
Abstract
Purpose
This study aimed to evaluate attention, memory, and language skills in children with auditory brainstem implants and cochlear implants.
Methods
This study included 20 children with auditory brainstem implants (ABI) and 20 cochlear implanted (CI) children between the ages of 6 years and 8 years 11 months and their families. “Test of Language Development: Primary (TOLD-P:4)” was used to assess language skills, "STROOP Test, Visual-Aural Digit Span (VADS) test, and Cancellation Test" were used to evaluate attention and memory skills. In addition, the functional outcomes of hearing skills in daily life were scored by “Auditory Behavior in Everyday Life (ABEL) scale”. The significance level was determined as 0.05.
Results
Children with ABI showed lower language skills than children with CI in terms of TOLD-P:4 language test scores, STROOP sub-test completion times, and the VADS and Cancellation test scores (p < 0.05). In addition, statistically significant correlations were found between language, attention, memory skills, and auditory behavior scale.
Conclusions
This study is one of the limited numbers of studies investigating cognitive processes in children with ABI. Since attention and memory are correlated with language skills, it is recommended that the development of cognition should be considered in follow-up and intervention approaches of children with ABI and/or CI.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Cochlear implants (CI) are systems used to improve language development and hearing performance in children with severe/profound hearing loss [1]. Auditory brainstem implants (ABI) are essential for hearing and language development in situations, where cochlear implantation is contraindicated, such as neurofibromatosis type 2 (NF2), cochlear nerve deficiency or aplasia, transverse temporal bone fracture, and severe inner ear malformations [2]. It is crucial to remember that children who receive CIs or ABIs differ from one another in a variety of ways, which causes some difficulties with language and cognitive performance [3].
Language skills in children with ABI are generally evaluated with closed-set pattern discrimination, word recognition, and open-set sentence recognition tests [4, 5]. Although it is known that children's speech perception develops rapidly in CI technology, it is still unclear what factors are important for improving speech perception in ABI technology [6, 7]. Children with ABI are ready for language development and make significant progress when they begin to hear, even if they are not in line with their typically developing peers [8, 9]. Pediatric ABI users have been reported to exhibit slow progressive improvement in auditory and language skills following ABI activation [10]. Similar studies revealed that auditory brainstem implantation benefited the development of language and auditory perception [2, 11]. A study conducted on children with unilateral ABI reported that there are many variables affecting written language skills [12]. The purpose of this literature review is to illustrate that previous studies with ABI pediatric users have only assessed children on speech perception outcomes, limiting our understanding of language and cognitive skills in this population. In addition, the current study differently evaluated children using the ABI with language tests and cognitive assessment.
It is generally approved that children with ABI may develop receptive and expressive language skills, albeit more slowly, than children with CI [3, 13]. On the other hand, the relationship between language skills and cognitive skills such as memory, attention, reasoning, and perceptual function has been the subject of research for many years [14,15,16]. The cognitive skills that affect human behavior and are essential to effective environmental interaction include language, memory, reasoning, imagery, and perceptual functioning [17]. Difficulty or delay in one skill may negatively impact a child's total cognitive development, since it is a multidimensional process that is connected to the acquisition of other skills [18]. Hearing loss is a significant dimension that is strongly related to language and cognitive problems. Therefore, auditory implants can improve not only language skills but also cognitive functions [14]. However, to the author's best knowledge, there are limited studies investigating attention and memory skills in children with ABI [8, 19, 20]. According to research by Colletti et al., ABI significantly improved hearing ability and several cognitive characteristics in children who were not good candidates for CI. They also recommended against excluding children from ABI implantation if they have cochlear or cochlear nerve abnormalities and related cognitive deficiencies [19]. Although not directly cognitive tests, studies using different tests have shown that ABIs improve to some extent speech perception and language. Accordingly, the ABI has helped to make significant improvements in language, auditory perception, and communication skills [3, 8, 13, 21].
Thus, the theoretical motivation of this research question has been the interrelationships between language, cognitive skills, and hearing. In short, it can be said that (1) hearing and language are at greater risk in ABI users; (2) hearing and language are associated with the cognitive development of memory and attention; and therefore, (3) children with ABIs may be at greater risk for memory and attention delays because of their hearing and language delays. Although there is extensive literature on children with CI to explain hypotheses about the mutual effects of language and cognitive functioning [14, 22, 23], there is very little research on this issue for children with ABI. In addition, it is considered very important to have data on children with ABI as they are so unique. In the current study, there were 40 children in each group who were comparable in age, gender, family education, and etiology, using 20 bilateral CIs and 20 bimodal CI-ABIs. While previous studies have mostly focused on speech and language tasks, this study assessed language as well as cognitive skills, such as attention and memory in bimodal CI-ABI users.
