
Abstract
Global Initiative on Chronic Obstructive Lung Disease (GOLD) guidelines recently removed stage 0, a group with symptoms but without airways obstruction, from their severity staging. However, in practice this group may still be diagnosed and medically managed. The aim of this study was to characterize healthcare utilization patterns of chronic obstructive pulmonary disease (COPD) patients by disease severity, focusing on the possible unique attributes of patients who would have been classified as GOLD stage 0. This is a prospective cohort pilot study performed at the Hines Veterans Administration Hospital. One hundred twenty patients with a diagnosis of COPD were enrolled. The participants completed quality-of-life questionnaires and a pulmonary function test. Healthcare utilization data were obtained 1 year prior and 2 years after the enrollment date. Three disease severity groups were defined based on GOLD criteria for comparison [GOLD stage 1–2 (GS 1–2), GOLD stage 3–4 (GS 3–4), and formerly GOLD stage 0 (“at risk”)]. The “at risk” group had an average of 14.4 (SD = 30.5) outpatient visits/year and 0.3 (SD = 0.8) hospitalizations/year, which were higher than the other groups, but this was not statistically significant. Respiratory medications were used by 6 (26%), 30 (59%), and 40 (91%) patients from “at risk” to GS 3–4, respectively. Patients in the “at risk” group had a decrement in health status, significant utilization of healthcare services, and were often receiving medications not consistent with guidelines.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Chronic obstructive pulmonary disease (COPD) is a common chronic disease affecting more than 24 million adults in the United States [1]. The Veterans Administration (VA) plays an important part in the care of patients with COPD in the United States as there are nearly 500,000 patients with a COPD diagnosis receiving care in a given year in the VA.
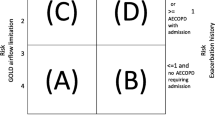
The updated Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines designate four stages of severity based on spirometry values [2]. Unlike the previous classification, this current version does not include stage 0 defined as the “at risk” population with symptoms, exposure to risk factors, and normal spirometry. Previous studies have shown that the diagnosis of COPD is often made without spirometric evidence with only a third of those with a new diagnosis of COPD having spirometry performed [3, 4]. Based on the National Health and Nutrition Examination Survey III (NHANES III) results, only 17.4 percent of adults with a self-reported diagnosis of COPD had 1987 American Thoracic Society-defined low lung function consistent with chronic obstruction [5, 6]. Even without a label within the GOLD staging of COPD, this former stage 0 group, in practice, may represent a considerable number of adults being diagnosed with COPD and managed with pharmacologic therapy.
There is limited information about this population with respect to their health status, healthcare utilization, and progression of disease. One of the studies to focus on this group showed that progression of COPD disease severity from GOLD stage 0 to stage II did not correspond to meaningful differences in health status although a worsening of health status was noted [7]. Whether the presence of chronic cough and sputum without airway obstruction (formerly GOLD stage 0) really identifies individuals at risk to develop future bronchial obstruction is still debatable [8–11]. However, studies have found that this population may have an increased mortality risk compared with asymptomatic smokers with normal lung function [12–15]. To ultimately understand the outcomes associated with the COPD disease severity groups, including the previously defined GOLD stage 0 group, an important step is to better understand the similarities and differences by group with respect to health status and healthcare utilization. We conducted a pilot study at a single institution to characterize health status and healthcare utilization patterns of COPD patients seeking care in the VA by disease severity, focusing on the possible unique attributes of patients who would have been classified as GOLD stage 0 due to presence of symptoms in the absence of airway obstruction.
Methods
This was an observational pilot study approved by the Human Studies Subcommittee of the Hines VA Hospital.
