We examined whether the relationship between livestock exposure and lung function was modified by having had lived on a farm during the first year of life, but the interaction was not statistically significant (data not shown). Alternatively, it is possible that participants who developed respiratory impairment due to livestock exposure migrated from the study area at an earlier time. Some evidence suggests that current livestock farmers, particularly those involved in pig production, have reduced lung function compared to those who leave the industry [55]. The lack of detail in our exposure measure, along with the cross-sectional design, prevents a more nuanced exploration of the reasons that might explain this positive association.
Consistent with previous research [7], lower SES was associated with reduced FEV1 and FVC in this rural sample. Associations remained even after adjusting for several factors hypothesized as contributing to SES inequities in lung function, such as smoking and exposure to household smoke [7, 56]. Other potentially mediating factors not assessed in this study include diet, physical inactivity, low birth weight, and childhood SES [57–59].
Study Strengths and Limitations
This investigation has several strengths, including the use of objective measures of lung function, conducted using a standardized protocol. Our relatively large sample size allowed us to examine a broad array of individual and contextual factors potentially associated with lung function and to test for potential interactions with gender. Gender has not often been positioned as a variable of importance in research examining determinants of lung function, particularly in rural settings.
However, limitations in measurement and study design are also present, serving to temper firm conclusions regarding associations between individual/contextual exposures and lung function, both within and between women and men. Most of the exposure variables were based on self-report, increasing the likelihood of misclassification. Previous research suggests moderate correlations between self-report and more objective measures of exposures such as smoking [60], secondhand smoke [61], and household dampness/mold [62], with estimates of the validity of self-reported occupational exposures more variable [63]. The underestimation of exposures independently of respiratory health status would likely result in an attenuation of study effects. The potential for non-differential misclassification was further exacerbated by the lack of detail in our exposure assessment, particularly information on frequency, intensity, and duration. We also lacked information on exposures likely of more relevance to the lung health of women, such as the use of household cleaning products, as well as potentially hazardous agents more often encountered in women-dominated occupations, such as clerical work and health care [64].
The cross-sectional design limits our ability to infer causal relationships between exposures and lung function. The study participants in this investigation were a volunteer sub-sample of a larger study sample. When compared to the overall sample, our clinic participants were younger, more highly educated, and more likely to be a non-smoker and to live on a farm. Although selection bias is a possibility, the focus of our study on estimating exposure-outcome associations, rather than on estimating prevalence, may mitigate this concern [65]. Just over 97 % of the sample indicated being of Caucasian origin thus preventing us from examining ethnicity as a potential correlate of lung function in this rural sample.
Conclusion
High-risk waist circumference was more strongly associated with reduced lung function in men than women. Longitudinal research combined with rigorous exposure assessment is needed to clarify how sex and gender interact to impact lung function in rural populations and in turn inform the development of programs and policies aimed at protecting lung health.
Notes
For brevity sake, we use the term gender throughout the rest of the paper; however, we recognize that the effects of sex and gender on human health are complexly interwoven throughout the life course [19].