The current study aimed to evaluate cognitive skills such as attention and memory as well as language skills in children using auditory brainstem implants and cochlear implants. In addition, it is aimed to contribute to the rehabilitation program by researching the strengths/weaknesses of children in cognitive function.
Methods
This study was ethically approved by the Non-Interventional Clinical Research Ethics Committee with decision number 2021/13–45. All children and their parents were informed about the content of the study and their agreement was obtained.
Participants
This study included a total of 40 children, aged 6 years to 8 years 11 months, 20 bilateral CI users and 20 bimodal users (using ABI in one ear and CI in the other ear). The inclusion criteria for the study are as follows: (1) age at diagnosis of hearing loss and age of onset of hearing aid use were less than 6 months, (2) age of the first auditory implantation surgery before 2 years, (3) had sequential or simultaneous bilateral auditory implant surgery, (4) be maximum 2 years between sequential implantations, (5) had at least 3 years of regular usage after the activation of the auditory implant, (6) be literate (those who could read a standard text in under a certain number of seconds were included), (7) a family education level of at least high school graduate. Children using bilateral CI have no inner ear and/or auditory nerve anomalies. During the auditory brainstem implant candidacy procedure, additional disabilities in child psychiatry, developmental pediatrics, neurology, etc. were examined preoperatively by experts in routine. Consequently, children with a diagnosis of additional disability in cognitive, psychological, motor, social and mental development or with syndromic hearing loss were excluded from the study.
Evaluation tools
Language, attention, and memory skills were assessed using standardized and valid tests. Test of Language Development: Primary (TOLD-P:4), The STROOP test, The Visual-Aural Digit Span (VADS) test, and The Cancellation test were performed in this order and reverse order. Children were randomly assigned to this or reverse order. No statistically significant differences were found between different orders of tests to rule out the effect of fatigue (p > 0.05). All tests were completed in a single session and lasted approximately 1 h depending on the child's cooperation. The children/parents have received interventions and evaluations on language, attention, and memory skills during the single session. These evaluations are demographical form, Test of Language Development: Primary (TOLD-P:4), The STROOP test, The Visual-Aural Digit Span (VADS) test, and The Cancellation test. All these evaluation tools were administered by a single researcher who had experience and competence in these tests.
Test of Language Development: Primary (TOLD-P:4), a norm-based test with high validity and reliability developed by P.L. Newcomer and D. Hammill, was used to assess language skills [24]. The validity and reliability study of the test was performed [25]. The TOLD-P:4 is a test applied to children between the ages of 4 and 8 years and 11 months. It consists of six main subtests: Picture Vocabulary (PV), Relational Vocabulary (RV), Word Description [26], Sentence Comprehension (SC), Sentence Repetition (SR), and Morpheme Completion (MC). As the name of the test suggests, TOLD-P:4 can evaluate the skills of semantic, syntactic, phonological, and morphological components of a language. The number of correct answers in these subtests creates the raw scores. The sums of these subtests in different combinations reflect the performance of listening, organizing, speaking, grammar, and semantics. According to this, it reflects the combined performance of PV + CS = listening, RV + SR = organizing, WD + MC = speaking, SC + SR + MC = grammar, and PV + RV + WD = semantics. The sum of all main subtests gives the verbal language score. According to TOLD-P:4 index scores, there are hierarchical descriptive categories as < 70 (very weak), 70–79 (weak), 80–89 (below average), 90–110 (average), and 111–120 (above average). Accordingly, the lower and upper categories of children's language performance are determined. The data relating to the descriptive categories according to norm values and the combined performance scores were analyzed in this study.