Study Sample
We identified patients who had made an inpatient or outpatient visit and who had a diagnosis of COPD [International Classification of Diseases, ninth revision (ICD-9) 491.x, 492.x, 496.x] during a 12-month period from a Hines VA facility (hospital or outpatient clinics). Eligible patients identified were contacted by letter inviting them to participate; up to two letters were mailed to each individual. Each letter contained a copy of the consent form, the Health Insurance Portability and Accountability Act form, and a one-page description detailing the protocol for the study and contact numbers for study personnel. Mailings were sent until 120 patients were enrolled in the study and informed consent was obtained. The first participant enrolled on May 12, 2003, and the last patient enrolled on September 1, 2004. A total of 1338 unique patients were contacted by letters to recruit 120 patients. Participants were required to attend a single study visit to the Hines Pulmonary Function Lab. Participants completed the St. George’s Respiratory Questionnaire followed by a pulmonary function test (PFT) and a 6-minute walk test (6MWT). All participants also completed a smoking history questionnaire, including a self report of current status as a current smoker, ex-smoker, or having never smoked. All spirometries were performed in the Hines VA Hospital Pulmonary Function Lab using a Morgan Scientific PFT system according to ATS standards. Each patient underwent a minimum of three maneuvers and if not reproducible additional maneuvers were performed.
St. George’s Respiratory Questionnaire (SGRQ)
The SGRQ is a disease-specific measure of quality of life and well being in patients with obstructive lung disease [16]. The instrument has been shown to be a valid and reliable measure of COPD-related quality of life [16–19]. The questionnaire provides an overall score as well as scores for symptoms, activity, and impact domains. The results from the instrument are measured from 0% (no impairment) to 100% (maximum impairment). A difference in scores of 4% has been shown to be a minimally important difference [16].
Healthcare Utilization
Healthcare utilization, including inpatient visits, outpatient visits, and outpatient respiratory medication utilization was obtained from VA encounter data for 12 months before and 24 months after each patient’s study visit. All-cause and COPD-related inpatient and outpatient encounters were analyzed for each group. COPD-related visits were defined as an outpatient or inpatient visit with any diagnosis for COPD. For medication utilization, each patient had to have more than one prescription for each drug category in a single year to be considered a regular user of that medication for that year. The aggregate of all medications for each disease category was obtained as a surrogate for healthcare consumption in relation to disease severity.
Severity of COPD
Three disease severity groups were defined based on GOLD criteria: formerly GOLD stage 0 (“at risk”) includes diagnosis of COPD without airway obstruction, GOLD stage 1–2 (GS 1–2) includes GOLD stages I and II (mild-moderate), and GOLD stage 3–4 (GS 3–4) includes GOLD stages III and IV (severe-very severe). The previous classification of GOLD stage 0 required chronic symptoms (cough, sputum production) and normal spirometry. The prebronchodilator values were used.
Statistical Analysis
Characteristics of the patients were summarized using counts and percentages to describe categorical variables and means and standard deviations to describe continuous variables. Comparisons of the means between the severity groups were made with an analysis of variance (ANOVA) model. Covariates that had a significant relationship to severity means or that changed the point estimates more than 10% were included in the adjusted model. Based on this criterion, the model was adjusted for age and smoking status and performed using the analysis of covariance (ANCOVA) model. Post hoc differences between groups were assessed by the Scheffè test [20]. For variables lacking normal distribution and/or homogeneous variance and could not be transformed, the Kruskal-Wallis test was used. Comparisons of means were performed if each group had a sample size greater than six, otherwise only percentages and means were used. A p value less than 0.05 was considered statistically significant.
Results
We recruited 120 patients for participation in the study; four patients were ultimately excluded due to inadequate spirometry based on ATS criteria. Approximately 94% of the patients were white and 98% were male. A total of 23 (19.8%) of the participants were classified as “at risk,” 49 (42.2%) as GS 1–2, and 44 (37.9%) as GS 3–4. Comparison of means for the subject characteristics and other laboratory values are shown in Table 1. The average body mass index (BMI) was significantly different between “at risk” and GS 3–4 only (ANOVA p = 0.033), with the “at risk” group having the highest BMI [31.2 (SD = 5.4) kg/cm2] and the GS 3–4 group having the lowest BMI [27.7 (SD = 5.5) kg/cm2]. The 6MWT was statistically different between GS 1–2 and GS 3–4. In the “at risk” group, the prevalence of diabetes mellitus was 26.1%, hypertension was 56.5%, and heart disease was 39.1%. The prevalence of these comorbid conditions was similar in the other groups.