References
Kannel W, Hubert H, Lew E (1983) Vital capacity as a predictor of cardiovascular disease: the framingham study. Am Heart J 105:311–315
Mannino D, Buist A, Petty T et al (2003) Lung function and mortality in the United States: data from the first national health and nutrition examination survey follow-up study. Thorax 58(5):388–393
Canoy D, Pekkanen J, Elliott P et al (2007) Early growth and adult respiratory function in men and women followed from the fetal period to adulthood. Thorax 62(5):396–402
Mirabelli MC, Preisser JS, Loehr LR et al (2016) Lung function decline over 25 years of follow-up among black and white adults in the ARIC study cohort. Respir Med 113:57–64
Eisner MD, Wang Y, Haight TJ et al (2007) Secondhand smoke exposure, pulmonary function, and cardiovascular mortality. Ann Epidemiol 17(5):364–373
Canoy D, Luben R, Welch A et al (2004) Abdominal obesity and respiratory function in men and women in the EPIC-norfolk study, United Kingdom. Am J Epidemiol 159(12):1140–1149
Hegewald MJ, Crapo RO (2007) Socioeconomic status and lung function. Chest 132:1608–1614
Pahwa P, Senthilselvan A, McDuffie HH et al (2003) Longitudinal decline in lung function measurements among Saskatchewan grain workers. Can Respir J 10:135–141
Huy T, De Schipper K, Chan-Yeung M, Kennedy SM (1991) Grain dust and lung function. Dose–response relationships. Am Rev Respir Dis 144:1314–1321
Wang XR, Zhang HX, Sun BX et al (2005) A 20-year follow-up study on chronic respiratory effects of exposure to cotton dust. Eur Respir J 26(5):881–886
Becklake M, Kauffmann F (1999) Gender differences in airway behaviour over the human life span. Thorax 54(12):1119–1138
Krieger N (2003) Genders, sexes, and health: what are the connections–and why does it matter? Int J Epidemiol 32(4):652–657
Eng A, Mannetje AT, McLean D et al (2011) Gender differences in occupational exposure patterns. Occup Environ Med 68(12):888–894
Statistics Canada (2011) Census of Agriculture. Highlights and analysis. Statistics Canada, Ottawa
Schenker MB, Christiani D, Cormier Y et al (1998) American thoracic society: respiratory health hazards in agriculture. Am J Respir Crit Care Med 158:S1–S76
Habib RR, Hojeij S, Elzein K (2014) Gender in occupational health research of farmworkers: a systematic review. Am J Ind Med 57(12):1344–1367
McDuffie HH, Pahwa P, Dosman JA (1992) Respiratory health status for 3098 Canadian grain workers studied longitudinally. Am J Ind Med 20:753–762
Gan WQ, Man SP, Postma DS et al (2006) Female smokers beyond the perimenopausal period are at increased risk of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Respir Res 7(1):52
Springer KW, Stellman JM, Jordan-Young RM (2012) Beyond a catalogue of differences: a theoretical frame and good practice guidelines for researching gender in human health. Soc Sci Med 74(11):1817–1824
Pahwa P, Karunanayake CP, Hagel L et al (2012) The Saskatchewan rural health study: an application of a population health framework to understand respiratory health outcomes. BMC Res Notes 5:400
Dillman DA (2000) Mail and internet surveys: the tailored design method, 2nd edn. Wiley, New York
Statement of the American Thoracic Society (1987) Standardization of spirometry: 1987 update. Am Rev Resp Dis 136:1285–1298
Canada Health (2003) Canadian guidelines for body weight classification in adults. Office of Nutrition Policy and Promotion, Ottawa
Statistics Canada (2008) National population health survey household component: documentation for the derived variables and the constant longitudinal variables. Statistics Canada, Ottawa
Chen Y, Rennie D, Cormier YF, Dosman J (2007) Waist circumference is associated with pulmonary function in normal-weight, overweight, and obese subjects. Am J Clin Nutr 85:35–39
Ochs-Balcom HM, Grant BJB, Muti P et al (2006) Pulmonary function and abdominal adiposity in the general population. Chest 129:853–862
Harik-Khan RI, Wise RA, Fleg JL (2001) The effect of gender on the relationship between body fat distribution and lung function. J Clin Epidemiol 54:399–406
