
Abstract
This study aimed to test the association between the European GWAS-identified risk IQGAP2 SNP rs457717 (A>G) and age-related hearing impairment (ARHI) in a Han male Chinese (HMC) population. A total of 2420 HMC subjects were divided into two groups [group 70+: >70 years (n = 1306), and group 70−: ≤70 years (n = 1114)]. The participants were categorised into case and control groups according to Z high scores for group 70− and the severity of hearing loss and different audiogram shapes identified by K-means cluster analysis for group 70+. The IQGAP2 tagSNP rs457717 was genotyped in accordance with the different ARHI phenotypes. The genotype distributions of IQGAP2 (AA/AG/GG) were not significantly different between the case and control groups (P = 0.613 for group 70−; P = 0.602 for group 70+). Compared with genotype AA, the ORs of genotypes AG and GG for ARHI were not significantly different following adjustment for other environmental risk factors. We demonstrated that the IQGAP2 TagSNP rs457717 (A/G) was not associated with ARHI in HMC individuals.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Age-related hearing impairment (ARHI), also known as presbycusis, is a multifactorial symmetric sensorineural loss that affects adults older than 50 years of age [1]. It is the most common sensory impairment and one of the top three chronic diseases among the elderly alongside cardiovascular problems and arthritis [2–4]. Environmental factors, including systemic diseases, central obesity, obstructive sleep apnoea, noise, chemical exposure, tobacco, ototoxic medication, hormonal replacement therapy, and socioeconomic status, have been reported to be associated with peripheral hearing function [5–7]. Genetic effects have been clearly demonstrated to account for approximately 50 % of the variances in ARHI [8–12]; however, the genetic factor that specifically determines the susceptibility to ARHI was not clarified until recently.
Before the advent of the genome-wide association study (GWAS) [13–15], several association studies based on a candidate gene approach were conducted to study the genetic susceptibility of ARHI. The potassium voltage-gated channel member 4 gene (KCNQ4, OMIM ID: 603537) [16], N-acetyltransferases (NAT2*6A, OMIM ID: 612182) [17–19], grainyhead-like 2 gene (GRHL2, OMIM ID: 608576) [20], Apolipoprotein E gene (APOE allele ε4, OMIM ID: 107741) [21], endothelin-1 gene (EDN1, OMIM ID: 131240) [22, 23], uncoupling protein gene (UCP2, OMIM ID: 601693) [24] and the mitochondrial DNA (mtDNA) 4977 common deletion have all been reported to correlate with ARHI [25, 26]. However, it is now widely accepted that a large-sample GWAS followed by verification in different populations represents the most direct and convincing evidence.
Based on a pooling GWAS, Friedman et al. reported an association between susceptibility to ARHI and variants of the glutamate receptor-7 gene (GRM7) [14]; GRM7 gene encodes a metabotropic glutamate receptor assumed to modulate hair cell excitability and synaptic efficacy. Newman et al. explored the relationship between the GRM7 haplotype and SNP genotypes with various measures of auditory perception in a European American population [27]. Another GWAS for ARHI was presented by Van Laer et al. in a Finnish Saami population [15], who are descendants of Europeans and East Asians, and also found that the top-ranked SNPs, rs457717 (coordinate: 75956728; P value 3.55E−07) and rs1697845 (coordinate: 75958260; P value 1.63E−05), located on intron 13 of the IQ motif-containing GTPase activating-like protein (IQGAP2, OMIM ID: 605401), were associated with ARHI. It is known that these two polymorphisms (rs457717 and rs1697845) in IQGAP2 were in strong linkage disequilibrium (LD) in the Finnish Saami population (D′ = 1; r 2 > 0.8). IQGAP2 is a member of the Ras superfamily of GTPases, which regulates a wide variety of cellular signalling pathways. IQGAP2 is expressed inside the cochlea [28] and has been implicated in cadherin-mediated cell adhesion [29]. However, a replication study in other populations has not been reported.
The aim of this study was to investigate the association between the IQGAP polymorphism, either rs457717 or rs1697845, and ARHI susceptibility in a large cohort of a southern Chinese Han subpopulation using different audiology data analyses. We analysed audiology data using the “Z score” method [30] based on the ISO standard in volunteers under the age of 70 years. To ensure accuracy of results, we used the statistical method “K means cluster analysis” [31] for subjects over the age of 70 years, who are not included in the current ISO standard [32].
