
Abstract
Epilepsy is a major risk factor for autism spectrum disorder (ASD) and complicates clinical manifestations and management of ASD significantly. Tuberous sclerosis complex (TSC), caused by TSC1 or TSC2 mutations, is one of the medical conditions most commonly associated with ASD and has become an important model to examine molecular pathways associated with ASD. Previous research showed reversal of autism-like social deficits in Tsc1 +/− and Tsc2 +/− mouse models by mammalian target of rapamycin (mTOR) inhibitors. However, at least 70 % of individuals with TSC also have epilepsy, known to complicate the severity and treatment responsiveness of the behavioural phenotype. No previous study has examined the impact of seizures on neurocognitive reversal by mTOR inhibitors. Adult Tsc2 +/− (Eker)-rats express social deficits similar to Tsc2 +/− mice, with additive social deficits from developmental status epilepticus (DSE). DSE was induced by intraperitoneal injection with kainic acid at post-natal days P7 and P14 (n = 12). The experimental group that modelled TSC pathology carried the Tsc2 +/− (Eker)-mutation and was challenged with DSE. The wild-type controls had not received DSE (n = 10). Four-month-old animals were analysed for social behaviour (T1), then treated three times during 1 week with 1 mg/kg everolimus and finally retested in the post-treatment behavioural analysis (T2). In the experimental group, both social interaction and social cognition were impaired at T1. After treatment at T2, behaviour in the experimental group was indistinguishable from controls. The mTOR inhibitor, everolimus, reversed social deficit behaviours in the Tsc2 haploinsufficiency plus DSE animal model to control levels.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder seen in about 1 % of the general population and is now recognized as a global public health concern [1]. At least 25 % of people with ASD have epilepsy, associated with more motor difficulties, developmental delay, a range of problem behaviours and significant treatment challenges [2]. However, there is a very limited understanding of the fundamental links between ASD and seizures and a dearth of pre-clinical or clinical intervention studies of ASD in the context of epilepsy.
The monogenetic disorder tuberous sclerosis complex (TSC) has high rates of ASD, intellectual disability and epilepsy. TSC is caused by mutations in either TSC1 or TSC2 and leads to dysregulation of the TSC1–TSC2-intracellular protein complex, causing overactivation of the mTOR signalling pathway [3]. Mouse models of TSC have been shown to have cognitive deficits that were reversed on mTOR inhibitors [4]; similarly Tsc1 +/− and Tsc2 +/− mice have been shown to have ASD-like social behaviour deficits that were also reversed on mTOR inhibitors [5, 6]. Epilepsy is seen in at least 70 % of individuals with TSC and is treatment resistant in up to 60 % of cases. Individuals with TSC plus epilepsy have a significantly greater neurological and neuropsychiatric morbidity [3]. In spite of the clinical overlap between epilepsy and ASD in TSC, there have so far been no fundamental investigations to explore whether social deficit behaviours seen in the context of TSC and seizures would be amenable to mTOR inhibitor treatment.
Infantile spasms are a severe form of epilepsy and start in early childhood. They are seen as a risk factor for intellectual disability, especially in TSC [7–10]. In TSC, infantile spasms typically start during the first year of life. With regard to brain development, the time span around P7 to P14 in rats is comparable with the first year of life in humans [11]. Developmental status epilepticus (DSE) induced by kainic acid between P1 and P14 in rats was associated with life-long impairment in spatial memory. These rats also exhibited impaired induction of hippocampal long-term potentiation [12, 13]. P7 in rats represents a period of high vulnerability to various stimuli like NMDA receptor antagonists leading to massive neuronal death in the brain and protracted behavioural abnormalities, including social deficits [14, 15]. These findings suggest that the first year of life in humans and the time span around P7 to P14 in rats are especially vulnerable phases in the development of the nervous system and disturbance may lead to later neuropsychiatric manifestations.
In adult rats with Tsc2 haploinsufficiency, we previously reported deficient social interaction that we interpreted as a correlate of the clinical manifestation in TSC patients with ASD. This social deficit in adult rats was accelerated by the previous experience of DSE induced during early childhood in these Tsc2 +/− (Eker)-rats [16–18]. Given that patients with ASD in TSC often have a history of previous developmental epilepsy, the P7 and P14 DSE scenario in Tsc2 +/− (Eker)-rats suggests an animal model of impaired social behaviour, closer to the situation of TSC patients than those caused by a Tsc1 or Tsc2 mutation alone. Here, we aimed to study whether an mTOR inhibitor, everolimus, would exert beneficial effects on social interaction and cognition also in the combination of Tsc2 haploinsufficiency and DSE. With regard to our model, not the presence of epileptic activity during the time of testing social behaviour was important, but the previous experience of DSE during childhood.