Steele R, Finucane F, Griffin S et al (2008) Obesity is associated with altered lung function independently of physical activity and fitness. Obesity 17:578–584
James AL, Palmer LJ, Kicic E et al (2005) Decline in lung function in the Busselton Health Study: the effects of asthma and cigarette smoking. Am J Respir Crit Care Med 171(2):109–114
Chen Y, Horne SL, Dosman JA (1991) Increased susceptibility to lung dysfunction in female smokers. Am Rev Respir Dis 143:1224–1230
Kohansal R, Martinez-Camblor P, Agusti A et al (2009) The natural history of chronic airflow obstruction revisited: an analysis of the Framingham Offspring cohort. Am J Respir Crit Care Med 180:3–10
Xu X, Dockery DW, Ware JH et al (1992) Effects of cigarette smoking on rate of loss of pulmonary function in adults: a longitudinal assessment. Am Rev Respir Dis 146:1345–1348
Jaakkola MS, Jaakkola JJ (2002) Effects of environmental tobacco smoke on the respiratory health of adults. Scand J Work Environ Health 28(2):52–70
Eisner MD (2002) Environmental tobacco smoke exposure and pulmonary function among adults in NHANES III: impact on the general population and adults with current asthma. Environ Health Perspect 110(8):765–770
Mendell MJ, Mirer AG, Cheung K et al (2011) Respiratory and allergic health effects of dampness, mold, and dampness-related agents: a review of the epidemiologic evidence. Environ Health Perspect 119:748–756
Hernberg S, Sripaiboonkij P, Quansah R et al (2014) Indoor molds and lung function in healthy adults. Respir Med 108:677–684
Norback D, Zock JP, Plana E et al (2013) Lung function decline in relation to mould and dampness in the home: the longitudinal European community respiratory health survey ECRHS II. Thorax 66:396–401
Rennie D, Chen Y, Lawson J et al (2005) Different effect of damp housing on respiratory health in women. J Am Med Women Assoc 60:46–51
Melenka LS, Hessel PA, Yoshida K et al (1999) Lung health in Alberta farmers. Int J Tuberc Lung Dis 3:913–919
McDuffie HH, Pahwa P, Dosman JA (1992) Respiratory health status for 3098 Canadian grain workers studied longitudinally. Am J Ind Med 20:753–762
Kennedy S, Loehoorn M (2003) Exposure assessment in epidemiology: does gender matter? Am J Ind Med 44:576–583
Messing K, Punnett L, Bond M et al (2003) Be the fairest of them all: challenges and recommendations for the treatment of gender in occupational health research. Am J Ind Med 43:618–629
Quinn MM (2011) Why do women and men have different occupational exposures? Occup Environ Med 68(12):861–862
Dimich-Ward H, Beking K, DyBuncio A et al (2012) Occupational exposure influences on gender differences in respiratory health. Lung 190(2):147–154
Schachter EN, Zuskin E, Moshier EL et al (2009) Gender and respiratory findings in workers occupationally exposed to organic aerosols: a meta-analysis of 12 cross-sectional studies. Environ Health 8(1):1–33
Lai PS, Hang JQ, Zhang FY et al (2013) Gender differences in the effect of occupational endotoxin exposure on impaired lung function and death: the shanghai textile worker study. Occup Environ Med 19:152–157
Lai PS, Hang JQ, Valeri L et al (2015) Endotoxin and gender modify lung function recovery after occupational organic dust exposure: a 30-year study. Occup Environ Med 72:546–552
Heederik D, Smit LA (2014) Gender differences in lung function recovery after cessation of occupational endotoxin exposure: a complex story. Occup Environ Med 72:543–544
Kirychuk SP, Senthilselvan A, Dosman JA et al (2003) Respiratory symptoms and lung function in poultry confinement workers in Western Canada. Can Respir J 10(7):375–380
Radon K, Weber C, Iversen M et al (2001) Exposure assessment and lung function in pig and poultry farmers. Occup Environ Med 58:405–410
Senthilselvan A, Dosman JA, Kirychuk P et al (1997) Accelerated lung function decline in swine confinement workers. Chest 111:1733–1741
Leynaert B, Neukirch C, Jarvis D et al (2001) Does living on a farm during childhood protect against asthma, allergic rhinitis, and atopy in adulthood? Am J Respir Crit Care Med 164(10):1829–1834
Lampi J, Canoy D, Jarvis D et al (2011) Farming environment and prevalence of atopy at age 31: prospective birth cohort study in Finland. Clin Exp Allergy 41(7):987–993