Materials and methods
The institutional review Ethics boards of Shanghai Jiatong University School of Medicine, Xinhua Hospital and RenJi Hospital approved the study protocol. The protocol was in compliance with the Declaration of Helsinki, and written informed consent was obtained from all participants.
Subjects
Subjects for this case–control study were recruited from the same geographical region (Shanghai) and were of the same ethnic origin (southern Chinese HAN population), but no subject was related to any other subject in the study. Male adult volunteers, aged 50–100 years, were recruited between July 2011 and July 2014 from the health check-up centres of Xinhua and RenJi Hospitals, which are affiliated with the Shanghai Jiatong University School of Medicine.
Clinical evaluation and audiological measurements
Health check-up centres offer routine annual health examinations, which include a short questionnaire of demographic data, systemic disease history and health behaviours (smoking, alcohol consumption) and a basic physical examination including body height, body weight, a chest X-ray, electrocardiography, and blood biochemistry tests.
Information regarding hearing loss history, including exposure to noise and ototoxic drug exposure, was also collected. An otoscopic examination was then conducted to exclude any ear pathology potentially affecting hearing. Audiological results were measured with air and bone conduction thresholds of pure tones with an audiometer (TDH39 earphone, Madsen Itera Inc, Taastrup, DENMARK.). Air conduction thresholds were assessed at 0.25, 0.5, 1, 2, 4, and 8 kHz, and bone conduction was assessed at 0.5, 1, 2, and 4 kHz. Pure-tone thresholds were measured in a quiet room and in each ear separately. A blood sample was taken from the subjects at the time of testing.
Individuals with symmetric sensorineural hearing loss were screened and included for genotyping and further analysis. In general, subjects with a pathology reported to influence hearing were excluded according to an extended exclusion list designed by an international European consortium [16].
PTA4 representing a pure-tone threshold average over 0.5, 1, 2, and 4 kHz of the better hearing ear, as adopted by the World Health Organization, was used in our analyses [33].
Z score method for subjects under the age of 70 years (group 70−)
According to the ISO 7029 standard, frequency-specific thresholds were converted into age- and sex-independent Z scores [30], representing the number of standard deviations by which hearing threshold differs from the median at a given frequency. For both ears of each participant, Z scores at 2, 4, and 8 kHz were averaged as Z high, and Z scores at 0.25, 0.5, and 1 kHz were averaged as Z low. Only the Z high of the better hearing ear was used for the analysis. The participants were then categorised into the case group (the 25 % of participants with the poorest hearing) or the control group (the 25 % participants with the best hearing), according to their Z high scores.
K means cluster analysis for subjects over the age of 70 years (group 70+)
The Z score method is not suitable for individuals over the age of 70 years because the age range for which the equation is valid in the current ISO 7029 standard is 18–70 years, inclusive [32]. According to WHO standardised hearing loss categories, normal hearing is defined as a hearing threshold of 0–25 dB for the better ear, and hearing impairments at 41 dB HL or above are defined as disabling [33]. The upper age limit of ISO 7029 is 70 years. There is no standard method for hearing correction over the age of 70 years, and so, the participants in Group 70+ who met our ARHI inclusion and exclusion criteria were categorised into the case group (PTA4 > 25 dB) or the control group (PTA4 ≤ 25 dB). For a more detailed analysis of the different hearing phenotypes of the ARHI case group, we employed K means cluster analysis as described by Lee to categorise the audiometric pattern shapes [31].
Genotyping
Genetic and statistical analyses were performed in the Molecular Biology of Hearing and Deafness Research Laboratory, Ear Institute, Shanghai Jiaotong University. Genomic DNA was extracted from whole blood samples using a standard extraction method. Risk SNPs rs457717 and rs1697845 also exist in Chinese Han in Beijing (CHB) dbSNP and are highly correlated (D′ = 1; r 2 = 0.965) [HapMap data on Rel 27 PhaseII + III, Feb09 (based on NCBI B36 assembly) dbSNP b126 (http://hapmap.ncbi.nlm.nih.gov/cgi-perl/gbrowse/hapmap27_B36/#search)]. Mutation screening of the IQGAP2 gene was performed using nest PCR amplification and directional sequencing. For the IQGAP2 region, including the SNP locus rs457717 (A/G coordinate: 75920972) shown in the HapMap, the forward and reverse of the first pair of PCR primers were 5′ TTATCCCAGCTACTTGGGAG 3′ and 5′ ATCTGGGCTAAAGGAGACCTC 3′, respectively. The forward and reverse of the second pair of PCR primers were 5′ GAGAATAGCTTGACCCTGAG 3′ and 5′ ATCTGGGCTAAAGGAGACCTC 3′, respectively.