Previous studies have evaluated the effect of mTOR inhibitors on pituitary and renal tumours in Tsc2 +/− (Eker)-rats [19, 20]. In male Wistar rats, a single intravenous injection of 1 mg/kg everolimus resulted in stable levels in the brain over at least 24 h [21]. To induce stable levels of everolimus in the brain of Tsc2 +/− (Eker)-rats plus DSE, we chose to inject 1 mg/kg everolimus intraperitoneally for three times in 1 week.
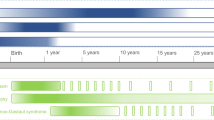
The experimental group that modelled TSC pathology carried the Tsc2 +/− (Eker)-mutation and was challenged with pharmacologically induced status epilepticus at post-natal days P7 and P14 (n = 12). The control group consisted of wild-type (Tsc2 +/+) carriers from the Eker rat line and did not receive DSE (n = 10). In TSC patients, ASD is a phenomenon persisting into adulthood and can be tested in children as well as in adults. We performed behavioural testing at young adult age (4 months) in the rat model because there is much less experience with testing at younger ages. All animals were initially investigated in the pre-treatment behavioural analysis (T1). They were then treated for 1 week with 1 mg/kg everolimus per bodyweight by intraperitoneal (i.p.) injection. Finally, they were retested in the post-treatment behavioural analysis (T2) (Fig. 1).

Experimental design. The upper panel shows the two experimental groups. The time scale is the lifespan of the animals. Group 1 is wild-type offspring from the Tsc2 +/− (Eker)-rat line which are free of DSE. Group 2 is haploinsufficient Tsc2 +/− offspring from the Tsc2 +/− (Eker)-rat line. At post-natal days P7 and P14, during brain development of the rats, status epilepticus was induced in group 2 by kainic acid injection. Animals from both groups were analysed at the age of 4 months. The dashed lines indicate how the lower panel is related to the upper panel. The lower panel shows the temporal relation of the pre-treatment (T1) and post-treatment behavioural (T2) analyses, injections with 1 mg/kg everolimus and assessments of body weight. The time scale starts at day 1 (d1) with habituation of the animals to the apparatuses and ends at day 32 (d32) with the last assessment of body weight
Materials and methods
Animals
The Eker rat strain carries the Tsc2 +/− (Eker)-mutation on Long–Evans background and was originally obtained from MD Anderson Cancer Center, University of Texas [22]. The mutation is haploinsufficient; homozygous mutants are non-viable. Rats were group-housed under a 12-h/12-h day–night cycle with lab chow and water available ad libitum. All breeding for this study was started at the same day, using as parents littermates from the Eker rat line. All animals used in this study were offspring from these crossings. For the Tsc2 +/− (Eker) plus developmental status epilepticus group, Tsc2 +/− from the pool of parental littermates were crossed. For the wild-type control group, wild-type animals from the pool of parental littermates were crossed. It was technically only possible to use the second generation from littermates, because the offspring received kainic acid injections at P7 and P14, whereas separation of the offspring from their mothers and subsequent genotyping was not possible before P21. Only male rats were used for experiments. Tsc2 +/− (Eker) and Tsc2 +/+ wild-type genotypes were determined by PCR [22]. Injection volumes did not exceed 10 µl/g body weight. All testing took place during the day phase. All experiments were conducted in accordance with the European Union guidelines on the care and use of laboratory animals and were approved by the local animal care committee (Regierungspräsidium Karlsruhe, file reference 35-9185.81/G-86/12).
Developmental status epilepticus
Kainic acid (KA) monohydrate (Sigma, Deisenhofen, Germany) was dissolved in phosphate-buffered saline. At P7, male offspring from the litters planned for the Tsc2 +/− (Eker) plus developmental status epilepticus group received an intraperitoneal injection with 3 mg/kg KA, and at P14, a second injection with 4 mg/kg KA [13]. The animals were returned to the home cage with their mother. About 15 min after injection, a crescendo-like status epilepticus started in all injected animals and lasted for several hours. Late-onset seizures were observed neither during animal care nor behavioural analysis.