Lampi J, Koskela H, Hartikainen AL et al (2015) Farm environment during infancy and lung function at the age of 31: a prospective birth cohort study in Finland. BMJ Open 5(7):e007350
Chenard L, Senthiselvan A, Grover V et al (2007) Lung function and farm size predict healthy worker effect in swine farmers. Chest 131:245–254
Gray LA, Leyland AH, Benzeval M, Watt GC (2013) Explaining the social patterning of lung function in adulthood at different ages: the roles of childhood precursors, health behaviours and environmental factors. J Epidemiol Community Health 67(11):905–911
McFadden E, Luben R, Wareham N et al (2009) How far can we explain the social class differential in respiratory function? A cross-sectional population study of 21,991 men and women from EPIC-Norfolk. Eur J Epidemiol 24(4):193–201
Bartley M, Kelly Y, Sacker A (2012) Early life financial adversity and respiratory function in midlife: a prospective birth cohort study. Am J Epidemiol 175(1):33–42
Tennant PW, Gibson GJ, Pearce MS (2008) Lifecourse predictors of adult respiratory function: results from the Newcastle thousand families study. Thorax 63(9):823–830
Wong SL, Shields M, Leatherdale S et al (2012) Assessment of validity of self-reported smoking status. Health Rep 23(1):47
Avila-Tang E, Elf JL, Cummings KM et al (2012) Assessing secondhand smoke exposure with reported measures. Tob Control 22:156–163
Jaakkola MS, Jaakkola JJ (2004) Indoor molds and asthma in adults. Adv Appl Microbiol 55:309–338
Teschke K, Olshan AF, Daniels JL et al (2002) Occupational exposure assessment in case-control studies: opportunities for improvement. Occup Environ Med 59(9):575–594
Camp PG, Dimich-Ward H, Kennedy SM (2004) Women and occupational lung disease: sex differences and gender influences on research and disease outcomes. Clin Chest Med 25(2):269–279
Rothman KJ, Gallacher JE, Hatch EE (2013) Why representativeness should be avoided. Int J Epidemiol 42(4):1012–1014
Acknowledgments
The Saskatchewan Rural Health Study Team consists of James Dosman, MD (Designated Principal Investigator, University of Saskatchewan, Saskatoon, SK Canada); Dr. Punam Pahwa, PhD (Co-principal Investigator, University of Saskatchewan, Saskatoon SK Canada); Dr. John Gordon, PhD (Co-principal Investigator, University of Saskatchewan, Saskatoon SK Canada); Yue Chen, PhD (University of Ottawa, Ottawa Canada); Roland Dyck, MD (University of Saskatchewan, Saskatoon SK Canada); Louise Hagel (Project Manager, University of Saskatchewan Saskatoon SK Canada); Bonnie Janzen, PhD (University of Saskatchewan, Saskatoon SK Canada); Chandima Karunanayake, PhD (University of Saskatchewan, Saskatoon SK Canada); Shelley Kirychuk, PhD (University of Saskatchewan, Saskatoon SK Canada); Niels Koehncke, MD (University of Saskatchewan, Saskatoon SK Canada); Joshua Lawson, PhD, (University of Saskatchewan, Saskatoon SK Canada); William Pickett, PhD (Queen’s University, Kingston ON Canada); Roger Pitbaldo, PhD (Professor Emeritus, Laurentian University, Sudbury ON Canada); Donna Rennie, RN, PhD, (University of Saskatchewan, Saskatoon SK Canada); and Ambikaipakan Senthilselvan, PhD (University of Alberta, Edmonton, AB, Canada). We are grateful for the contributions of the rural municipality administrators and the community leaders of the towns included in the study that facilitated access to the study populations and to all of participants who donated their time to complete and return the survey.
Funding
Canadian Institutes of Health Research MOP-187209-POP-CCAA-11829.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflicts of Interest
None.
Additional information
The Saskatchewan Rural Health Study Team are listed in “Acknowledgments.”
Rights and permissions
About this article

Cite this article
Janzen, B., Karunanayake, C., Rennie, D. et al. Gender Differences in the Association of Individual and Contextual Exposures with Lung Function in a Rural Canadian Population. Lung 195, 43–52 (2017). https://doi.org/10.1007/s00408-016-9950-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00408-016-9950-8