The 25 μL PCR reactions were performed in a 2720 Thermal Cycler (Applied Biosystems, Foster City, CA). The PCR cycling conditions included an initial denaturation step at 94 °C for 5 min followed by 33 cycles of denaturation at 94 °C for 30 s, annealing at 55 °C for 45 s, extension at 72 °C for 45 s, and a final extension step at 72 °C for 7 min. Sequencing of the product after PCR was performed using an ABI PRISM 3730xl Genetic Analyzer (Applied Biosystems).
Statistical analyses
The data are presented as mean ± standard deviation unless indicated otherwise. SNPs were tested using a Chi squared test for Hardy Weinberg Equilibrium. The statistical power of the study was estimated using QUANTO software version 1.2 4 (http://hydra.usc.edu/gxe/). A significant association between SNPs was tested using the Chi square test or Fisher’s exact test for genotype frequency distributions and allele frequency between ARHI patients and healthy controls. Association of SNP with ARHI was further confirmed by logistic regression analysis adjusted for possible confounding factors, including central obesity (CO), and cardiovascular disease (CAD), hypertension (HTN), diabetes mellitus (DM), dyslipidaemia (DL), chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), anaemia, osteoporosis (OP) smoking, and alcohol consumption (AC). Odds ratios (ORs) and 95 % confidence intervals (CIs) were used to analyse the occurrence of the high-risk genotypes in the Chinese Han population sample. The level of significance was set at 0.05 to correct for the effects of multiple comparisons. All calculations were performed using the statistical software package 19.0.0 (IBM SPSS Statistics, Inc., Chicago, IL).
Results
A total of 2420 Han Chinese male volunteers who meet the inclusion and exclusion criteria were recruited to participate in this study. They were divided into two groups, group 70+ (>70 years; n = 1306) and group 70− (≤70 years; n = 1114). Whole blood samples of all subjects were collected and subjected to genotyping for the SNP rs457717.
Group 70−
The participants of group 70− were categorised into the case group (n = 279, 25 % with poorest hearing) and the control group (n = 278, 25 % with best hearing) according to the Z high score converted from the original frequency-specific hearing thresholds.
The mean age was similar in the case and control groups (63.38 ± 5.214 vs 62.99 ± 5.539 years). The mean Z high score was higher in the case group (1.213 ± 0.401) than in the control group (−0.555 ± 0.216).
Table 1 shows the distributions of IQGAP2 rs457717 genotypes and other variables in the control and case groups for group 70− according to the Z high scores. Genotype distributions of the IQGAP2 rs457717 (AA/AG/GG) were not significantly different between the control and case groups (χ 2 test, P Unadjusted = 0.613). We also compared allele frequencies of rs457717 for group 70− (ORUnadjusted 1.114 (95 % CI = 0.883–1.409), P freq = 0. 37).
Logistic regression models were constructed to control potential confounding effects of other non-genetic factors on the correlation between IQGAP2 genotypes and audiological phenotypes. As shown in Table 2, the OR of the AG and GG genotypes of IQGAP2 rs457717 for ARHI did not decrease significantly compared with genotype AA of IQGAP2 rs457717 after adjusting for other environmental risk factors (OR 1.212, 95 % CI 0.793–1.855, P = 0.375 for AG; OR 1.261, 95 % CI 0.806–1.973, P = 0.310 for GG).
Group 70+
A total of 1306 male volunteers (age >70 years) met our selection criteria. As the Z score method is not suitable for subjects over the age of 70 years [32], we used a pure-tone threshold average over 0.5, 1, 2, and 4 kHz (PTA4) of the better ear to further assign these subjects into the healthy control (PTA4 ≤ 25 dB, n = 324) and case (PTA4 > 25 dB, n = 982) groups. For the control group, the mean age was 80.31 ± 5.373 years (71–94 years), and the average PTA of the better ear was 21.23 ± 2.84 dB. A total of 982 subjects were included in the ARHI case group. The mean age of this group was 80.84 ± 5.45 years (71–100 years), and the average PTA4 of the better ear was 43.78 ± 13.84 dB. There was no significant difference in age between the ARHI case and control groups.