Schedule of behavioural analyses and pharmacological inhibition of mTOR
Behavioural analysis was initiated when all animals were 4 months old. Everolimus suspension was provided by Novartis (Basel, Switzerland) in a proprietary vehicle at 20 mg/ml. It was diluted in water and given at 1 mg/kg intraperitoneally [21]. Day 1 (d1): all animals were habituated for 5 min to the open field. Day 2 (d2): locomotor activity was assessed in the open field. Day 3 (d3): social interaction and social recognition memory were assessed in the open field. Body weight was recorded and animals received the first injection of 1 mg/kg everolimus. Day 5 (d5): body weight. Injection of 1 mg/kg everolimus. Day 8 (d8): body weight. Injection of 1 mg/kg everolimus. Reassessment of behavioural phenotype started on day 10 (d10): locomotor activity was assessed in the open field. Day 11 (d11): social interaction and social recognition memory. Day 32 (d32): body weight.
Locomotor activity
The open field arena had an area of 52 × 52 cm2, a height of 45 cm and was made of grey polyvinylchloride (PVC). Light intensity was 50 lx. Movements were recorded with a digital video camera and analysed on a personal computer using Biobserve Viewer (Biobserve, Bonn, Germany) tracking software. At the beginning of the 30-min session, animals were placed in the centre of the arena. Data were analysed as 5-min bins.
Social interaction
Social interaction with an unfamiliar juvenile male social partner (Long–Evans rats, Charles River, Sulzfeld, Germany, 6–7 weeks of age) was assessed in an open field as previously described [23]. The frequency of the following behaviours was quantified during the initial 5-min interaction period for the test rat only: Social exploration: (a) anogenital and (b) non-anogenital investigation of the partner (sniffing or licking the anogenital or any part except for the anogenital area, respectively) and (c) approaching and/or following the social partner throughout the test arena.
Social recognition memory
The initial 5-min social interaction period with the unfamiliar social partner (A) served as sample phase (P1) for the social recognition test [23]. In the subsequent test for social recognition memory, a second unfamiliar juvenile rat (B) was introduced into the test (P2). After the 15-min intertrial interval, the familiar (A′) and a novel social partner (B) were presented to the experimental animal for 3 min in P2. The time for social investigation (anogenital exploration, non-anogenital exploration and approach/following) was recorded during P1 and P2. For the calculation of social discrimination, the exploration time of the novel conspecific was expressed as percentage of the total exploration time of both conspecifics during P2 (100/(A′ + B) × B).
Statistics
Analyses [two-way analysis of variance (ANOVA) or two-way repeated measures ANOVA, followed by Bonferroni post hoc or multiple comparison tests, respectively, and two-way t tests] were performed with Prism software (GraphPad, San Diego, CA, USA). Differences were considered statistically significant if P < 0.05. Graphical artwork was created with Prism and CorelDraw software (Corel Corporation, Ottawa, Canada). Graphs with ANOVA show mean, standard error of the mean (SEM) and significant results from Bonferroni post hoc tests. Graphs with repeated measures ANOVA show mean and significant results from the statistical analysis, if relevant. One asterisk in a graph represents P < 0.05, two asterisks P < 0.01, three asterisks P < 0.001. “NS” indicates a non-significant result (P > 0.05).
Results
Growth assessment
The mTOR pathway is involved in general growth mechanisms. Four-month-old adult rats from both experimental groups were intraperitoneally injected with 1 mg/kg everolimus at days d3, d5 and d8 (Fig. 1). To assess an influence of everolimus on growth, body weight was measured at d3, d5, d8 and d32. Body weight was not influenced by group allocation (Fig. 2a) (two-way repeated measures ANOVA for genotype and status epilepticus [F(1,20) = 0.022, P > 0.05], time [F(3,60) = 72.12, P < 0.001] and interaction [F(3,60) = 1.144, P > 0.05]; Bonferroni multiple comparisons tests: genotype and status epilepticus at d3: P > 0.05, d5: P > 0.05, d8: P > 0.05 and d32: P < 0.05). A decrease in body weight from d3 to d8 was not significant for both experimental groups (two-way t test, Tsc2 +/− (Eker) plus DSE group: P > 0.05, control group: P > 0.05); however, a significant increase in weight could be observed from d8 to d32 (two-way t test, Tsc2 +/− (Eker) plus DSE group: P < 0.01, control group: P < 0.01).