The STROOP test was used to assess the ability to suppress a routinized chain of behavior, especially focused attention, and to perform an unusual behavior [27]. There are four STROOP test cards with color names, colored circle shapes, and colored neutral words. There are blue, green, red, and yellow color names written in black on the first card. On the second card, these words are written in color and each word is written in a different color from the color it refers to. On the third card, there are colored printed circles. On the last card, there are colored neutral words like "as much, weak, if, medium". In the first section, the child is asked to read the words printed in black on the first card. In the second section, child is asked to read the colored printed words on the second card. In the third section, the colors of the circles are asked to be said. In the fourth section, the colors of the neutral words on the fourth card are asked to be said. In the last section, which is the most difficult step, it is expected to say the colors of the words on the second card. Here, the STROOP effect is obtained when the color used in the spelling of the word and the color the word expresses are different. For example, a Stroop effect is created, as in the word "red" written in blue [27,28,29]. The best performance in the test is 0 errors and the number of corrections and completing the test as soon as possible. The STROOP task was presented via the standard original cards of the test. One trial was conducted for each condition and completion was timed with a stopwatch. Test completion time and error/correction numbers were analyzed in this study.
The Visual-Aural Digit Span (VADS) test was used to evaluate memory capacity, sensory-motor organization, sequencing ability, attention, and/or short-term memory. This test, which was created by Koppitz in 1977, its normalization was studied, and it is a standard, valid, and reliable test with 0.90 Cronbach's alpha [30, 31]. Even though the backward number sequence is generally used for working memory evaluation [32], in this study, short-term memory skills are mostly evaluated by asking them to repeat in the order presented. Thus, the proposed methodology was followed in the validity-reliability study of the test [30, 33]. We presented the numbers by visually and audibly, then we asked participants to repeat numbers by verbally or written on one trial. As the person repeats or writes correctly, the number of sequences is increased. The maximum number of correct repeatable sequence length is recorded as a score. The sum of the auditory-verbal, visual-verbal, auditory-written, and visual-written subtests is the overall score [30, 33].
The Cancellation test was used to evaluate the participant's capacity for sustained and selective attention, visual and spatial scanning, as well as reaction time [34, 35]. This test includes four forms: regular letters, regular shapes, irregular letters, and irregular shapes. The person is asked to mark all the target letters or shapes in these forms as soon as possible. There are 60 target stimuli in each form. The color of the pencil is changed every time the child marks 10 targets, at least six different colored pencils are used for this. The benefit of colored pencils is to determine the spatial scanning direction of the child. The time to complete the test and the number of skipped/mismarked targets were analyzed in this study.
Finally, the Auditory Behavior in Everyday Life (ABEL) scale was performed to assess the reflections of hearing-related attention, memory, and language skills on daily life and parental perceptions of children's auditory behaviors. The scale is designed for parents with children aged 4–14 years who use hearing aids or auditory implants. The 24-item and 6-point Likert-type (0—Never, 6—Always) scale evaluates three basic skills in children with hearing loss: Auditory-Verbal, Auditory Awareness, and Social/Speech Skills. It is a valid, reliable, and standardized test with 0.93 Cronbach's alpha, and the overall total scores of the questionnaire were analyzed in this study [36,37,38].
Statistical analysis
Statistical analyzes were performed using the SPSS software version 25. The variables were investigated using histograms and probability plots and Kolmogorov–Smirnov/Shapiro–Wilk tests to determine whether or not they are normally distributed. The descriptive analyses were presented using mean and standard deviation for normally distributed variables and using the median and interquartile range for non-normally distributed variables. The TOLD-P:4, the STROOP, the VADS, and the Cancellation test scores of children with bilateral CI and bimodal CI-ABI were compared with the Student's t test when the values were normally distributed, and with the Mann–Whitney U test when the values were non-normally distributed. The main hypothesis of the study is to investigate whether there is a significant difference in language, memory, and attention skills between children using bilateral CI and bimodal CI-ABI. In addition, it has been mentioned in the previous sections that cognitive development is multidimensional and related to language skills. Based on this, it was investigated whether there was a relationship between language, attention, and memory skills of all children. The Pearson test was used to determine correlation coefficients and statistical significance when both variables had a normal distribution. When at least one variable has non-normal distribution, the Spearman test was performed. Type-1 error level was accepted as 5%.
Results
The mean age of the children in the ABI group (11 girls, 9 boys) was 7.51 years (SD = 0.70), and it was 7.59 years (SD = 0.76) in the CI group (11 girls, 9 boys). There was no statistically significant difference between the two groups in terms of chronological age (p = 0.736). All children were diagnosed with hearing loss before 6 months and started using bilateral hearing aids. Table 1 presents the findings about the use of hearing aids and implants in children. Accordingly, there were no statistically significant differences between the groups in terms of age at first implantation and duration of implant use.