Table 1 shows that distributions of the IQGAP2 rs457717 genotypes (AA/AG/GG) were not significantly different between the control and case groups for group 70+ (χ 2 test, P Unadjusted = 0.602). Logistic regression models were constructed to control for potential confounding effects of other non-genetic factors on the correlation between IQGAP2 genotypes and audiological phenotypes. As shown in Table 2, the OR of the AG and GG genotypes of IQGAP2 rs457717 for ARHI did not decrease significantly compared with genotype AA of IQGAP2 rs457717 after adjusting for other environmental risk factors (OR 1.131, 95 % CI 0.827–1.546, P = 0.442 for AG; OR 1.170, 95 % CI 0.837–1.633, P = 0.358 for GG).
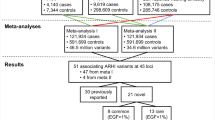
Two methods (classification using the WHO grades of hearing impairment and K-means cluster analysis) were applied to further evaluate the hearing impairment of the case group within group 70+, followed by the association studies on the relationship between IQGAP2 rs457717 genotypes and hearing impairment within the case group (Tables 3, 4, 5).
First, according to the WHO grades of hearing impairment, which define the severity of hearing loss based on the volume at which pure tones can be heard in the audiometric test, the case group was further categorised into 4 subgroups: mild (26–40 dB, n = 464), moderate (41–60 dB, n = 409), severe (61–80 dB, n = 90) and profound (81 dB or greater, n = 19) hearing impairments (Table 3). WHO has defined hearing impairment for the better ear at 41 dB or above as disabling hearing impairment [33]. According to this classification, the moderate, severe and profound hearing loss subgroups, which comprise 518 subjects, were defined as having disabling hearing impairment (Table 3). Second, within group 70+, four audiogram shapes were identified by K means cluster analysis [31, 34], i.e., 2–4 kHz abrupt loss (AL), 8-kHz dip (8D), down-sloping (SL) and flat (FL) shapes.
We next investigated the distribution patterns of the SNP rs457717 genotypes of the control group (n = 324) and different case subgroups classified by either the WHO grades of hearing impairment or the K means cluster analysis. As shown in Table 3, the percentage of each SNP rs457717 genotype was similar among these groups. In addition, the relationship between SNP rs457717 and ARHI in the case group was further confirmed by the logistic regression analysis adjusted for possible confounding factors (Tables 4, 5). However, genotypes AG and GG of IQGAP2 rs457717 appeared to be unrelated to hearing impairment within each ARHI subgroup (Tables 4, 5).
Discussion
It is extremely important to study real ARHI patients, as it is well known that environmental noise and ototoxic agents can influence hearing in the elderly. A difference due to gender has also been universally acknowledged as a major factor that influences hearing loss with age. Hearing loss due to age tends to decline faster and earlier, and the loss is more severe in men than in women [35–37]. Thus, environmental factors must be strictly excluded to avoid confusion and interference by compounding variables during research on the genetic factors of ARHI, and studies should be carefully designed to account for the influence of gender in studies of ARHI. This is why we have selected only male volunteers and designed strict inclusion and exclusion criteria to carry out this research.
The Z score method has been widely used in previous ARHI association studies and converts frequency-specific thresholds to a gender- and age-independent value [14, 16, 20], referred to as the Z score based on the ISO 7029 standards. The current ISO standard does not include subjects older than 70 years of age. Due to this restriction, case–control association studies on genetic susceptibility to ARHI rarely involve the elderly population (those over the age of 70 years). However, we believe that those over the age of 70 years are likely to be more representative for ARHI genetic susceptibility research. There is considerable variation in the age of onset, progression and severity of ARHI, even though every individual shows a steady decline in hearing ability with age. Even if hearing is completely normal under the age of 70 years in an individual, this may not be the case once they are over the age of 70 years. In other words, it is possible that the control group also contained some patients with ARHI in the case group, which may lead to false–negative results. It is also difficult to distinguish truly different ARHI hearing phenotype patterns using the Z score method. ARHI candidate gene association studies in people over the age of 70 are very necessary.
IQGAPs comprise a class of multidomain proteins that are present in diverse organisms ranging from yeast and Caenorhabditis elegans to Xenopus laevis and mammals [38]. There are three IQGAPs in humans. IQGAP2, which is 62 % identical to IQGAP1, was identified in 1996 [39]. The vast majority (>85 %) of the published literature focuses on IQGAP1. Less is known about IQGAP2 [40 primary papers in PubMed (http://www.ncbi.nlm.nih.gov/pubmed) at the time of writing]. IQGAP2 is found predominantly in liver, but can be detected in prostate, kidney, thyroid, stomach, testis, platelets and salivary glands [39–42]. Loss of IQGAP2 contributes to the tumourigenesis of hepatocellular carcinoma, gastric cancer and prostate cancer. IQGAP2 has long been studied for its role in tumourigenesis, until Lut Van Laer [15] reported an ARHI GWAS study on IQGAP2 in a Finnish Saami population. IQGAP2 was reported to be expressed inside the cochlea [28] and has been implicated in cadherin-mediated cell adhesion [29]. Cadherin-23 (CDH23) plays an important role in sensory hair cells [43], and mutations in CDH23 are responsible for syndromic deafness: Usher syndrome type 1D (Usher 1D) [44–46] and non-syndromic autosomal recessive deafness DFNB12 in humans, and age-related hearing loss in inbred mouse strains [47].