Growth assessment and locomotor behaviour. a Body weight was assessed at experimental days d3, d5, d8 and d32. There is in both groups a non-significant tendency to growth deceleration between d3 and d8, whereas from d8 to d32, body weight increases. b Locomotor behaviour in the open field, assessed before treatment with everolimus (T1). Locomotor activity is reduced in the Tsc2 +/− (Eker) plus DSE group. c Locomotor behaviour in the open field, after treatment with everolimus (T2). Locomotor activity is still reduced in the Tsc2 +/− (Eker) plus DSE group. Graphs show mean, SEM and results from two-way repeated measures ANOVA or two-way t test, respectively. Black symbols represent the Tsc2 +/− (Eker) plus DSE group (n = 12) and white symbols control animals (n = 10). One asterisk in a graph represents P < 0.05 and two asterisks P < 0.01. “NS” indicates a non-significant result (P > 0.05)
Locomotor activity
We tested locomotor activity as a general behavioural parameter. Locomotor activity was reduced in the Tsc2 +/− (Eker) plus DSE group (Fig. 2b) (two-way repeated measures ANOVA for genotype and status epilepticus [F(1,20) = 7.853, P < 0.05], time [F(5,100) = 117.1, P < 0.001] and interaction [F(5,100) = 2.073, P > 0.05]; Bonferroni multiple comparisons tests: genotype and status epilepticus at interval 0–5 min: P < 0.001, interval 5–10 min: P > 0.05, interval 10–15 min: P > 0.05, interval 15–20 min: P < 0.05, interval 20–25 min: P < 0.05 and interval 25–30 min: P < 0.05). This effect was not affected by everolimus (Fig. 2c) (two-way repeated measures ANOVA for genotype and status epilepticus [F(1,20) = 4.880, P < 0.05], time [F(5,100) = 37.07, P < 0.001] and interaction [F(5,100) = 2.105, P > 0.05]; Bonferroni multiple comparisons tests: genotype and status epilepticus at interval 0–5 min: P < 0.001, interval 5–10 min: P > 0.05, interval 10–15 min: P > 0.05, interval 15–20 min: P < 0.05, interval 20–25 min: P < 0.05 and interval 25–30 min: P < 0.05).
Social interaction
In a previous study, we described a phenotype of impaired social interaction in Tsc2 +/− (Eker)-rats with additive social deficits contributed by DSE [18]. The analysis of social interaction repeated here, between the test animal and a social partner, included anogenital and non-anogenital exploration as well as approach and following behaviour. Total exploration was impaired in Tsc2 +/− (Eker) plus DSE rats. This effect was abrogated by everolimus treatment (Fig. 2a) (two-way ANOVA for genotype and status epilepticus [F(1,40) = 7.843, P < 0.01], everolimus treatment [F(1,40) = 0.616, P > 0.05] and interaction [F(1,40) = 2.074, P > 0.05]; Bonferroni post hoc tests: genotype and status epilepticus within pre-treatment P < 0.01, genotype and status epilepticus within post-treatment P > 0.05). Anogenital exploration was impaired in Tsc2 +/− (Eker) plus DSE rats. This effect was reversed by everolimus treatment (Fig. 2b) (two-way ANOVA for genotype and status epilepticus [F(1,40) = 5.365, P < 0.05], everolimus treatment [F(1,40) = 1.039, P > 0.05] and interaction [F(1,40) = 1.306, P > 0.05]; Bonferroni post hoc tests: genotype and status epilepticus within pre-treatment P < 0.05, genotype and status epilepticus within post-treatment P > 0.05). Similarly, non-anogenital exploration was impaired in Tsc2 +/− (Eker) plus DSE rats. Again, this effect was reversed by everolimus treatment (Fig. 2c) (two-way ANOVA for genotype and status epilepticus [F(1,40) = 8.616, P < 0.01], everolimus treatment [F(1,40) = 0.008, P > 0.05] and interaction [F(1,40) = 2.469, P > 0.05]; Bonferroni post hoc tests: genotype and status epilepticus within pre-treatment P < 0.01, genotype and status epilepticus within post-treatment P > 0.05). Finally, approach and follow behaviours was analysed. There were no differences between Tsc2 +/− (Eker) plus DSE and naïve wild-type rats, and this effect was not changed by everolimus treatment (Fig. 2d) (two-way ANOVA for genotype and status epilepticus [F(1,40) = 2.981, P > 0.05], everolimus treatment [F(1,40) = 1.334, P > 0.05] and interaction [F(1,40) = 0.756, P > 0.05]; Bonferroni post hoc tests: genotype and status epilepticus within pre-treatment P > 0.05, genotype and status epilepticus within post-treatment P > 0.05).