Only two children in each group have FM systems, although they only periodically use them in a classroom or other educational environment. In terms of family education level, parents of 9 children in the ABI group have graduate degrees from high school and 11 parents have bachelor's degrees. Similarly, in the group with CI, 11 parents have a graduate degree from high school and 9 of them have a bachelor's degree. There was no statistically significant difference between the groups in terms of family education level (p = 0.532).
The children with bilateral cochlear implants performed statistically better in TOLD-P:4 scores (see Table 2). Since the findings of the grammar and semantics were normally distributed, descriptive statistics were presented as mean and standard deviation. According to the norm values of the test in verbal language performance, two of the children with CI were included in the very weak, 12 of them were in weak and 6 of them were in below average categories. On the other hand, 13 of the children with ABI were in the very weak category and 7 of them were in the weak category (see Fig. 1). In addition, Fig. 2 shows the mean values of TOLD-P:4 verbal language scores by groups in a chart.

Descriptive categories of TOLD-P:4 verbal language

Box-plot graph of TOLD-P:4 verbal language scores
The findings about the STROOP test completion times of the children are presented in Table 3. Accordingly, there were statistically significant differences between the children using ABI and CI in the STROOP test section 1, section 2, and section 5. The children with ABI completed the sections in longer times. For example, the median values of time for performing the fifth section, which is the most difficult, were 122.50 s in the ABI group, while it is 100.50 s in the CI group.
The number of errors and corrections in the fifth section of the STROOP test were also analyzed. Accordingly, the median of the error numbers of the children with CI was 0 and the interquartile range was 1, while the median of the error numbers of the children with ABI was 1 and the interquartile range was 2. The median and interquartile range for the number of corrections made in the fifth section of the test was also 2 and 2 in the CI group, and 3 and 3 in the group with ABI, respectively. There were statistically significant differences between the groups in terms of error and correction numbers (p < 0.001).
The maximum amount of repeatable digit span related to the memory skills of children is presented in Table 4. Accordingly, statistically significant differences were obtained between the groups in the auditory-verbal and visual-verbal tests. On the other hand, there were no statistically significant differences in auditory-written and visual-written tests. The mean and standard deviation of the VADS total score was 13.30 ± 2.08 in children with CI and 11.85 ± 1.84 in children with ABI. There was a statistically significant difference between the children with CI and ABI in terms of VADS total score (p = 0.025).
Statistically significant differences were found between children with CI and ABI in terms of completing time of the regular letter, regular shape, irregular letter, and irregular shape subtests in the Cancellation test (p < 0.005). Typically, the children with ABI completed the tests in a long time and skipped more targets than their peers with CI. Table 5 displays the number of incorrectly marked or skipped target letters/figures in these tests. Accordingly, no statistically significant differences were found between the groups in the number of errors in the other subtests, except for the irregular shape test errors. Besides, statistically significant differences were found between the groups in the number of skipped targets.
The ABEL auditory awareness, social/speech skills, and overall scores were analyzed. Accordingly, while the ABEL general score was 83.05 ± 11.49 in the ABI group, it was 97.05 ± 9.01 in the CI group. Median–interquartile range of ABEL auditory awareness scores were 60–33 and 30.5–49 in ABI and CI groups, respectively. The median-interquartile range of the scores obtained in the social/speaking skills questions were 22–17, and 69–57 in the ABI and CI groups, respectively. Statistically significant differences were found between children with CI and ABI in terms of all the ABEL scores (p < 0.001).
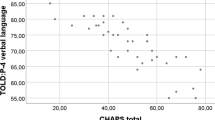
The relationships between attention, memory skills, and language skills were analyzed by the scores of all participants. Accordingly, the relationships between the TOLD-P:4 verbal language score and the STROOP five sections completion times, VADS scores, and Cancellation test completion times were investigated (see Table 6). There were statistically significant correlations between the completion times of the five sections of the STROOP test and the TOLD-P:4 verbal language score. These negative relationships were strong for sections 1, 2, 3, and 5, and moderate for section 4. Focused attention and coping with the STROOP effect are associated with verbal language skills. The faster children complete the STROOP test, the better their language skills.