In the present study, we found that the IQGAP2 tag SNP rs457717 as identified by a European GWAS did not contribute to ARHI in a Han male Chinese population both before and after adjusting for environmental risk factors. Our negative results were replicated in two groups (group 70− and group 70+). According to the HapMap data on Rel 27 PhaseII + III, Feb09 (based on NCBI B36 assembly) dbSNP b126 (http://hapmap.ncbi.nlm.nih.gov/cgi-perl/gbrowse/hapmap27_B36/#search), SNPs rs457717 and rs1697845 also exist in Beijing (CHB) dbSNP and are highly correlated (D′ = 1; r 2 = 0.965). The high correlation means that the validation’s results of the two risk SNP rs457717 and rs1697845 in Chinese Han people will be exactly the same. We confirmed the second risk SNP rs1697845 associated with ARHI in the GWAS of van Laer et al was also not associated with ARHI in HMC individuals.
In addition, different audiogram patterns might confound the relationship between candidate gene polymorphisms and ARHI [16, 48]. The genotypes of IQGAP2 did not show a significant effect on ARHI in different audiogram patterns after adjustment for other variables in group 70+.
There is no standard method for hearing correction over the age of 70 years. According to WHO standardised hearing loss categories, normal hearing is defined as a hearing threshold of 0–25 dB for the better ear; when testing the hearing of people markedly over 70 years of age, part of any observed hearing loss will probably be associated with age. In the Mild subgroup (26 ≤ dB HL < 40), false-negative results of the association study may be caused by the hearing data being uncorrected. Therefore, we designed another subgroup, the Hearing disability subgroup (41≤ dB HL), according to WHO standards. We also found no positive association between the IQGAP2 tag SNP rs457717 and ARHI in Han Chinese.
The inconsistency between the results of the previous study performed in Europeans and those of the present study might be attributed to the population differences, which have been reported as key factors leading to non-replication (i.e., failure to replicate findings) among genetic association studies [49]. This result does not exclude the possibility of other causative variants in the IQGAP2 gene. Further testing within the IQGAP2 gene or of the whole gene might be warranted to better elucidate this. Further meta-analysis studies with larger sample sizes and collaborative data comparing different ethnic groups to search for population-specific causative variants might help to explain the inconsistency between these association studies.
Conclusion
The results of our study are the first reported association study between IQGAP2 and ARHI in an Asian ethnic group. We demonstrated that the IQGAP2 risk SNP locus (rs457717: A/G) in intron 13 identified by a European GWAS was not associated with ARHI in Han male Chinese individuals. Population differences could be a key factor leading to the observed non-replication. Further testing within the IQGAP2 gene or of the whole gene might be warranted to better elucidate this.