Social recognition memory
We continued the analysis of social behaviour by measurement of social cognition. Social recognition memory probes the ability of a test animal to distinguish between an unfamiliar social partner and a partner that was previously encountered. Healthy animals are able to distinguish and show more interest in the new partner. We observed a robust impairment of social recognition memory in Tsc2 +/− (Eker) plus DSE rats. This effect was fully reversed by the mTOR inhibitor (Fig. 4). Social discrimination expresses the exploration time of the novel conspecific as percentage of the total exploration time (Fig. 4a) (two-way ANOVA for genotype and status epilepticus [F(1,40) = 3.865, P > 0.05], everolimus treatment [F(1,40) = 4.754, P < 0.05] and interaction [F(1,40) = 2.905, P > 0.05]; Bonferroni post hoc tests: genotype and status epilepticus within pre-treatment P < 0.05, genotype and status epilepticus within post-treatment P > 0.05). The discrimination index expresses the same relation in seconds (Fig. 4b) (two-way ANOVA for genotype and status epilepticus [F(1,40) = 3.973, P > 0.05], everolimus treatment [F(1,40) = 2.003, P > 0.05] and interaction [F(1,40) = 4.570, P < 0.05]; Bonferroni post hoc tests: genotype and status epilepticus within pre-treatment P < 0.05, genotype and status epilepticus within post-treatment P > 0.05). Exploration times of the unfamiliar juvenile in P1 did not differ significantly between the groups at any time (values: P1 untreated: Tsc2 +/− (Eker) plus DSE 86 ± 6.6, controls 101.6 ± 7.6; P1 everolimus treated: Tsc2 +/− (Eker) plus DSE 51.5 ± 3.8, controls 62.7 ± 8.1; Student’s t test, P > 0.05).
Discussion
We investigated the effect of mTOR inhibitor everolimus on social behaviour deficits in adult Tsc2 +/− (Eker)-rats with previously induced status epilepticus (DSE) during development. The drug did not affect body weight. Locomotor activity was reduced in Tsc2 +/− (Eker)-rats with DSE, but not changed by everolimus. The mTOR inhibitor specifically reversed the autistic-like phenotype of impaired social exploration behaviours. It also reversed the deficits in social recognition memory.
Everolimus is a ubiquitous inhibitor of the mTOR pathway and is not restricted to neurons. Injection with everolimus (6 mg/kg) in mice, every other day from P7–P9 to P30, resulted in growth retardation [24]. At the dose of 1 mg/kg administered three times a week to adult rats from the Eker line, body weight was stable (Fig. 2). In Tsc2 +/− (Eker)-rats plus DSE, locomotor activity was reduced, seen as a trend in our previous study [18]. Developmental delay in locomotor skills is frequently observed in neurodevelopmental disorders [25]. Locomotor activity was not changed by the mTOR inhibitor, suggesting that the reduction was not regulated by the mTOR protein complex.
In the assessment of social behaviour, we first replicated in the Tsc2 +/− (Eker) plus DSE group impairment of social interaction (Fig. 3), in confirmation of our previous results [18]. Everolimus reversed the deficient social behaviour phenotype in the social interaction test. The experimental paradigm and the effect induced by the mTOR inhibitor were similar to the findings in Tsc2 +/− mice that did not have any induced or spontaneous seizures [6]. We additionally introduced a social behaviour paradigm to test short-term social recognition memory. Social cognition and its impairment, a feature of intact social and autistic behaviours in humans, respectively, had not been investigated so far in TSC animal models. Social recognition memory was impaired in the Tsc2 +/− (Eker) plus DSE group, and this impairment was also reversed by everolimus (Fig. 4).

Social interaction. Rats were assessed with a novel social partner for 5 min in the open field. a Total exploration summarises all data from anogenital, non-anogenital and approach and follow behaviours. Total exploration is reduced in the Tsc2 +/− (Eker) plus DSE group at T1. At T2, this effect is reversed. b Anogenital exploration is reduced in the Tsc2+/− (Eker) plus DSE group at T1. At T2, this effect is reversed. c Non-anogenital exploration is reduced in the Tsc2 +/− (Eker) plus DSE group at T1. At T2, this effect is reversed. d There is only a tendency to reduced approach and follow behaviours in the Tsc2 +/− (Eker) plus DSE group. Graphs show mean, SEM and results from Bonferroni post hoc tests. Black symbols represent the Tsc2 +/− (Eker) plus DSE group (n = 12), white symbols control animals (n = 10). One asterisk in a graph represents P < 0.05 and two asterisks P < 0.01. “NS” indicates a non-significant result (P > 0.05)

Social recognition memory. Rats were tested with a novel and a previously known social partner for 5 min in the open field. Social recognition probes the ability of a rat to remember and discriminate familiar from novel social partners and hence direct explorative behaviours towards the novel partner. a Social discrimination is reduced in the Tsc2+/− (Eker) plus DSE group at T1. At T2, this effect is reversed. b The discrimination index expresses the same relationship in seconds. Graphs show mean, SEM and results from Bonferroni post hoc tests. Black symbols represent the Tsc2 +/− (Eker) plus DSE group (n = 12) and white symbols control animals (n = 10). One asterisk in a graph represents P < 0.05 and two asterisks P < 0.01. “NS” indicates a non-significant result (P > 0.05)