Similarly, TOLD-P:4 verbal language scores were positively significantly related to the VADS scores; low–moderate with auditory-verbal score, moderately with auditory-written score, and moderate with an overall score. Apart from these, no statistically significant correlations were found between visual-verbal and visual-written scores and verbal language skills. The verbal language skills improved with greater short-term and working memory.
There were significant negative correlations between sustained attention skills (Cancellation test scores) and verbal language skills as follows: strong with a completion time of regular letter test, regular shape test, irregular letter test, irregular shape test. Sustainable attention, visual-motor synchronization, and selective attention skills are also associated with verbal language skills. The faster children can perform on the Cancellation test, the better their language skills. Finally, with the ABEL overall score; the VADS overall score and completion time of the STROOP section 5 were moderately statistically significantly related. There were significant positive correlations between the verbal language score and the total ABEL score, the social/speech skills, and the auditory awareness score. In general, the better the language-memory-attention skills, the better children's daily auditory behavior.
Discussion
This study is one of the limited numbers of studies evaluating language, attention, and memory skills in children with bilateral CI and bimodal CI-ABI. It revealed that language and cognitive skills are related and that children with bilateral CI perform better. Especially, children with ABI are one of the populations that should be carefully controlled. They are influenced by several factors, including hearing loss before implantation, difficulty with audiological evaluation, different surgical techniques, anatomical and tonotopic characteristics of the implantation site, unfavorable side effects, challenges with fitting sessions, and slow rehabilitation progress [6, 7, 39]. In addition to studies focusing on language skills and auditory performance in children with ABI [10, 12, 39, 40], attention and memory processes that support the development of language skills should also be investigated.
Similar to this study, it was stated that auditory perception and language development are supported by ABI in children [4, 6, 8]. On the other hand, their language skills fall behind compared to children with CIs, which may be due to the difficulties of auditory brainstem implantation in terms of surgery, programming, and rehabilitation follow-up [39]. Thus, while bilateral CIs are very effective, the effectiveness of ABIs may be limited. Unlike studies [6, 8, 19, 39] conducted on children with only ABI, the current study provides important findings by including 40 volunteer children with CI-ABI and bilateral CI who are relatively homogeneous in terms of many variables. To the best knowledge of the authors, the attention and memory skills assessment tools used in the present study were not previously applied to children with ABI.
The ability to disrupt a routinized chain of behavior, especially focused attention, was assessed with the STROOP test. Since it is the most difficult task here, the ability to read the color names written in different colors in the fifth section was included in the analysis. There was a significant difference between the two groups in terms of completion times in the first, second, and fifth sections of the STROOP test and no difference in the third and fourth sections may be related to the type of task. The third and fourth sections may be relatively easy and familiar tasks that do not require high-level processing for both ABI and CI users. In addition, the number of errors made in the fifth section is detected more in ABI users and this may be due to poor focused attention skills, since these children divided their cognitive resources [20] more for hearing-related tasks.
Likewise, the differences between the two groups in all subsections in the Cancellation test, which specifically measures selective attention and sustained attention skills, are consistent with other findings. The differences between the two groups in terms of visual and spatial scanning and/or perception of visual selectivity and visual-motor synchronization skills measured by the Cancellation test may be due to the weaker sustained attention skills of children with ABI. Similarly the current study, it was revealed that children using ABI need more development in terms of memory and attention processes [9]. In addition, Sennaroğlu et al. stated that attention deficit hyperactivity disorder; mild mental retardation and vision problems accompanying hearing loss may cause language development delays in children using ABI [41].
Furthermore, the current study determined that children had more difficulties in the VADS subtests which required auditory stimulation and verbal response, that is, in tasks which hearing and language skills were predominantly used. The study by Colletti et al. in children using ABI clearly showed that improvement in auditory perception provides a significant development in cognitive skills. They also noted that children with cochlea and/or cochlear nerve malformations along with cognitive deficits should not be excluded from ABI [19]. There were no statistically significant differences between the two groups in the auditory-written and visual-written scores in the VADS tests. This situation can be explained by the common difficulties of both groups in their ability to express themselves in writing while storing and processing information for a short time. It has been previously reported that not only verbal communication but also visual elements such as visual cues, gestures and facial expressions, and sign language are at the forefront in the communication of children with ABI [6, 42]. Similar scores on the VADS visual subtests may be explained by the similarity of ABI users to their peers with CI, thanks to the use of visual elements and cross-model reorganization.