The SGRQ scores by disease severity are seen in Table 2. After adjusting for age and smoking status, the SGRQ total scores were lowest for the “at risk” group and highest for the GS 3–4 group. Most of the differences in scores between groups reached statistical significance. The exceptions were the total, activity, and impact scores, which were not different between the “at risk” group and GS 1–2, and the symptom domain, which showed a difference only between the “at risk” group and GS 3–4 [41.9 (SD = 22.7) vs. 57.9 (SD = 23.9)].
Healthcare visits are summarized in Table 3. The “at risk” group had the highest proportion and most all-cause inpatient visits with 30.4% of the group, averaging 1.89 (SD = 1.36) visits per patient-year. The “at risk” group also had the most all-cause outpatient visits, averaging 14.40 (SD = 30.79) visits per patient-year, while GS 1–2 and GS 3–4 had 10.50 (SD = 13.53) and 10.73 (SD = 14.24) visits per patient-year, respectively. This was not statistically significant.
Medication utilization for each severity group is summarized in Table 4. The proportions in each group receiving medications were 26.1, 59.2, and 90.9% in the “at risk” group, GS 1-2, and GS 3–4, respectively. The means days supplied for the proportion of each group receiving medications were follows: “at risk” was 205.6 (SD = 120.6), GS 1–2 was 331.8 (SD = 240.7), and GS 3–4 was 501.8 (SD = 328.1) days supplied per patient-year. For individual drug categories, the largest proportions of users for all groups were noted for inhaled anticholinergics, followed by inhaled short-acting β-agonists.
Discussion
Approximately one fifth of our cohort with an existing diagnosis of COPD had no bronchial obstruction noted on spirometry. As expected, GS 3–4 had the most COPD-related outpatient visits per patient-year and the largest proportion utilizing COPD-related inpatient care. However, the “at risk” group had the most all-cause inpatient and outpatient visits per patient per year, although not statistically significant. Also as expected, the proportion of patients in each group utilizing medications increased with increasing disease severity. About 25% of the “at risk” patients received respiratory medications on a regular basis, while more than 40% in GS 1–2 did not receive any respiratory medications, suggesting a pattern of care not consistent with GOLD guidelines. Because the “at risk” group has no comparison group in the American Thoracic Society and European Respiratory Society, no prior recommendations for treatment exist for this group.
Consistent with previous findings, in this VA population sample, categorizing patients based on the GOLD staging system resulted in differences in health status in the SGRQ between mild-moderate disease (GS 1–2) and severe-very severe disease stages (GS 3–4) [7, 21]. Our findings also indicate that the “at risk” patients have health status deterioration similar to patients with mild-moderate disease [7]. This deterioration in health status may be attributable to symptoms and/or other coexisting illnesses, as indicated by the healthcare utilization patterns. Our study did not find differences in the proportion of each group having common comorbidities; however, we are limited by the relatively small sample included in this study. Interestingly, the average BMI of the “at risk” group is classifiable as obese according to Center for Disease Control criteria. Perhaps, the higher prevalence of obesity in the “at risk” group is a factor in these patients being diagnosed as having COPD. They may have symptoms consistent with mild COPD, such as increased dyspnea, while they do not meet criteria for diagnosis of COPD based on lung function testing. Whether these patients truly represent early COPD and optimal treatment are questions that need to be addressed.