In Tsc1 +/− and Tsc2 +/− knockout mice, animal models of Tsc1 and Tsc2 mutations alone, social interaction was impaired [5, 6]. Correlation between the phenotype and overactivated mTOR signalling was described in Tsc2 +/− mice. The mTOR inhibitor rapamycin reversed the social deficit phenotype [6]. Similarly, in Purkinje cell-specific Tsc1 mutant mice, rapamycin rescued the social deficit behaviour [5]. These pre-clinically studies provide compelling evidence of the potential of mTOR inhibitors to treat autistic behaviours in mutant TSC1 or TSC2 gene carriers. A case report of a TSC patient with a history of developmental epilepsy, infantile spasms, described beneficial effects of mTOR inhibitors on social deficit behaviours [26]. In TSC, at least 70 % of individuals with ASD also suffer from epilepsy, notably infantile spasms during development [27]. Our animal model of Tsc2 haploinsufficiency plus developmental status epilepticus may therefore represent a scenario closer to the human situation, albeit status epilepticus at P7 and P14 is itself only a model of developmental epilepsy. We have, however, previously shown that two episodes of status epilepticus during development in wild-type rats are sufficient to induce a social deficit phenotype similar to that caused by the Tsc2 +/− (Eker) mutation [18]. As outlined above, mTOR inhibitors can reverse deficient social behaviour phenotypes in Tsc1 +/− and Tsc2 +/− knockout mice [5, 6]. We demonstrated here that an mTOR inhibitor also reverses the social deficit phenotype caused by the combination of Tsc2 +/− (Eker) mutation and DSE. Thus, the mTOR inhibitor may have restored not only the social behaviour deficit caused by Tsc2 haploinsuffiency, but also that one caused by the previous experience of DSE.
The co-occurrence of ASD and epilepsy in the general population is well established [7, 28] with a rate of epilepsy in ASD estimated around 25 % [29]. There is a bimodal distribution in the age of onset of epilepsy in ASD, with a peak during development in early childhood and a larger one in adulthood [30]. In TSC, typically infantile spasms occur during early childhood and are seen as a major risk factor for both intellectual disability and ASD [3, 31–33]. Besides infantile spasms in infancy and childhood and the development of ASD or intellectual disability in TSC, there is also epilepsy itself persisting into adulthood. Both clinical phenomena presumably have overlapping aetiology and mechanisms, but could represent different trajectories in the progression of the disease. Treatment with rapamycin suppressed persisting epilepsy in Tsc1 GFAP CKO mice [34] and everolimus reduced treatment-resistant epilepsy in 2–21-year-old TSC patients [35].
Our animal model, however, is a model of early childhood epilepsy, not of persisting epilepsy. Early treatment with rapamycin, starting at P14, prevented the development of spontaneous epilepsy in Tsc1 GFAP CKO mice [34]. This suggests that the early childhood phase, which is in patients vulnerable to seizures, especially infantile spasms, is in Tsc1 GFAP CKO mice sensible to dysregulation of the mTOR complex. There is a growing body of evidence from both pre-clinical and clinical studies that mTOR inhibitors could treat infantile spasms [24, 35, 36]. These findings raise the question whether the long-term effects of developmental epilepsy in patients and DSE in animal models, on persisting epilepsy and persisting deficient social behaviours, are also mediated by dysregulation or overactivation of the mTOR complex. For persisting epilepsy, there is evidence to support this [35, 36].
TSC mutations result in overactivation of the mTOR complex which in turn is suggested to be linked with persisting ASD [37–39]. The unanswered question is, are persisting deficient social behaviours in adult animals, caused by DSE in wild-type rats or augmented in Tsc2 +/− (Eker) rats, and persisting ASD in TSC patients, augmented by early childhood epilepsy, also caused by overactivation of the mTOR pathway? The findings from our present study suggest that this could be the case, but do not prove it.
There are several limitations in our study. First, additional experimental groups with DSE in wild-type controls and Tsc2 +/− (Eker)-rats naïve for induced seizures are necessary. Although we have previously distinguished between effects caused by the factors developmental status epilepticus and Tsc2 haploinsufficiency [18], we did not do this here for subsequent mTOR inhibitor treatment. Second, we did not directly assess mTOR activity in the brains of the experimental groups to analyse the mechanisms on the mTOR pathways proposed here. Third, we did not reassess social behaviour after the mTOR inhibitor has been washed out to determine the duration of the behavioural effect. Fourth, albeit persisting epilepsy was not observed on the behavioural level of neither Tsc2 haploinsufficient nor DSE treated rats or the combination of these two factors [18], it is not known whether there are persisting epileptiform discharges on the EEG level. These would all be interesting questions to explore in future studies. In summary, our study contributes to the growing evidence on the importance of mTOR inhibitors as experimental therapies in TSC. There are a number of clinical trials underway of neurological and neuropsychiatric manifestations of TSC using mTOR inhibitors, including ASD as the primary outcome [3]. More research is necessary to further understand the role of mTOR and mTOR inhibitors in the spectrum of TSC, ASD and epilepsy.