As in the current study, it is important to note that children with ABI show significant development in selective visual/spatial attention, memory, and multisensory executive functions with the auditory input [4, 14]. On the contrary, a child with hearing loss has difficulty coding the information, because he/she cannot receive the auditory stimulus with all its acoustic properties. Since the child receives incomplete and/or distorted stimuli, he/she cannot sustain attention, has difficulties in working memory performance related to encoding and learning pathways may be negatively affected. Thus, the current study is important in terms of being helpful in the follow-up and intervention processes of children with ABI and guiding the experts working on this issue. This study emphasized that cognitive skills, such as short-term memory, working memory, sustained attention, and selective attention, which are closely related to the development of language skills, should also be developed.
Children with auditory implants have difficulties in providing joint attention in changing conditions, using selective attention skills toward the target sound source, and focusing. This situation can be predicted from the answers given by the parents to the questions about listening environments encountered in daily life in the ABEL subsections. Since children cannot fully receive the auditory stimulus, they may be more distracted and separated from the communication's context and the target speaker. Daily life hearing performance is closely related to language, attention, and memory skills. On the other hand, there are a limited number of studies evaluating daily life hearing performance and quality of life in ABI users. Similar to current findings, it was revealed that people's quality of life improves significantly with ABI [43].
The study's limitations include the variety of implant models, processing techniques, and hearing loss etiologies. Because few studies have investigated language, attention, and memory skills as well as hearing quality in children with ABI, there are limitations in how the findings can be discussed. Furthermore, since the intelligence of children with auditory implants, including general fluid intelligence, is routinely assessed in a multidisciplinary approach in the preoperative evaluation, the children's general fluid intelligence was not tested separately in this study. As a result, it is impossible to determine whether the differences between the groups were caused by variations in the particular cognitive domains tested, or by general cognitive differences between these two populations. Finally, children who have bilateral CI and bimodal CI-ABI were included in this study. According to the experience of the authors, it is suggested that children with only ABI may experience difficulties in cooperating with the tests, depending on their developmental level, but it is recommended to be investigated. Future studies with similar evaluations for bilateral ABI users are needed.
Besides, the absence of additional disabilities in the children with ABI included in the current study and the homogeneity in terms of implant age, duration of deafness, etc. are the remarkable points of the study. The sample size of 40 children ensures homogeneity across the groups in these categories, which is another positive aspect. To the best of the authors' knowledge, it is the only study in the current literature that uses the VADS and The Cancellation, the STROOP tests, and a scale for daily living hearing performance in children with ABI. Shortly, this study is significant and distinctive, since there is a lack of information on the cognitive outcomes of children with ABIs. The investigation of cognitive/language outcomes following ABI, the study's focus on children aged 6 years to 8 years 11 months, and the study's relatively high sample size for the demographic and age range under study are its strong points.
Conclusion
This study revealed that children with bilateral CI had better performance than children with bimodal CI-ABI in school-age language skills, selective attention, focused attention, sustained attention, visuospatial perception and visual-motor synchronization, short-term memory, and working memory, and daily life hearing performance. This may be due to the limited effectiveness of the ABI compared to the CI. The intervention and follow procedures should be considered the strengths and weaknesses in cognitive skills, such as attention and memory, as well as the language and communication skills of children with ABI.
Data availability
The data supporting the results reported in the manuscript are kept by the first author. Where appropriate, data analyzed or generated during the study may be shared.