Our study is unique in characterizing the healthcare utilization patterns of patients with chronic symptoms and no airway obstruction, formerly referred to as the GOLD stage 0 group. Based on the NHANES III results, 82.6% with self-reported obstructive lung disease did not have obstruction according to ATS guidelines [5, 6]. Therefore, many in this group would have been classified as stage 0 based on GOLD guidelines. We found that a significant proportion of these patients are being treated with bronchodilators in the absence of bronchial obstruction. In addition, the fact that these patients are using more healthcare services than the other groups may be an indicator that they are, on average, a sicker group of patients. It is unclear whether treatment in this setting offers any benefits in symptom reduction but there is clearly an added economic burden to the overall costs associated with COPD.
Our study has some limitations. First, the patients were enrolled by sending out letters, therefore, there could be self-selection bias. This bias may have produced a healthier cohort willing to make an extra visit to participate without compensation. However, the final cohort expressed a good distribution of disease severities with no differences in mean age. Second, as expected with a VA population, the cohort was predominantly men, and thus we were unable to assess any gender differences. Third, lack of statistical significance between the early-disease severity stages does not always correlate with clinical significance. Although the SGRQ symptom score from “at risk” to GS 1–2 and from GS 1–2 to GS 3–4 was more than 4%, considered a minimally important difference, there was no statistically significant difference in our study; however, this may not be so in a larger sample. Also, the overall proportions of patients for medication utilization were too small to obtain valid statistical significance. Fourth, we did not have pharmacy data outside of the VA system. However, the majority of our cohort would have been Medicare eligible and at the time of the study there were no Medicare pharmaceutical benefits. Because the “at risk” group is younger, we would expect they would be the group to more likely have supplemental insurance and pharmacy benefits. In that case, our findings would underestimate the percentage of patients in this group receiving medications. Finally, we cannot rule out misclassification due to reversible reactive airways disease. However, our study emphasizes current practice patterns and classification designated by providers and thus is a reflection of healthcare utilization regardless of misclassification.
In this single-center pilot study, patients with a diagnosis of COPD without airway obstruction, formerly referred to as the GOLD stage 0 “at risk” group, had a decrement in health status, significant utilization of healthcare services not always associated with a diagnosis of COPD, and were likely to be receiving regular medications not consistent with guidelines. Although controversy exists as to whether this group is “at risk” for COPD, in clinical practice a proportion of them are being managed as if they have obstruction. It is unclear whether this group benefits from the observed treatment pattern. In the future, larger studies of this formerly “at risk” group may help to identify the optimal management of these patients to improve and/or better understand outcomes, in particular quality of life, disease progression, and mortality.
References
Morbidity & Mortality (2007) Chart book on cardiovascular, lung, and blood diseases. National Institutes of Health, National Heart, Lung, and Blood Institute, Bethesda, MD
Global Inititiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease (updated 2006). http://www.goldcopd.org/Guidelineitem.asp?l1=2&l2=1&intId=989. Accessed 1 December 2007
Han MK, Kim MG, Mardon R, Renner P, Sullivan S, Diette GB, Martinez FJ (2007) Spirometry utilization for COPD: how do we measure up? Chest 132:403–409
Lee TA, Bartle B, Weiss KB (2006) Spirometry use in clinical practice following diagnosis of COPD. Chest 129:1509–1515
Agency for Healthcare Research and Quality (2005) Use of spirometry for case finding, diagnosis and management of chronic obstructive pulmonary disease (COPD). www.ohrq.gov/downloads/pud/evidence/pdf/spirocopd/spiro.pdf. Accessed 1 December 2007