References
Baird G, Simonoff E, Pickles A et al (2006) Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: the Special Needs and Autism Project (SNAP). Lancet 368:210–215
Tuchman R, Rapin I (2002) Epilepsy in autism. Lancet Neurol 1:352–358
Curatolo P, Moavero R, de Vries PJ (2015) Neurological and neuropsychiatric aspects of tuberous sclerosis complex. Lancet Neurol 14:733–745. doi:10.1016/S1474-4422(15)00069-1
Ehninger D, Han S, Shilyansky C et al (2008) Reversal of learning deficits in a Tsc2+/− mouse model of tuberous sclerosis. Nat Med 14:843–848
Tsai PT, Hull C, Chu Y et al (2013) Autistic-like behavior and cerebellar dysfunction in Purkinje cell Tsc1 mutant mice. Nature 488:647–651
Sato A, Kasai S, Kobayashi T et al (2012) Rapamycin reverses impaired social interaction in mouse models of tuberous sclerosis complex. Nat Commun 3:1292. doi:10.1038/ncomms2295
Riikonen R, Amnell G (1981) Psychiatric disorders in children with earlier infantile spasms. Dev Med Child Neurol 23:747–760
Primec ZR, Stare J, Neubauer D (2006) The risk of lower mental outcome in infantile spasms increases after three weeks of hypsarrhythmia duration. Epilepsia 47:2202–2205
Goh S, Kwiatkowski DJ, Dorer DJ, Thiele EA (2005) Infantile spasms and intellectual outcomes in children with tuberous sclerosis complex. Neurology 65:235–238
O’Callaghan FJ, Harris T, Joinson C et al (2004) The relation of infantile spasms, tubers, and intelligence in tuberous sclerosis complex. Arch Dis Child 89:530–533
Workman AD, Charvet CJ, Clancy B et al (2013) Modeling transformations of neurodevelopmental sequences across mammalian species. J Neurosci 33:7368–7383. doi:10.1523/JNEUROSCI.5746-12.2013
Lynch M, Sayin U, Bownds J et al (2000) Long-term consequences of early postnatal seizures on hippocampal learning and plasticity. Eur J Neurosci 12:2252–2264
Sayin U, Sutula TP, Stafstrom CE (2004) Seizures in the developing brain cause adverse long-term effects on spatial learning and anxiety. Epilepsia 45:1539–1548
Ikonomidou C, Bosch F, Miksa M et al (1999) Blockade of NMDA receptors and apoptotic neurodegeneration in the developing brain. Science 283:70–74
Lim AL, Taylor DA, Malone DT (2012) Consequences of early life MK-801 administration: long-term behavioural effects and relevance to schizophrenia research. Behav Brain Res 227:276–286. doi:10.1016/j.bbr.2011.10.052
von der Brelie C, Waltereit R, Zhang L et al (2006) Impaired synaptic plasticity in a rat model of tuberous sclerosis. Eur J Neurosci 23:686–692. doi:10.1111/j.1460-9568.2006.04594.x
Waltereit R, Welzl H, Dichgans J et al (2006) Enhanced episodic-like memory and kindling epilepsy in a rat model of tuberous sclerosis. J Neurochem 96:407–413
Waltereit R, Japs B, Schneider M et al (2011) Epilepsy and Tsc2 haploinsufficiency lead to autistic-like social deficit behaviors in rats. Behav Genet 41:364–372
Kenerson HL, Aicher LD, True LD, Yeung RS (2002) Activated mammalian target of rapamycin pathway in the pathogenesis of tuberous sclerosis complex renal tumors. Cancer Res 62:5645–5650
Kenerson H, Dundon TA, Yeung RS (2005) Effects of rapamycin in the Eker rat model of tuberous sclerosis complex. Pediatr Res 57:67–75. doi:10.1203/01.PDR.0000147727.78571.07
O’Reilly T, McSheehy PMJ, Kawai R et al (2009) Comparative pharmacokinetics of RAD001 (everolimus) in normal and tumor-bearing rodents. Cancer Chemother Pharmacol 65:625–639
Rennebeck G, Kleymenova EV, Anderson R et al (1998) Loss of function of the tuberous sclerosis 2 tumor suppressor gene results in embryonic lethality characterized by disrupted neuroepithelial growth and development. Proc Natl Acad Sci USA 95:15629–15634
Schneider M, Schomig E, Leweke FM (2008) Acute and chronic cannabinoid treatment differentially affects recognition memory and social behavior in pubertal and adult rats. Addict Biol 13:345–357