References
Sharma SD, Cushing SL, Papsin BC, Gordon KA (2020) Hearing and speech benefits of cochlear implantation in children: a review of the literature. Int J Pediatr Otorhinolaryngol 133:109984
Martins QP, Gindri BDFS, Valim CD, Ferreira L, Patatt FSA (2023) Hearing and language development in children with brainstem implants: a systematic review. Braz J Otorhinolaryngol 88:225–234
van der Straaten TF, Netten AP, Boermans PPB, Briaire JJ, Scholing E, Koot RW et al (2019) Pediatric auditory brainstem implant users compared with cochlear implant users with additional disabilities. Otol Neurotol 40(7):936–945
Colletti L (2007) Beneficial auditory and cognitive effects of auditory brainstem implantation in children. Acta Otolaryngol 127(9):943–946
Sennaroglu L, Ziyal I, Atas A, Sennaroglu G, Yucel E, Sevinc S et al (2009) Preliminary results of auditory brainstem implantation in prelingually deaf children with inner ear malformations including severe stenosis of the cochlear aperture and aplasia of the cochlear nerve. Otol Neurotol 30(6):708–715
Aslan F, Yücel E, Sennaroglu G, Yaralı M, Sennaroglu L (2022) Audiological outcome with ABI. Inner ear malformations. Springer, pp 349–361
Sennaroglu L, Sennaroglu G, Yücel E (2022) Cochlear nerve deficiency and current management of ınner ear malformations. Inner ear malformations: classification, evaluation and treatment. Springer, pp 363–379
Sung JKK, Luk BPK, Wong TKC, Thong JF, Wong HT, Tong MCF (2018) Pediatric auditory brainstem implantation: impact on audiological rehabilitation and tonal language development. Audiol Neurotol 23(2):126–134
Yucel E, Aslan F, Özkan HB, Sennaroglu L (2015) Recent rehabilitation experience with pediatric ABI users. Int Adv Otol. https://doi.org/10.5152/iao.2015.915
Fernandes NF, Gomes MDQT, Tsuji RK, Bento RF, Goffi-Gomez MVS (2020) Auditory and language skills in children with auditory brainstem implants. Int J Pediatr Otorhinolaryngol 132:110010
Yousef M, Mesallam TA, Almasaad A, Alhabib S, Hagr A, Alzhrani F (2021) Cochlear implantation versus auditory brainstem implantation in children with auditory nerve deficiencies. Eur Arch Oto-Rhino-Laryngol. https://doi.org/10.1007/s00405-021-06792-8
Ozkan HB, Aslan F, Yucel E, Sennaroglu G, Sennaroglu L (2022) Written language skills in children with auditory brainstem implants. Eur Arch Otorhinolaryngol 279(8):3937–3945
Baş B, Yücel E (2022) Evaluation of phoneme recognition skills in pediatric auditory brainstem implant users. Eur Arch Otorhinolaryngol 279(4):1741–1749
Almomani F, Al-Momani MO, Garadat S, Alqudah S, Kassab M, Hamadneh S et al (2021) Cognitive functioning in deaf children using Cochlear implants. BMC Pediatr 21(1):1–13
Nittrouer S, Caldwell-Tarr A, Low KE, Lowenstein JH (2017) Verbal working memory in children with cochlear implants. J Speech Lang Hear Res 60(11):3342–3364
Zhang H, Ma W, Ding H, Peng G, Zhang Y (2022) Phonological awareness and working memory in Mandarin-speaking preschool-aged children with cochlear implants. J Speech Lang Hear Res 65(11):4485–4497
Almomani F, Al-Sheyab NA, Al-Momani MO, Alqhazo M (2018) Memory and potential correlates among children in Jordan. BMC Psychiatry 18:1–9
Meinzen-Derr J, Wiley S, Choo DI (2011) Impact of early intervention on expressive and receptive language development among young children with permanent hearing loss. Am Ann Deaf 155(5):580–591
Colletti L, Zoccante L (2008) Nonverbal cognitive abilities and auditory performance in children fitted with auditory brainstem implants: preliminary report. Laryngoscope 118(8):1443–1448
Miyamoto RT, Wong D, Pisoni DB, Hutchins G, Sehgal M, Fain R (1999) Positron emission tomography in cochlear implant and auditory brain stem implant recipients. Am J Otol 20(5):596
Yousef M, Mesallam TA, Garadat SN, Almasaad A, Alzhrani F, Alsanosi A et al (2021) Audiologic outcome of cochlear implantation in children with cochlear nerve deficiency. Otol Neurotol 42(1):38–46
Hu Z, Sun J-Q, Guan R-R, Chen L, Sun J-W, Guo X-T (2021) Deficient sensory and cognitive processing in children with cochlear implants: an event-related potential study. Hear Res 408:108295