References
Pacala JT, Yueh B (2012) Hearing deficits in the older patient: “I didn’t notice anything”. JAMA 307(11):1185–1194
Cruickshanks KJ, Wiley TL, Tweed TS, Klein BE, Klein R, Mares-Perlman JA, Nondahl DM (1991) Prevalence of hearing loss in older adults in Beaver Dam, Wisconsin. The epidemiology of hearing loss study. Am J Epidemiol 148(9):879–886
Dalstra JA, Kunst AE, Borrell C, Breeze E, Cambois E, Costa G, Geurts JJ, Lahelma E, Van Oyen H, Rasmussen NK, Regidor E, Spadea T, Mackenbach JP (2005) Socioeconomic differences in the prevalence of common chronic diseases: an overview of eight European countries. Int J Epidemiol 34(2):316–326
Parmet S, Lynm C, Glass RM (2007) JAMA patient page. Adult hearing loss. JAMA 298(1):130
Van Eyken E, Van Camp G, Van Laer L (2007) The complexity of age-related hearing impairment: contributing environmental and genetic factors. Audiol Neurootol 12(6):345–358
Hwang JH, Chen JC, Hsu CJ, Liu TC (2011) Association of obstructive sleep apnea and auditory dysfunctions in older subjects. Otolaryngol Head Neck Surg 144(1):114–119
Hwang JH, Wu CC, Hsu CJ, Liu TC, Yang WS (2009) Association of central obesity with the severity and audiometric configurations of age-related hearing impairment. Obesity (Silver Spring) 17(9):1796–1801
Huang Q, Tang J (2010) Age-related hearing loss or presbycusis. Eur Arch Otorhinolaryngol 267(8):1179–1191
Christensen K, Frederiksen H, Hoffman HJ (2001) Genetic and environmental influences on self-reported reduced hearing in the old and oldest old. J Am Geriatr Soc 49(11):1512–1517
Gates GA, Couropmitree NN, Myers RH (1999) Genetic associations in age-related hearing thresholds. Arch Otolaryngol Head Neck Surg 125(6):654–659
Karlsson KK, Harris JR, Svartengren M (1997) Description and primary results from an audiometric study of male twins. Ear Hear 18(2):114–120
Wingfield A, Panizzon M, Grant MD, Toomey R, Kremen WS, Franz CE, Jacobson KC, Eisen SA, Lyons M (2007) A twin-study of genetic contributions to hearing acuity in late middle age. J Gerontol A Biol Sci Med Sci 62(11):1294–1299
Huyghe JR, Van Laer L, Hendrickx JJ, Fransen E, Demeester K, Topsakal V, Kunst S, Manninen M, Jensen M, Bonaconsa A, Mazzoli M, Baur M, Hannula S, Mäki-Torkko E, Espeso A, Van Eyken E, Flaquer A, Becker C, Stephens D, Sorri M, Orzan E, Bille M, Parving A, Pyykkö I, Cremers CW, Kremer H, Van de Heyning PH, Wienker TF, Nürnberg P, Pfister M, Van Camp G (2008) Genome-wide SNP-based linkage scan identifies a locus on 8q24 for an age-related hearing impairment trait. Am J Hum Genet 83(3):401–407
Friedman RA, Van Laer L, Huentelman MJ, Sheth SS, Van Eyken E, Corneveaux JJ, Tembe WD, Halperin RF, Thorburn AQ, Thys S, Bonneux S, Fransen E, Huyghe J, Pyykkö I, Cremers CW, Kremer H, Dhooge I, Stephens D, Orzan E, Pfister M, Bille M, Parving A, Sorri M, Van de Heyning PH, Makmura L, Ohmen JD, Linthicum FH Jr, Fayad JN, Pearson JV, Craig DW, Stephan DA, Van Camp G (2009) GRM7 variants confer susceptibility to age-related hearing impairment. Hum Mol Genet 18(4):785–796
Van Laer L, Huyghe JR, Hannula S, Van Eyken E, Stephan DA, Mäki-Torkko E, Aikio P, Fransen E, Lysholm-Bernacchi A, Sorri M, Huentelman MJ, Van Camp G (2010) A genome-wide association study for age-related hearing impairment in the Saami. Eur J Hum Genet 18(6):685–693
Van Eyken E, Van Laer L, Fransen E, Topsakal V, Lemkens N, Laureys W, Nelissen N, Vandevelde A, Wienker T, Van De Heyning P, Van Camp G (2006) KCNQ4: a gene for age-related hearing impairment? Hum Mutat 27(10):1007–1016
Dupret JM, Rodrigues-Lima F (2005) Structure and regulation of the drug-metabolizing enzymes arylamine N-acetyltransferases. Curr Med Chem 12(3):311–318
Unal M, Tamer L, Doğruer ZN, Yildirim H, Vayisoğlu Y, Camdeviren H (2005) N-Acetyltransferase 2 gene polymorphism and presbycusis. Laryngoscope 115(12):2238–2241