Meikle L, Pollizzi K, Egnor A et al (2008) Response of a neuronal model of tuberous sclerosis to mammalian target of rapamycin (mTOR) inhibitors: effects on mTORC1 and Akt signaling lead to improved survival and function. J Neurosci 28:5422–5432. doi:10.1523/JNEUROSCI.0955-08.2008
Rutter M, Bishop D, Pine D et al (2010) Rutter’s child and adolescent psychiatry, 5th edn. Wiley-Blackwell, Hoboken
Ishii R, Wataya-Kaneda M, Canuet L et al (2015) Everolimus improves behavioral deficits in a patient with autism associated with tuberous sclerosis: a case report. Neuropsychiatr Electrophysiol 1:6. doi:10.1186/s40810-015-0004-x
Chu-Shore CJ, Major P, Camposano S et al (2010) The natural history of epilepsy in tuberous sclerosis complex. Epilepsia 51:1236–1241. doi:10.1111/j.1528-1167.2009.02474.x
Deykin EY, MacMahon B (1979) The incidence of seizures among children with autistic symptoms. Am J Psychiatry 136:1310–1312
Woolfenden S, Sarkozy V, Ridley G et al (2012) A systematic review of two outcomes in autism spectrum disorder—epilepsy and mortality. Dev Med Child Neurol 54:306–312. doi:10.1111/j.1469-8749.2012.04223.x
Tuchman R, Cuccaro M (2011) Epilepsy and autism: neurodevelopmental perspective. Curr Neurol Neurosci Rep 11:428–434. doi:10.1007/s11910-011-0195-x
Smalley SL (1998) Autism and tuberous sclerosis. J Autism Dev Disord 28:407–414
Gomez MR, Sampson JR, Whittemore VH (1999) The tuberous sclerosis complex. Oxford University Press, New York
de Vries PJ, Prather PA (2007) The tuberous sclerosis complex. N Engl J Med 356:92
Zeng L-H, Xu L, Gutmann DH, Wong M (2008) Rapamycin prevents epilepsy in a mouse model of tuberous sclerosis complex. Ann Neurol 63:444–453. doi:10.1002/ana.21331
Krueger DA, Wilfong AA, Holland-Bouley K et al (2013) Everolimus treatment of refractory epilepsy in tuberous sclerosis complex. Ann Neurol 74:679–687. doi:10.1002/ana.23960
Wong M (2013) A critical review of mTOR inhibitors and epilepsy: from basic science to clinical trials. Expert Rev Neurother 13:657–669. doi:10.1586/ern.13.48
de Vries PJ, Howe CJ (2007) The tuberous sclerosis complex proteins—a GRIPP on cognition and neurodevelopment. Trends Mol Med 13:319–326
Ehninger D, de Vries PJ, Silva AJ (2009) From mTOR to cognition: molecular and cellular mechanisms of cognitive impairments in tuberous sclerosis. J Intellect Disabil Res 53:838–851
Napolioni V, Moavero R, Curatolo P (2009) Recent advances in neurobiology of Tuberous Sclerosis Complex. Brain Dev 31:104–113. doi:10.1016/j.braindev.2008.09.013
Acknowledgments
The work was supported by an investigator-initiated research grant from Novartis Germany to R.W. Everolimus formulation was supplied by Novartis, Basel, Switzerland. P.J.dV. was supported by the National Research Foundation of South Africa, the Programme for the Enhancement of Research Capacity (University of Cape Town) and the Struengmann Fund. Author’s contributions: R.W. designed research, M.S, K.S. and R.W. performed research, M.S. contributed new analytical tools, M.S. and R.W. analysed data, and M.S., P.J.dV., K.S., V.R. and R.W. wrote the paper. We thank Dr. David Kwiatkowski and Dr. Karsten Palfner for valuable discussions. We are grateful to Christian Gluch and Lena Wendler for excellent technical assistance.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Schneider, M., de Vries, P.J., Schönig, K. et al. mTOR inhibitor reverses autistic-like social deficit behaviours in adult rats with both Tsc2 haploinsufficiency and developmental status epilepticus. Eur Arch Psychiatry Clin Neurosci 267, 455–463 (2017). https://doi.org/10.1007/s00406-016-0703-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00406-016-0703-8