Torkildsen JBK, Hitchins A, Myhrum M, Wie OB (2019) Speech-in-noise perception in children with cochlear implants, hearing aids, developmental language disorder and typical development: The effects of linguistic and cognitive abilities. Front Psychol 10:2530
Newcomer PL, Hammill DD (2008) TOLD-P: 4: test of language development. Primary, Pro-Ed Austin
Topbaş S, Güven O (2017) Türkçe Okulçağı Dil Gelişimi Testi-TODİL [Test of Language Development–Fourth Edition: Turkish Version]. Detay Yayıncılık
Gantz BJ, Turner C, Gfeller KE, Lowder MW (2005) Preservation of hearing in cochlear implant surgery: advantages of combined electrical and acoustical speech processing. Laryngoscope 115(5):796–802
Karakaş S, Erdoğan E, Sak L, Soysal AŞ, Ulusoy T, Ulusoy İY et al (1999) Stroop Testi TBAG Formu: Türk kültürüne standardizasyon çalışmaları, güvenirlik ve geçerlik. Klinik Psikiyatri 2(2):75–88
Karaka S et al (2006) Path analysis of stroop test performance: Attention and/or interference? Int J Psychophysıol 61(3):347–348
Stroop JR (1992) Studies of interference in serial verbal reactions. J Exp Psychol Gen 121(1):15
Karakas S (1995) Görsel İşitsel Sayı Dizileri Testi B Formunun 13–54 Yaş Grupları Üzerideki Standardizasyon Çalışması. Turk Psikoloji Derg 10(34):20–31
Karakaş S, Eski R, Başar E (1996) Türk kültürü için standardizasyonu yapılmış nöropsikolojik testler topluluğu: BİLNOT Bataryası. 32. Ulusal Nöroloji Kongresi Kitabı Türk Nöroloji Dergisi ve Bakırköy Ruh ve Sinir Hastalıkları Hastanesi İstanbul, Ufuk Mat
Mashburn CA, Burgoyne AP, Engle RW (2023) Working memory, intelligence, and life success. Memory in science for society: there ıs nothing as practical as a good theory. Oxford University Press, Oxford, p 149
Koppitz EM (1981) The visual aural digit span test for seventh graders: a normative study. J Learn Disabil 14(2):93–95
Kılıç BG, Irak M, Koçkar Aİ, Şener Ş, Karakaş S (2002) İşaretleme Testi Türk Formu’nun 6–11 Yaş Grubu Çocuklarda Standardizasyon Çalışması. Klinik Psikiyatri Derg 5(4):213–228
Weintraub S, Mesulam M-M (1987) Right cerebral dominance in spatial attention: further evidence based on ipsilateral neglect. Arch Neurol 44(6):621–625
Avcı Can Ö, Baydan Aran M, Tokgöz YS (2022) Turkish Validity and Reliability Study of Auditory Behavior in Everyday Life Scale. Türk Klinikleri Sağlık Bilimleri Derg 7(2):484
Özses M, Ozbal Batuk M, Yilmaz Isikhan S, Cicek CB (2022) Validity and Reliability of Turkish Version of the Auditory Behavior in Everyday Life Questionnaire. Am J Audiol 31(1):155–165
Purdy SC, Farrington DR, Moran CA, Chard LL, Hodgson S-A (2002) A parental questionnaire to evaluate children’s Auditory Behavior in Everyday Life (ABEL). Am J Audiol. https://doi.org/10.1044/1059-0889(2002/010)
Aslan F, Ozkan HB, Yücel E, Sennaroglu G, Bilginer B, Sennaroglu L (2020) Effects of age at auditory brainstem implantation: impact on auditory perception, language development, speech intelligibility. Otol Neurotol 41(1):11–20
Eisenberg LS, Hammes Ganguly D, Martinez AS, Fisher LM, Winter ME, Glater JL et al (2018) Early communication development of children with auditory brainstem implants. J Deaf Stud Deaf Educ 23(3):249–260
Sennaroglu L, Sennaroglu G, Atay G (2013) Auditory brainstem implantation in children. Curr Otorhinolaryngol Rep 1(2):80–91
Rouger J, Lagleyre S, Démonet JF, Fraysse B, Deguine O, Barone P (2012) Evolution of crossmodal reorganization of the voice area in cochlear-implanted deaf patients. Hum Brain Mapp 33(8):1929–1940
Fernandes NF, Goffi-Gomez MVS, Magalhães ATDM, Tsuji RK, De Brito RV, Bento RF (2017) Satisfaction and quality of life in users of auditory brainstem implant. CoDAS. https://doi.org/10.1590/2317-1782/20172016059
Funding
No.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
No.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yildirim Gökay, N., Yücel, E. Evaluation of language, attention, and memory skills in children with auditory brainstem implants. Eur Arch Otorhinolaryngol 281, 1683–1692 (2024). https://doi.org/10.1007/s00405-023-08262-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-023-08262-9