Bared A, Ouyang X, Angeli S, Du LL, Hoang K, Yan D, Liu XZ (2010) Antioxidant enzymes, presbycusis, and ethnic variability. Otolaryngol Head Neck Surg 143(2):263–268
Van Laer L, Van Eyken E, Fransen E, Huyghe JR, Topsakal V, Hendrickx JJ, Hannula S, Mäki-Torkko E, Jensen M, Demeester K, Baur M, Bonaconsa A, Mazzoli M, Espeso A, Verbruggen K, Huyghe J, Huygen P, Kunst S, Manninen M, Konings A, Diaz-Lacava AN, Steffens M, Wienker TF, Pyykkö I, Cremers CW, Kremer H, Dhooge I, Stephens D, Orzan E, Pfister M, Bille M, Parving A, Sorri M, Van de Heyning PH, Van Camp G (2008) The grainyhead like 2 gene (GRHL2), alias TFCP2L3, is associated with age-related hearing impairment. Hum Mol Genet 17(2):159–169
O’Grady G, Boyles AL, Speer M, DeRuyter F, Strittmatter W, Worley G (2007) Apolipoprotein E alleles and sensorineural hearing loss. Int J Audiol. 46(4):183–186
Uchida Y, Sugiura S, Nakashima T, Ando F, Shimokata H (2009) Endothelin-1 gene polymorphism and hearing impairment in elderly Japanese. Laryngoscope 119(5):938–943
Scherer EQ, Arnold W, Wangemann P (2005) Pharmacological reversal of endothelin-1 mediated constriction of the spiral modiolar artery: a potential new treatment for sudden sensorineural hearing loss. BMC Ear Nose Throat Disord 29(5):10
Sugiura S, Uchida Y, Nakashima T, Ando F, Shimokata H (2010) The association between gene polymorphisms in uncoupling proteins and hearing impairment in Japanese elderly. Acta Otolaryngol 130(4):487–492
Markaryan A, Nelson EG, Hinojosa R (2009) Quantification of the mitochondrial DNA common deletion in presbycusis. Laryngoscope 119(6):1184–1189
Seidman MD, Khan MJ, Bai U, Shirwany N, Quirk WS (2000) Biologic activity of mitochondrial metabolites on aging and age-related hearing loss. Am J Otol 21(2):161–167
Newman DL, Fisher LM, Ohmen J, Parody R, Fong CT, Frisina ST, Mapes F, Eddins DA, Robert Frisina D, Frisina RD, Friedman RA (2012) GRM7 variants associated with age-related hearing loss based on auditory perception. Hear Res 294(1–2):125–132
Robertson NG, Khetarpal U, Gutiérrez-Espeleta GA, Bieber FR, Morton CC (1994) Isolation of novel and known genes from a human fetal cochlear cDNA library using subtractive hybridization and differential screening. Genomics 23(1):42–50
Yamashiro S, Abe H, Mabuchi I (2007) IQGAP2 is required for the cadherin-mediated cell-to-cell adhesion in Xenopus laevis embryos. Dev Biol 308(2):485–493
Fransen E, Van Laer L, Lemkens N, Caethoven G, Flothmann K, Govaerts P, Van de Heyning P, Van Camp G (2004) A novel Z score-based method to analyze candidate genes for age-related hearing impairment. Ear Hear 25(2):133–141
Lee CY, Hwang JH, Hou SJ, Liu TC (2010) Using cluster analysis to classify audiogram shapes. Int J Audiol. 49(9):628–633
International Organisation of Standardisation (2000) ISO 7029 Acoustic-threshold of hearing by air conduction as a function of age and sex for otologically normal persons. Geneva
World Health Organization (2006) Prevention of deafness and hearing impairment: grades of hearing impairment. http://www.who.int/pbd/deafness/hearing_impairment_grades/en/. Accessed 20 May 2007
Luo H, Yang T, Jin X, Pang X, Li J, Chai Y, Li L, Zhang Y, Zhang L, Zhang Z, Wu W, Zhang Q, Hu X, Sun J, Jiang X, Fan Z, Huang Z, Wu H (2013) Association of GRM7 variants with different phenotype patterns of age-related hearing impairment in an elderly male Han Chinese population. PLoS One 8(10):e77153
Dubno JR, Lee FS, Matthews LJ, Mills JH (1997) Age-related and gender-related changes in monaural speech recognition. J Speech Lang Hear Res 40(2):444–452
Wiley TL, Chappell R, Carmichael L, Nondahl DM, Cruickshanks KJ (2008) Changes in hearing thresholds over 10 years in older adults. J Am Acad Audiol 19(4):281–292 (quiz 371)
Price K, Zhu X, Guimaraes PF, Vasilyeva ON, Frisina RD (2009) Hormone replacement therapy diminishes hearing in peri-menopausal mice. Hear Res 252(1–2):29–36