Mannino DM, Gagnon RC, Petty TL, Lydick E (2000) Obstructive lung disease and low lung function in adults in the United States: data from the National Health and Nutrition Examination Survey, 1988–1994. Arch Intern Med 160:1683–1689
Antonelli-Incalzi R, Imperiale C, Bellia V, Catalano F, Scichilone N, Pistelli R, Rengo F (2003) Do GOLD stages of COPD severity really correspond to differences in health status? Eur Respir J 22:444–449
Enright PL, Crapo RO (2000) Controversies in the use of spirometry for early recognition and diagnosis of chronic obstructive pulmonary disease in cigarette smokers. Clin Chest Med 21:645–652
Lindberg A, Eriksson B, Larsson LG, Ronmark E, Sandstrom T, Lundback B (2006) Seven-year cumulative incidence of COPD in an age-stratified general population sample. Chest 129:879–885
Lindberg A, Jonsson AC, Ronmark E, Lundgren R, Larsson LG, Lundback B (2005) Ten-year cumulative incidence of COPD and risk factors for incident disease in a symptomatic cohort. Chest 127:1544–1552
Vestbo J, Lange P (2002) Can GOLD Stage 0 provide information of prognostic value in chronic obstructive pulmonary disease? Am J Respir Crit Care Med 166:329–332
Ekberg-Aronsson M, Pehrsson K, Nilsson JA, Nilsson PM, Lofdahl CG (2005) Mortality in GOLD stages of COPD and its dependence on symptoms of chronic bronchitis. Respir Res 6:98
Ferrer M, Alonso J, Morera J, Marrades RM, Khalaf A, Aguar MC, Plaza V, Prieto L, Anto JM (1997) Chronic obstructive pulmonary disease stage and health-related quality of life. The Quality of Life of Chronic Obstructive Pulmonary Disease Study Group. Ann Intern Med 127:1072–1079
Mannino DM, Doherty DE, Sonia Buist A (2006) Global Initiative on Obstructive Lung Disease (GOLD) classification of lung disease and mortality: findings from the Atherosclerosis Risk in Communities (ARIC) study. Respir Med 100:115–122
Stavem K, Sandvik L, Erikssen J (2006) Can global initiative for Chronic Obstructive Lung Disease stage 0 provide prognostic information on long-term mortality in men? Chest 130:318–325
Jones PW, Quirk FH, Baveystock CM (1991) The St George’s Respiratory Questionnaire. Respir Med 85 Suppl B:25–31; discussion 33–27
Barr JT, Schumacher GE, Freeman S, LeMoine M, Bakst AW, Jones PW (2000) American translation, modification, and validation of the St. George’s Respiratory Questionnaire. Clin Ther 22:1121–1145
Jones PW, Quirk FH, Baveystock CM, Littlejohns P (1992) A self-complete measure of health status for chronic airflow limitation. The St. George’s Respiratory Questionnaire. Am Rev Respir Dis 145:1321–1327
Rutten-van Molken M, Roos B, Van Noord JA (1999) An empirical comparison of the St. George’s Respiratory Questionnaire (SGRQ) and the Chronic Respiratory Disease Questionnaire (CRQ) in a clinical trial setting. Thorax 54:995–1003
Kleinbaum DG, Kupper LL, Muller KE, Nizam A (1988) Applied Regression Analysis and Other Multivariate Methods. Brooks/Cole Publishing Company, Pacific Grove, CA, pp 451–457
Stahl E, Lindberg A, Jansson SA, Ronmark E, Svensson K, Andersson F, Lofdahl CG, Lundback B (2005) Health-related quality of life is related to COPD disease severity. Health Qual Life Outcomes 3:56
Acknowledgments
This study was partly funded by an unrestricted research grant from Boehringer-Ingelheim Pharmaceuticals. This material was also based upon work supported by the HSR&D Service, Center for Management of Complex Chronic Care COE, Hines VA Hospital. The funding agency had no role in the design, conduct, or interpretation of the study results. Kevin Weiss was the Director for the Management of Complex Chronic Care, Hines VA Hospital, Hines, IL, and the Institute for Healthcare Studies at Northwestern University Feinberg School of Medicine, Chicago, IL, when this work was performed. This work was performed while all authors were employees of the Hines Veterans Administration Hospital. As U.S. government employees, this article was made in that capacity, thus assignment applies only to the extent allowable by U.S. law.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Joo, M.J., Lee, T.A., Bartle, B. et al. Patterns of Healthcare Utilization by COPD Severity: A Pilot Study. Lung 186, 307–312 (2008). https://doi.org/10.1007/s00408-008-9095-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00408-008-9095-5