Briggs MW, Sacks DB (2003) IQGAP1 as signal integrator: Ca2+, calmodulin, Cdc42 and the cytoskeleton. FEBS Lett. 542(1–3):7–11
Brill S, Li S, Lyman CW, Church DM, Wasmuth JJ, Weissbach L, Bernards A, Snijders AJ (1996) The Ras GTPase-activating-protein-related human protein IQGAP2 harbors a potential actin binding domain and interacts with calmodulin and Rho family GTPases. Mol Cell Biol 16(9):4869–4878
Wang S, Watanabe T, Noritake J, Fukata M, Yoshimura T, Itoh N, Harada T, Nakagawa M, Matsuura Y, Arimura N, Kaibuchi K (2007) IQGAP3, a novel effector of Rac1 and Cdc42, regulates neurite outgrowth. J Cell Sci 120(Pt 4):567–577
Schmidt VA, Scudder L, Devoe CE, Bernards A, Cupit LD, Bahou WF (2003) IQGAP2 functions as a GTP-dependent effector protein in thrombin-induced platelet cytoskeletal reorganization. Blood 101(8):3021–3028
Cupit LD, Schmidt VA, Miller F, Bahou WF (2004) Distinct PAR/IQGAP expression patterns during murine development: implications for thrombin-associated cytoskeletal reorganization. Mamm Genome 15(8):618–629
Kazmierczak P, Sakaguchi H, Tokita J, Wilson-Kubalek EM, Milligan RA, Müller U, Kachar B (2007) Cadherin 23 and protocadherin 15 interact to form tip-link filaments in sensory hair cells. Nature 449(7158):87–91
Bolz H, von Brederlow B, Ramírez A, Bryda EC, Kutsche K, Nothwang HG, Seeliger M, C-Salcedó Cabrera M, Vila MC, Molina OP, Gal A, Kubisch C (2001) Mutation of CDH23, encoding a new member of the cadherin gene family, causes Usher syndrome type 1D. Nat Genet 27(1):108–112
Bork JM, Peters LM, Riazuddin S, Bernstein SL, Ahmed ZM, Ness SL, Polomeno R, Ramesh A, Schloss M, Srisailpathy CR, Wayne S, Bellman S, Desmukh D, Ahmed Z, Khan SN, Kaloustian VM, Li XC, Lalwani A, Riazuddin S, Bitner-Glindzicz M, Nance WE, Liu XZ, Wistow G, Smith RJ, Griffith AJ, Wilcox ER, Friedman TB, Morell RJ (2001) Usher syndrome 1D and nonsyndromic autosomal recessive deafness DFNB12 are caused by allelic mutations of the novel cadherin-like gene CDH23. Am J Hum Genet 68(1):26–37
Tabor HK, Risch NJ, Myers RM (2002) Candidate-gene approaches for studying complex genetic traits: practical considerations. Nat Rev Genet 3(5):391–397
Noben-Trauth K, Zheng QY, Johnson KR (2003) Association of cadherin 23 with polygenic inheritance and genetic modification of sensorineural hearing loss. NatGenet. 35(1):21–23
de Heer AR, Pauw RJ, Huygen PL, Collin RW, Kremer H, Cremers CW (2009) Flat threshold and mid-frequency hearing impairment in a Dutch DFNA8/12 family with a novel mutation in TECTA. Some evidence for protection of the inner ear. Audiol Neurootol 14(3):153–162
Van Eyken E, Van Camp G, Fransen E, Topsakal V, Hendrickx JJ, Demeester K, Van de Heyning P, Mäki-Torkko E, Hannula S, Sorri M, Jensen M, Parving A, Bille M, Baur M, Pfister M, Bonaconsa A, Mazzoli M, Orzan E, Espeso A, Stephens D, Verbruggen K, Huyghe J, Dhooge I, Huygen P, Kremer H, Cremers CW, Kunst S, Manninen M, Pyykkö I, Lacava A, Steffens M, Wienker TF, Van Laer L (2007) Contribution of the N-acetyltransferase 2 polymorphism NAT2*6A to age-related hearing impairment. J Med Genet 44(9):570–578 (Epub 2007 May 18)
Acknowledgments
This research was supported by grants from Medical Engineering (Technology) Cross Research Fund, Shanghai Jiao Tong University (No. YG2014MS47), and grants from the Medical Research Fund of Shanghai Municipal Health and Family Planning Commission (No. 201440295).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors indicate they have no financial relationship with the organisation that sponsored the research. And the authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Luo, H., Wu, H., Shen, H. et al. The European GWAS-identified risk SNP rs457717 within IQGAP2 is not associated with age-related hearing impairment in Han male Chinese population. Eur Arch Otorhinolaryngol 273, 1677–1687 (2016). https://doi.org/10.1007/s00405-015-3711-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-015-3711-9